
Abstract
Stroke is the third leading cause of death in the developed world and the primary cause of adult disability. The most common site of stroke is the middle cerebral artery (MCA), an artery that supplies a range of areas involved in both language and motor function. As a consequence, many stroke patients experience a combination of language and motor deficits. Indeed, those suffering from Broca’s aphasia have an 80% chance of also suffering hemiplegia. Despite the prevalence of multifaceted disability in patients, the current trend in both clinical trials and clinical practice is toward compartmentalization of dysfunction. In this article, we review evidence that aphasia and hemiplegia do not just coexist, but that they interact. We review a number of clinical reports describing how therapies for one type of deficit can improve recovery in the other and vice versa. We go on to describe how language deficits should be seen as a warning to clinicians that the patient is likely to experience motor impairment and slower motor recovery, aiding clinicians to optimize their choice of therapy. We explore these findings and offer a tentative link between language and arm function through their shared need for sequential action, which we term fluency. We propose that area BA44 (part of Broca’s area) acts as a hub for fluency in both movement and language, both in terms of production and comprehension.
Introduction
About 150 years ago, a number of scientists began writing about a special relationship they had noticed between language function and right hemiplegia in children with cerebral paralysis. 1 This discussion was maintained for many years, right up until about 20 years ago.2-6 What was never resolved was whether this link was symptomatic of an overlap in function or merely a quirk of anatomy. Given the physical proximity of various functionally distinct cortical areas and the fact that cerebral blood flow does not respect their functional boundaries, it is quite possible that multiple, unrelated functional deficits can and do result from a single stroke event.
With the advent of more sophisticated electrophysiological tools and models of cortical function one might think that this debate had since been resolved. Unfortunately, in more recent times, study of an interaction between the 2 disorders has become more the exception rather than the rule, halting progress on an important question that goes to the heart of neural organization and routes to therapy. This lack of an integrated approach is not unique to limb movement and language but is symptomatic of a trend toward increased discipline specialization across the medical sciences. 7
This trend toward specialization is having an impact not just at the level of basic science but right through the system, up to and including our approach to treatment. Recent years have seen huge improvements in patient treatment and rehabilitation through maintenance and analysis of detailed patient record data, but neglect of the link between aphasia and motor deficit makes it surprisingly difficult, even in this age of big data, to test for interactions between the 2 disorders. 8 To quantify the problem, we carried out a brief literature search (Table 1.). The search turned up thousands of articles on upper limb impairment, or language deficit, but very few articles that consider both.
Articles Found on PubMed on March 13, 2018. a
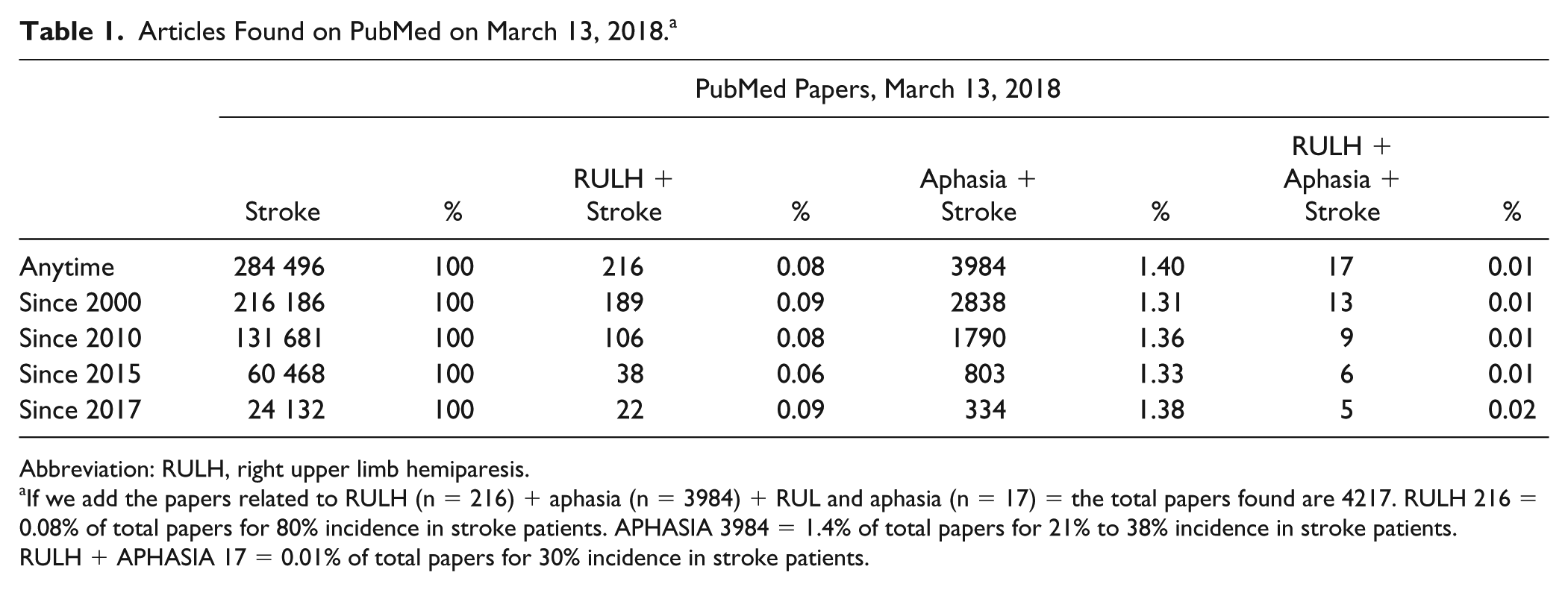
Abbreviation: RULH, right upper limb hemiparesis.
If we add the papers related to RULH (n = 216) + aphasia (n = 3984) + RUL and aphasia (n = 17) = the total papers found are 4217. RULH 216 = 0.08% of total papers for 80% incidence in stroke patients. APHASIA 3984 = 1.4% of total papers for 21% to 38% incidence in stroke patients. RULH + APHASIA 17 = 0.01% of total papers for 30% incidence in stroke patients.
The total number of papers related to right upper limb hemiparesis (RULH) was 216. The total on the topic of aphasia was 3984. The total number of papers dealing with both RULH and aphasia was just 17. These numbers do not translate well into actual incidence in stroke patients. RULH affects 80% of stroke patients, 9 whereas the incidence of aphasia is comparatively lower, at 21% to 38%.10-12 Most striking of all though, was the tiny number of papers considering both of these disabilities, despite an incidence in stroke patients of close to 30%.13-17 What is more, the few papers that have considered hemiparesis and aphasia together were, in general, weakly cited (Balliet et al, 1986 cited 41; Martinez Segon, 2013 cited 1; Maitra, 2006 cited 15; Arya, 2014 cited 4; Harnish, 2014 cited 11), confirming the low level of interest in the combination of deficits. This lack of interest flows on into treatment as well. Based on 3 major repositories for information on current and past clinical trials for stroke, a similar pattern emerges—see Table 2 and the appendix.
Number of Trials Found on the 3 Main World Registries on March 13, 2018.
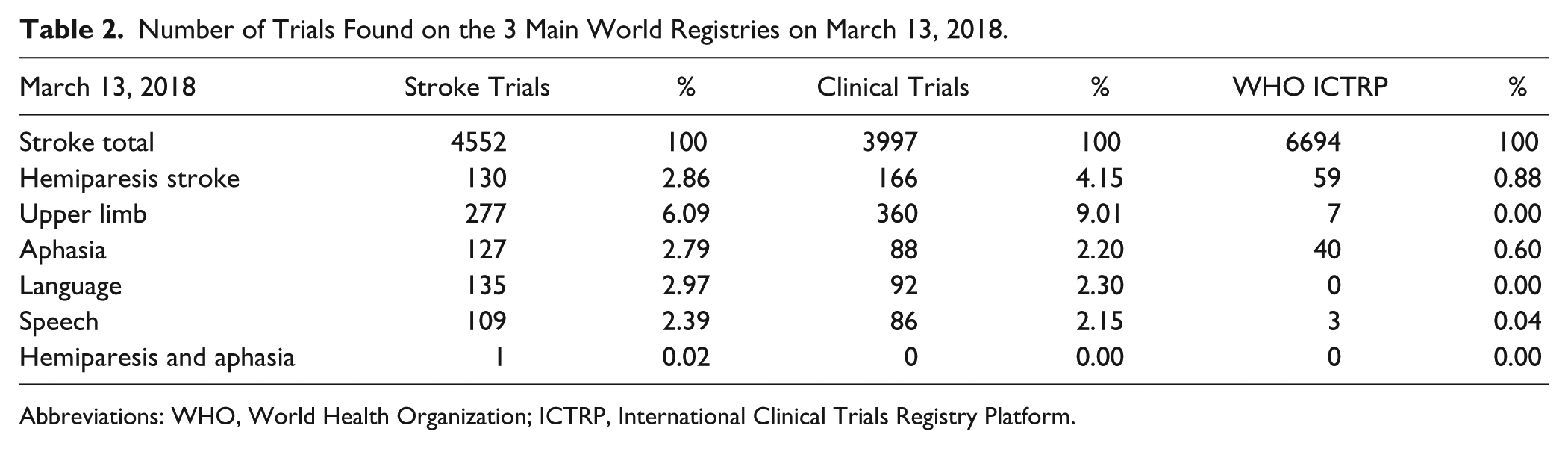
Abbreviations: WHO, World Health Organization; ICTRP, International Clinical Trials Registry Platform.
These figures underline how the current siloed approach to the study of stroke is impacting research and publications, treatments and clinical trials, as well as funding. It seems likely that this trend is reflected in health care planning as well.
The Case for a Link
A review of the basic science on aphasia reveals that the impetus for change is already there. Aphasia is now acknowledged as being associated (or co-occurring) with an array of deficits in motor and cognitive domains. This is why, more and more, scientists talk of an aphasic “syndrome”18,19 in which language deficit is just one typical feature of an underlying deficit, which includes impairments of cognitive function and memory.
As we will describe in the coming pages, this thinking is supported by many lines of evidence pointing to the existence of a link between motor and language impairment, a link that goes far beyond a shared blood supply. From a purely functional perspective one reason for linking the two activities is that they share a common goal, that of preparing a sequence of actions which demand acute control of timing. We hypothesize that motor and language systems share a common neural substrate, and that its impact can be behaviorally observed as a lack of fluency in the output of both systems. Note here that language fluency encompasses all levels of language processing including articulation, syntax, semantics, and coherence. 20 Thus, motor and language systems deficits will often coexist because of the shared neural resources subserving them. It was no accident that Broca referred to the language impairment he studied as nonfluent aphasia. It was the lack of fluency of the spoken language that first struck him. And it is the same lack of fluency that we find in other deficits such as stuttering, which often presents after stroke.21-23 This may well explain why therapy for one deficit can help improve performance on both types of task, because it works on the fluency feature, or better, it works to compensate for the lesion of the networks that are in charge of the characteristic of fluency, be it in language or movement.
Advances in anatomical and functional imaging have allowed researchers to study the causes of impaired fluency both in stroke and in congenital dysfunction. In the case of stuttering, for example, Beal and his team found that the trajectory of gray matter development is abnormal in people who stutter. 24 In particular, the thickness of the grey matter in the left pars opercularis of Broca’s area (corresponding to Brodmann’s area 44, BA44) did not have the typical linear maturation pattern, being thinner in younger patients and thicker in older ones compared with the control group. This suggests that the neuroanatomic microstructure of the area is essential for the development of fluent language-motor control. Similarly, we see that nonfluent aphasics carry their lack of fluency across into different modalities. For example, they cannot perform a pantomime fluently. 25 Even healthy people, when engaged in dual motor tasks like reading and drawing, demonstrate that language (listening and speaking) and manual fluency or disfluency go together, either they are both fluent or not. 26 Clearly, fluency is a feature which goes beyond one cognitive function and for that reason, it is managed by higher order systems. 27 Based on various results from different fields, one of the system hubs seems to be located in Broca’s area, more specifically in BA44.28,29
The Evolution of Language
One of the strands of evidence in support of a link between motor behavior and language comes from considering how language evolved. Corballis has suggested that language existed originally in the form of gesture and that our human ancestors switched their mode of communication to speech about 50 000 years ago. 30 This theory is supported by neuroimaging work showing similarities between humans’ and nonhumans primates’ recognition of speech and gestures, drawing an indirect path from gestural communication in apes to a “language ready brain” in Homo sapiens. 31 As well as co-development on evolutionary time scales, there is also circumstantial evidence, at least, that motor and speech faculties develop in partnership over the lifetime of an individual as well. Piaget and Vygotsky discuss the relationship between speech and symbolic play, dreams, and deferred imitation, faculties which are all seen to emerge together during infancy, in general synchrony with the 6 stages of sensorimotor development.32,33
Of course, if the 2 systems are so closely intertwined, one might ask why other apes failed to make the transition to speech. Certainly, recent anatomical and genetic studies have revealed just how closely our physiology matches that of other apes. For example, Diogo and his team, revealed that the laryngeal muscle arytenoideus obliquus, can be found in chimpanzees and gorillas despite the long-held belief that it was uniquely associated with speech production. 34 One possible explanation is that speech (and perhaps language) only emerged through a precursor stage in which primate calls were progressively refined and developed, reducing the relative importance of gestural communication. 35 Ultimately, whichever hypothesis one prefers, it is clear that gesture has been, and remains, a central method for conveying meanings and communicating, and it seems not unreasonable to suppose that speech may well have emerged from preexisting cortical systems governing this closely related ability.
To understand how preexisting gestural/language systems might have been adapted or coopted for speech we need only think about the classic sensory substitution experiments of Bach-Y-Rita. 36 Some neural reuse theorists argue that this capacity for adapted use is exactly what cortex was designed for. They argue that neural circuits are designed to be exapted (exploited, recycled, redeployed) over evolutionary or lifetime development, and put to different uses, often without losing their original functions and without an injury to trigger the change. These theories offer a distinct perspective on the evolution and development of the brain, including the evolutionary-developmental pathway supporting primate tool use and human language. The concept is not without practical application either. In fact, it offers highly practical implications in the areas of rehabilitative medicine. 37 Brainport, for example, is the translation of Bach-Y-Rita’s work into rehabilitation. 38
Cognitive Models of Language and Motor Control
The idea of a deep link between motor and cognition is not new. The first motor theories of perception were formulated in the early 18th century by Berkeley in his “New Theory of Vision.” 39 The idea was further developed by several researchers, including William James and, later, Roger Sperry. Sperry argued that perception and action processes are functionally intertwined: perception is a means to action and action is a means to perception. 40 In the same year, Cooper and colleagues presented a motor theory of speech perception, 41 which was to form the basis of the highly influential paper by Liberman and Mattingly 42 in which they proposed that comprehension of language is partly dependent on the perception of oral articulatory movements.
More recently, Jeannerod developed his theory of motor cognition in which specific words are associated with specific movements. 43 This idea received support through the discovery of mirror neurons in primate cortex, which appear to show how perceptual and motor systems share common computational codes and neural architectures. 44 Building on these discoveries, Purvelmüller and colleagues have described how cortical cell assemblies link knowledge not just about actions and perceptions but across a wide range of higher cortical functions, including attention, meaning and concepts, sequences, goals, intentions and, importantly, communicative social interaction. 45 From their perspective, language learning leads to the formation of action perception circuits with specific distributions across cortical areas. 46
Part of Pullvermüller’s evidence for this idea comes from event-related functional magnetic resonance imaging (fMRI) showing activation of cortical areas along the motor strip during the reading of action words referring to the face, arm or legs and actual movements of the tongue, fingers, and legs. 47 Further investigations have confirmed the interdependency of circuits for action and perception with motor circuits contributing to the comprehension of phonemes, semantics, and grammar. 48
Hence it seems that language learning and consequent language deficits may be rooted in a person’s ability to perform complex sensorimotor transformations.49-51 For example, a preactivation of hand- and leg-motor networks by finger/foot movements facilitates the ignition of semantic cell assemblies for hand- and leg-related words, respectively. 52 It has also been reported that during a conversation, the neural processes supporting speech production and perception, overlap in time. 53 Moreover motor system activity can have facilitatory and inhibitory effects on language processing of action related words. 54
Apraxia–Imitation–Comprehension
It has been known for some time that people with aphasia (PWA) have difficulties in pantomiming actions. This inability is generally regarded as an apraxic disorder (mainly ideomotor apraxia), and hence not simply due to a general communication disorder. Recent studies have found links between gesture ability and aphasia type. What is more, aphasia type appeared to have an impact on the types of gesture the PWA produced. The gestural expression of the participants with Broca’s aphasia was characterized by a depiction of concrete images and a rich demonstration of the characters’ actions in the story. All the participants with Wernicke’s aphasia used iconic gestures and had a high use of metaphoric, that is, they depicted the story abstractly.
Also, an interesting correlation was reported between speech fluency and gesture production. The proportion of PWA using gesture/pantomime in their narratives was higher in the low fluency group, usually Broca’s as strategy to compensate the failure in verbal communication. Same higher proportion was seen in PWA with low score in word retrieval (typical of anomic aphasia where speech is fluent but there is difficulty in finding words, which is the results of no specific brain lesion) indicating that the failure in output is compensated by the use of gestures. These differences should encourage clinicians to perform an empirical investigation before considering gesture-based treatments. For example, patients with Broca’s—who are likely to be capable of pantomime production—could be encouraged to produce these gestures during communication repair, especially if the individual is not spontaneously doing so. 55
Understanding and producing speech requires semantic processing. 56 For many years, it was believed that PWA who also had concurrent right arm hemiparesis would experience greater language loss, simply because they would be forced to use their nondominant left arm, leading to more limited performance in pantomiming. In fact evidence suggests that there is no difference in the number of gestures used by PWA and hemiparesis versus those who do not have hemiparesis. 57 There also does not appear to be any impact on the comprehensibility of their gestures. 58 Instead, a limiting factor appears to be the severity of their aphasia and the patient’s capacity for semantic processing. 59 In a recent trial, van Nispen, discovered that PWA were able to convey information using pantomime that they could not with speech. However, the comprehensibility of pantomime was shown to be lower in PWA than healthy subjects based on the difficulties in semantic processing. Comprehensibility was also lower in apraxia and the inability to use the right hand, underlining the potential benefit of pantomime for rehabilitation. 60 The results are not in accordance with previous studies but 2 factors could explain the controversy: PWA using the nondominant hand maybe produce pantomime less accurate therefore less comprehensible (ie, pretending to write with the left hand); also some pantomimes require both hands. For individuals with language difficulties, pantomime offers a useful means for communication. The fact that PWA will often also experience deficits in pantomime makes it important to identify whether a PWA does indeed struggle in this area, and if so what aspects of pantomime production they struggle with. 61
Apraxic stroke patients with left hemisphere lesions show deficits in action imitation, action recognition, and action comprehension. A study of the locus of their lesions consistently points to disruption of areas central to the putative mirror neuron system (MNS). Patients with apraxia performed significantly worse in all 3 motor cognitive tasks compared with nonapraxic patients. Despite the overlap in lesions, deficits in gesture comprehension were mainly associated with lesions of more anterior parts of the MNS, whereas lesions located more posteriorly mainly resulted in gesture imitation deficits, supporting the hypothesis that left hemisphere lesions to the MNS core regions affected the imitation, recognition, and comprehension of meaningful actions. Deficits in gesture tasks were associated within left operculum and the left insula lesions as well as the left IFG (including BA 44). Subcortically, lesions affecting the left pallidum and left putamen were significantly associated with lower accuracy in gesture comprehension indicating a role of basal ganglia not just in regulation of movements, in learning and memory, therefore in understanding gestures. White matter tracts, as the superior occipitofrontal fascicle and the superior longitudinal fascicle, were also associated with deficits in gesture comprehension, an important point to keep in mind when thinking of possible recovery enabled by neuroplasticity (we know that neuroplasticity degree is much lower for white matter). 62
Clinical Practice–Imitation Therapy–Pantomime
The move to redefine what is meant by aphasia has in part been fueled by a significant problem facing clinical practice, namely the heterogeneity of symptoms seen across patients. Even if one considers patients from within just one of the two classically delineated groups of Broca’s aphasia and Wernicke’s aphasia, variations in symptoms and recovery rates abound. To date, it has proven very difficult for any classification to accommodate such variability.63-66 This is a problem because it suggests that current standard therapies are failing to meet any one patient’s specific needs. This is why development of a comprehensive model of the root causes of a specific deficit is important.
A model of the kind we are proposing clearly predicts not only the co-occurrence of specific deficits but also interactions in their treatment. A review of the clinical literature does indeed reveal evidence for such interactions. For example, recent studies have shown that speech therapy improves motor function of the arm and vice versa (as described below), suggesting that instead of applying one selective therapy at a time for a single deficit, it may be possible to treat multiple impairments simultaneously with significantly improved outcomes for patients. In one of these studies, Maitra et al 67 reported the impact of concurrent self-speech in a reaching task involving chronic stroke patients with hemiparesis. After 6 weeks patients required to speak at the moment of movement initiation attained higher reaching velocities than no speech controls. 67
The beneficial effects of motor training on language have likewise been reported by Arya et al. 68 Another study on 14 chronic PWA was conducted with the aim of shifting laterality from left frontal lobe to right during word production. fMRI posttreatment revealed a successful shift only when picture naming was accompanied by left hand movements. Moreover, patients showed a benefit for untrained categories as well, suggesting that there was a general engagement of intact cortical substrates (right frontal lobe). 69 In a rehabilitation program using repetitive transcranial magnetic stimulation, the authors targeted motor function, proposing that left hand motor movement would engage the intentional cognitive system and the pre–supplemental motor area. They demonstrated that this, in turn, improved language outcomes. Likewise, patients with chronic aphasia showed long term improvements in communication after transcranial direct current stimulation over the left primary motor cortex combined with language therapy, underlining how the motor system is functionally connected to the language network. 70
This intrinsic link between motor and right-upper limb recovery is also evident in reports of therapies which have targeted the MNS,69,71-80 or made use of music and have shown a benefit for both types of deficit.59,81-83 For example, observation and repetition training has been used in patients with impaired language function. Hand action observation prompted improvements compared with static object observation, and this was concomitant to higher activations in MNS detected in fMRI, thus confirming that mirror neuron–based therapy can facilitate the recovery of language function in PWA. 73
Marangolo and Buccino found similar results when studying the effect of action observation treatment in rehabilitation after stroke in Parkinson patients, in children with cerebral palsy, and in language therapy.72,84 Imitation-based aphasia therapy was associated with increased narrative content in patients with chronic aphasia after left hemisphere stroke; furthermore, the therapy promoted a generalized gain to an unrelated narrative production task. 76
Speech
Two dissociable frontal networks seem to be engaged during speech production, as seen in stroke patients with left hemisphere damage and aphasia: motor areas relate to verbs and perception areas to nouns.79,85
Mina and colleagues explored the possible impact of language therapy on the integration level of the default mode network in patients suffering from anomia (impaired noun retrieval). They reported that language therapy not only can improve integration in circuits other than language processing circuits, it also has a prognostic value in guiding the clinicians to the most effective therapy. 77 Consistent with the suggestions being made in this article, the authors explicitly state that trans-disciplinary therapies should be adopted. 86
A study on limb apraxia and aphasia came to the conclusion that there are numerous ways in which apraxia and aphasia are linked, while also acknowledging that there are distinct and nonoverlapping aspects to these conditions too. The authors sought to underline the fact that the very coexistence of apraxia and aphasia “may have a direct impact on efforts towards patients’ rehabilitation.” 87
Based in part on these studies, researchers have been trying to understand the possible relationship between syntax, space (the spatial position of a word in a sentence and syntax reflect the real-world ordering of events with subject-verb-object or subject-object-verb order accounting for 90% of world’s languages) and upper limb usage during a task involving language skills, with results suggesting that the control of language, space and upper limb movement represent three distinct yet intertwined systems. 88
Crinion and Leff’s literature review on recovery of stroke aphasia aimed to clarify numerous issues relating to post-stroke recovery and the impact of therapy. 89 The authors began by considering why many previous studies have actually found little or no benefit of therapy over and above levels of spontaneous recovery. In their view, this is due to a number of factors that boil down to a lack of statistical power: issues such as small sample size, inherent large interindividual differences, and the use of interventions that were too short (<40 hours). In particular, the authors argue that interindividual differences are crucial, since the capability of learning differs among patients with apparently similar language impairments. Keeping in mind that learning involves many cognitive processes (eg, attention, memory, reward) and that the neural substrates for language and nonlanguage processes overlap, they suggested that aphasia therapy should target the capacity of the patient to learn in different domains (eg, motor) instead of targeting the language impairment alone. 74
For over a century, pantomime of tool use has been employed to diagnose limb apraxia, a disorder of motor cognition primarily induced by left brain damage. Matters grow complicated because 2 main nodes (anterior and posterior) involved in the network of pantomime and tool-use can be affected and evaluated at multiple levels: such as the action’s semantic characteristic versus the purely motor aspects. The findings of Finkel et al 90 support a model in which anterior and posterior nodes of the left fronto-temporo-parietal network contribute differentially to pantomime of tool use, with communicative aspects represented in more anterior-ventral regions and motor-cognitive aspects in more posterior-dorsal nodes of a left fronto-temporo-parietal network.
In practice, more recent, large-scale studies have clearly identified a benefit for a range of aphasia treatments. 91 Hence the question is no longer whether treatment is effective, but whether novel combined language and motor treatments offer more than targeted, language-specific treatments. This is where more work needs to be done. As mentioned in our sketch of the problem above, large-scale, well-controlled studies are not easy to find. Instead we have to turn to clinical reports on small-scale studies. One such report has described improvements in untreated language function after intensive upper limb rehabilitation in chronic-phase patients, some of whom were many years poststroke 79 and hence unlikely to be experiencing any further, spontaneous recovery.92-94 Other studies were conducted on chronic patients, confirming that the recovery was solely the result of the treatment therefore taking out of the equation the possibly confounding factor of spontaneous recovery.67,70,76,79,81,95 The team’s explanation for the concomitant improvements of language and arm function again supports the hypothesis that language and arm movements are in some respects dependent on the same neural hardware. 78 In order to progress this field, what is needed now is a large-scale, suitably controlled study in which traditional and combined therapies are directly compared in a functionally prescreened aphasic population.
When thinking about gesture therapy for patients with aphasia, we agree with Mokaya that it would be useful to observe gesture comprehension, to videotape the patient gesturing and to include family members in gesture-based therapy. 96 One thing to bear in mind is the functions the gestures play in the life of the patient (eg, a communicative purpose) and that co-morbid deficits may impact a patient’s ability to learn to use gestures. Interestingly, researchers found that more gestures were used during non-fluent than during fluent speech and that there was a positive relationship between gestures and fluency. The participants in the study used more gestures when they were experiencing nonfluency, but it did not help them become more fluent. The more gestures were used, the lower their fluency, and the more severe the aphasia, the more gestures were used.
Prediction–Broca–Wernicke
A third reason for emphasizing the link between language and motor systems is that the presence (or absence) of specific forms of aphasia has the potential to act as a predictor for the presence (or absence) of motor deficits and their likely cause. This then carries significant implications for the choice of chronic-phase treatment and program of rehabilitation.
In the early 1980s, it was discovered that Broca’s aphasics do not just suffer from impaired language production, but comprehension as well, especially with more complex syntactic structure. This led to a later discovery that motor-cortex stimulation may strengthen content-specific word-to-semantic concept associations during language treatment in poststroke aphasia. 97
In general, patients with nonfluent forms of aphasia (eg, Broca’s) have more difficulty retrieving verbs than nouns, whereas those with fluent forms of aphasia (eg, anomic) have more difficulty retrieving nouns than verbs. What is more, after treatment, individuals with Broca’s aphasia improve more for noun retrieval and patients with fluent forms of aphasia (conduction and Wernicke’s), improved especially for verbs.
If there is a link between verbs and gesture knowledge, verb retrieval may be particularly amenable to gesture + verbal training in left hemisphere poststroke aphasia. That type of training has the potential to improve communication by increasing spoken word retrieval and by promoting use of gesture as a means to communicate when word retrieval fails. In one study, improvements in gesture production were evident for all the participants (except one with Wernicke’s aphasia). 98
One of the largest studies to directly assess this predictive link was conducted by Gialanella et al, 99 who reported data from 262 patients. In their study they reported that, compared to patients without aphasia, aphasic patients had significantly lower motor functional independence measure and cognitive functional independence measure scores both at admission and after treatment. However, in contrast to our hypothesis, the authors chose to attribute this to a comprehension deficit which they argued prevented patients from understanding therapeutic instructions. This interpretation could have been corroborated if they had chosen to distinguish the types of aphasia, but unfortunately, they did not present these data.
Similar results were published by Martinez Segon et al 100 and by Hilari 101 who both reported lower motor and functional recovery for PWA. Other studies confirmed aphasia as a predictor of worse outcomes especially based on difficulty in comprehension102,103 and attention/working memory. 104 On the other hand, Pedersen et al 12 reported that aphasia had no effect either on recovery or functional independence at discharge. The main problem interpreting this or any of the reported studies is that it can be difficult to draw comparisons because the type of aphasia is not reported, or it is not correlated specifically to the outcome. This is further complicated by the concomitant presence of apraxia of speech (AOS speech motor planning/programming disorder) and aphasia (language-based impairment).
Despite the limited and at times mixed findings from these types of retrospective analyses, another important source of evidence for a link between aphasia and motor deficit comes from the impact of acute-phase treatment on outcomes. At least two groups are currently advocating the use of thrombolytic treatment for patients with aphasia, even in cases of mild ischemic stroke that would not normally be considered on the basis of the motor-related NIHSS (National Institutes of Health Stroke Scale) alone.105,106
Of course, in more general terms, the presence of multiple deficits should be seen as a red flag, if only because it is indicative of more widespread damage or damage to important connective tissue. Ramsey and his team have highlighted the crucial role played by connective, white matter tissue in motor and language deficits, an issue that has been largely ignored in favor of the study of cortical lesions. 107 More to the point, Ramsey et al 107 found a direct association between damage to the white matter and poor outcomes. This finding is consistent with a report that neuroplasticity is higher in patients with cortical damage than in those with damage to white tracts, specifically those who received surgical treatment for low-grade glioma. 108
Overall, based on the evidence described here, and in the preceding section on clinical practice, we would argue that the presence of specific language deficits poststroke should serve as a red flag to clinicians, warning that motor ability should also be especially carefully assessed. Where motor deficits do exist, there is growing evidence that the presence of aphasia indicates that any motor impairment is likely to take longer to recover and that specific therapies which target broader abilities such as fluency, may be most appropriate.95,109-111
Very often, stroke patients present with concomitant apraxia of speech (AOS speech motor planning/programming disorder) and aphasia (language-based impairment), making the prediction of recovery more difficult. For that reason, Ballard et al 112 constructed a predictive model with the aim of improving the efficiency of diagnosis.
Networks: Aphasia–Apraxia–Hemiparesis
The fourth and final element to the solution requires a change of mind-set, one that embraces a more integrated and global view of brain function. Much of the early progress made in our understanding of brain function came from the study of stroke. But progress was necessarily limited by our capacity to assess the true cellular impact of a stroke event. Up until 20 or 30 years ago, neuroscientists had to wait months or sometimes years after a stroke event before they were able to perform an autopsy. And it was only then that they could begin to relate patient’s symptoms to specific brain lesions. What they found was often a focal lesion. This supported a localized view of brain function.
Although the advent of anatomical MRI has allowed us to view damage in the still active, intact brain, it has largely perpetuated the localization model. In more recent years, functional imaging, diffusion tractography, brain stimulation work, and electroencephalography (EEG) have all helped provide us with a more comprehensive view of the living brain both in the healthy and in stroke patients. Now we can see networks and we can see how they continuously change when performing specific tasks. This work has helped identify a role for regions not classically associated with language, in language recovery. For example, Geranmayeh et al 113 used functional imaging to isolate regions involved in language production from those involved in general cognitive function. The group concluded that long-term language recovery was predicted by the level of activity recorded in “domain-general” cortical regions such as the pre–supplemental motor area/dorsal anterior cingulate. In more general terms, imaging and stimulation studies have revealed how varied the sites of damage can be in patients presenting with functionally similar deficits,70,89 challenging classical models and providing the framework for a more integrative understanding of the systems supporting motor behavior and language ability.
Studies based on event-related potentials in EEG have identified activity in the left inferior frontal gyrus, in particular Broca’s area BA44, which is linked to mediating morpho-syntax. This means that the processing of syntax recruits Broca’s area and semantic processes recruits the medial temporal lobe, results that run contrary to the notion of a unitary language system. 114
For example, Hogrefe et al 115 compared the comprehensibility of gestural communication of persons with severe aphasia and nonaphasic controls and found that patients with aphasia conveyed more information via gestures a compensatory tool. The voxel-based lesion symptom mapping (VLSM) analysis suggested that poor gestural expression was associated with lesions in anterior temporal and inferior frontal regions, anatomically adjacent and connected by the uncinated fasciculus. The authors propose that the anterior temporal regions are involved in retrieval of semantic information, acting as a supramodal hub, whereas the frontal regions contribute to selection of communicative strategies, revealing a cooperation among areas in the form of a distributed network. Exploration of the neural substrates of gestural expression has potential ecological significance as a help for finding the optimal strategies to compensate loss of verbal expression in severe aphasia.
The very fact that apraxia is regularly associated with aphasia, opens the question of whether their co-occurrence is the expression of a common deficit or the result of anatomical proximity of their neural substrates. We can find conflicting answers depending on which of their symptoms are considered. Using the VLSM, Goldenberg and Randerath 116 discovered 2 areas of overlap between aphasia and apraxia. Lesions in the anterior temporal lobe and left inferior parietal lobe interfered with pantomime of tool use and with all linguistic tests.
Furthermore, the more common occurrence of apraxia with aphasia (90% as reported by Piercy et al 117 ) compared with the less common occurrence of aphasia with apraxia (53%) brings into the debate how language and praxis are co-represented in the left hemisphere. Looking at the results of their study, Weiss et al 118 concluded that, as lesions of BA44 led to combined apraxic and aphasic deficits, BA44 is involved in semantic processing and acts as an interface between language and (meaningful) action. A further analysis of BA44, based on connectivity and receptor for neurotransmitter mapping, supported a parcellation schemes with lesion of subarea BA44 ventral specifically resulting in combined aphasia and apraxia, encompassing its role in the detection of supramodal meaning. 118 Not to forget the different cytoarchitectonic and connections of BA44 and BA45. 119
Apart from lesions to specific areas, we should bear in mind that lesion to fasciculus connecting areas result in impairments. Imitation of tool-use gestures (transitive; eg, hammering) and communicative (intransitive; eg, waving goodbye) is indeed frequently impaired after left-hemispheric lesions. But they rely on ventrodorsal and ventral streams, respectively, because transitive actions demand a higher temporospatial processing (transitive) while intransitive gestures rely more strongly on semantic information. 120
In their 2013 article, Kobayashi and Ugawa sought to develop a model that could explain why apraxia of speech is often present after stroke in the left hemisphere and concomitant with expressive aphasia. Their model, based on sharing of sensory-motor integration, symbolic representation and anatomical overlapping of the 2 systems, unifies the characteristics shared by apraxia and aphasia while also acknowledging that there are distinct and nonoverlapping aspects to these conditions. 121 A later study on limb apraxia and aphasia came to the same conclusion, underlining the fact that the very coexistence of apraxia and aphasia “may have a direct impact on efforts towards patients’ rehabilitation.” 87
To date, a problem plaguing the modeling of poststroke recovery is finding evidence of neural repair to correlate with functional recovery. One promising area of current investigation lies in the application of EEG recordings focused on firing coherence. A recent study found reports evidence that coherence in firing between language and motor nodes correlated with performance on motor and language tests at 3 weeks and 3 months after stroke. 122
Conclusion
So, how can this short excursion through the literature help clinicians in their role of delivering the best therapy when it comes to a stroke patient? As underlined earlier in this article, it is essential to consider multiple deficits like aphasia and hemiparesis together. A lack of fluency in language should be a red flag for practitioners when considering motor treatments and therapies. Likewise, detailed analysis of area BA44 appears important for considering deficits in either domain. When these features are present, we already know that therapies that involve mirror neurons such as pantomime, imitation observation and so on, may well not work because the very neurons that are supposed to help, are damaged. On the other hand, if a patient is fluent and/or BA44 is not damaged, such therapies may be beneficial. This approach provides a simple and effective way to divide stroke patients in 2 groups, and above all, to avoid putting patients under further distress by exposing them to the wrong therapy.
Footnotes
Appendix
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.