
Abstract
Background. Executive control deficits are deleterious and enduring consequences of moderate-severe traumatic brain injury (TBI) that disrupt everyday functioning. Clinically, such impairments can manifest as behavioural inconsistency, measurable experimentally by the degree of variability across trials of a reaction time (RT) task (also known as intraindividual variability [IIV]). Growing research on cognition after TBI points to cognitive deterioration in the chronic stages postinjury. Objective. To examine the longitudinal recovery of RT characteristics (IIV and more detailed ex-Gaussian components, as well as the number of impulsively quick responses) following moderate-severe TBI. Methods. Seventy moderate-severe TBI patients were assessed at 2, 5, 12, and 24+ months postinjury on a go/no-go RT task. RT indices (ex-Gaussian parameters mu and sigma [mean and variability of the normal distribution component], and tau [extremely slow responses]; mean, intraindividual coefficient of variation [ICV], and intraindividual standard deviation [ISD]) were analyzed with repeated-measures multivariate analysis of variance. Results. ICV, ISD, and ex-Gaussian tau significantly decreased (ie, improved) over time in the first year of injury, but worsened from 1 to 2+ years, as did the frequency of extremely fast responses. These quadratic patterns were accentuated by age and shown primarily in tau (extremely slow) and extremely fast (impulsive) responses. Conclusions. The pattern of early recovery followed by decline in executive control function is consistent with growing evidence that moderate-severe TBI is a progressive and degenerative disorder. Given the responsiveness to treatment of executive control deficits, elucidating the trajectory and underpinnings of inconsistent behavioral responding may reveal novel prognostic and clinical management opportunities.
Keywords
Moderate-severe traumatic brain injury (TBI) results in enduring deficits to attention1,2 that impede return to school and work.3,4 An individual’s moment-to-moment inconsistency of attention—a hallmark of the clinical presentation of TBI 5 —is thought to reflect compromised executive control functions, which in turn undermine the ability to allocate and sustain attention. 6 Inconsistency of reaction time has been found to be a sensitive marker of persisting impairment in TBI.7-11 For example, Collins and Long 12 found that inconsistency (across trials of a reaction time task) remained impaired in brain damaged participants who had fully recovered from their other cognitive deficits, as measured by clinical neuropsychological assessment.
Within-subject inconsistency, commonly referred to as “intraindividual variability” (IIV), is frequently indexed by measuring the spread of data across trials of a reaction time task (ie, RT IIV). A relatively novel approach to investigating variability is to examine the entire RT distribution within each individual by applying an ex-Gaussian analysis. An ex-Gaussian distribution is the convolution of a normal (Gaussian) function with an exponential function and has 3 parameters: mu (Gaussian mean), sigma (Gaussian standard deviation), and tau (exponential right tail). Reaction time data typically fit ex-Gaussian functions very well because they accurately describe attentional behavior—the tendency for speeded responses to generally be normally distributed, with the addition of occasional/sporadic extremely slow responses creating positive skew (tau). These exceptionally slow responses are thought to represent brief attention lapses due to decreased efficiency of executive control processes, 6 and recent research suggests that they are the critical component being captured by conventional measures of RT IIV. 13 In comparison, mu and sigma reflect the general speed and variability of the distribution, respectively, excluding those extremely slow responses. 14
It is important to understand IIV because deficits in the executive control of attention have been found to be remediable. 15 A better understanding of whether such deficits resolve or worsen with time, and the underlying mechanisms of such deficits, would aid in treatment efforts for TBI. To date, there are no longitudinal studies of IIV in this population, and only a single cross-sectional study, which compared moderate-severe TBI patients at 5 and 10 years postinjury; here, Hetherington et al 16 found higher variability in the 5-year postinjury group than in the 10-year postinjury group.
We present here longitudinal data of RT indices from a large group of moderate-severe TBI patients with high follow-up retention over 4 time points (2, 5, 12, and 24+ months postinjury). Most longitudinal studies of TBI recovery show an asymptotic pattern of recovery within the first year of injury, 16 and until recently, it was believed that moderate-severe TBI patients achieved cognitive stability in the chronic stages of injury. 17 However, our group previously observed cognitive decline in nearly one-third of patients from 12 to 24+ months postinjury using the reliable change index 18 ; other groups have found similar declines in the later stages of injury.19-21
Given the sensitivity of IIV to persisting TBI deficits, 12 we wanted to examine whether patients would show similar such declines in the later stages of injury (ie 12 to 24+ months postinjury) or whether they might show improvement, as observed by Hetherington et al. 22 To do so, we examined conventional RT IIV and conducted an ex-Gaussian analysis. With regard to the first year postinjury, we predicted that (1) improvement of RT IIV would be observed from 2 to 5 and from 5 to 12 months, with lesser recovery from 5 to 12 months postinjury; (2) ex-Gaussian tau would also be a sensitive indicator of recovery, paralleling the pattern observed with RT IIV; and, (3) RT IIV in subacute TBI would be elevated (poorer) as compared with controls, but over time would resolve to a level consistent with healthy performance, indicative of recovery. (4) Last, as prior longitudinal studies on RT IIV in healthy older adults have shown an increase in variability with age,23,24 a fourth prediction was that poorer recovery of IIV would be observed in our older TBI patients.
Method
Participants
Participants were recruited from the inpatient Acquired Brain Injury service of the Neurorehabilitation Program at the Toronto Rehabilitation Institute in Toronto, Canada. The study received approval from the Toronto Rehabilitation Institute Research Ethics Board. Patients were eligible for inclusion if they met the following criteria: (1) acute care diagnosis of TBI; (2) posttraumatic amnesia (PTA) of 1 hour or more and/or Glasgow Coma Scale (GCS) of 12 or less either at emergency or the scene of accident and positive acute care computed tomography or magnetic resonance imaging findings; (3) age between 18 and 80 years; (4) able to follow simple commands in English based on speech language pathologist intake assessment; and, (5) competency to provide informed consent or availability of a legal decision maker. Participants were excluded on the basis of the following criteria: (1) orthopedic injuries affecting both upper extremities; (2) history of stroke; (3) history of psychotic disorder; or (4) not emerged from PTA by 6 weeks postinjury, as measured by the Galveston Orientation Amnesia Test 25 , to ensure that patients were not in PTA during the first occasion of testing. Demographic and injury characteristics (see Table 1) were obtained through review of medical records and clinical interviews (see Table 2 for neuropsychological data). At the time of the initial testing session, TBI participants were receiving rehabilitation treatment for their injuries.
Traumatic Brain Injury Sample Demographics.
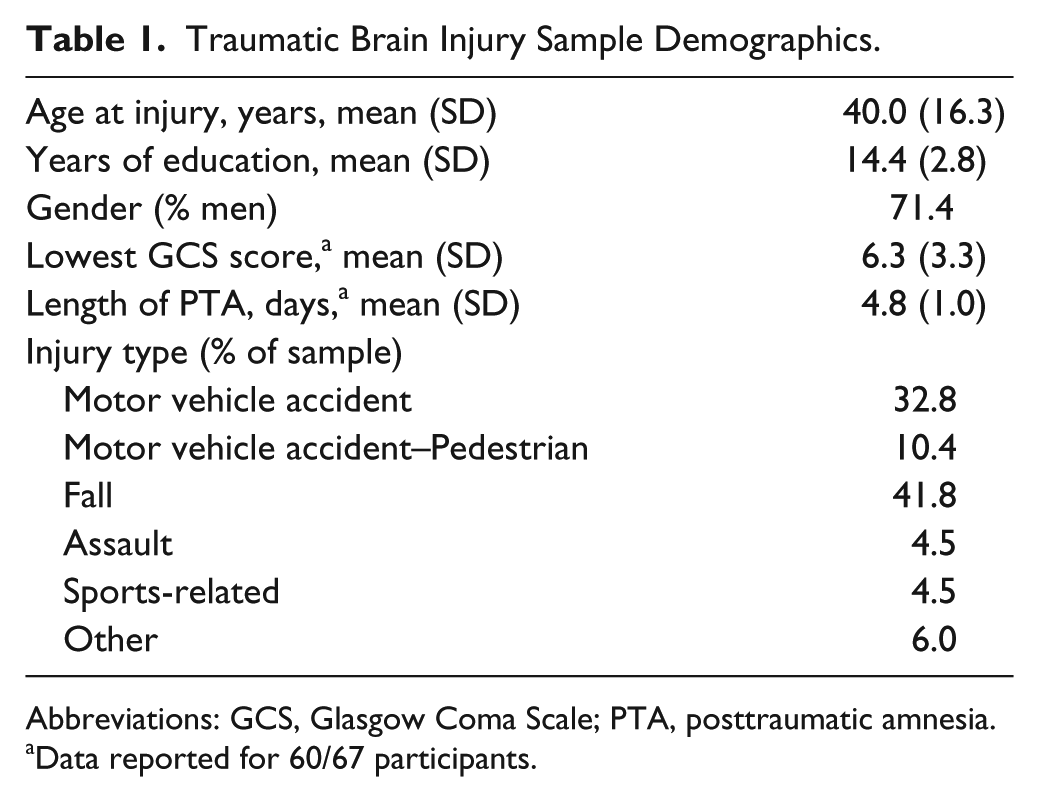
Abbreviations: GCS, Glasgow Coma Scale; PTA, posttraumatic amnesia.
Data reported for 60/67 participants.
Neuropsychological Characteristics of Traumatic Brain Injury Group at Initial Testing Session.
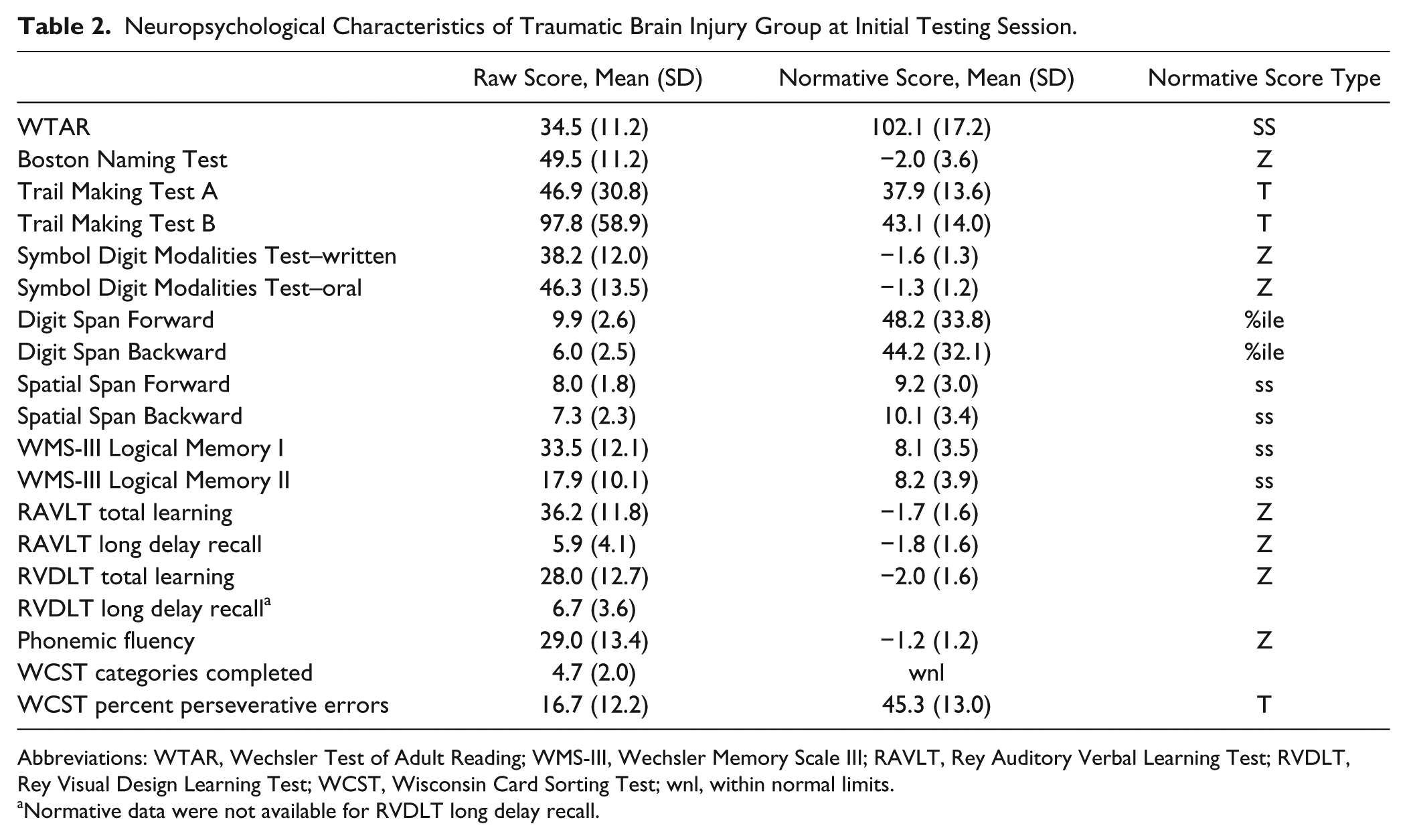
Abbreviations: WTAR, Wechsler Test of Adult Reading; WMS-III, Wechsler Memory Scale III; RAVLT, Rey Auditory Verbal Learning Test; RVDLT, Rey Visual Design Learning Test; WCST, Wisconsin Card Sorting Test; wnl, within normal limits.
Normative data were not available for RVDLT long delay recall.
The current study was a secondary analysis of a larger data set16,26 using only those data from patients who had completed all 4 time windows of assessment: 2, 5, 12, and 24+ months postinjury. Seventy of the patients in the database were eligible; of those, three were excluded because of missing data, leaving 67 moderate-severe TBI patients (Table 1).
A control group of healthy participants (n = 21) with data available at 3 time points were included in the analyses. We included these subjects in one of our analyses to provide a benchmark of any longitudinal change due to aging or test re-test practice effects.
Materials
The Sustained Attention to Response Task (SART) 27 is a computerized, go/no-go reaction time task that is a widely used sustained attention measure. In the original version of the task, participants are presented with the digits 1 to 9 in random order at a rate of one every 1.15 seconds. Each digit is presented for 250 ms followed by a 900 ms mask. The digits are presented in 1 of 5 randomly allocated font sizes to enhance the demands for numerical processing. The mask following each digit consists of a ring with a diagonal cross in the middle. Participants were told to click the left mouse button for every number except a 3, for which they must withhold their response (the “no-go” trials). The task consists of a total of 225 trials (25 of each of the 9 digits) and lasts approximately 4.3 minutes.
Data Preparation
Three versions of the data set were created—one including all raw data, one with lower bound outliers (<150 ms) removed, and a third data set containing only those lower bound outliers removed from the second data set. We removed responses less than 150 ms in the second data set based on the rationale that such responses are too fast for processing of the stimulus, making a decision, and executing a response; these were infrequent, representing 2.78% of responses. Values for removed data points were not imputed. Note that extreme upper value outliers, representing response error, were not possible because the task continuously moved forward to the next trial after 1150 ms, fixing the upper limit for reaction time. If the participant did not respond within that time, it was counted as an omission error.
Calculation of Intraindividual Variability and Examination of the Reaction Time Distribution
We employed the intraindividual coefficient of variation (ICV) and the intraindividual standard deviation (ISD), which both account for systematic mean trends in performance and tend to be highly correlated. The ICV simply involves dividing the within-person SD across trials, by the within-person mean. For calculating ISD, we followed standardized data “purification” steps in accordance with consensus from the field. 28 Individual trial RTs were regressed on trial number for each participant and the unstandardized residuals were saved. Finally, ISDs were calculated from these residual values. We also fit each participant’s data to an ex-Gaussian distribution. Ex-Gaussian parameters (mu, sigma, and tau) were computed for all participants’ SART RT distributions using the MATLAB toolkit distrib v2.3. 14
Statistical Analysis
Prior to conducting the main analyses, we examined the potential for injury severity to contribute to the effects observed in the RT data by first running correlations between Glasgow Coma Scale (GCS) and length of posttraumatic amnesia (LPTA) with the RT data from 12 months postinjury, as well as time point difference scores (2 to 12 and 2 to 24+ months) for the RT data. This preliminary analysis revealed no significant correlations for indicators of injury severity, P > .1 on all analyses, consistent with the findings of Stuss et al. 5 Thus, GCS and LPTA were not included in the main set of analyses. This may be related, in part, to the absence of patients with PTA for longer than 6 weeks, which was an exclusion criterion.
Primary analyses on all RT variables were run with the outlier removed data set, with the exception of a healthy control comparison, which necessitated that summary data be used due to missing raw data. In this case, ex-Gaussian parameters could not be estimated and ICV (without the removal of outliers) was calculated for comparison.
To address objectives 1 and 2, RT data from the SART (mean, ICV, ISD, mu, sigma, tau) for correct responses, number of responses made in less than 150 ms, error data, and cognitive performance data were separately analyzed in repeated-measures multivariate analyses of variance (MANOVA). Four time points were entered as the repeated variable—2, 5, 12, and 24+ months postinjury. Where there were significant multivariate effects, follow-up univariate analyses were performed with polynomial contrasts. We considered a response that occurs faster than 150 ms as one without intention, as it is simply too fast for someone to complete the cognitive operations required.29-31 Thus, these extremely fast responses, in the context of the SART, may represent instances of impulsivity related to deficient inhibitory control and/or automatization due to attentional disengagement. Two types of errors were included: omission, where there was an absence of response to a non-3, and commission, where a response was made on a 3. Cognitive functioning was assessed with neuropsychological tests of processing speed and executive functioning (Trails A and B, WAIS-III Digit Span Backward, WAIS-III Spatial Span Backward).
For the control comparison goal of objective 3, ICV from the SART for correct responses was analyzed in a repeated-measures analysis of variance (ANOVA) with group (TBI or control) as a between-subjects factor. Only 3 time points (2, 5, and 12 months postinjury/initial visit) were entered as the repeated variable because control data for a fourth time point was not available. Follow-up within-subject polynomial contrasts were then performed.
Finally, for our investigation of age effects (objective 4), we first applied a median split using age at time of injury yielding younger and older age groups, 17-39 years (n = 33) and 40-79 years (n = 34), respectively. We then performed a repeated-measures MANOVA using age group (younger and older) as a between-subjects factor.
Results
RT Distribution and Variability
SART Correct RT (Outliers Removed)
A significant multivariate effect was found for time using Pillai’s trace, V = .59, F(18, 49) = 3.88, P < .001,
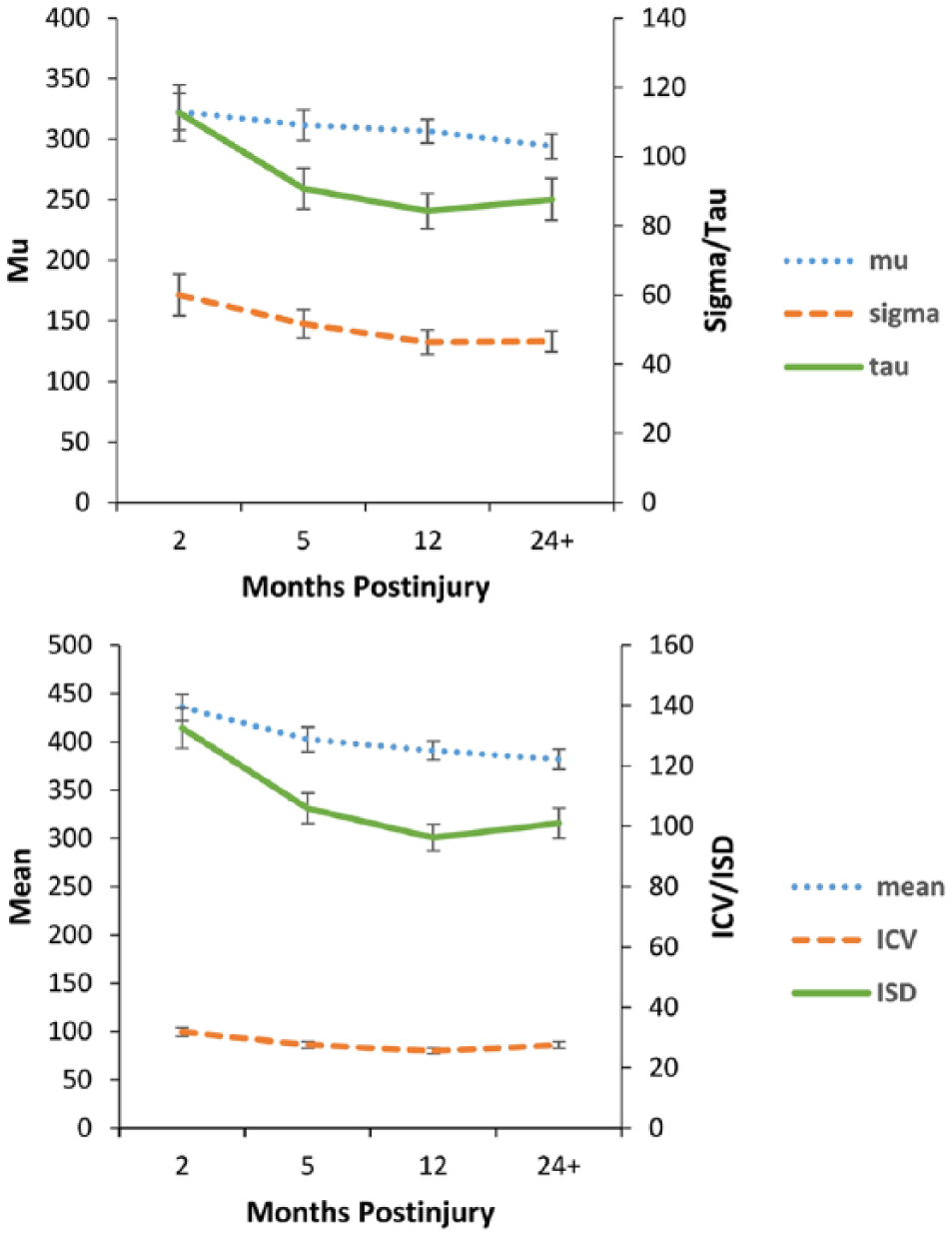
Traumatic brain injury recovery over time—reaction time (RT) indices of the Sustained Attention to Response Task (outliers removed). Error bars represent standard error
Responses Below 150 ms
A significant effect was found using Pillai’s trace for time, V = .180, F(3, 64) = 4.69, P = .005,
SART Correct RT (Full Data Set)
A significant interaction was found using Pillai’s trace for time × group, V = .12, F(2, 86) = 5.70, P = .005,
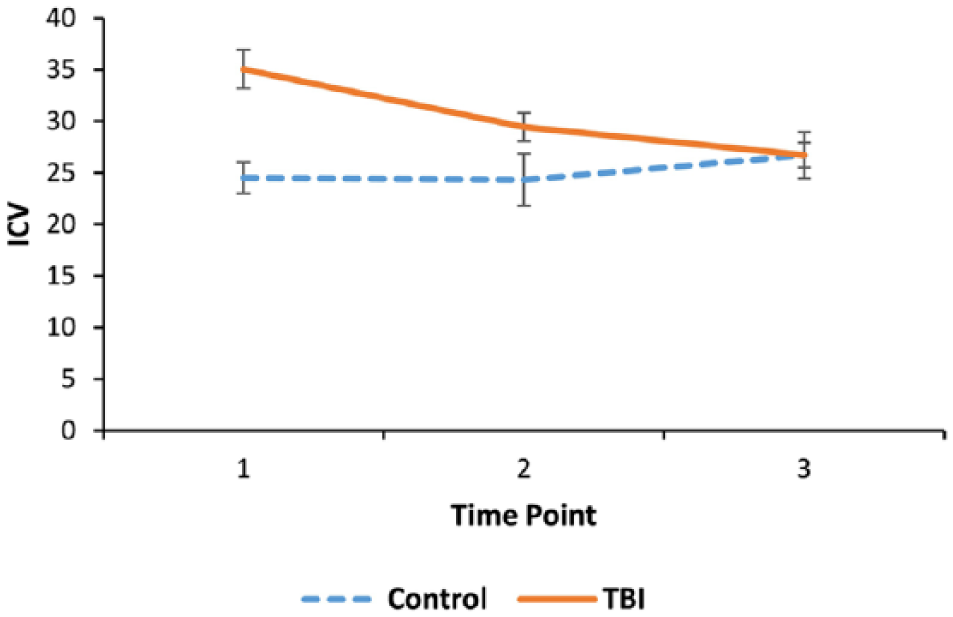
Traumatic brain injury recovery over time compared with controls—intraindividual coefficient of variation (ICV) of the Sustained Attention to Response Task (full data set). Error bars represent standard error
SART Errors (Omission and Commission)
A significant multivariate effect was found using Pillai’s trace for time, V = .34, F(6, 54) = 4.71, P = .001,
Reaction Time and Error Performance From the Sustained Attention to Response Task (Outliers Removed). a
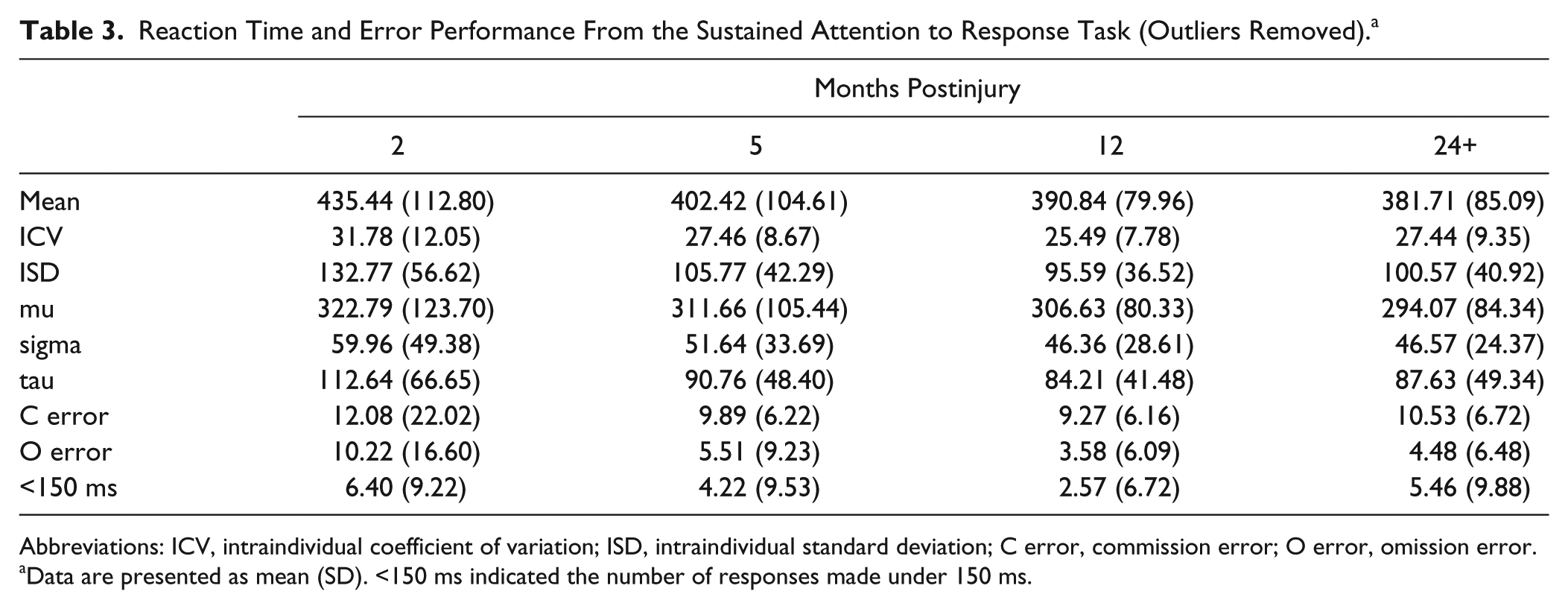
Abbreviations: ICV, intraindividual coefficient of variation; ISD, intraindividual standard deviation; C error, commission error; O error, omission error.
Data are presented as mean (SD). <150 ms indicated the number of responses made under 150 ms.
Reaction Time and Error Performance From the Sustained Attention to Response Task—Control Comparison. a
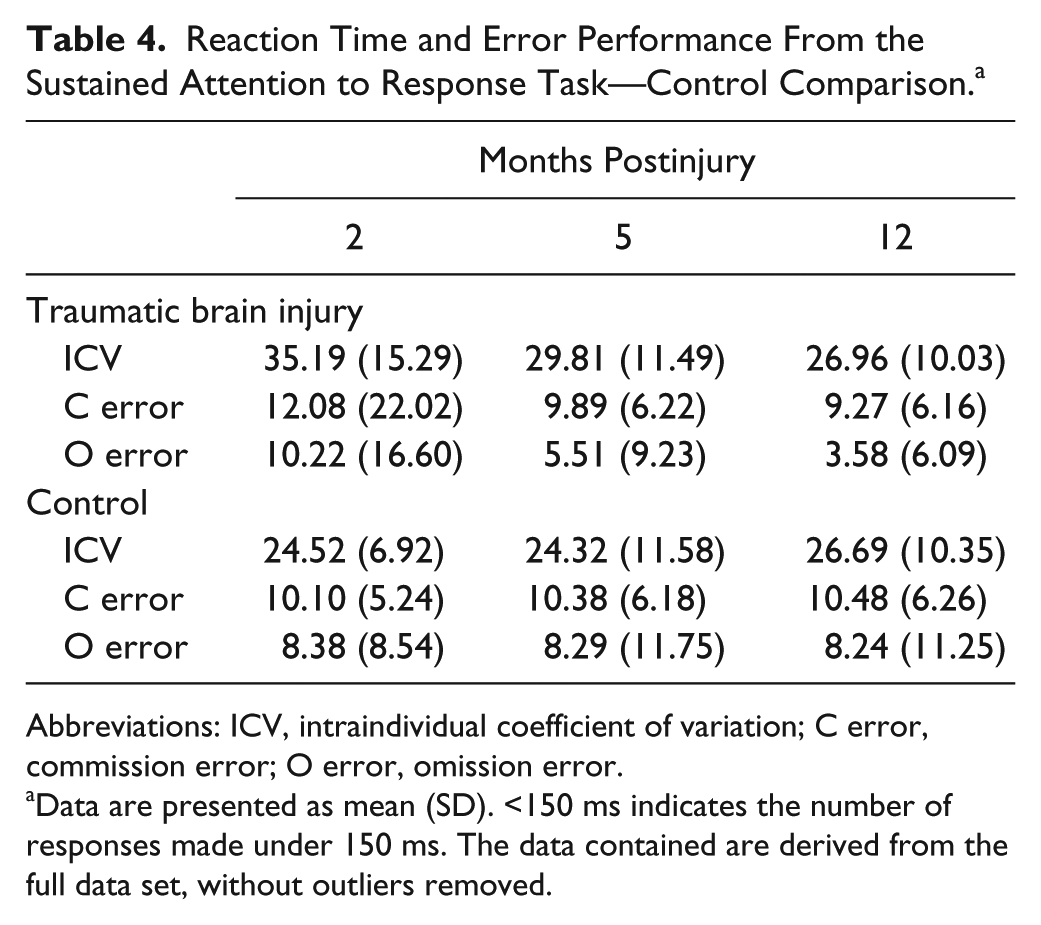
Abbreviations: ICV, intraindividual coefficient of variation; C error, commission error; O error, omission error.
Data are presented as mean (SD). <150 ms indicates the number of responses made under 150 ms. The data contained are derived from the full data set, without outliers removed.
Age Effects
SART Correct RT (Outliers Removed)
The analysis yielded no significant multivariate interaction between age group and time point. We then conducted separate MANOVAs with younger and older age groups individually. Significant multivariate effects were found for time using Pillai’s trace in both the younger, V = .84, F(18, 15) = 4.49, P = .003,
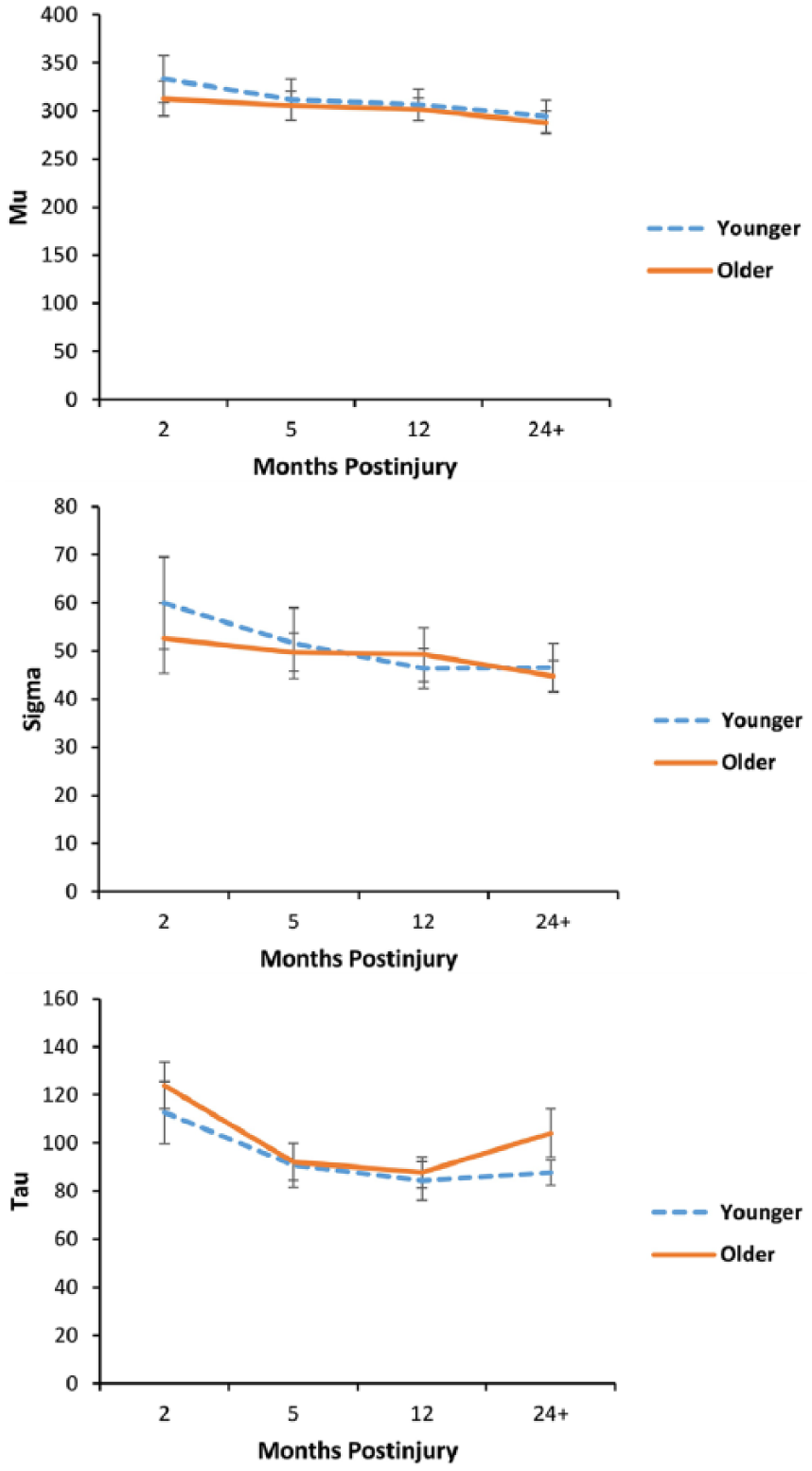
Traumatic brain injury recovery over time as a function of age—ex-Gaussian parameters of the Sustained Attention to Response Task (outliers removed). Error bars represent standard error
Cognitive Change
For the cognitive variables, a significant multivariate effect was found using Pillai’s trace for time, V = .55, F(12, 45) = 4.51, P < .001,
Discussion
The current study examined longitudinal, within-subject changes in RT distributional indices of SART performance after moderate-severe TBI in the subacute to chronic stages of injury. We found specific patterns of recovery in the RT distribution profiles of TBI participants from 2 to 12 months postinjury when patients were compared to controls. Individuals with TBI displayed elevations (ie, impairments) in ICV following injury, but recovery of RT variability was clearly visible within the first several months to a level similar to the control group by 1 year. Recovery, as gauged by RT IIV, likely reflects neural changes, as implied by previous research showing that improved brain signal metrics (ie, multiscale entropy) accompany more consistent responding. 32
Trajectory of Recovery in RT Performance
The results displayed a linear effect for mean and sigma, indicating that from 2 months to 24+ months postinjury, individuals with TBI improved on speed and variability across the normal portion of the distribution. There was no significant change in mu, however, suggesting that an effect of mean RT was only present due to combined influences of tau with mu. The reason behind the linear improvement of sigma is unclear, though one possibility is that it reflects a unique aspect of neural recovery. For example, changes in sigma may be related to improvements in general signal transmission, whereas tau may be indicative of executive control network efficiency and integration.
All other measures of variability (ie, ICV, ISD, and tau) showed a quadratic effect over time, suggesting an initial decrease in RT variability early on in recovery followed by a later increase by 24+ months postinjury. Examination of the pattern of RT performance over time indicates that traditional measures of IIV (ie, ICV and ISD) tracked with ex-Gaussian tau. The correspondence between ex-Gaussian tau and traditional measures of variability at each time point, along with the finding that sigma (a measure of variability excluding extremely slow responses) did not show the same pattern, provides evidence that ICV and ISD largely reflect sporadic exceptionally slow responses that make up the positively skewed portion of the distribution. The hypothesis that deficient executive control is responsible for brief attention lapses that manifest as sporadic, extremely slow responses has been proposed previously in the aging literature,6,13 in research on attention deficit hyperactivity disorder, 33 and hinted at in TBI. 8
The SART encourages an automatic mode of responding, requiring individuals to endogenously engage attention (inhibitory control) in order to break out of automatic pilot and withhold no-go responses. Deficient attentional deployment can lead to inconsistent responding as we have discussed, but it can also lead to impulsive “too quick” responses. Extremely fast responses evinced a longitudinal pattern mirroring the findings for RT IIV—a quadratic effect with the instances of “too quick” reactions decreasing over time early in recovery, but then increasing in the chronic stage.
The present findings are congruent with previous literature showing initial elevations in RT IIV for TBI patients compared to healthy controls, 5 and that variability decreases to healthy levels within a year of injury. 34 This study for the first time longitudinally characterizes the longer term course of RT IIV, showing deterioration from 12 to 24+ months postinjury. The current findings are discrepant from those of Hetherington et al, 22 who found improvement from 5 to 10 years postinjury in their cross-sectional study. This disparity may be due to differences in design or time-lines between the 2 studies.
The neuropsychological data also demonstrated similar findings. Here, a measure of processing speed showed linear improvement over time, whereas cognitive flexibility initially improved, but then plateaued by session 4. Aspects of executive control measured on neuropsychological testing mirrored the trajectory of recovery observed in reaction time variability; however, performance on other neuropsychological tasks (eg, working memory) yielded a different pattern, suggesting less mechanistic overlap in those cognitive processes. 13 RT distribution indices appear to be more sensitive to momentary attentional disruption and recovery of executive control than typically measured commission errors or conventional neuropsychological instruments. Further research is required to confirm this postulation. The present study provides further evidence that moderate-severe TBI leads to a decreased ability to maintain attention on task, and uniquely shows that attentional efficiency has a specific quadratic trajectory of recovery from subacute to late chronic stages.
Influence of Age
Exploration of age effects revealed linear trends in ICV and tau, and a quadratic function for sigma in the younger adults. In contrast, individuals in the older age group showed quadratic effects for mean, ICV, ISD, and tau (mu and sigma were not significant). The predominance of a quadratic pattern of RT performance over the recovery period for the older group suggests that these individuals were less able to maintain recovery benefits into the chronic stage postinjury. These findings require stronger support from a TBI aging study capable of detecting an age by time interaction. This was not possible with the current data because we did not have adequate numbers of participants to represent meaningful older adult age groups.
Reaction time IIV is known to increase from young adulthood into old age, demonstrated longitudinally,23,24 and inferred through cross-sectional age differences in large prospective cohort studies.35,36 It is unclear whether the current data characterize the start of the (normative) aging trajectory or, more insidiously, the synergistic effects of aging and early neurodegeneration. Contemporary research on the course of recovery for TBI has shown that there is a period of neural stabilization (ie, resolution of edema, development of gliosis) and behavioral improvement occurring in the acute and subacute stages postinjury, but moderate-severe TBI patients may experience post-recovery neural and cognitive decline in the later stages21,37,38; these changes occur independent of age, but may be exacerbated by it. Further research is required to determine whether the RT IIV decrements observed in the chronic stage of TBI recovery represent an accelerated aging process.
Conclusions
The present study examined RT indices longitudinally from subacute to chronic stages of recovery from TBI and found that individuals improved in the first year of injury, but then showed more variable performance, including increases in sporadic, extremely slow responses thereafter. The frequency of extremely fast responses, possibly indicative of impulsivity, paralleled the changes observed in RT performance. These findings are compatible with a small number of studies that show deterioration in the chronic stages of moderate-severe TBI. Further research is required to determine whether reduced executive control capacity in chronic TBI is due to combined effects of aging and an insidious neurodegenerative process.
Given that elevated RT variability has been observed even when other neuropsychological impairments are fully recovered, 12 executive control deficits may be a hidden and worsening impairment of patients with moderate-severe TBI. The results suggest, at least preliminarily, that patients with TBI, and particularly older adults, should be assessed for impairments in consistency/executive control. This would allow for consideration of interventions that ameliorate executive control of attention 15 and may serve to increase functioning in this vulnerable population.
Footnotes
Acknowledgements
We thank Wendy Gu, Shafaq Shereen Khan, and Caitlin Dao for help conducting literature searches and data entry. Brandon Vasquez’s primary affiliation is now Neuropsychology and Cognitive Health, Baycrest Health Sciences. Jennifer Tomaszczyk’s primary affiliation is now the Krembil Research Institute of the University Health Network.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from Canada Research Chairs (950-211602 & 950-230647), Canadian Institutes of Health Research (MOP 86704), Physicians Services Inc. Foundation (12-43), and Ontario Neurotrauma Foundation (2007517).