
Abstract
Background. While older adults are able to attend to goal-relevant information, the capacity to ignore irrelevant or distracting information declines with advancing age. This decline in selective attention has been associated with poor modulation of brain activity in sensory cortices by anterior brain regions implicated in cognitive control. Objective. Here we investigated whether participation in an executive control training program would result in improved selective attention and associated functional brain changes in a sample of healthy older adults (N = 24, age 60-85 years). Methods. Participants were enrolled in a goal-oriented attentional self-regulation (GOALS) program (n = 11) or a brain health education workshop as an active control condition (n = 13). All participants performed a working memory task requiring attention to or suppression of visual stimuli based on goal-relevance during functional magnetic resonance imaging. Results. We observed a pattern of enhanced activity in right frontal, parietal and temporal brain regions from pre- to posttraining in the GOALS intervention group, which predicted the selectivity of subsequent memory for goal-relevant stimuli. Conclusions. Executive control training in older adults alters functional activity in brain regions associated with attentional control, and selectively predicts behavioral outcome.
Introduction
We are constantly bombarded by multiple channels of information in our everyday lives. From the incessant ping of text messages to the continuous cycle of news and entertainment, and the constant din of our increasingly urban and wired world, our attention is divided in myriad ways. To maintain adaptive functioning, it is necessary to stream this information into that which is relevant for the task at hand, and that which is irrelevant and distracting. As we age, this capacity to stream information based on task-relevance declines1 -4 and older adults show a decline in the capacity to inhibit attention to non–goal relevant or distracting information. 5 At the level of the brain, this has been characterized as an inability to suppress neural representations of distracting stimuli, although enhancement of neural response to relevant stimuli appears to be preserved.6,7 One model of age-related decline in selective, or goal-directed, attention suggests that poor top-down modulation of sensory cortices (eg, visual association areas) by brain regions implicated in cognitive control (eg, prefrontal cortex [PFC]) may lead to the processing of goal-irrelevant, or distracting, information.6,8 -10 Furthermore, these changes have implications for real-world function as poor goal-directed attention is associated with reduced capacity in activities of daily life and loss of independence in aging and brain disease. 11
In this context, rehabilitative efforts to enhance executive control, aimed at improving real-world outcomes, provide a critical avenue of research in aging. Earlier studies have investigated the impact of executive control training in normal aging with positive outcomes.12,13 Goal Management Training (GMT) 14 is a theory-driven intervention aimed at enhancing goal-directed behavior. It emphasizes strategies to reengage endogenous attention processes, as well as teaching problem-solving techniques to enhance goal-directed attention capacity. GMT has been associated with improvements in psychosocial adjustment to executive dysfunction and increased goal-directed behavior in older adults.12,13 An adapted version of the GMT protocol, Goal-Oriented Attention Regulation (GOALS), 15 targeted at improving executive control by training attentional processes, emphasizes strategies for suppressing external and internal distractions and promotes activities to foster the transfer of training gains into everyday functional settings. GOALS has been associated with improvements in neuropsychological functioning in patients with acquired brain injury. 15 Consistent with a brain-based model of goal-directed attention, 6 we recently demonstrated that training-related gains in a sample of acquired brain injury subjects following GOALS participation were associated with enhanced goal-directed modulation of sensory cortices by frontal brain regions. 16
This study aims to extend and add to previous research conducted with GOALS training 15 and GMT12,13 in older adults by investigating the potential neural mechanisms associated with executive control training in older adults. In the current study, we used functional magnetic resonance imaging (fMRI) and a task that demands selective information processing 16 to investigate differential functional brain changes following GOALS training in a sample of cognitively normal older adults. We directly contrast GOALS training with a closely matched, psychoeducational control intervention. Our hypotheses align with previous findings,16,17 suggesting that prefrontal brain regions modulate activity in visual processing regions in a goal-directed manner. Specifically, we hypothesized that GOALS training would be associated with increased activation of prefrontal and visual association cortices during tasks requiring selective (ie, goal-directed) processing of visual stimuli. Furthermore, these changes would be greater for the selective attention task relative to a nonselective control task. To investigate these training-related brain changes we used a multi-variate analysis method: partial least squares (PLS). 18 PLS identifies patterns of covarying functional brain activity that reliably differentiate experimental conditions and/or groups, making it an ideal approach to investigate training-related changes in this spatially distributed model of executive control. Provided that the strategy that is focused on in GOALS is one that is aimed at improving suppression of distracting information, we were also interested in examining whether differential brain activity observed posttraining during selective information processing, predicts subsequent memory for relevant relative to nonrelevant information. To examine this possibility, we identified brain activity patterns that maximally differentiated the selective from nonselective attention conditions. Subject-wise measures of this activation pattern were used to predict subsequent memory for attended versus ignored stimuli.
Materials and Methods
Participants
Thirty-four healthy older adults, aged 60 to 85 years, were recruited into the study after providing written informed consent in accordance with a protocol approved by the University of California, Berkeley Committee for the Protection of Human Subjects. Thirty participants (age range: 60-85 years, 18 females) completed the pre- and postintervention assessments and were included in the current study. Four participants did not complete the full training protocol owing to altered time and scheduling commitments that occurred over the course of training. Of these, 11 (age range: 61-70 years; 3 males; mean years of education: 17.3) in the GOALS group and 13 (age range: 62-75 years; 6 males; average years of education: 17.09) in the control group had artifact-free fMRI data for both pre- and post-MRI sessions. All 6 participants excluded from the analysis had motion artifacts that were beyond minimum thresholds (2 mm in either rotation or displacement) or scanner artifacts (eg, spiking) that could not be resolved through preprocessing methods in either the pre- or postscan fMRI data. All remaining participants (n = 24) were right-handed and had normal, or corrected-to-normal, vision. There were no significant differences between the 2 groups in age (GOALS mean = 65.9 years, SD = 5.20 years; Brain Health Education Group [BHE] mean = 69.36 years, SD = 5.20 years), t(22) = −1.64, P = .72, or years of education (GOALS mean = 17.30 years, SD = 1.83 years; BHE mean = 17.09 years, SD = 2.34 years), t(22) = 0.23, P = .99.
All participants were screened for currently active or untreated medical or psychiatric conditions, and past history of neurological (e.g. head injury involving loss of consciousness) or psychiatric diagnosis (eg, schizophrenia, currently active major depression). Participants currently taking medication with known impacts on cogntion (eg, benzodiazepines, methylphenidate) were also excluded. All decisions regarding medical exclusions were overseen by the lead neurologist on the project (M.D.). Participants were normal on cognitive screen (ie, no score less than 1.5 standard deviations below expected performance in more than one cognitive domain for neuropsychological assessments of memory, concentration, verbal fluency and visuospatial function). A complete neuropsychological evaluation was not available for 1 participant; however, their Mini-Mental State Examination (MMSE) 19 score was 28. Table 1 provides a summary of domain-specific baseline performance on neuropsychological tests. Detection of reliable associations between functional brain measures and standard neuropsychological test performance in a healthy aging cohort would require significantly larger sample sizes than would be feasible for the current study (see Yarkoni 20 for a discussion of statistical challenges in detecting brain-behavior correlations). As a result, we have focused here on investigating associations with the in-scanner task and related subsequent memory measures. The impact of GOALS training on neurocognitive and functional outcomes are the subject of another study (G. R. Turner et al, 2017, unpublished data).
Average z Scores for Domain-Specific Baseline Scores Based on Standardized Neuropsychological Tests for Goal-Oriented Attentional Self-Regulation Training Group (GOALS) and Brain Health Education Group (BHE). a
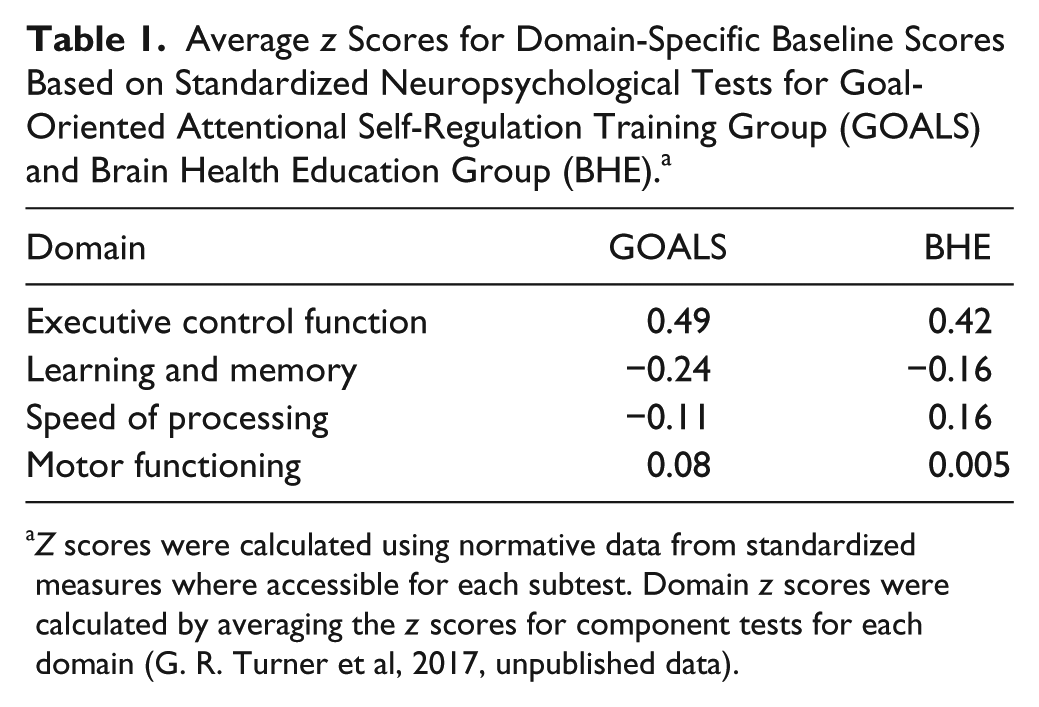
Z scores were calculated using normative data from standardized measures where accessible for each subtest. Domain z scores were calculated by averaging the z scores for component tests for each domain (G. R. Turner et al, 2017, unpublished data).
Interventions
Participants were randomly assigned to 1 of 2 intervention conditions: (a) training in goal-oriented attentional regulation (GOALS training) 15 or (b) a comparison educational activity (a Brain Health Education program, BHE), which served as the active control group. Participants were blinded as to study design and predictions with regard to the intervention protocols. Pre- and posttraining assessments were conducted by research personnel blinded to the condition assignment of the participants. The GOALS training protocol was based on the adaptations from original GMT protocol,12,14,21 as well as principles highlighted in other attention, mindfulness, and problem-solving interventions.22 -26 Both the GOALS and BHE protocols involved 10 two-hour sessions of group-based training, 3 individual 1-hour training sessions, and 20 hours of home practice over 5 weeks. The protocols were delivered in a small group format with 3 to 5 participants and 2 instructors per group. To ensure consistency of administration, intervention manuals were written for instructors and participants. Clinicians (occupational therapists, neuropsychology resident) were trained in administering both interventions and were supervised by neuropsychologists (G.T., T.N.A.).
GOALS Protocol
Full details of the GOALS protocol may be found in Novakovic-Agopian et al 15 and are briefly summarized here. Mindfulness-based attentional regulation training was emphasized in the first half of the GOALS intervention. Goal management strategies applied to participant-defined goals were emphasized in the second half of the training protocol. Initial group sessions focused on incorporating strategies for reducing distractibility, emphasizing principles of applied mindfulness to redirect cognitive processes toward goal-relevant activities in the context of increasing levels of distraction. Strategies included identifying the primary goal, identifying information as either relevant or nonrelevant, and working to selectively maintain relevant information while letting go of nonrelevant information. Introductory training via in-class exercises began with a brief applied mindfulness exercise as a first step in refocusing on tasks at hand. This was applied to progressively more challenging situations, including maintaining increasing amounts of information in mind during distractions. These exercises were supported by homework assignments, including daily practice with mindfulness. Homework then progressively emphasized application of these skills to challenging situations in each individual’s daily life. To assist with application in daily life situations, participants were trained in applying a single phrase meta-cognitive strategy (“Stop-Relax-Refocus”) to stop activity when distracted and/or overwhelmed, relax and then refocus attention on the current, primary goal.
The second phase of the GOALS training protocol emphasized learning strategies for accomplishing individually salient, self-generated complex goals. In order to emphasize active application of these strategies, participants were asked to identify feasible and realistic functional goals as individual projects (eg, planning a meal, learning to use an organizer and follow a schedule) and group projects (eg, planning a group outing or presentation), and were then trained to apply attention-regulation and goal-management strategies on the functional task(s) of their choice.
Brain Health Education Protocol
The BHE control intervention was designed to be an engaging education protocol that was closely matched with the GOALS protocol for in-class and homework time as well as therapist interactions and group participation. All sessions were interactive (see Supplemental Table S1 for a list of session topics) and the therapists were encouraged to explain the relevance of the learning to the participant’s everyday lives. All sessions required 1 to 2 hours of homework (reviewing an article, DVD viewing, formulating a question for the subsequent discussion section). DVDs were provided and included educational lectures in neuroscience topics from the Great Courses Company (http://www.thegreatcourses.com). Session topics included “Brain Plasticity,” Emotion and Executive Function, and Sleep and Dreaming (see Supplemental Table S1 for a full list of topics). Reading assignments included popular science articles from the ScienceDaily series (eg, Mild Memory Loss Is Not a Part of Normal Aging; Eating Berries May Activate the Brain’s Natural Housekeeper for Healthy Aging; Distinguishing “Senior Moments” from Alzheimer’s).
Each session began with a discussion of the reading and the DVD episode. One participant was selected to introduce their question and lead a discussion, moderated by the therapist. Homework discussions lasted approximately 20 minutes, followed by a 10-minute review of material from the previous session, which included quizzes and “What does this mean to me?” elements to encourage deeper understanding and active engagement with the in-class and homework materials. The review was followed by a discussion of the current session topic. All participants were provided with review handouts at the end of each session. Finally, to encourage active learning, sessions also included hands-on exercises such as filling out self-awareness scales regarding diet, exercise, or sleep patterns and these were discussed among group members. The same trainers conducted both intervention groups.
Study Design
Participants were randomly assigned to either the GOALS or BHE training groups. Both groups completed baseline neuropsychological, fMRI and structural MRI assessments before they began the intervention and at the end of the 5-week training program.
Cognitive Task (fMRI)
To assess brain functioning associated with selective attention demands pre- and posttraining, we used a face/scene delayed matching task 16 (see Figure 1). In all task conditions, participants viewed a series of images composed of 2 categories (faces and scenes) interleaved in a pseudo-randomized order and presented sequentially for 500 ms with an interstimulus jitter of 3, 5, or 7 seconds. Perceptual information was matched across four behavioral conditions. In the baseline condition (Categorize) participants were asked to categorize each stimulus as a face or a scene. In the selective attention conditions (Scenes and Faces), participants were instructed to selectively attend to relevant images in one stimulus category (eg, images of scenes in the scene-relevant condition) while suppressing attention to images from the irrelevant category (eg, images of scenes in the face-relevant condition). Participants were required to hold in-mind relevant stimuli and indicate whether the current stimulus matched the stimulus viewed one trial back—in the relevant stimulus stream. These selective working memory conditions require selective attention to goal-relevant information and selective suppression of goal-irrelevant information.
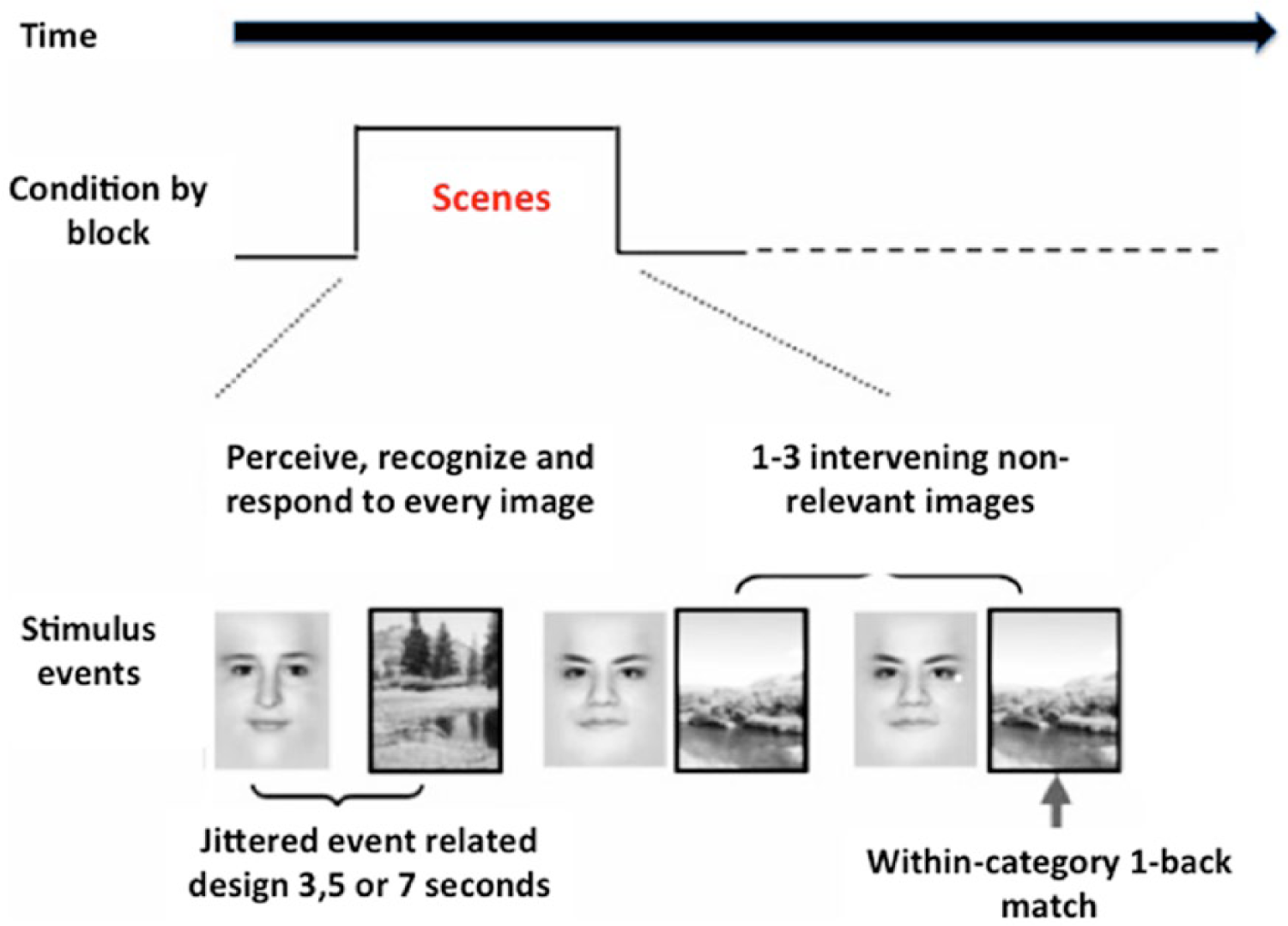
Visual working memory task performed during functional magneic resonance imaging (fMRI) acquisition. Participants viewed a series of images composed of 2 categories (Faces and Scenes). Participants were instructed to selectively attend and hold in mind images from one stimulus category. In the condition depicted here, scenes were task relevant, while faces were task irrelevant.
Task performance required identification of one-back matches within the relevant category (Scenes/Faces) by 1 of 2 button-presses indicating whether the current image was a “match” or “nonmatch” to the preceding image from the relevant category. Images in the nonrelevant stream were always labeled as “nonmatch.” To successfully complete the task, participants had to attend to relevant images and hold these in mind while suppressing distracting (ie, nonrelevant) images. A fourth condition (“Both”) required participants to attend to both stimulus categories and identify one-back matches. This non-selective condition was not the focus of current investigation and is not discussed further.
In each task block (Faces, Scenes, Categorize), 20 images (10 faces and 10 scenes) were presented sequentially. Jittering and image category orders were balanced across condition blocks and counterbalanced across participants. Five blocks of each experimental condition were presented during the session, resulting in a sample of 100 stimulus events per condition. Condition order within runs was counterbalanced over the course of the scanning session. Four alternate sets of stimuli were generated for use in multiple sessions, and set order was permuted across subjects.
Functional Magnetic Resonance Imaging
Imaging was performed using a 3-T Siemens Magnetom Trio whole-body magnetic resonance scanner with a transmit-receive 12-channel quadrature birdcage head coil at the Henry H. Wheeler Jr Brain Imaging Center at the University of California, Berkeley. A T1-weighted magnetization-prepared rapid-acquisition gradient echo (MPRAGE) was acquired for each subject for characterization of structural anatomy. For each task block, 114 whole-brain, T2-weighted echo planar images were acquired (slice thickness, 5mm; 0.5 mm skip; 18 slices; repetition time = 1000 ms; echo time = 27 ms; flip angle = 62; matrix, 64 × 64 axial field of view). The echo-planar acquisition parameters resulted in incomplete coverage for the most posterior aspect of the inferior temporal lobe, resulting in inadequate coverage of the fusiform face area. As we were unable to measure blood oxygen–level dependent (BOLD) signal in this region reliably across participants, neuroimaging and subsequent memory analyses are limited to the “Scenes-relevant” selective attention condition.
Subsequent Memory
Approximately 5 minutes after conclusion of scanning (at both time points), participants performed a recognition memory test in which they were presented with 120 images, including 60 target (scene), 60 distractor (face), and 30 novel (15 scene/face) stimuli. Images were displayed one at a time on a computer monitor, and participants indicated their level of recognition on a 4-point scale: 1 = definitely new; 2 = probably new; 3 = probably old; 4= definitely old. We obtained confidence ratings for stimuli that were goal relevant (scene images in the “Scenes” condition) and nonrelevant (scene images in the “Faces” condition).
Data Analysis
Cognitive Task Analysis
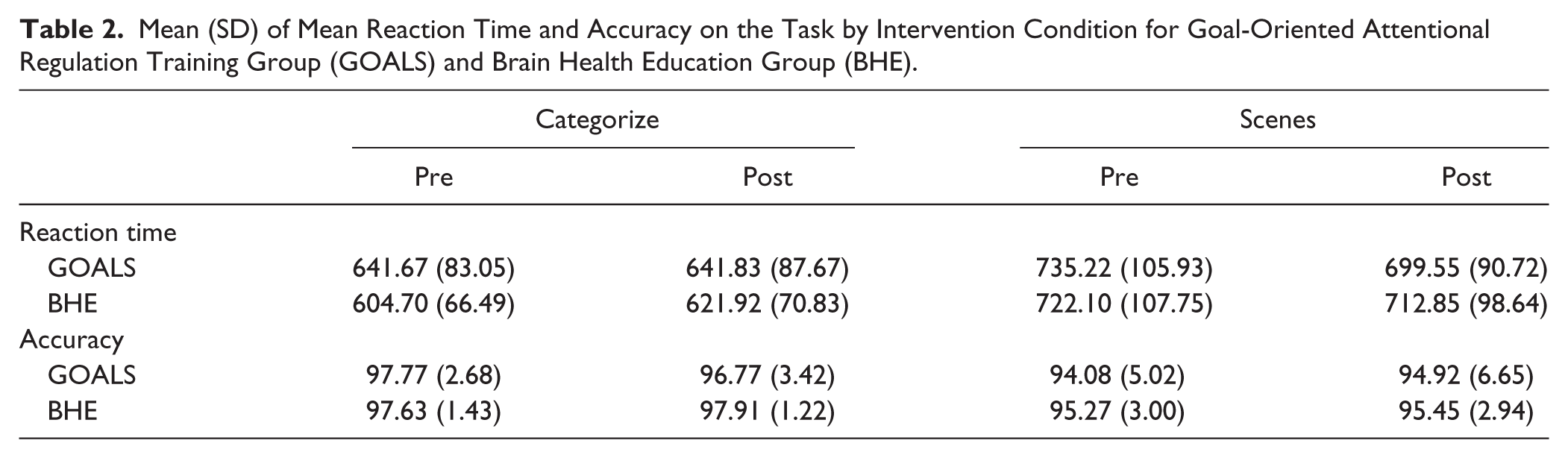
Mean reaction time (RT) for hits and overall percent accuracy for the Categorize and Scenes were submitted to a mixed analysis of variance (ANOVA), with group (GOALS, BHE) as a between-subject factor and time (pre- and post-) as a within-subject factor. Table 2 provides means and standard deviations for RT and percent accuracy for both these conditions.
Mean (SD) of Mean Reaction Time and Accuracy on the Task by Intervention Condition for Goal-Oriented Attentional Regulation Training Group (GOALS) and Brain Health Education Group (BHE).
fMRI Task Analysis
Functional data were preprocessed with Analysis of Functional Neuroimages (AFNI). 27 Images were corrected for slice timing differences and head motion across the run by coregistering to the eighth TR of the first run in each session. The data were coregistered across sessions within participants first and then into MNI space 28 and spatially smoothed within a whole-brain mask using a Gaussian kernel with a full width at half maximum of 6 mm and resampled to a voxel size of 3 mm3.
Whole-brain fMRI analyses were conducted using PLS, 18 a multivariate analysis technique that identifies whole-brain patterns of activity related to the experimental design (task-PLS). This method is similar to principal component analysis, in that it identifies a set of principal components or “latent variables” (LVs) that optimally capture the covariance between 2 sets of measurements. With respect to the current investigation, PLS has several advantages over univariate analytical methods. First, our neuromodulatory account of goal-directed attention implicates distributed brain changes including both anterior and posterior cortices involved in control and perceptual processing. 10 Furthermore, previous research suggests that goal-directed control of attention is an emergent property of interactions among networks of distributed brain regions. 9 PLS uses a data-driven approach to identify covarying patterns of brain activation changes that are reliably associated with the task design. A further advantage of PLS is that decomposition and associated resampling techniques consider all voxels simultaneously, thus avoiding the problem of multiple statistical comparisons. In task-PLS, each LV identifies a pattern of brain regions that, as a whole, maximally relate to task and/or group contrasts. Each brain voxel has a weight, referred to as a salience, which indicates how strongly that voxel contributes to the pattern represented in the LV. The significance of each LV was determined with permutation testing, 29 using 500 permutations. In addition, the reliability of each subject’s contribution to a particular LV was tested by submitting all saliences to a bootstrap estimation of the standard errors (SEs), 30 using 100 bootstraps. Peak voxels with a salience/SE ratio 3.0 (P < .001) were considered to be reliable. Clusters containing at least 10 reliable contiguous voxels were extracted, with a local maximum defined as the voxel with a salience/SE ratio higher than any other voxel in a 2-cm cube centered on that voxel (the minimum distance between peaks was 10 mm). A 10-voxel cluster-size threshold was selected as a conservative threshold without excluding significant activations in smaller brain regions where the hemodynamic response is more variable across individuals.31,32 Finally, to obtain summary measures of each participant’s expression of each LV pattern, we calculated “brain scores” by multiplying each voxel’s salience by the BOLD signal in the voxel, and summing over all brain voxels for each participant in each condition. These brain scores were then mean-centered (using the grand mean across all participants) and confidence intervals (95%) for the mean brain scores in each condition were calculated from the bootstrap. 18 To specifically examine the effects of intervention (GOALS, BHE) on functional brain activity during selective attention, we included the baseline Categorize condition and Scenes-relevant condition, which were perceptually matched and differed only in attention and memory demands (see Figure 1).
Subsequent Memory Analysis
Using the average confidence ratings for relevant and irrelevant scene stimuli, we calculated a D-prime index for recognition posttraining. The D-prime index reflects the relative confidence in recall of an attended versus an ignored stimulus, a marker of goal-directed attention. Higher D-prime values represent better post-test recognition of attended stimuli. We next examined the relationship between each participant’s subsequent memory for attended versus ignored stimuli in the scanner task and the degree to which they expressed the pattern of enhanced functional engagement identified by the LV (ie, the individual brain scores, Figure 2) postintervention. We computed a priori, single-tailed correlations between brain scores corresponding to the Scenes condition and D-prime values reflecting confidence in recall of attended versus ignored scene stimuli.
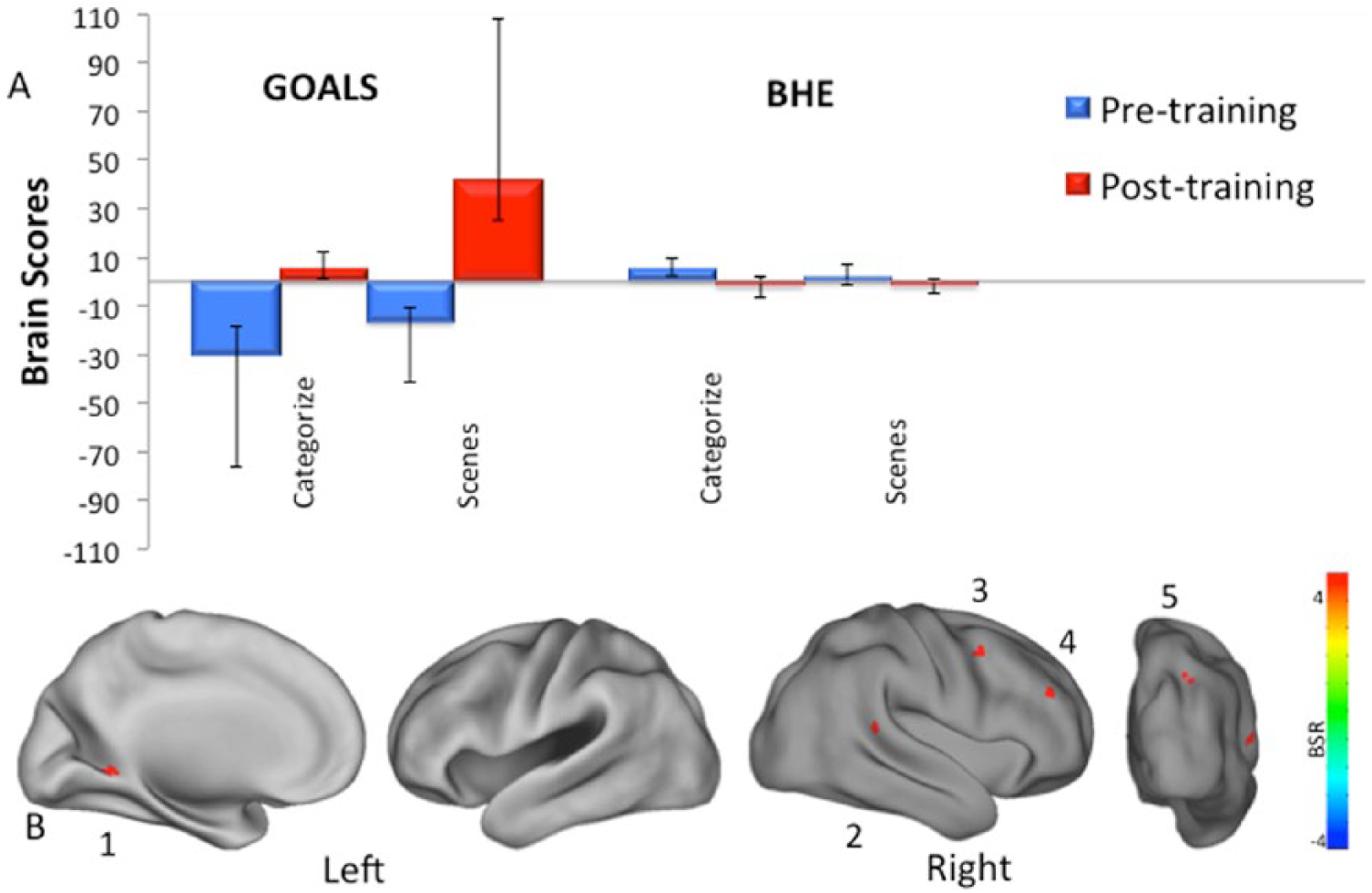
(Panel A) Latent variable (LV) 1: Brain scores represent the degree to which each participant expresses the neural pattern seen in panel B. The bars represent the average brain score across participants in a group by condition. Error bars represent 95% confidence intervals for the mean-centered brain scores for each group by condition. (Panel B) Brain regions reliably demonstrating the pattern from panel A. Brain activity is projected onto a cortical surface map using AFNI SUMA27. Regions positively reflecting the LV pattern: (1) left parahippocampal gyrus, (2) right temporal parietal junction, (3) right middle frontal gyrus, (4) right superior frontal gyrus, and (5) right precuneus.
Results
Cognitive Task Performance
Categorize Condition
On measures of RT, there was no significant main effect of time, F(1, 22) = 0.65, P = .43,
Select Scenes Condition
On measures of RT, there were no significant main effects of time, F(1, 22) = 2, P = .17,
fMRI Data Analysis
PLS Analyses
One significant LV (P < .001) was identified, reflecting a pattern of functional brain response that is maximally related to the experimental design, which included 3 factors: Task condition (Categorize and Scenes), Time (pre- and posttraining), and Group (GOALS and BHE). This LV represents a significant 3-way interaction (Figure 2A). Specifically, a pattern of increased brain activity from pre- to postintervention was observed in the GOALS group during the Scenes relative to the Categorize condition. Voxels with positive and negative salience (ie, those expressing reliable positive and negative associations with the LV pattern) 18 survived our bootstrap ratio threshold of ±3, k =10 voxels. Brain regions that exhibited this pattern of activity included the right middle and superior frontal gyrus, temporal parietal junction, precuneus, and left parahippocampal gyrus (See Figure 2B and Table 3).
Brain Areas Showing Greater Activity in the Goal-Oriented Attentional Self-Regulation Training Group (GOALS) Postintervention for the Scenes Condition (LV1).
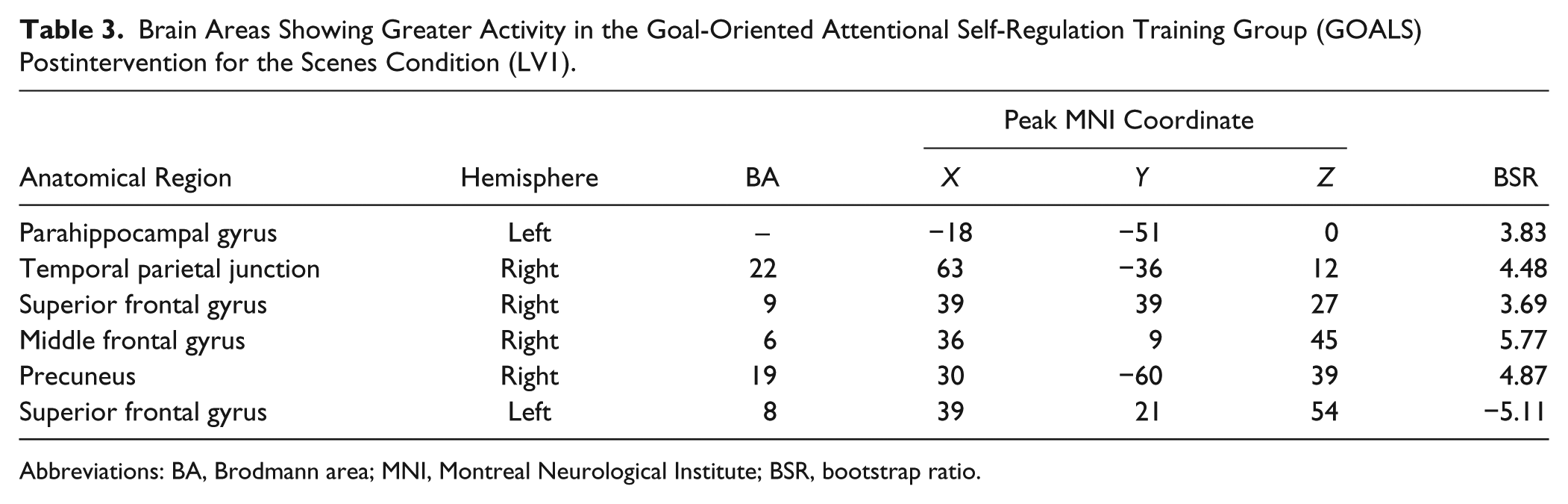
Abbreviations: BA, Brodmann area; MNI, Montreal Neurological Institute; BSR, bootstrap ratio.
As PLS identifies whole-brain patterns of covariance in BOLD activity, we investigated how the pattern of training-related brain changes observed in the GOALS groups aligned with previously identified whole-brain patterns of functional connectivity derived using resting-state functional connectivity. We used a resting state functional connectivity map derived from 1000 healthy subjects, 33 which identified seven functional networks including visual, somatomotor, dorsal attention, ventral attention, limbic, frontoparietal, and default. The pattern of enhanced activation during the selective attention condition in the GOALS group posttraining was topographically aligned with the frontoparietal (middle and superior frontal gyrus, precuneus), ventral attention (temporal parietal junction), and visual (parahippocampal gyrus) networks defined by Yeo et al 33 (Figure 3).
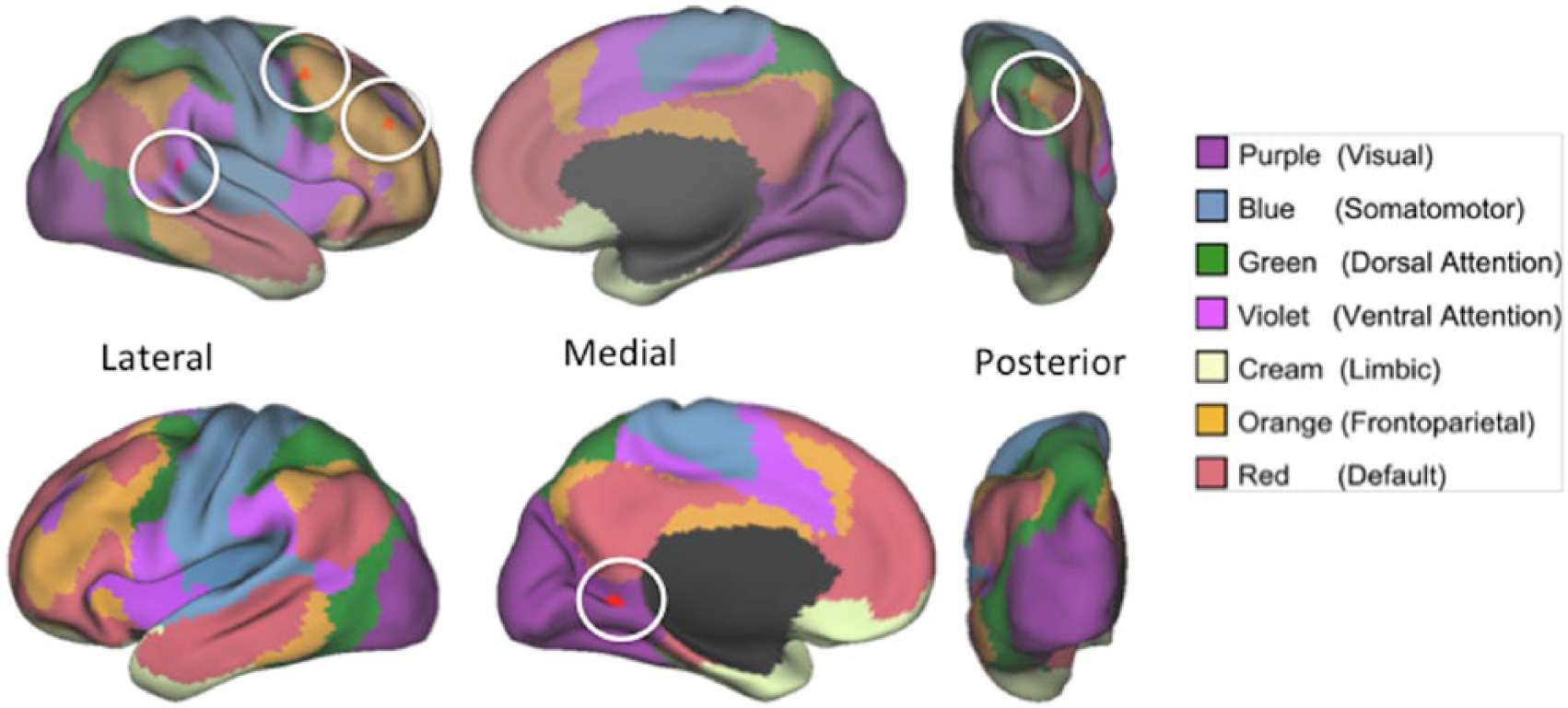
Overlap between 7 networks reported by Yeo et al 33 and findings reported in Figure 2. Colored legend shows corresponding network names. The right middle and superior frontal gyrus and precuneus overlap with the frontoparietal network (orange; Yeo et al 33 ),the temporal parietal junction overlaps with the ventral attention network (violet) and the parahippocampal gyrus overlaps with the visual system (purple).
Subsequent Memory Performance
An independent-sample t test was used to assess differences in subsequent memory assessed post-training (ie, D-prime) between GOALS and BHE. There was no significant difference in the D-prime index between GOALS (M = 0.14, SD = 0.18) and BHE (M = 0.12, SD = 0.03), t(9.58) = 0.35, P = .73. We computed a priori, single-tailed correlations between brain scores corresponding to the Scenes condition and D-prime values reflecting confidence in recall of attended versus ignored scene stimuli. We observed a correlation between D-prime and brain scores for the GOALS group that fell just below standard threshold for significance of 0.05, r(8) = 0.49, P = .07, η2 = .24. This correlation did not approach significance for the BHE group, r(8) = −0.30, P = .20, η2 = .09. Figure 4 depicts these findings. To confirm that these brain-behavior correlations were different between intervention groups they were Z-transformed, and compared using a Fisher’s Z-test. Correlations between brain changes and subsequent memory posttraining were significantly different between the 2 groups (Z = 1.57, P = .05).
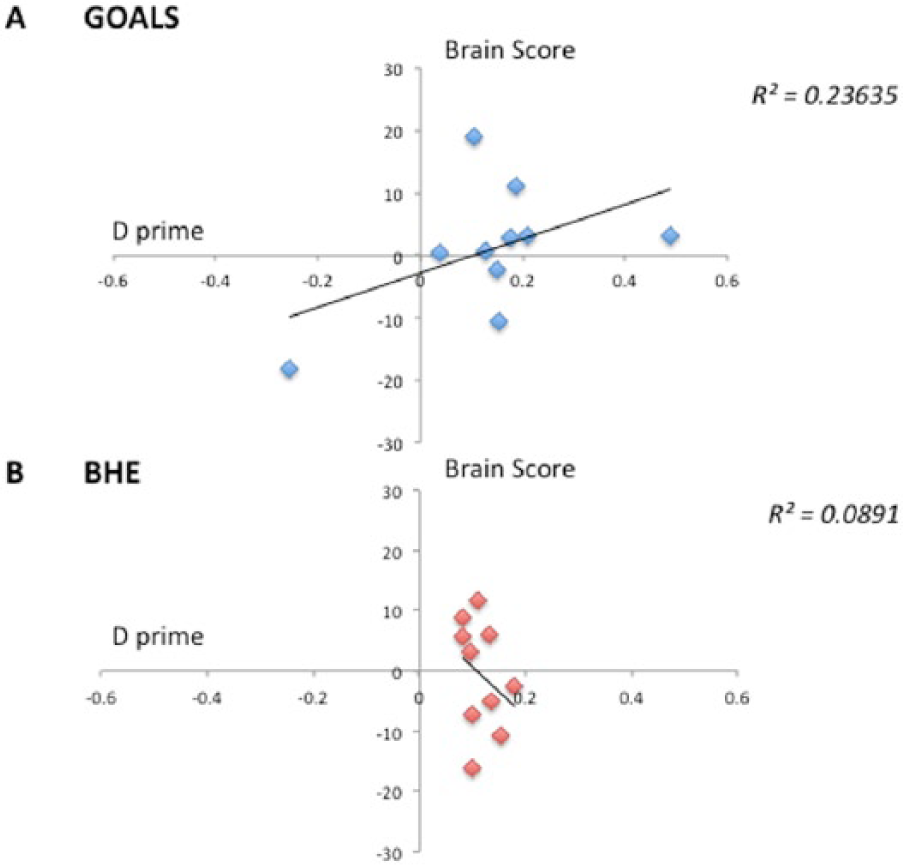
Correlations between participant brain scores (see Figure 2) during the Scenes condition postintervention and subsequent memory performance (D prime). Correlation plots for the Goal-Oriented Attentional Self-Regulation Training (GOALS) intervention group (A) and the Brain Health Education (BHE) group (B).
In addition, we conducted a multiple regression by group to investigate how participant age, years of education, and brain scores predicted D-prime for subsequent memory. For the GOALS group, the full model, including demographic variables and brain scores, did not reliably predict D-prime, F(3, 6) = 1.88, P = .23. In contrast, brain scores significantly predicted subsequent memory performance (β = 0.017, P = .05) while age (β = 0.02, P = .15) and years of education individually did not (β = 0.09, P = .17). For the BHE group, the full model failed to predict subsequent memory, F(3, 6)= 0.28, P = .84. Brain scores (β = −0.0009, P = .52), age (β = −0.0008, P = .76), or years of education (β = −0.001, P = 0.83) did not independently predict D-prime for the BHE group.
Discussion
We investigated whether participation in a cognitive training intervention designed to enhance executive control would be associated with functional brain changes in older adults. Participants were assigned to either an executive control training program (GOALS), where they were taught strategies to maintain goal focus and reduce off-task behaviors or an active comparison intervention that involved brain health education but not executive control skill training. Our mechanistic model of goal-directed attention regulation posits that top-down modulation of sensory association cortices is associated with both enhanced attention for goal relevant stimuli and suppression irrelevant or distracting stimuli (see Turner and D’Esposito 10 for a review). Consistent with this model, the GOALS training protocol includes strategies for attending to relevant stimuli and ignoring distractions. To capture both aspects of the attention regulation training we predicted that the relative change in attention to targets versus distractors, operationalized here as the discrimination index for subsequent recall of target versus ignored or novel stimuli, would be associated with functional brain activity post-GOALS. Posttraining performance on a selective information processing task that required participants to enhance attention to goal-relevant stimuli and suppress attention to distractor items, was associated with increased brain activity in the right middle and superior frontal gyrus, temporal parietal junction, precuneus, and left parahippocampal gyrus during the selective, relative to a nonselective, attention condition. Furthermore, this pattern of functional brain change was only observed in the active training group. These brain regions closely overlap with frontal-parietal and ventral attention networks previously implicated in goal-directed cognition.17,34,35 Behavioral comparisons of performance (reaction time and accuracy) did not reveal any group by time interactions, suggesting that brain-based measures of training change are more sensitive to training outcome than behavioral outcome on a given task. Furthermore, this pattern of relative enhancement of brain activity in attention and scene-selective visual association cortices was significantly predicted subsequent memory for attended versus ignored task stimuli, specific to the GOALS group. This is particularly interesting provided that the rationale for GOALS is to provide older adults with a meta-cognitive strategy to suppress or filter out distractions and focus their attention on task relevant stimuli. Furthermore, this pattern of enhancement of brain activity in attention and scene-selective visual association cortices was positively associated with subsequent recall of attended relative to ignored or novel task stimuli (ie, the discrimination index), only for the GOALS group. This finding, linking brain changes to behavior, while preliminary, provides support for our mechanistic model of training goal-directed attention modulation (ie, enhancement and suppression capacities) in older adults.
Attention Training and Neurocognitive Aging
There are a growing number of studies evaluating the impact of cognitive training on brain function in normal aging.36 -42 Both increases and decreases in neural activation following training have been reported, and these functional changes have been associated with better cognitive performance in older adults. 43 Here we investigated the impact of executive control training in a sample of cognitively normal older adults using a training protocol previously shown to modulate functional brain activity and remediate executive control deficits following acquired brain injury.15,16 The intervention is founded, in part, on a neuromodulation hypothesis of functional brain aging, suggesting that loss of top-down control, mediated by prefrontal brain regions, may reduce goal-directed modulation of activity in perceptual brain regions, resulting in reduced attention control. 10 Our findings suggest that targeted training, based on this neuromodulation account, is associated with increased activity during a selective attention task in brain regions associated with executive control. Furthermore, increased activity in these brain regions post-GOALS training was positively associated with subsequent recall of goal-relevant versus nonrelevant information. Together, these findings suggest that the training-related functional brain changes may reflect increased goal-directed executive control.
Neuromodulation and Selective Attention
Age-related cognitive decline has been associated with poor suppression of distracting, or goal-irrelevant, information. 5 Older adults have greater subsequent memory for information that they are instructed to ignore during selective attention tasks, suggesting poor selective attention to goal relevant versus nonrelevant information. 7 At the level of the brain, reduced ability to suppress distractions in older adults has been associated with reduced goal-directed modulation of perceptual processing regions by prefrontal regions, resulting in inefficient information filtering.7,10 Recent work has provided direct evidence for prefrontal modulation of posterior visual processing regions using transcranial magnetic stimulation methods in younger adults.17,44 This modulatory capacity may decline in older adulthood, reducing the ability of older adults to selectively filter goal-relevant from distracting information for information processing. Alterations in PFC functioning during cognitive control processing is a hallmark of neurocognitive aging. 45 Changes include poor modulation of PFC activity in the context of increasing task challenge46,47 as well as compensatory engagement of prefrontal brain regions to sustain goal-directed attention in the context of increasing cognitive control demands. 48 Here, we provide evidence that selective attention training may enhance PFC activity, resulting in enhanced goal-directed executive control in older adulthood.
The GOALS training protocol is predicated on earlier reports that suppression of goal-irrelevant information is reduced in older adulthood. 6 We reasoned that by targeting this neural mechanism through training participants on the Stop-Relax-Refocus meta-cognitive strategy, older adults would demonstrate increased capacity to modulate attention based on task goals, enhancing attention to relevant while ignoring irrelevant stimuli. These results, and previous findings from our group, 16 highlight the potential of this “brain-based” approach for designing increasingly targeted cognitive interventions to enhance or remediate cognitive functioning.
GOALS Training and Functional Brain Networks
Cognitive neuroscience research is increasingly investigating changes in the pattern of coordinated activity among distributed brain regions as the neural basis of cognitive function and dysfunction. Based on our neuromodulatory account of age-related changes in selective attention, we used multivariate neuroimaging analysis (PLS) to identify co-varying patterns of brain activity that reliably mapped onto our experimental design. As reviewed above, we observed a pattern of covarying increases in activity in right middle and superior frontal gyrus, temporal parietal junction, precuneus, and left parahippocampal gyrus. This pattern reflected pre to post changes only in the GOALS group. The right middle and superior frontal gyrus and precuneus are brain regions within a frontoparietal network, 33 thought to be critical for cognitive control. 35 Increases in this network covaried with increases in the temporal-parietal junction and parahippocampal gyrus, nodes in the ventral attention and visual networks. 33 While the current study did not investigate network dynamics directly, these findings suggest that GOALS training increased activity and coherence between top-down (ie, goal directed) and bottom-up (ie, stimulus based) attentional systems. Increased coherence between perceptual and attentional processing regions may, in turn, enhance the processing of goal-relevant versus irrelevant stimuli. This coherence account of goal-directed executive control will need to be confirmed in future research. However, the current results are consistent with recent work showing that lateral PFC (specifically the inferior frontal gyrus) is involved in determining the task relevance of incoming visual information and communicating that information to a distributed frontoparietal network of regions 17 and orienting of attention. 49
Recent work has also investigated how the type of training can be a critical factor in determining the pattern of brain activation. 50 Bellevile et al 50 found that practice training leads to reduced activation, while training programs that target teaching of metacognitive processes lead to increased activation. This INTERACTIVE training model 50 suggests that activation changes depend on training modalities as well as a complex interaction between those and the specific characteristics of the participants. Our findings are consistent with the INTERACTIVE model, given that our training targeted executive control processes through an interactive, meta cognitive strategy, consistent with other studies of metacognitive training strategies showing increased patterns of activation posttraining.51 -53
Limitations
We recognize the limitation of the small sample sizes in the current study. Indeed, we have been noting this as a common challenge of cognitive rehabilitation research for more than a decade.54 -56 The complexity of the study protocol, involving multiple assessment sessions to collect brain and behavioral data pre- and posttraining, in addition to the training protocol itself, placed significant time commitments on participants and thus increased recruitment challenges. In addition, data loss due to attrition, as well as MRI data quality issues resulted in reduced group sizes. We have made every attempt in our protocol design to mitigate this limitation. These include a within-subject design, a demographically matched control group, and perhaps most important, the inclusion of a closely matched, active control condition (BHE). Further, this rehabilitation protocol has previously been associated with positive brain and behavioral outcomes in acquired brain injury with cohorts of similar sizes15,16,57. Ongoing work in our laboratories is attempting to develop virtual training protocols to be delivered at home, thereby reducing participant burden, which should allow for larger sample sizes in future research studies.
Conclusion
The posttraining changes observed here following GOALS training are particularly striking given the intact cognitive status of the older adult cohort, and our careful matching of the GOALS and BHE interventions. We suggest that our capacity to identify reliable training-related brain changes, given this tightly controlled experimental design and relatively small group sizes, may be attributable to 2 main factors. First, as described above, we designed the protocol to target a specific cognitive process with known susceptibility to aging, and a well-characterized neural signature. Second, the GOALS training protocol emphasizes real-world application. In contrast to protocols that train tasks with poor ecological validity or relevance, we used participant-generated goals to practice executive control in contexts that are personally meaningful. While not the focus of the current report (G. R. Turner et al, 2017, unpublished data), this emphasis on real-world functional gains likely increased participant engagement and commitment to the training protocol, and provided numerous opportunities to apply and practice learned skills over the intervention period.
In sum, our findings provide strong empirical support for the brain-based approach to cognitive training adopted here. By linking the intervention protocol with a specific neural mechanism, we were able to leverage over a decade of cognitive neuroscience research to inform the design of a targeted cognitive training protocol. We believe this approach holds considerable promise for the future development of clinically relevant, cognitive training and rehabilitation interventions in aging, brain injury, and disease.
Footnotes
Acknowledgements
The authors wish to thank the participants and colleagues who made this study possible, in particular: Brian Levine, PhD; Ian Robertson, PhD; and Tom Manly, PhD, for providing us with the original Goal Management Training materials; Joseph Viviano and Terry Nycum for technical assistance; Jeff Cooney and Adam Gazzaley for functional MRI visual stimuli; Jessica Black, Michelle Murphy, PhD, Annemarie Rossi, OTR/L, Elaine Laguerta, and Courtney Gallen for assistance managing and organizing the study, Kevin Barrows, MD, for use of his CD for mindfulness home practice.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the National Institutes of Health (grant number AG034642) to M.D.; Canadian Institutes of Health Research (CIHR, grant number: 273007), Heart and Stroke Foundation and Ontario Graduate Scholarship to A.A.