
Abstract
Background. One bout of high-intensity cardiovascular exercise performed immediately after practicing a motor skill promotes changes in the neuroplasticity of the motor cortex and facilitates motor learning in nondisabled individuals. Objective. To determine if a bout of exercise performed at high intensity is sufficient to induce neuroplastic changes and improve motor skill retention in patients with chronic stroke. Methods. Twenty-two patients with different levels of motor impairment were recruited. On the first session, the effects of a maximal graded exercise test on corticospinal and intracortical excitability were assessed from the affected and unaffected primary motor cortex representational area of a hand muscle with transcranial magnetic stimulation. On the second session, participants were randomly assigned to an exercise or a nonexercise control group. Immediately after practicing a motor task, the exercise group performed 15 minutes of high-intensity interval training while the control group rested. Twenty-four hours after motor practice all participants completed a test of the motor task to assess skill retention. Results. The graded exercise test reduced interhemispheric imbalances in GABAA-mediated short-interval intracortical inhibition but changes in other markers of excitability were not statistically significant. The group that performed high-intensity interval training showed a better retention of the motor skill. Conclusions. The performance of a maximal graded exercise test triggers only modest neuroplastic changes in patients with chronic stroke. However, a single bout of high-intensity interval training performed immediately after motor practice improves skill retention, which could potentially accelerate motor recovery in these individuals.
Keywords
Introduction
The innate ability of the human brain to repair itself from neurological damage through neuroplasticity forms the basis of stroke rehabilitation. 1 However, the optimal window for neuroplasticity to positively affect motor recovery spans only some weeks after the stroke has occurred. 2 After this initial period, the rate of recovery slows down and functional improvements become more difficult to achieve. 3 Interventions that promote neuroplasticity early after stroke or extend this initial window of neuroplasticity have the greatest potential to improve motor recovery in individuals who are poststroke. 4 One simple and cost-effective intervention that promotes neuroplasticity is cardiovascular exercise.5,6 Experiments using stroke animal models have confirmed that this type of exercise reduces the size of the lesion 7 as well as the inflammation and oxidative stress in perilesional areas. 8 In individuals who are poststroke, cardiovascular exercise has shown to improve some aspects of cognition and motor function.9,10 However, the effects of this aerobic intervention on the neuroplasticity of the corticospinal pathway and, more important, on the capacity to recover lost motor skills, is unknown.
In individuals without disability, even a single bout of cardiovascular exercise is accompanied by neuroplastic changes in the primary motor cortex (M1),11-15 a therapeutic target area for motor recovery poststroke. 16 One bout of exercise, performed alone11-15 or in combination with noninvasive brain stimulation protocols applied over M1,17,18 amplifies changes in different markers of excitability such as corticospinal excitability (CSE) and intracortical facilitation (ICF) and reduces short-interval intracortical inhibition (SICI). 14 These transient changes in excitability precede more long-lasting neuroplastic adaptations, which are needed for motor learning. 14 We have shown in healthy adults that, in close temporal proximity to motor practice,19,20 exercise-induced changes in CSE have functional implications for the consolidation of procedural memory. 21 When performed immediately before or after practicing a motor skill, a bout of high-intensity interval training (HIIT) induces a sustained increase in CSE17,21 and improves the retention of motor skills.19,22,23 Whether a bout of intense cardiovascular exercise may elicit similar effects in patients with stroke is not known.24,25
Studies investigating the neuroplastic response to acute exercise in neurologically intact individuals indicate that the intensity of exercise is crucial. Mang et al 17 showed that 20 minutes of HIIT (with only 9 minutes at 90% of maximal oxygen uptake, VO2peak) performed on a cycle ergometer amplified the response to an excitatory paired associative stimulation protocol, increasing CSE 26 assessed from the M1 representation of a hand muscle and improved skill retention. In contrast, 30 minutes of moderate intensity continuous training performed at 60% VO2peak had no effects on CSE or motor learning, 27 Furthermore, 30 minutes of moderate-intensity continuous training performed immediately before a continuous theta burst (cTBS) protocol applied with transcranial magnetic stimulation (TMS) on M1, protected the decay in CSE commonly observed after cTBS. 28 In contrast, when cTBS was preceded by a bout of low-intensity exercise, there was no suppression of cTBS effects on CSE. 18 We have shown that when motor practice is followed by 15 minutes of HIIT (90% VO2peak), improvements in skill retention are more pronounced than when moderate intensity (45% VO2peak) is used. 23 Increasing exercise intensities could potentially amplify the gains that cardiovascular exercise has on neuroplasticity and motor recovery poststroke. 29
The practical challenge remains in that cardiovascular exercise performed at a vigorous intensity and for long periods of time is difficult for individuals with stroke. 30 After stroke, individuals may have motor deficits or be too deconditioned to maintain the intensity required to achieve the desired training effect.31-33 This imposes a ceiling on the capacity to exercise at high intensities and thus to promote neuroplasticity and motor recovery. 34 Finding new exercise strategies that allow higher intensities and provide greater physiological stimulus could maximize the benefits of cardiovascular exercise in stroke rehabilitation. 30 HIIT combines short bursts of high-intensity exercise with periods of rest or active recovery, 35 allowing even very deconditioned patients to achieve higher intensities during exercise and thus induce greater cardiorespiratory and metabolic adaptations. 36 Recent investigations 37 provide preliminary evidence supporting the use of HIIT as a safe and feasible exercise intervention to improve functional and cardiorespiratory outcomes in stroke rehabilitation but the effects of HIIT on motor learning poststroke have not been evaluated. 25
The primary objective of this study was to investigate the effects of a single bout of HIIT performed after motor practice on motor learning in individuals with chronic stroke. Based on our previous studies in young individuals,17,19,22,23 we hypothesized that HIIT would improve motor learning by optimizing skill retention. The secondary objective was to determine if an exercise bout performed at maximal intensity could reopen a new window of neuroplasticity in chronic stroke, promoting transient changes in motor cortex excitability. To this end, we used TMS to measure CSE, ICF, SICI, and the cortical silent period (CSP) from the affected and nonaffected M1 upper limb area before and after a maximal graded exercise test (GXT) performed to assess cardiorespiratory fitness. These measures of excitability represent different markers of neuroplasticity 38 underlying motor learning processes26,39 that predict skill retention in nondisabled individuals 21 and functional recovery in patients with stroke. 40 We hypothesized that the GXT would modify excitability reducing the interhemispheric imbalances commonly observed after stroke. 4
Methods
Experimental Design
Patients attended 3 experimental sessions (Figure 1). On the first session, after an initial physical and cognitive evaluation (see below), all patients performed a maximal, symptom-limited GXT to assess their VO2peak. 41 Immediately before and 15 minutes after the GXT, TMS was applied over M1 to evaluate the acute effects of exercise on CSE, ICF, SICI, and the CSP in both hemispheres. Between 2 and 7 days after the first session, participants reported to the laboratory again to practice a time-on-target motor task (second session). Immediately after, they were randomly allocated (1:1) into either an exercise or nonexercise (control) group. The exercise group performed 15 minutes of HIIT and the control group simply rested for the same period. Twenty-four hours later (third session) all patients underwent a test of the motor task to assess skill retention. Participants were instructed not to engage in moderate- or high-intensity physical activity during the 24 hours prior to the second and third sessions. A human research review board approved the project.
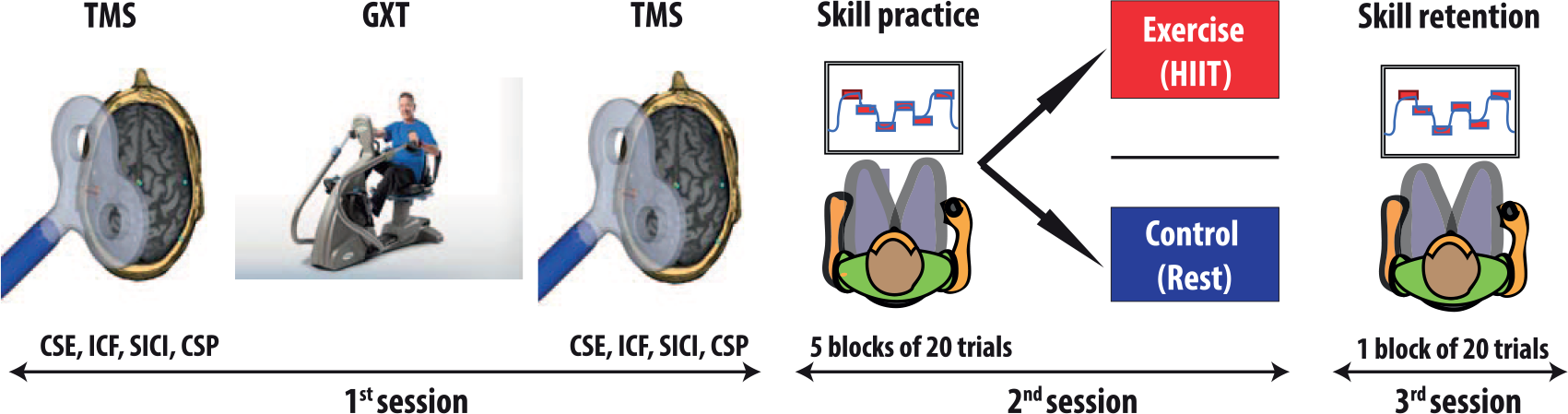
Design of the study.
Patients
We recruited a sample of convenience, including patients with (1) chronic stroke, (2) no upper limb musculoskeletal or neurological conditions other than stroke-related motor deficits, (3) sufficient ability/capacity to perform the exercise protocols and demonstrate improvements during the practice of the motor task, and (4) a score ≥20 in the Montreal Cognitive Assessment (MoCA). We used this cutoff score because the score of <26 normally used to establish cognitive impairment would render 78% of the patients ineligible. 42 Participants were not excluded because of the location and type of stroke but they needed to show capacity to improve skill scores in 3 or more blocks of practice in comparison with baseline levels. The use of such broad eligibility criteria was intentional. This was a proof-of-concept study that investigated whether the positive results that we have observed in nondisabled young individuals17,19,21-23 could be replicated in patients with different characteristics and motor impairment levels. All participants provided written informed consent prior to participation.
Initial Evaluation
Patients were tested for cognitive function using the MoCA test. In addition, we administered the Chedoke-McMaster Stroke Assessment 43 to assess their level of hand impairment in the most affected limb. Other descriptive measures, including, age, weight, height as well as the type of stroke, location and time since stroke were also collected.
Graded Exercise Test
We used a well-validated GXT protocol 41 that uses a whole-body recumbent stepper ergometer to assess VO2peak in patients with stroke. Heart rate (HR) and blood pressure (BP) were measured continuously with a HR and a BP monitor, respectively. Electrocardiography monitoring was used in those individuals with cardiac comorbidities. The rate of perceived exertion was monitored with the Borg scale. 44
Transcranial Magnetic Stimulation
Using neuronavigation we first co-registered the patients’ heads to a standard magnetic resonance image template to identify and mark the optimal coil position (“hot-spot”) of M1 for eliciting motor-evoked potentials (MEPs). TMS was applied through a 70-mm coil with a Super Rapid Plus Magstim stimulator to the M1 representational areas of the first dorsal interosseous muscle on both the affected and unaffected sides. This muscle is heavily recruited during the motor task used in the experiment and has a low resting motor threshold (RMT). 45 This ensures that MEPs can be elicited at relatively low stimulation intensities, which is critical in patients with stroke, who usually require higher intensities. 38 The “hot-spot” was determined through a mini-mapping procedure identifying the coil position that elicited the largest possible MEP amplitudes obtained at a fixed suprathreshold intensity. Electromyographic activity, recorded via 2 surface electrodes placed over the first dorsal interosseous at ~1 cm of distance, was acquired at 2000 Hz with a gain of 300 and filtered using a high- and low-pass cutoff filter of 10 Hz and 500 Hz, respectively. 21 Once we identified the “hot-spot,” we determined the RMT, defined as the minimum stimulation intensity required to elicit consistent MEPs of 0.05 mV in at least 10 of 20 trials. 38
Maximal Voluntary Contraction
Immediately after finding the “hot-spot” and determining the RMT, we assessed the handgrip maximal voluntary contraction (MVC) force for the muscles of the affected and nonaffected hand using a custom script built on LabView. Patients were seated in front of a 27-inch computer monitor grasping a grip force response pad with their hand in a neutral semiprone position (Figure 1). A slider displaying the force applied was shown on the screen. Patients made a fist, “squeezing” the force pad and the slider moved vertically. They performed 3 MVCs of approximately 3 seconds each separated by a 30-second pause. The highest MVC was recorded and saved.
Corticospinal Excitability
We assessed CSE both at rest and during an active muscle contraction sustained at 20% of the MVC. The LabView script used to measure MVC provided visual feedback while participants were asked to maintain the muscle contraction at the 20% MVC force level. CSE was quantified by measuring the average peak-to-peak TMS-induced MEP amplitude of 40 stimulations (20 for resting and 20 for active CSE) elicited at an intensity of 120% RMT. 39 MEP amplitude provides an estimation of the excitability of the corticospinal pathway, with larger MEPs amplitudes reflecting larger CSE. 26 To minimize the potential effects of repetitive TMS on CSE each stimulation was delivered 5 seconds apart.
Intracortical Facilitation and Short-Interval Intracortical Inhibition
Measures of intracortical excitability allowed us to examine neuroplastic changes modulated by the activity of intracortical neurotransmitter receptors.
38
ICF provides information of facilitation mediated by N-methyl-
Cortical Silent Period
The CSP is a period of electrical silence in the surface EMG activity that occurs immediately after an MEP elicited during a muscle contraction. 38 When elicited at relatively high intensities of stimulation (ie, generating CSPs >100 ms) the CSP provides information about the inhibitory activity modulated by GABAB receptors. 38 Long CSPs reflect large inhibition levels. 38 The CSP was measured in the 20 stimulations elicited at 120% RMT during tonic contraction to assess active CSE. We first measured the EMG baseline signal amplitude 200 ms before stimulation. The end of the MEP and the recovery of the voluntary electromyographic activity (ie, increase of 2 standard deviations [SDs] above the mean baseline signal amplitude) marked the beginning and the end of the CSP, respectively. 38 The accuracy of the CSP detection was confirmed through visual inspection and the average CSP duration calculated.
Time-on-target Motor Task
We used a motor task that requires modulating hand-grasping force because this skill is essential in many activities of daily living. Participants seated in front of a computer screen held the same grip force response pad used for the MVC assessment with their more affected hand. 22 The screen displayed 12 red square (1.5 × 3 cm) targets placed horizontally at different heights (Figure 1). A blue cursor crossed the screen from left to right at 8 seconds/screen. Participants increased grip force to move the cursor up and reach the targets. The goal was to keep the cursor within the target as much time as possible. The force required to reach the highest target was ~20% of the subjects’ MVC. To minimize skill level differences at baseline, participants could practice the task before training until they reached a score of 30 (see below how scores were calculated). Training consisted of 5 blocks of 20 trials and retention 1 block of 20 trials. Patients had ~1 minute of rest between blocks. Feedback on performance (a score from 0 to 100) was given after each trial. 22 The score was calculated from the total time that the cursor was on target area (ToT) divided by the total time of each trial (Tt) multiplied by 100 (score = (ToT/Tt) × 100). The difference in mean scores from baseline to the best block of training reflected skill acquisition and the difference between the best block of training and the 24-hour retention block reflected retention.
High-Intensity Interval Training
Ten minutes after motor practice patients randomized into the exercise group performed HIIT on the same recumbent stepper used for the GXT (see details of a similar HIIT protocol in Roig et al 22 ). HIIT started with 2 minutes of warm-up (25% peak workload GXT) followed by three 3-minute blocks of high intensity (100% peak workload GXT) interspersed with two 2-minutes blocks of low intensity (25% peak workload GXT) in between. Participants were asked to maintain a stepping cadence of 80 steps/min. 41 Intensity was monitored with a HR monitor and rate of perceived exertion with the Borg scale. 44
Statistical Analysis
Differences between the exercise and control group in demographic variables were assessed with unpaired t tests and chi-square tests. The effects of the GXT on the different measures of excitability (CSE, ICF, SICI, and CSP) and their interhemispheric ratio (affected/unaffected) (see details in Madhavan et al 25 and Di Lazzaro et al 47 ) were tested with Wilcoxon matched-pair signed-rank tests. Interhemispheric ratios were used to determine if exercise could reduce asymmetries in excitability between hemispheres. 4 Two-way repeated-measures analysis of variance (ANOVA) with training block as within-subjects factor and group as between-subjects factor was used to determine group differences in skill acquisition. Group differences in skill retention were assessed with unpaired t tests. To quantify the effect of the GXT on excitability the effect size (d) was calculated from the difference between excitability (post − pre measures) divided by the pooled SD. 48 Similarly, the effect of HIIT on skill retention was calculated from the difference between mean change scores (score retention block − score best training block) of the exercise and control group divided by the pooled SD. 48 All analyses were performed with 2-tailed probability tests with the statistical significance level set at P ≤ .05.
Results
Two participants that could not improve skill level after baseline and one who had a MoCA score of 12 were screened but did not participate in the study (Figure 2). The characteristics of the 22 participants finally included in the study are shown in Table 1. The MoCA scores ranged from 21 to 30 (average = 25.3) and the Chedoke scores ranged from 1 to 7 (average = 6.1). Despite the heterogeneity within each group and an unequal sex distribution between groups due to the randomization procedure, the exercise and control groups were similar in terms of mean age, cognitive status (MoCA), hand impairment (Chedoke), time since stroke, VO2peak, and responses to the GXT (HR). Patients completed the GXT and HIIT without any adverse effect other than fatigue. The mean (SD) HR and rate of perceived exertion during the last block of the HIIT protocol was 128.81 (14.79) and 16.18 (2.96), respectively. One participant with bilateral stroke did not to complete the TMS procedures. In another study participant, MEPs could not be collected at comfortable intensities (Figure 2). TMS data for these 2 participants are not reported. Furthermore, one participant in the control group did not perform the retention test and thus behavioral data are not reported because skill retention could not be calculated.
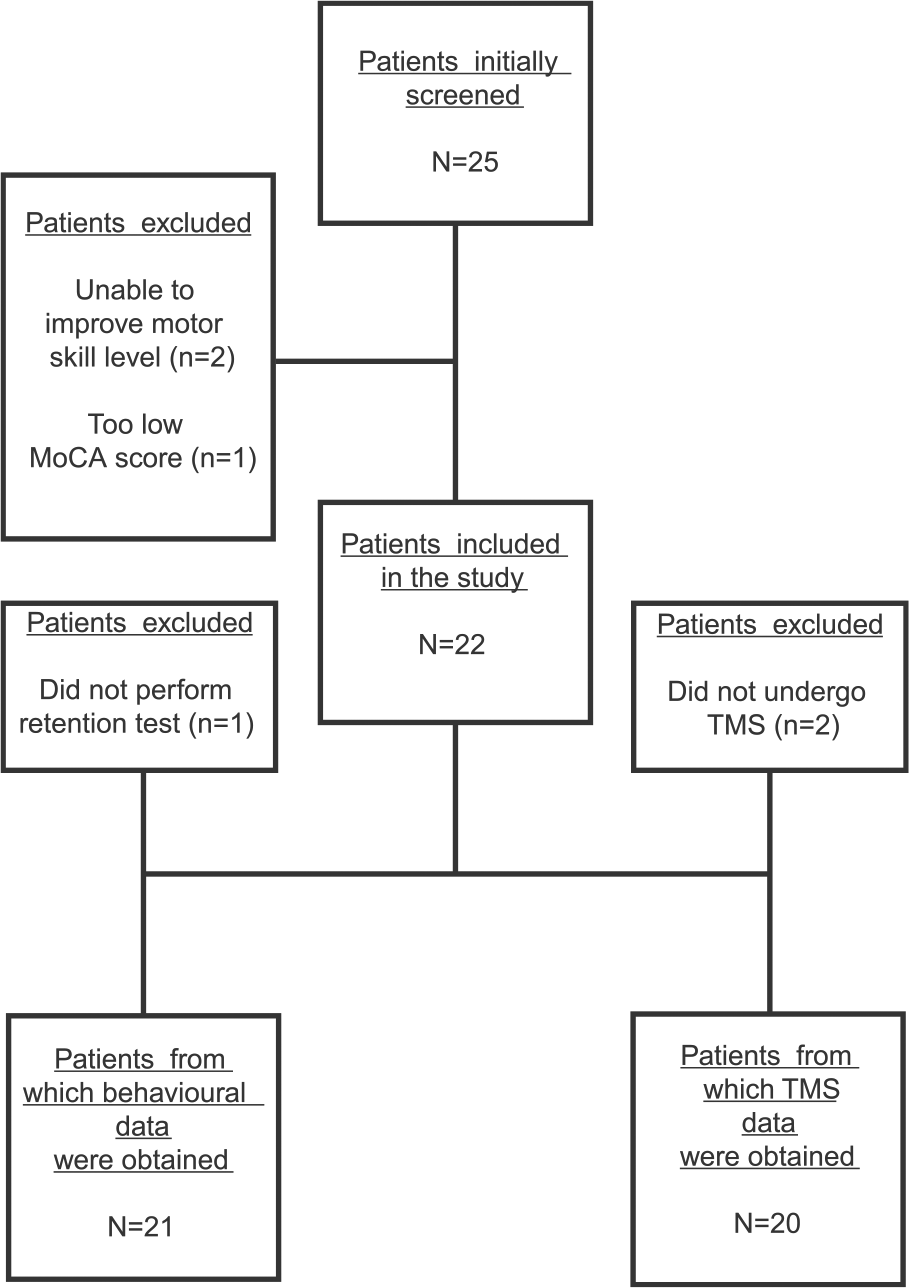
Flow diagram showing the different phases of the study for recruitment and testing.
Characteristics of All the Patients Included in the Study.
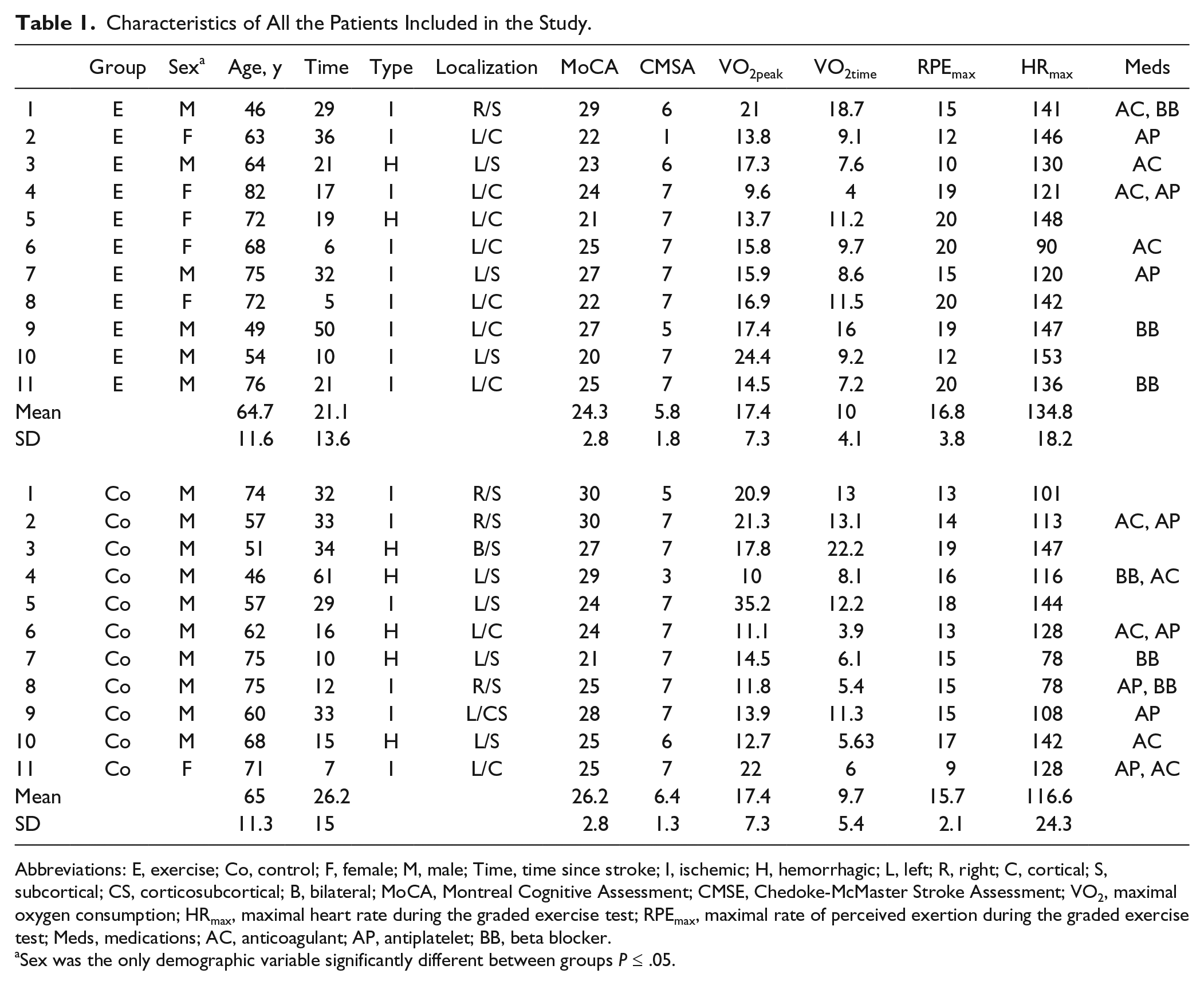
Abbreviations: E, exercise; Co, control; F, female; M, male; Time, time since stroke; I, ischemic; H, hemorrhagic; L, left; R, right; C, cortical; S, subcortical; CS, corticosubcortical; B, bilateral; MoCA, Montreal Cognitive Assessment; CMSE, Chedoke-McMaster Stroke Assessment; VO2, maximal oxygen consumption; HRmax, maximal heart rate during the graded exercise test; RPEmax, maximal rate of perceived exertion during the graded exercise test; Meds, medications; AC, anticoagulant; AP, antiplatelet; BB, beta blocker.
Sex was the only demographic variable significantly different between groups P ≤ .05.
Motor Skill Acquisition and Retention
All subjects showed improvements in skill performance during training (average improvement = 23.7%). Importantly, both groups had a similar skill level at baseline (unpaired t test, t(19) = 0.31; P = .75) and last block of practice (unpaired t test, t(13.86) = −0.30; P = .77). Furthermore skill acquisition through the 5 blocks of practice between groups was not statistically different (ANOVA repeated measures, F(2.5, 47.68) = 0.91; P = .42) (Figure 3). Skill retention was significantly better in the HIIT group (unpaired t test, t(19) = 2.20; P = .04; effect size d = 0.96), which showed a 9% improvement in skill level compared with the end of acquisition while the control group showed a 4% decay (Figure 4). Specifically, 7 out of 11 participants in the HIIT group improved their mean score in the retention block compared with the best block of training while only 3 participants in the control group showed improvement.
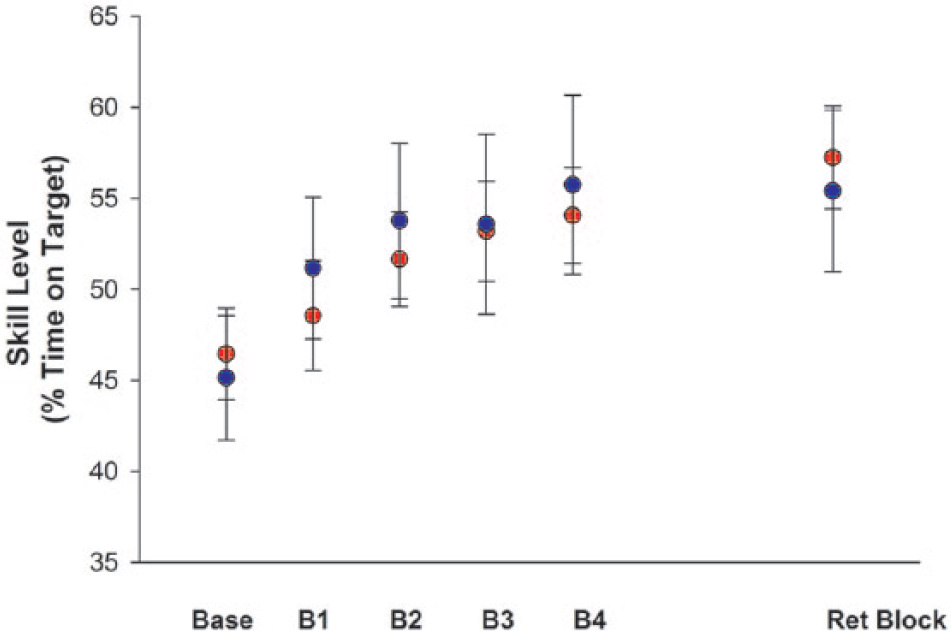
Performance of the motor sill at baseline (Base), the 4 blocks of practice (B1-B4) and the retention block (Ret Block) performed 24 hours after motor practice. Differences between groups in the rate of skill acquisition (Base – B4) were not statistically significant (analysis of variance repeated measures, F(2.5, 47.68) = 0.91; P = .42). The high-intensity interval training (HIIT) group is depicted in red and the nonexercise (control) group in blue. Error bars are standard error of the mean.
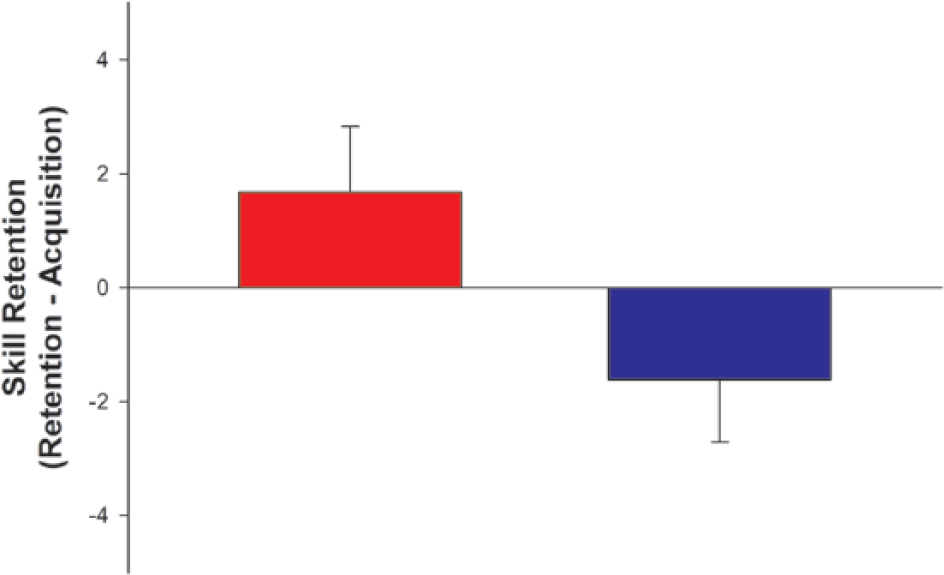
Skill retention, measured as difference in skill level between the best block of motor practice during acquisition and the 24 hours retention block. Skill retention, was significantly better in the high-intensity interval training (HIIT) group (unpaired t test, t(19) = 2.20; P = .04; effect size d = 0.96). The HIIT group is depicted in red and the nonexercise (control) group in blue. Error bars are standard error of the mean.
Measures of Corticospinal and Intracortical Excitability
Mean changes in CSE, SICI, ICF, CSP and their interhemispheric ratios after the GXT are shown in Table 2. Both resting and active CSE measures in the affected side increased after the GXT, however, changes were not significant. CSE measures tended to increase more in the affected side but changes in interhemispheric ratios were not statistically significant. SICI showed a tendency to decrease in the affected side and, as result, its interhemispheric ratio increased significantly. ICF, CSP, and their respective ratios, in contrast, did not show any significant change.
Changes in the Different Measures of Excitability After the Graded Exercise Test (GXT). a
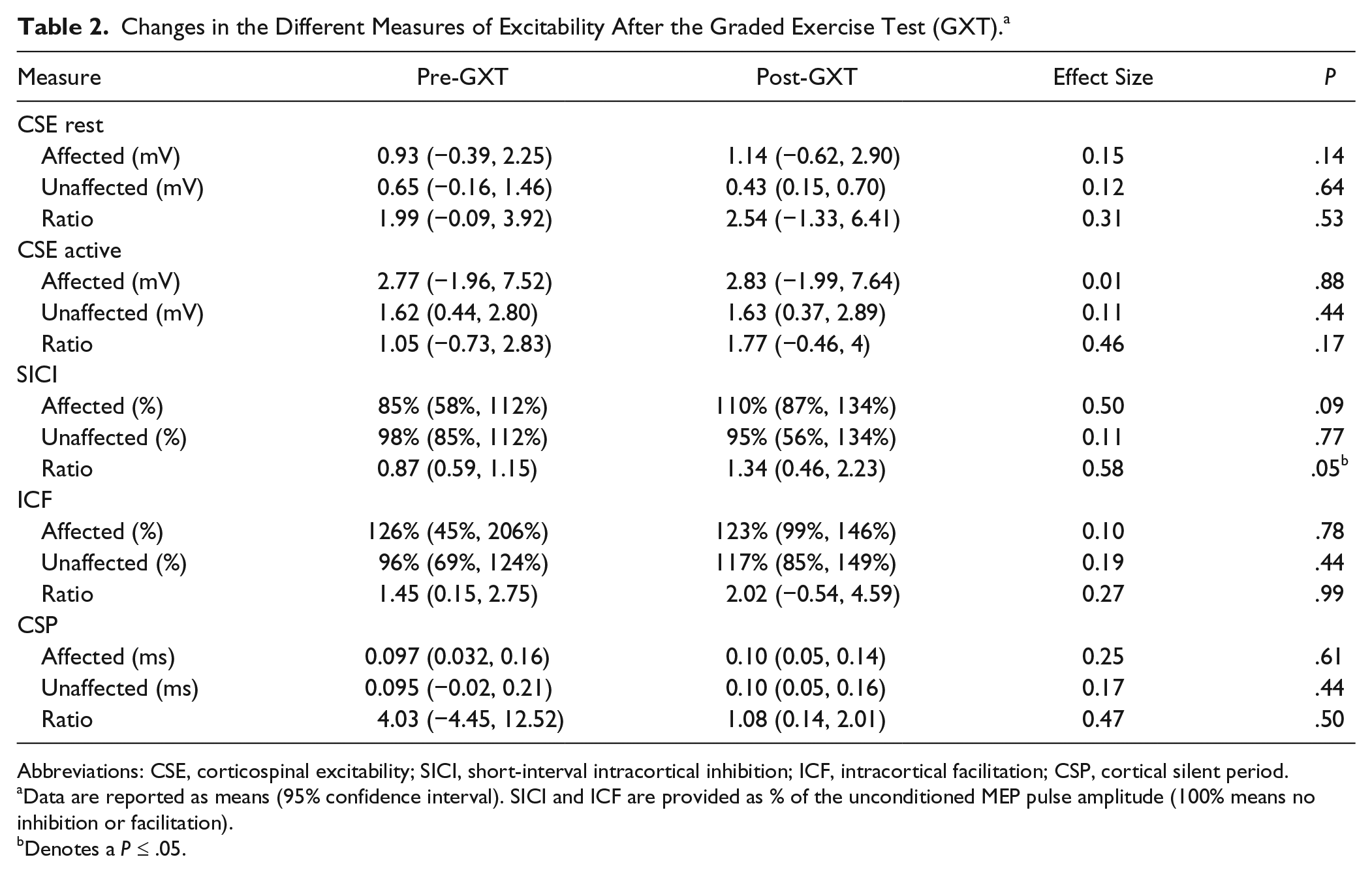
Abbreviations: CSE, corticospinal excitability; SICI, short-interval intracortical inhibition; ICF, intracortical facilitation; CSP, cortical silent period.
Data are reported as means (95% confidence interval). SICI and ICF are provided as % of the unconditioned MEP pulse amplitude (100% means no inhibition or facilitation).
Denotes a P ≤ .05.
Discussion
This study aimed to determine if high-intensity cardiovascular exercise improves motor learning in individuals with chronic stroke. Similarly to what we have shown in young adults without disability,19,22,23,49 we found that a short bout of HIIT performed immediately after motor practice improves skill retention in these individuals. The relatively large effect of HIIT on skill retention (d = 0.96) suggests that this intervention could be clinically relevant. When performed at moderate intensity and separately from motor practice, regular bouts of exercise have only modest effects on motor learning in patients with chronic stroke. 10 Our results suggest that by increasing the intensity of exercise and temporally matching the exercise stimulus with motor practice the effectiveness of this intervention could be enhanced. 50 Although we only assessed the effects of a single bout of exercise, repeated bouts of HIIT closely combined in time with motor practice might augment cumulative gains in motor learning after several rehabilitation sessions and thus accelerate functional recovery. 51 Longitudinal studies with more functional motor tasks will be needed to confirm the efficacy and applicability of this novel multimodal intervention in stroke rehabilitation.
The effects of HIIT on skill retention shown in this study reinforce the importance of looking beyond motor practice in rehabilitation. Designing strategies that improve the efficacy of motor practice is essential for the recovery of sensorimotor function after stroke. 52 However, what happens immediately before and after motor practice may also influence how effectively the gains obtained during practice are retained between training sessions and thus determine the speed of the recovery process. 53 When performed immediately after motor practice, exercise promotes neuroplastic changes that facilitate the consolidation of procedural memories,5,21,49 which encompass the sensorimotor information encoded during motor practice. 22 Improving memory consolidation through exercise leads to an stabilization of the procedural memory or even to enhancements in skill level without additional practice. 53 Indeed, an important finding of our study was that the exercise group increased their skill level at retention compared with the end of practice (Figure 4). This suggests that a single bout of HIIT could not only strengthen procedural memories during consolidation but also promote off-line gains and accelerate motor learning between practice sessions. 54
We explored if a GXT could trigger changes in the excitability of the motor cortex and corticospinal pathway in individuals with chronic stroke. Our results indicate that, compared with people without disability,11-15,17,21,55 the neuroplastic response to acute intense exercise in these individuals might be hindered. In healthy young individuals, acute exercise has shown to increase CSE and ICF in some13,21 but not all 56 studies and to reduce SICI.11,15,56 Information regarding changes in CSP and other similar TMS measures of GABAB receptor activity (eg, long intracortical inhibition) is scarce and less consistent. 11 In this study, SICI showed a tendency to decrease in the affected side but only its interhemispheric ratio increased significantly (Table 2). Murdoch et al 24 recently reported that a single bout of exercise performed at low-to-moderate intensity (rate of perceived exertion = 11-13) had no effect on SICI assessed from the affected side in people with chronic stroke. 24 The tendency toward a reduction of SICI found in our study suggests that the higher intensities achieved during the GXT (mean rate of perceived exertion = 16.3) could amplify the neuroplastic response to a single bout of cardiovascular exercise in these individuals.
Reductions in GABAA-ergic inhibitory activity are associated with superior motor learning performance in healthy individuals. 57 Furthermore, SICI levels in the affected side are negatively associated with motor function at 3 and 6 months after stroke. 58 More studies assessing the combined effects of exercise and motor learning 21 will be required to determine whether the reduction of intracortical inhibition found after the GXT also contributed to the effects of HIIT on skill retention in individuals with chronic stroke. Perhaps the fact that ICF levels appear to be normal after stroke 4 or the less consistent effects of exercise on ICF 11 might explain why this parameter remained relatively unchanged after the GXT.
The fact that, after the GXT, CSE in the affected side did not increase more significantly could be simply due to a reduction of the neuroplastic potential after stroke. 59 Indeed, in young individuals without disability,18,55 one bout of exercise has shown to reduce the suppressing effects of cTBS on CSE. In contrast, in individuals with chronic stroke, one bout of exercise does not amplify the facilitatory effects that intermittent TBS has shown to have on CSE, 24 suggesting that after stroke, neuroplasticity is less responsive to change with exercise. Another important aspect to consider when interpreting our results is the age of the participants (Table 1). It is well established that neuroplasticity in corticospinal structures tends to decline with aging. 60 It is likely that, besides the effects of stroke, the advanced age of our participants could also have contributed to the small effects that exercise showed to have on the different markers of excitability.
Limitations
We used the GXT to minimize the burden on the patients reducing the number of experimental sessions. However, there was variability in the performance of the GXT among study participants in terms of intensity and time of exercise (Table 1). This variability could have limited our capacity to detect exercise-induced changes in excitability. Exercise protocols with a fixed duration and adjusted to each participant’s individual intensity level could perhaps provide more consistent data. We applied TMS before and after the GXT to determine the effects of high-intensity exercise on excitability. Although the intensities achieved in the GXT and HIIT were very similar (Table 1), due to the differences between protocols, we cannot ensure that the same changes in excitability were elicited with HIIT. It should also be noted that the sample size of the study was small, which could increase the occurrence of type II error, and that most participants had a relatively well preserved upper limb function (Table 1). More studies with individuals with greater impairments will be required to confirm the applicability of this intervention to a broader stroke population.
Conclusions
This study shows that when performed immediately after motor practice, a single bout of HIIT improves skill retention, which could have important implications to accelerate motor recovery in stroke rehabilitation. The results also indicate that one intense bout of cardiovascular exercise (GXT) reduces the interhemispheric imbalances in GABAA-mediated excitability which are common after stroke. 4 However, compared with younger people without disability, the neuroplastic response to acute intense cardiovascular exercise in people with chronic stroke appears to be significantly reduced.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: For this project, MR was supported with funds from the Réseau Provincial de Recherche en Adaptation-Réadaptation (Recherche Clinique), the Canada Foundation for Innovation (John R. Evans Leaders Fund) and the Montreal Centre for Interdisciplinary Research in Rehabilitation (New Investigator Fund). AT was supported by a personnel award from the Heart and Stroke Foundation, Ontario Provincial Office (CS I 7468).