
Abstract
Background. There has been an increasing research interest in upper limb rehabilitation in multiple sclerosis (MS). The current changes in the research field inquire a new literature review. Objective. This systematic review aimed to provide an overview of the upper limb rehabilitation strategies in people with MS (PwMS). Methods. Articles published in PubMed and Web of Knowledge were selected when written in English, published in the past 25 years, peer reviewed, that included at least 5 PwMS, and described the effects of an intervention study including rehabilitation strategies targeting the upper limbs. Included articles were screened based on title/abstract and full text by 2 independent reviewers. Results. Thirty articles met the criteria and were included for data extraction. Only half of the included studies investigated the effects of a training program specially targeted toward the upper limbs, while in the other studies, a general whole body therapy was used. The therapy content and dosage varied greatly between the different included studies. Multidisciplinary and robot-based rehabilitation were the most investigated rehabilitation strategies and showed to improve upper limb capacity. Strength and endurance training improved the upper limb body functions and structures but did not influence the upper limb capacity and performance. Conclusions. The results of this systematic review indicated that different types of upper limb rehabilitation strategies can improve upper limb function in PwMS. Further research is necessary to compare directly the effects of different rehabilitation strategies and to investigate the optimal therapy dosage according to the upper limb disability level.
Introduction
Multiple sclerosis (MS) is a chronic inflammatory and neurodegenerative immune-mediated disease of the central nervous system and is the leading cause of nontraumatic disability in young and middle-aged adults.1,2 People with MS (PwMS) typically present with neurological deficits such as motor and sensory impairments, cerebellar symptoms, fatigue, impaired vision, cognitive deficits, speech and swallowing problems, bladder and bowel disorders, and sexual dysfunction.1,3 According to Kister et al, 4 impaired sensory function (85%), fatigue (81%), impaired hand function (60%), and mobility (50%) were the most frequently reported symptoms in the first year of the disease. A combination of symptoms causes disability, which often hampers the ability to perform activities of daily life (ADL) and social activities, resulting in a decreased quality of life. 5
To date, no single pharmacological treatment is available to cure MS. Current treatment strategies focus on slowing down the disease course in order to maintain the functional status of PwMS by providing pharmacological treatment in combination with (multidisciplinary) rehabilitation. 6 Different literature reviews in MS have indicated the effectiveness of rehabilitation strategies such as exercise training,7-9 physical therapy, 10 occupational therapy,11-13 and multidisciplinary therapy. 14 Remarkably, the studies included in these systematic reviews primarily aimed to improve general or lower limb disability and mainly included ambulatory persons with mild to moderate MS. Rehabilitation research targeting the upper limbs in MS is scarce compared to research targeting the lower limbs in MS and upper limb research performed in other neurological diseases such as stroke.
Upper limb dysfunction is, besides walking disability, fatigue, and cognitive deficits, one of the important dysfunctions present in PwMS. 4 Different studies4,15,16 revealed a high percentage of PwMS reporting upper limb dysfunction, even in the early stage of the disease. More than 50% of 205 PwMS (mean Expanded Disability Status Scale [EDSS] = 3.5, standard deviation [SD] = 2.0) reported impairments or restrictions related to upper limb function, with the highest prevalence of upper limb disability found in the group with a progressive type of the disease. 15 In the study of Johansson et al, 76% of the included 219 PwMS (EDSS range = 0-9.5) had disability in their manual dexterity. 16 Impaired manual dexterity may present bilaterally in large numbers of PwMS.17,18 In addition, Kierkegaard et al found manual dexterity to be an important predictor of overall activity and participation within the community. 19 Upper limb dysfunction in MS contributes to a reduced ability to perform ADL, 18 resulting in decreased independence and quality of life. 5
Due to the impact of upper limb dysfunction on daily life performance, and the positive rehabilitation results in the lower limbs, 20 there is recently an increasing research interest in upper limb rehabilitation in MS. The effects of motor training programs targeting the upper limbs were reviewed by Spooren et al in 2012. 21 Meanwhile, there has been an uprising of new upper limb rehabilitation strategies such as task-oriented training, sensory training, robotics, and technology-supported rehabilitation devices. The current changes in the research field inquire a new systematic literature review including all types of rehabilitation strategies aiming to improve the upper limb function in MS. Therefore, this systematic literature review aimed to provide an overview of the current applied rehabilitation strategies targeting the upper limb and their effects, which may help clinicians select evidence-based rehabilitation strategies for the upper limb function in MS and may guide future research.
Methods
This systematic review was conducted according the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement. 22 The literature search started in February 2015 and ended in April 2015. During the review and writing process (April-June 2015), the literature search was regularly updated. Articles published in the electronic databases (PubMed and Web of Knowledge) were screened using the following string of Medical Subject Headings (MeSH) and keywords: multiple sclerosis AND (upper extremity OR upper limb OR arm) AND (rehabilitation OR exercise OR physical therapy modalities OR upper limb training OR robot assisted therapy OR robotics) NOT (deep brain stimulation OR medication). All selected articles were screened based on title and abstract by 2 independent reviewers (WD and SG). The full text was read when more information was needed to make a decision. In case of doubt, feedback of a third reviewer (IL) was obtained. Articles were included when written in English, published in the past 20 years, peer reviewed, that included at least 5 PwMS, described the effects of an intervention study or a clinical trial including rehabilitation strategies targeting the upper limbs to maintain or enhance the person’s functioning and independency, and included upper limb outcome measures to evaluate the effect of the intervention. Studies investigating the use of cooling equipment, medication, and deep brain stimulation were excluded. Additionally, the reference lists of the included articles were screened for other relevant articles.
Quality Assessment
The risk of bias in the included intervention studies was checked by 2 independent reviewers (IL and AM) using the Physiotherapy Evidence Database (PEDro) checklist.23,24 Disagreement between the 2 reviewers on the methodological quality was resolved through discussion in presence of a third reviewer (DS).
Data Extraction
The following data were extracted by 2 independent raters (IL and AM): study characteristics, descriptive characteristics of the study population, intervention parameters, included upper limb outcome measures and the results of the intervention and/or control group on the upper limb outcome measures. Pre and post values for each upper limb outcome measures, P values describing the differences after intervention within one group, P values describing the pre and post differences between groups, and P values describing the group by time interactions were extracted from the articles. Effect sizes (Hedges’ g′) were established by calculating the difference between the means of an outcome measure at post-intervention and at baseline divided by the pooled standard deviations for that outcome measure multiplied with a factor. 25 Effect sizes were classified according to Cohen’s classification: effect sizes <0.2 were considered small, between 0.2 and 0.5 as moderate, and >0.5 as large. Disagreement regarding data extraction and interpretation was resolved through discussion in presence of a third reviewer (DS).
Results
The systematic literature search resulted in 67 (PubMed) and 140 (Web of Knowledge) articles. After removing the duplicates, 164 articles were retained of which 29 articles met the inclusion criteria (see Figure 1). No additional articles were found after screening the reference lists. One eligible article was published during the writing process of this review and was included as well. Eleven of the 30 included intervention studies were randomized controlled trials (RCT) while other studies were controlled trials (n = 8), crossover studies (n = 4), or case series (n = 7).
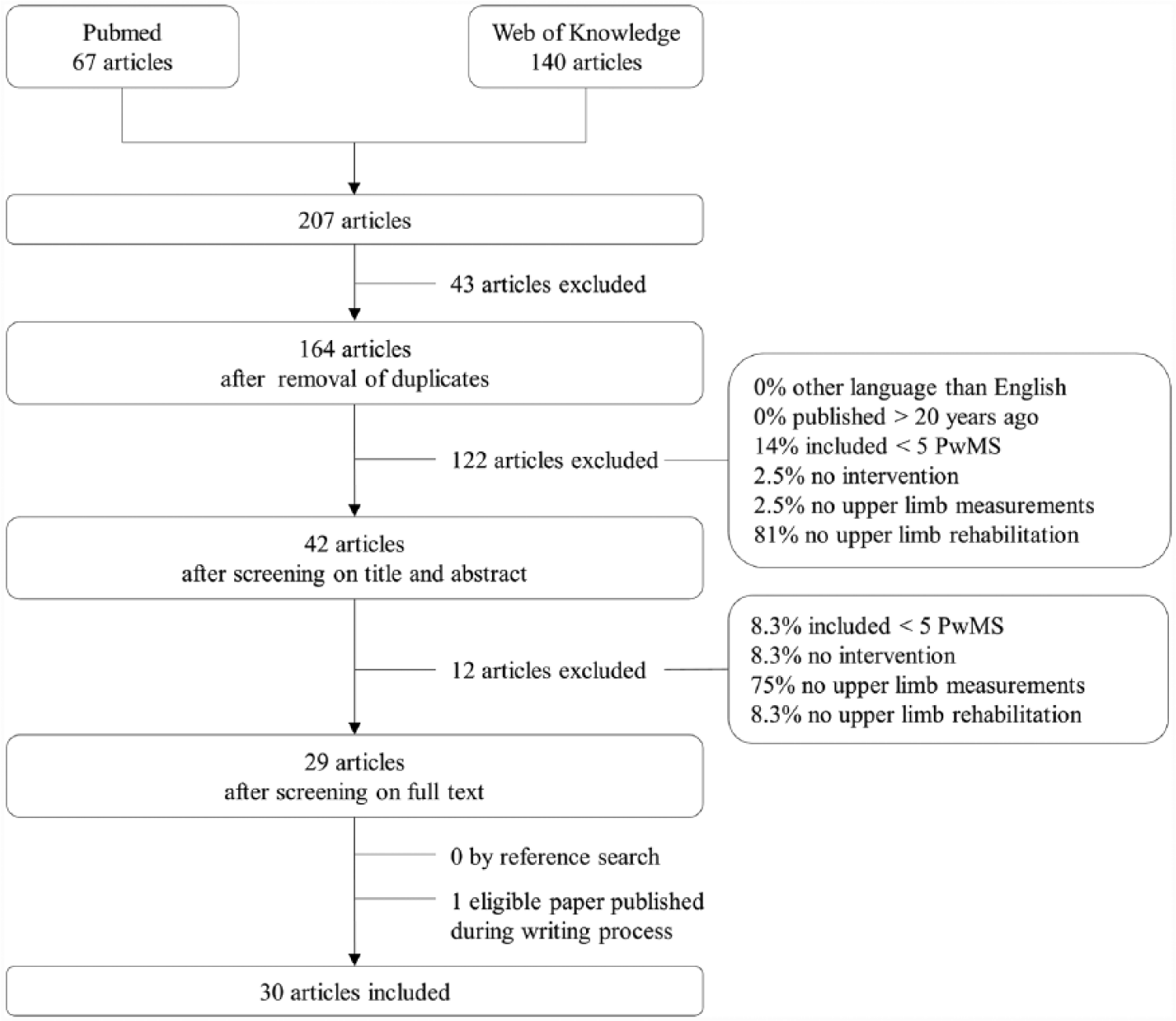
Literature search strategy and results.
Quality Assessment
The results of the quality assessment of the included intervention studies are presented in Table 1. Criteria 1 (eligibility criteria), 9 (intention-to-treat analysis), and 11 (point measures and measures of variability) of the checklist were fulfilled for more than 95% of the studies. The criteria of concealment of allocation (criterion 3) and blinding of subjects and therapist (criteria 5 and 6) were not satisfied in most of the studies. The quality of the included case series was lower compared to those of the controlled trials, whereas only 4 criteria of the checklist (criteria 1, 8, 9, and 11) were satisfied. All identified studies were included in the review for data extraction as they provided information to answer the research question of this review.
Quality Assessment of the Included Studies Using the PEDro Checklist.
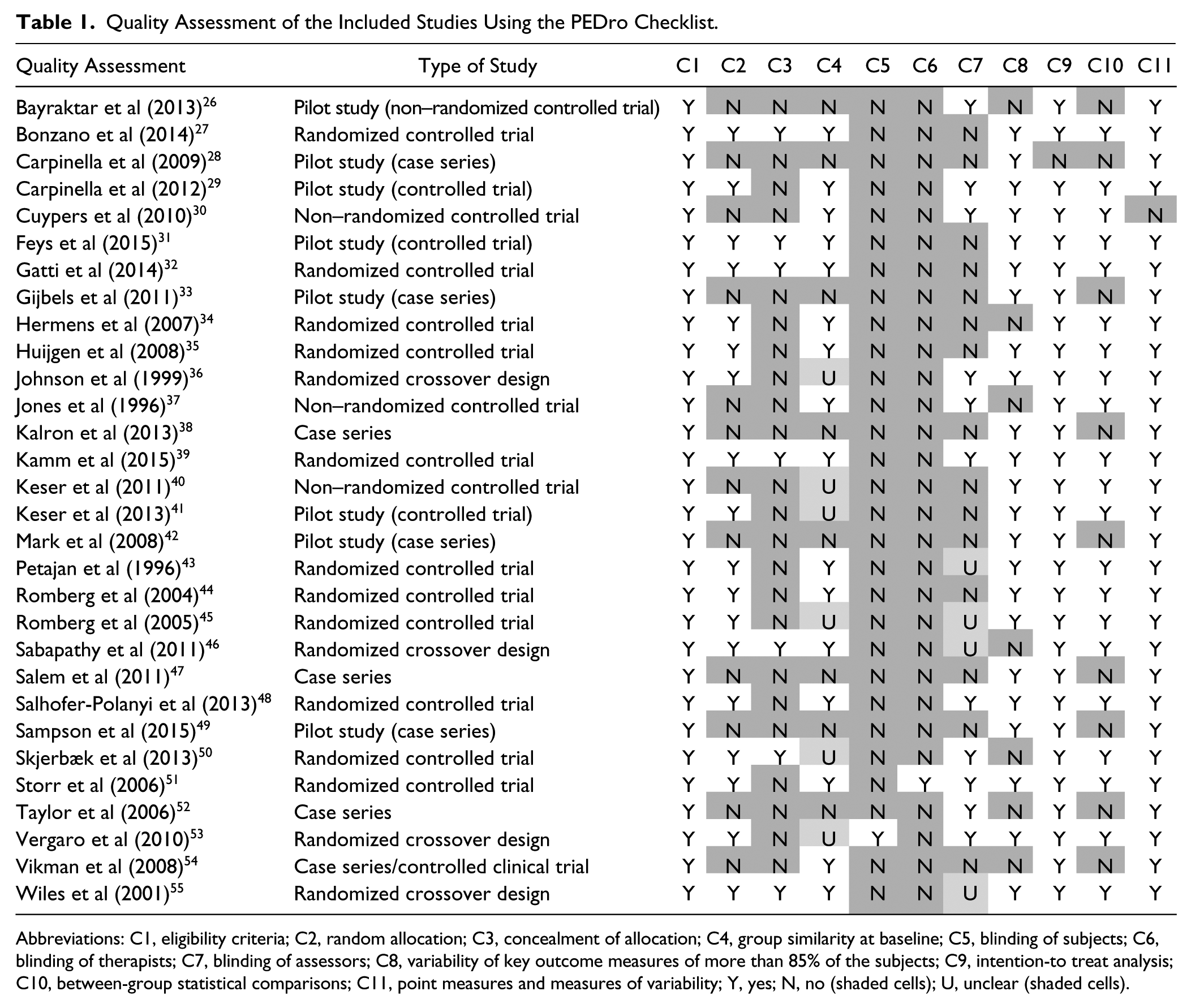
Abbreviations: C1, eligibility criteria; C2, random allocation; C3, concealment of allocation; C4, group similarity at baseline; C5, blinding of subjects; C6, blinding of therapists; C7, blinding of assessors; C8, variability of key outcome measures of more than 85% of the subjects; C9, intention-to treat analysis; C10, between-group statistical comparisons; C11, point measures and measures of variability; Y, yes; N, no (shaded cells); U, unclear (shaded cells).
Data Extraction
The objectives and patient characteristics of the included interventions studies are presented in Table 2. The sample sizes of the included studies ranged from 5 to 95 persons. Twelve studies had a sample size less than 10 PwMS in each group. Dropout was reported in the majority of the included studies. The reasons for dropout were in all cases not related to the intervention (eg, personal reasons, work-related reasons, difficulties with time commitment, and relapse unrelated to the intervention). The mean EDSS of the included participants in the intervention studies ranged from 1 to 8. The average disease duration varied across the included studies and ranged from 1.5 to 25 years. Four out of 30 studies included PwMS with a progressive type of MS, while the majority of the studies included PwMS with different types of MS (relapse remitting, secondary progressive, and primary progressive).
Objectives and Patient Characteristics of the Included Studies a .
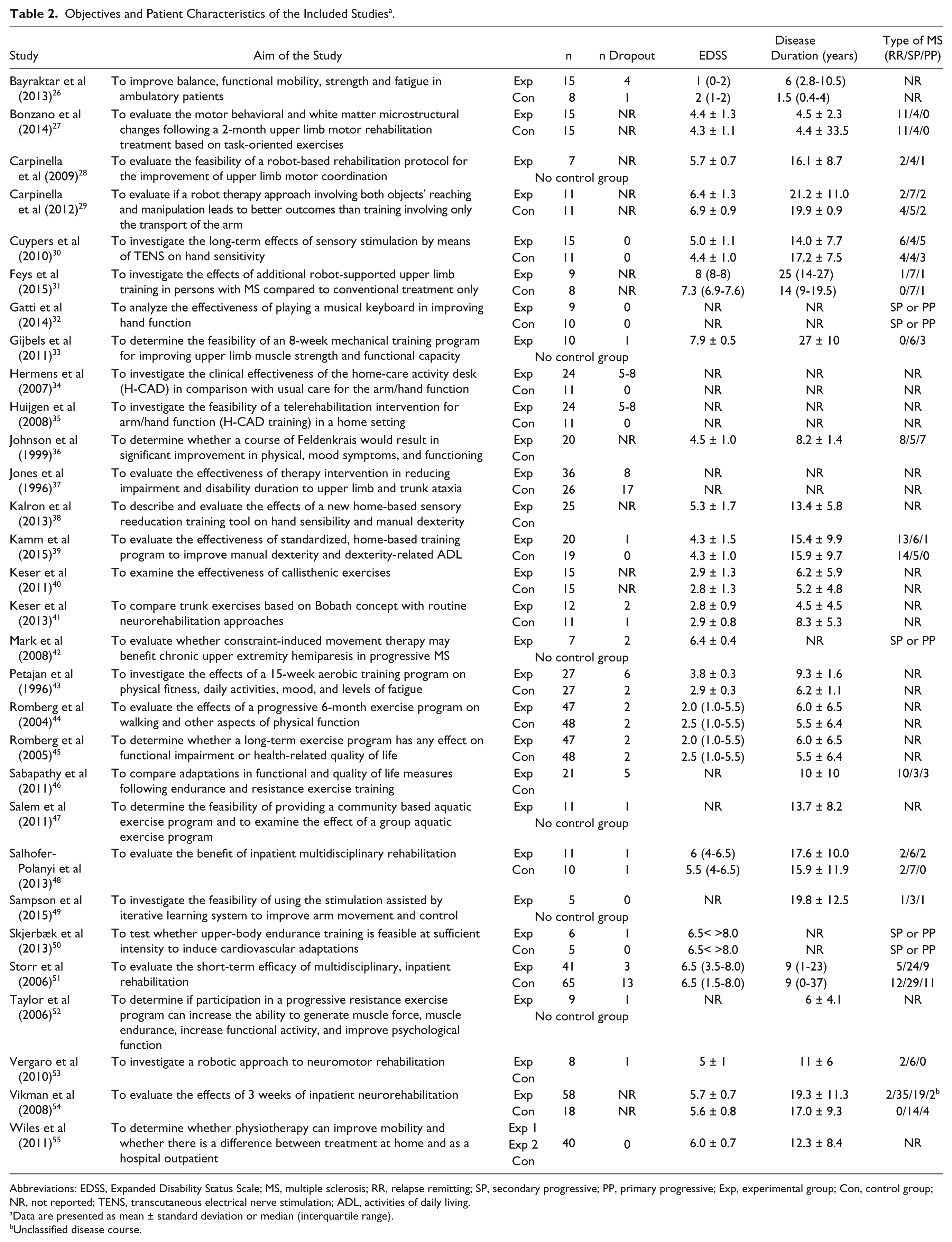
Abbreviations: EDSS, Expanded Disability Status Scale; MS, multiple sclerosis; RR, relapse remitting; SP, secondary progressive; PP, primary progressive; Exp, experimental group; Con, control group; NR, not reported; TENS, transcutaneous electrical nerve stimulation; ADL, activities of daily living.
Data are presented as mean ± standard deviation or median (interquartile range).
Unclassified disease course.
The type of intervention, targeted body parts, and training parameters are shown in Table 3. A large variety of intervention strategies have been investigated in MS ranging from strength and endurance training on body functions and structures level to task-oriented upper limb training on activity level. A pooling and classification of all the included intervention strategies (experimental and control) is provided in Figure 2. The majority of the reported interventions was given individually and supervised (Table 3). The setting of the intervention varied between the included studies (Table 3). Four studies investigated the effects of additional therapy, while in 10 studies the intervention was not given additionally to conventional rehabilitation treatment or routine neurorehabilitation (Table 3). The other half of the included studies gave no information whether the rehabilitation program was given additionally to the conventional treatment. The content of the conventional treatment was in the majority of the studies poorly described, and it is unclear whether the participants received other forms of treatment such as physiotherapy, occupational therapy, cognitive training, speech therapy, or medication. Fifteen of 30 included studies investigated the effects of a training program specially targeted toward the upper limbs alone, while the other half targeted both the upper limbs and the trunk or the lower limbs. Most of the interventions specifically targeting the upper limbs were unilateral training programs, while only 2 studies38,39 included a bilateral training program and 1 study 27 provided a combined unilateral and bilateral training program.
Intervention Details of the Included Studies.
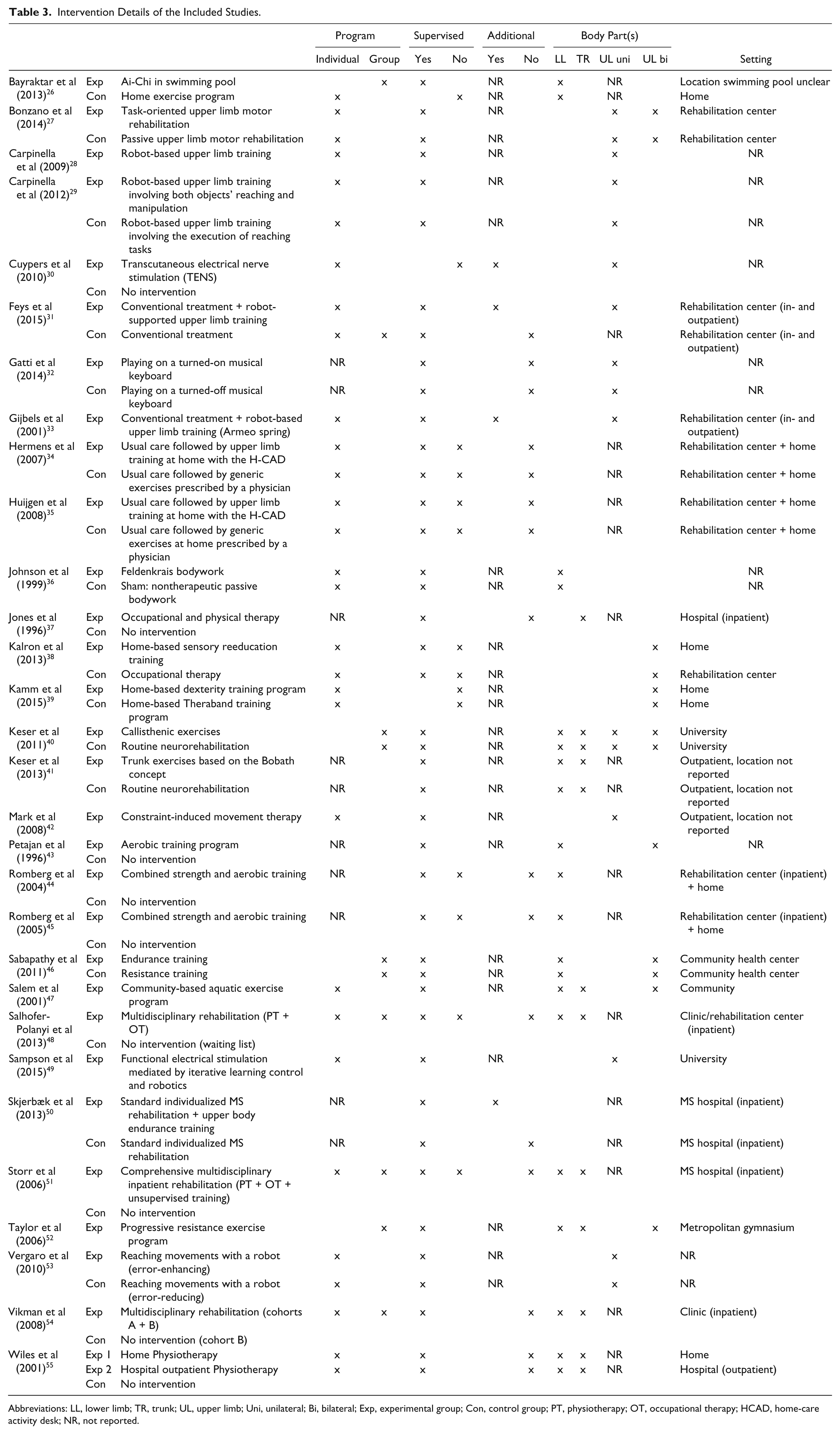
Abbreviations: LL, lower limb; TR, trunk; UL, upper limb; Uni, unilateral; Bi, bilateral; Exp, experimental group; Con, control group; PT, physiotherapy; OT, occupational therapy; HCAD, home-care activity desk; NR, not reported.
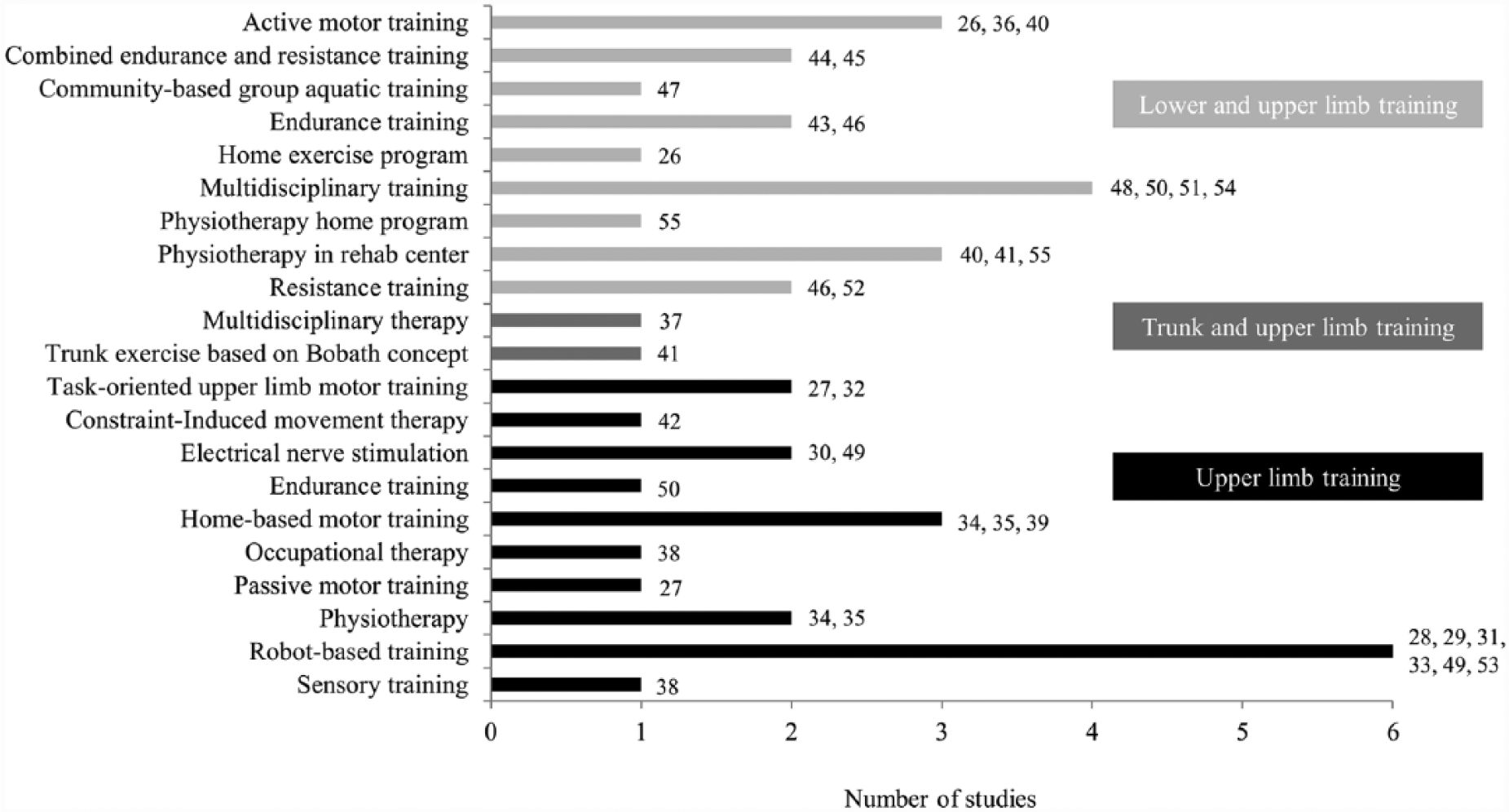
Pooling and classification of all the included intervention strategies (experimental and control interventions).
An overview of the training parameters of each intervention strategy is given in Table 4. The duration of the intervention programs ranged from 1.5 to 26 weeks, with a frequency ranging from 2 to 7 days/week and a session duration of 20 to 60 minutes. As a result, the total amount of training ranged from 240 to 2880 minutes. The intensity of training was only reported in the studies using robot-supported training by reporting the number of movements performed in one training session and in studies using strength and/or endurance training by reporting the number of sets, repetitions, applied resistance in function of the repetition maximum, or the VO2max.
Therapy Dosage Parameters of the Included Studies.
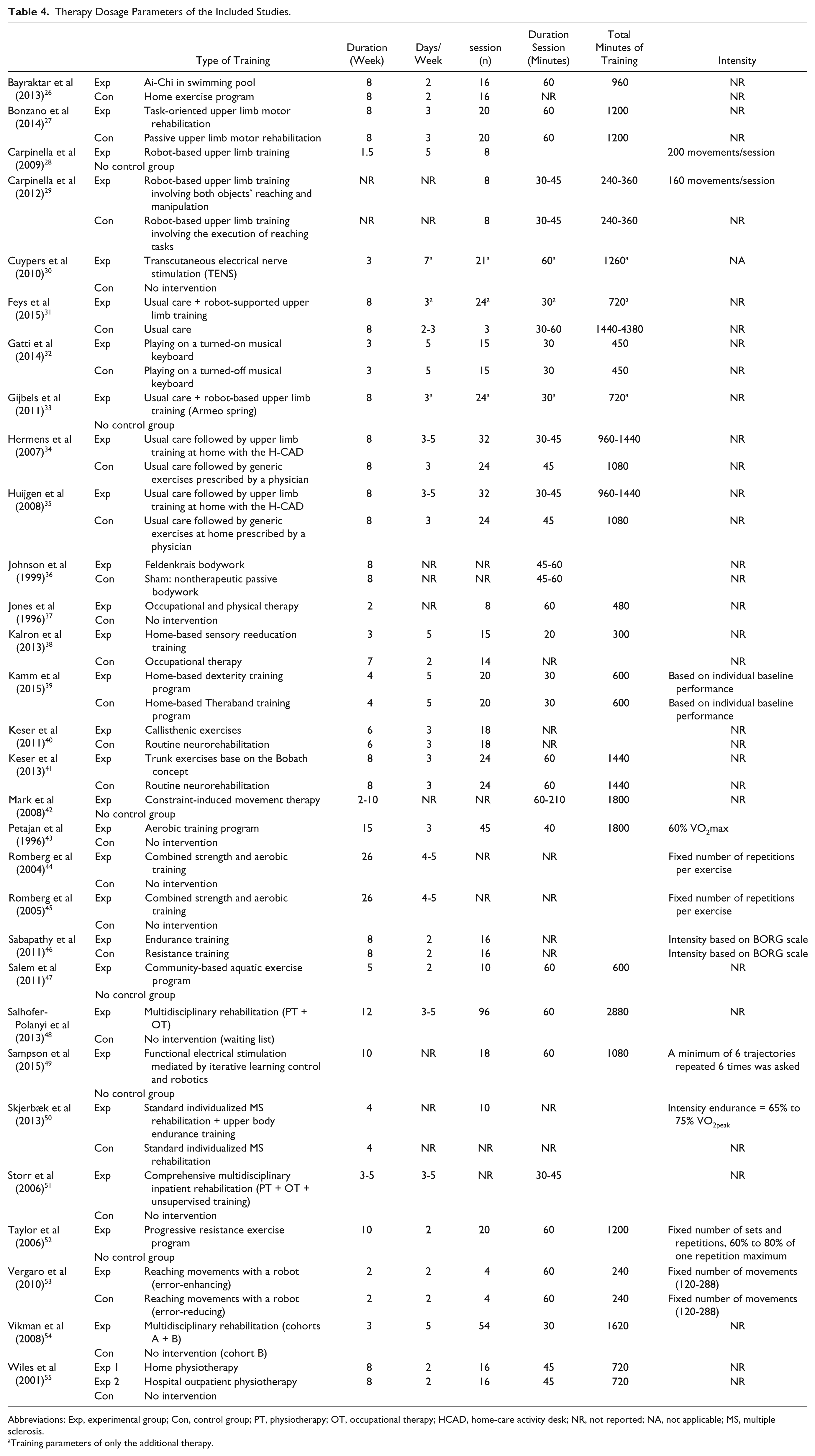
Abbreviations: Exp, experimental group; Con, control group; PT, physiotherapy; OT, occupational therapy; HCAD, home-care activity desk; NR, not reported; NA, not applicable; MS, multiple sclerosis.
Training parameters of only the additional therapy.
Tables 5 to 8 give an overview of the effects of each intervention study by presenting the pre- and postintervention values, P values, and effect sizes. Table 5 gives an overview of the results of studies comparing an experimental intervention strategy with another intervention strategy or sham. Ai-Chi training in a swimming pool, 26 active and passive motor training, 27 robot-based training, 29 playing a music keyboard, 32 and a home-based dexterity training program 39 enhance improvements on body functions and structures level as well on activity level of the International Classification of Functioning (ICF). The effect sizes found for these studies were small to high (range ES = 0.02-1.14).
Data Extraction of Trials Comparing an Experimental Group With Another Intervention Group or a Sham Group a .
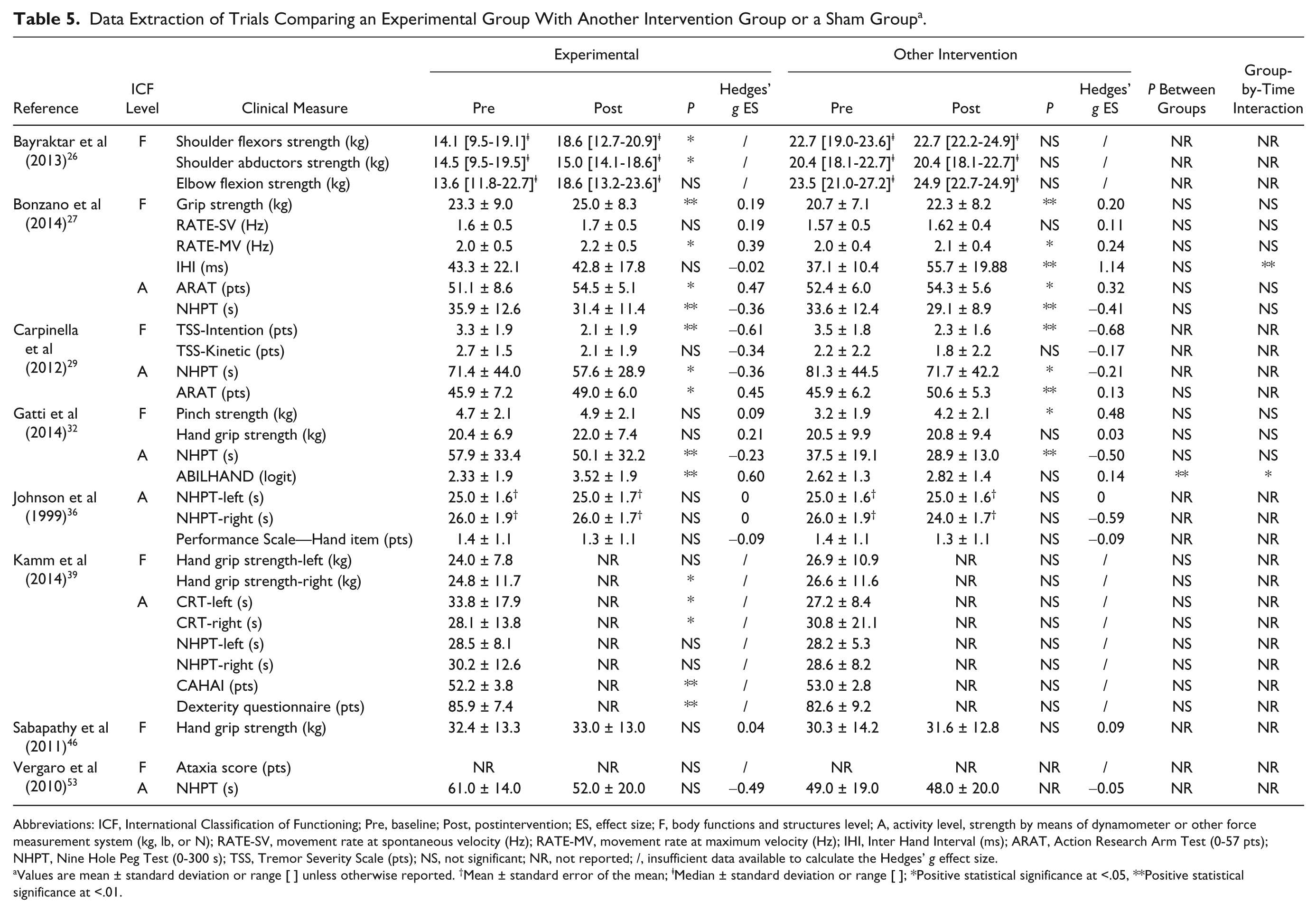
Abbreviations: ICF, International Classification of Functioning; Pre, baseline; Post, postintervention; ES, effect size; F, body functions and structures level; A, activity level, strength by means of dynamometer or other force measurement system (kg, lb, or N); RATE-SV, movement rate at spontaneous velocity (Hz); RATE-MV, movement rate at maximum velocity (Hz); IHI, Inter Hand Interval (ms); ARAT, Action Research Arm Test (0-57 pts); NHPT, Nine Hole Peg Test (0-300 s); TSS, Tremor Severity Scale (pts); NS, not significant; NR, not reported; /, insufficient data available to calculate the Hedges’ g effect size.
Values are mean ± standard deviation or range [ ] unless otherwise reported. †Mean ± standard error of the mean; ⱡMedian ± standard deviation or range [ ]; *Positive statistical significance at <.05, **Positive statistical significance at <.01.
Data Extraction of Trials Comparing an Experimental Group With a Control Group Receiving Conventional Treatment a .
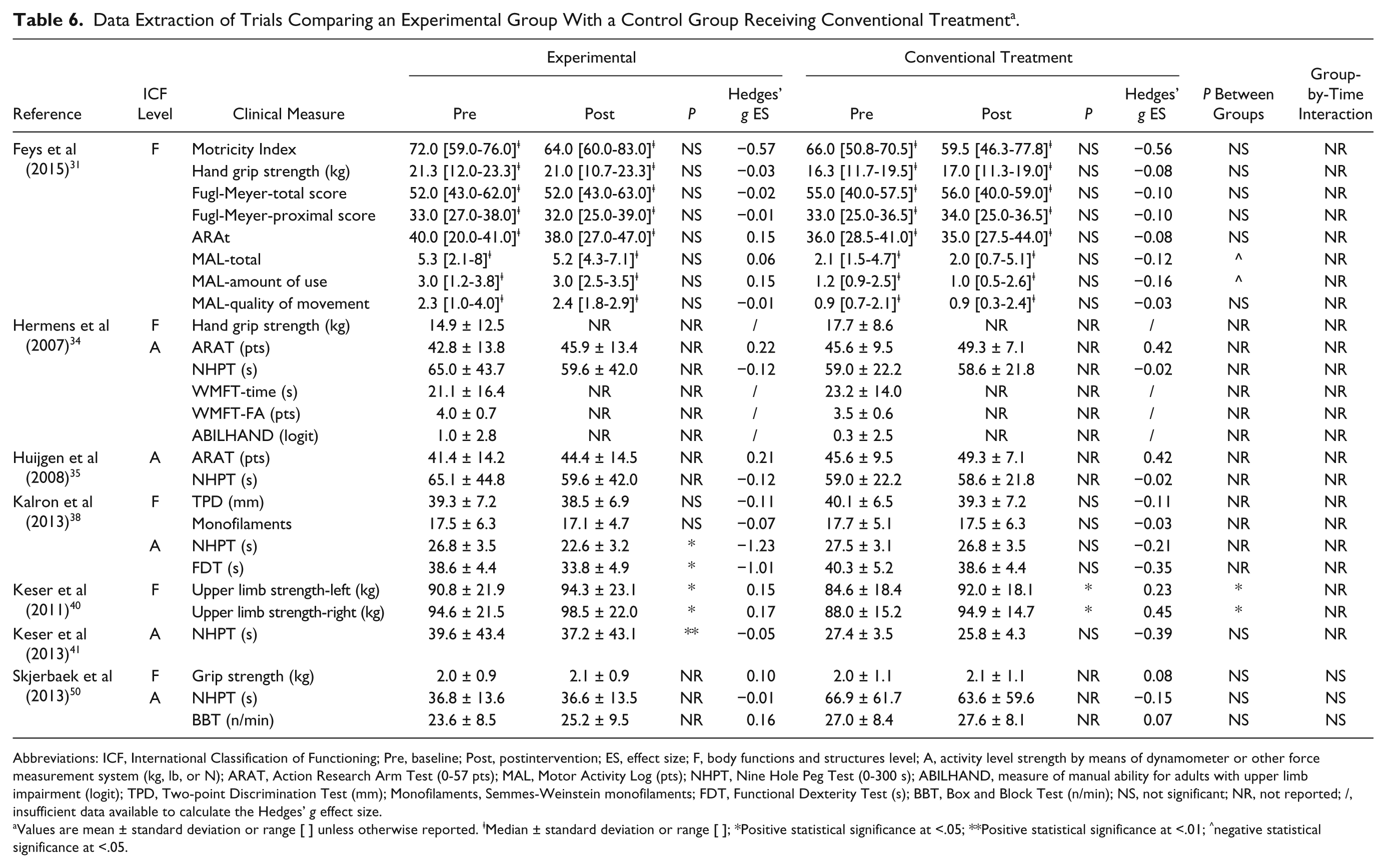
Abbreviations: ICF, International Classification of Functioning; Pre, baseline; Post, postintervention; ES, effect size; F, body functions and structures level; A, activity level strength by means of dynamometer or other force measurement system (kg, lb, or N); ARAT, Action Research Arm Test (0-57 pts); MAL, Motor Activity Log (pts); NHPT, Nine Hole Peg Test (0-300 s); ABILHAND, measure of manual ability for adults with upper limb impairment (logit); TPD, Two-point Discrimination Test (mm); Monofilaments, Semmes-Weinstein monofilaments; FDT, Functional Dexterity Test (s); BBT, Box and Block Test (n/min); NS, not significant; NR, not reported; /, insufficient data available to calculate the Hedges’ g effect size.
Values are mean ± standard deviation or range [ ] unless otherwise reported. ⱡMedian ± standard deviation or range [ ]; *Positive statistical significance at <.05; **Positive statistical significance at <.01; ^negative statistical significance at <.05.
Data Extraction of Trials Comparing an Experimental Group With a Control Group Receiving No Intervention a .
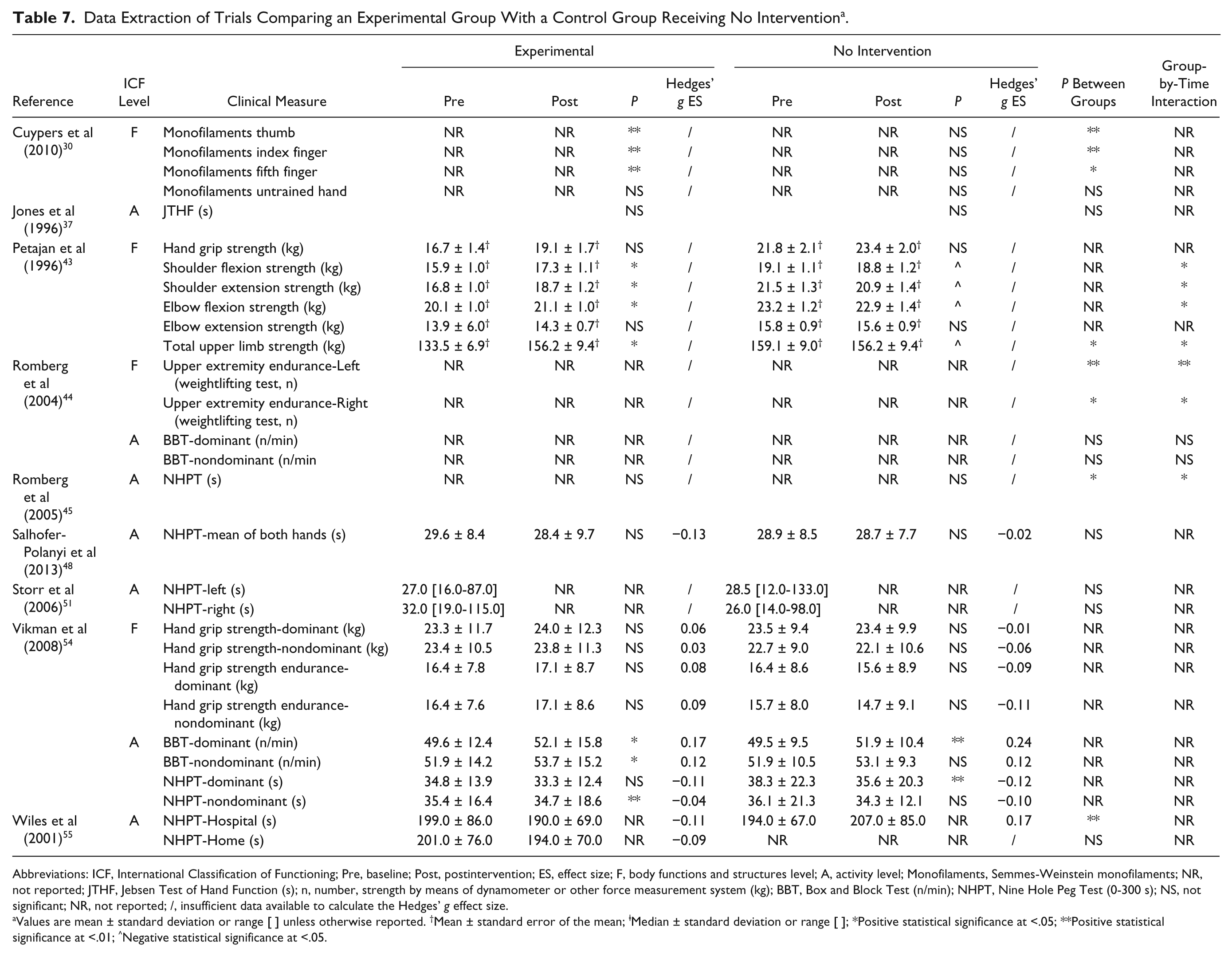
Abbreviations: ICF, International Classification of Functioning; Pre, baseline; Post, postintervention; ES, effect size; F, body functions and structures level; A, activity level; Monofilaments, Semmes-Weinstein monofilaments; NR, not reported; JTHF, Jebsen Test of Hand Function (s); n, number, strength by means of dynamometer or other force measurement system (kg); BBT, Box and Block Test (n/min); NHPT, Nine Hole Peg Test (0-300 s); NS, not significant; NR, not reported; /, insufficient data available to calculate the Hedges’ g effect size.
Values are mean ± standard deviation or range [ ] unless otherwise reported. †Mean ± standard error of the mean; ⱡMedian ± standard deviation or range [ ]; *Positive statistical significance at <.05; **Positive statistical significance at <.01; ^Negative statistical significance at <.05.
Data Extraction of the Uncontrolled Studies a .
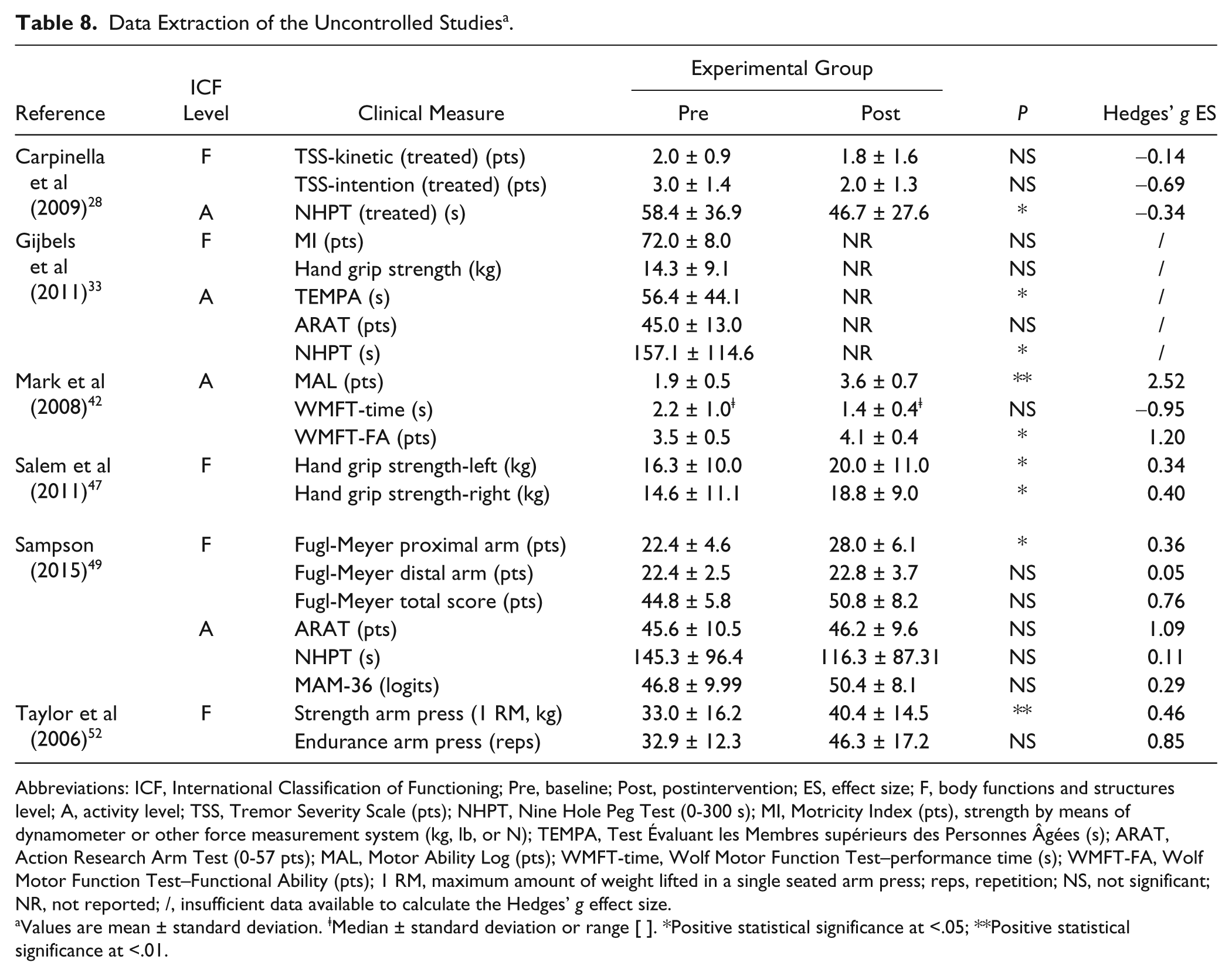
Abbreviations: ICF, International Classification of Functioning; Pre, baseline; Post, postintervention; ES, effect size; F, body functions and structures level; A, activity level; TSS, Tremor Severity Scale (pts); NHPT, Nine Hole Peg Test (0-300 s); MI, Motricity Index (pts), strength by means of dynamometer or other force measurement system (kg, lb, or N); TEMPA, Test Évaluant les Membres supérieurs des Personnes Âgées (s); ARAT, Action Research Arm Test (0-57 pts); MAL, Motor Ability Log (pts); WMFT-time, Wolf Motor Function Test–performance time (s); WMFT-FA, Wolf Motor Function Test–Functional Ability (pts); 1 RM, maximum amount of weight lifted in a single seated arm press; reps, repetition; NS, not significant; NR, not reported; /, insufficient data available to calculate the Hedges’ g effect size.
Values are mean ± standard deviation. ⱡMedian ± standard deviation or range [ ]. *Positive statistical significance at <.05; **Positive statistical significance at <.01.
Table 6 gives an overview of the results of studies comparing an experimental intervention strategy with conventional treatment. Significant improvements were found for the experimental groups in the studies of Kalron et al 38 and Keser et al,40,41 who compared the effects of a home-based sensory reeducation program, callisthenic exercises, and trunk exercises based on the Bobath concept with the effects of conventional treatment. The effect sizes were small to high (range ES = 0.05-1.23), with the highest effect sizes found in the study of Kalron et al. 38 Only in the study of Keser et al 40 a significant improvement after conventional treatment was found, while in the study of Feys et al 31 a significant decrease was found in the perceived performance measure after conventional treatment.
The overview in Table 7 shows that 5 of the 9 studies30,43-45,54 investigating the effects of training compared to no intervention reported significant improvements after the intervention. PwMS receiving no intervention did not improve or even significantly decreased in their upper limb strength. 43 The uncontrolled cases series showed that robot-based upper limb training,28,31 constraint-induced movement therapy, 42 aquatic exercises, 47 and progressive resistance training 52 induce improvements with low to high effect sizes on body functions and structures level as well on activity level.
Only 3 studies30,33,42 included follow-up measurements in their study design and reported long-term improvements after 3, 30 4, 42 and 8 33 weeks posttraining on sensory function, 30 upper limb capacity, 33 and performance. 42
Discussion
This systematic review provided an overview of the current applied upper limb rehabilitation strategies and their effects. Surprisingly, only half of the included studies consisted of a training program that specially targeted the upper limbs alone, while the other half targeted both the upper limbs and the trunk or the lower limbs. Despite the low number of included studies, the results of this review suggest that upper limb rehabilitation can improve upper limb function in PwMS. Although it is impossible to provide guidelines due to the diversity in therapy content and dosage, findings and suggestions regarding therapy content and therapy dosage are discussed in more detail within this discussion.
Therapy Content
This review shows that a large number of different rehabilitation strategies have been applied to improve the upper limb function in PwMS ranging from resistance and endurance training on body functions and structures level to task-oriented training on activity level. Robot-based upper limb training and multidisciplinary rehabilitation were the most frequently investigated rehabilitation strategies in the literature. Together with task-oriented training, the latter rehabilitation strategies were also the most recently investigated strategies, which matches their popularity in other neurological diseases such as stroke. 56 The majority of the included studies trained only the dominant or the most impaired upper limb despite the fact that a large number of ADL are performed bilaterally. Only 3 studies, with most of them recently published, paid more attention toward bilateral training of the upper limbs. Recently, evidence for bilateral training in MS was given by Bertoni et al, who found that 75% of the PwMS have bilaterally impaired manual dexterity, even in an early stage of the disease. 17 In addition to these findings, we found that the majority of the reported interventions was given individually and was supervised. None of the included studies investigated whether this approach had more beneficial effects compared to group training or unsupervised training and whether there is a difference in the cost-effectiveness. Furthermore, it is difficult to draw conclusions regarding the setting of the intervention (eg, outpatient, inpatient, community or home-based) as the approaches varied between the different included studies.
Regarding the effects of the rehabilitation strategies, we saw that the majority of the intervention studies reported improvement of the upper limb function on the same ICF level as the rehabilitation strategy that it focused on. For example, resistance and/or endurance training seem to improve upper limb strength43,52 and endurance 44 on body functions and structures level, while task-oriented training,27,32 constraint-induced movement therapy, 42 and some types of robot-supported training28,29,33 focused on activity level and thus improved capacity and performance on activity level. Sensory training30,38 in turn seemed to improve sensory function in the hand on body functions and structures level and upper limb capacity on activity level. In summary, these findings indicate the importance of selecting a training program in function of the desired improvements (eg, resistance training to improve strength or task-oriented training to improve upper limb capacity and performance in daily life). Remarkably, only 3 studies reported upper limb improvements after conventional 40 and multidisciplinary54,55 treatment. The lack of sufficient evidence for conventional and/or multidisciplinary treatment may be due to the fact that it does not target the upper limbs exclusively. Furthermore, the content of these types of treatment was in the majority of included studies poorly described and there was no information available on how much attention was given toward the upper limbs. Therefore, it is difficult to draw conclusions regarding the effects of experimental interventions over conventional treatment in PwMS. Furthermore, based on the rather limited amount of well-designed studies with small sample sizes, it is difficult to give recommendations regarding the optimal therapy content for PwMS.
Furthermore, the variety of patient characteristics, the different upper limb disability levels of the included patients and the use of the different outcome measures makes it difficult to compare the results between the included studies. The current rehabilitation studies included PwMS with a variety of upper limb disability or mainly PwMS with a relatively preserved upper limb function as suggested by the different baseline values reported in Tables 5 to 8. In our opinion, it is important to differentiate between PwMS with different disability levels as they present with different impairments and report other limitations on activity level. 17 It is, for example, unlikely that PwMS with different upper limb disability levels will improve to a similar extent after the same rehabilitation intervention.
In summary, more studies comparing the effects of different upper limb rehabilitation strategies in PwMS with different upper limb disability levels are needed to specify clear recommendations regarding upper limb rehabilitation in PwMS.
Therapy Dosage
The importance of therapy dosage, including training duration, frequency of training sessions, duration of a single training session, and intensity of training, has been indicated in people after a stroke. A recent literature study concluded that there is a positive relationship between the total therapy time and therapy outcomes. 57 In MS, there is currently no attention for the therapy dosage of upper limb rehabilitation. The majority of the included studies had an intervention duration of 8 weeks or more. The frequency of training ranged from 2 to 5 days per week while the duration of a training session ranged from 30 to 60 minutes. Intensity of training was rarely reported, except in the studies using robot-supported training, strength, and/or endurance training as these types of intervention allowed controlling of and documentation of the number of repetitions and training intensity. However, as shown in stroke, also the intensity of task-oriented upper limb training or home-based training could be monitored and controlled in future research by using accelerometers. 58
In none of the included studies, background reasons regarding the selection of the therapy dosage was given. It is, however, unclear whether the interventions would have the same results with a lower therapy dosages or better results if the PwMS had received a higher therapy dosage. Furthermore, it is unknown whether the relationship between therapy dosage and therapy outcome would be the same in all disability levels and which therapy dosage parameters are important (eg, training duration, frequency of training, intensity of training). It could be, for example, that PwMS in a more advance disease stage and with marked upper limb dysfunction or PwMS with a progressive type of MS cannot perform a high-intensity training due to decreased physical fitness, potential presence of motor fatigue, and reduced neural reserves. In addition, one may hypothesize that those PwMS may benefit from a longer training duration at low intensity to obtain some effects. Future research should aim to investigate the effects of therapy dosage parameters in PwMS with different upper limb disability levels and different types of MS as it is already shown to play an important role in other neurological diseases. 57
Recommendations for Future Research
Besides the need for RCTs with large sample sizes investigating therapy content and dosage in PwMS, there is a need for studies investigating whether reported improvements by the current intervention studies are caused by improvements of disuse or neuroplasticity or by a combination of both factors. It is sometimes difficult to decide whether to focus on preventive, restorative, or compensatory treatment strategies or to provide a combination in PwMS. One may inquire which type of the latter strategies would be more beneficial in PwMS at different stages of the disease. To answer this question, it is important that future RCTs categorize their included PwMS according to their upper limb disability level and include appropriate clinical, self-reported, physiological, and neuroimaging outcome measures. Recommendations regarding the use of clinical and self-reported upper limb outcome measures were recently published and may help in the selection of appropriate outcome measure for future RCTs.59,60 Guidelines regarding the use of physiological and neuroimaging outcome measures are currently lacking. To date, only one study has already included neuroimaging measures and found that task-oriented upper limb training positively affected the white matter architecture in PwMS. 27 Furthermore, there is a need for studies investigating the effects of upper limb rehabilitation in PwMS with a progressive type of MS, as effective disease-modifying drugs are not available for them. 61 In this review, we only found 4 studies32,33,42,50 investigating specifically the effects of upper limb rehabilitation in PwMS with progressive type of MS. In addition, besides interventions studies targeting the upper limbs in MS, well-designed longitudinal studies describing the natural course of upper limb dysfunction in MS are lacking. These studies may probably provide new and more insights regarding upper limb dysfunction in MS, which can be used to further improve rehabilitation strategies. Last, we recommend using the Template for Intervention Description and Replication checklist and guide when reporting the results of interventions studies. 62 The use of the checklist and guide will improve the completeness of reporting and ultimately the replicability of interventions as sometimes important information was missing in the published intervention studies.
Study Limitations
No meta-analysis was performed as the methodological quality of the included studies varied from low to high with only 11 RCTs out of the 30 included studies. The other included studies were controlled trials, crossover studies, or cases series that received lower scores on the PEDro checklist and thus a lower level of evidence. The criteria of the PEDro checklist such as concealment of allocation and blinding of subjects and therapist were in most of the studies not satisfied. The latter is often not feasible in rehabilitation studies. Despite the low methodological quality and the relatively low sample sizes of some of the included studies, we decided to include them for the data extraction performed in this systematic review as they still provided information and insights in the effects of upper limb rehabilitation in MS. A second reason why no meta-analysis was performed was that the included studies used different outcome measures, different type of intervention strategies, and included patients with different disability level, which makes it difficult to cluster and compare the studies. However, we provided ES to indicate the magnitude of change in the different studies.
Conclusions
The results of this systematic review indicated that different types of upper limb rehabilitation strategies can improve upper limb function in MS. Further research is necessary to compare directly the effects of different rehabilitation strategies and to investigate the optimal therapy dosage taken for the upper limb disability of the PwMS into account.
Footnotes
Acknowledgements
We would like to acknowledge all the authors of the included articles who provided us with additional data to perform the data analysis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.