
Abstract
Background. Paresis in stroke is largely a result of damage to descending corticospinal and corticobulbar pathways. Recovery of paresis predominantly reflects the impact on the neural consequences of this white matter lesion by reactive neuroplasticity (mechanisms involved in spontaneous recovery) and experience-dependent neuroplasticity, driven by therapy and daily experience. However, both theoretical considerations and empirical data suggest that type of stroke (large vessel distribution/lacunar infarction, hemorrhage), locus and extent of infarction (basal ganglia, right-hemisphere cerebral cortex), and the presence of leukoaraiosis or prior stroke might influence long-term recovery of walking ability. In this secondary analysis based on the 408 participants in the Locomotor Experience Applied Post-Stroke (LEAPS) study database, we seek to address these possibilities. Methods. Lesion type, locus, and extent were characterized by the 2 neurologists in the LEAPS trial on the basis of clinical computed tomography and magnetic resonance imaging scans. A series of regression models was used to test our hypotheses regarding the effects of lesion type, locus, extent, and laterality on 2- to 12-month change in gait speed, controlling for baseline gait speed, age, and Berg Balance Scale score. Results. Gait speed change at 1 year was significantly reduced in participants with basal ganglia involvement and prior stroke. There was a trend toward reduction of gait speed change in participants with lacunar infarctions. The presence of right-hemisphere cortical involvement had no significant impact on outcome. Conclusions. Type, locus, and extent of lesion, and the loss of substrate for neuroplastic effect as a result of prior stroke may affect long-term outcome of rehabilitation of hemiparetic gait.
There is accumulating evidence that deep white matter lesions damaging corticospinal and corticobulbar pathways are the predominant and, in many cases, exclusive cause of paresis after stroke.1 -12 This is particularly clear in the case of lower-extremity paresis because, with the exception of the rare anterior cerebral artery (ACA) distribution stroke, the portion of the motor cortex supporting lower-extremity function is completely spared. Deep white matter lesions appear to play a crucial role in the genesis of paresis, whether the lesion is an infarct or a hemorrhage, whether the infarct is large vessel or lacunar, and whether the lesion locus is cerebral or brainstem. A reasonable conclusion, therefore, is that recovery of paresis after stroke predominantly reflects the impact on the neural consequences of the white matter lesion by the combination of reactive neuroplasticity (reflecting mechanisms of spontaneous recovery) and experience-dependent neuroplasticity, driven by rehabilitation treatment and daily experience. Nevertheless, the potential impact of lesion type, involvement of the basal ganglia, side of lesion, and the presence of premorbid ischemic demyelination or stroke on recovery of function have not been adequately defined. This is the focus of the present investigation.
The Locomotor Experience Applied Post-Stroke (LEAPS) trial was a prospective, randomized, parallel group, phase III trial of 2 physical therapy interventions directed at improving functional walking ability in 408 patients, 2 months or 6 months poststroke, as measured at 1 year poststroke.13,14 The 2 interventions were body-weight-supported treadmill training along with overground training performed in a rehabilitation center and impairment-based strength and balance training performed in the participant’s home. Imaging studies were available in 391 of the 408 participants in the trial, and the scan defined the responsible lesion in 360 participants. These data provide the basis for the present analysis. We sought, in a series of regression models, to test the following hypotheses:
Hypothesis 1. Because damage to the descending corticospinal tract and corticobulbar tracts (corticoponto-reticulospinal, corticomedullary-reticulospinal, and cortico-vestibulospinal) appears to be largely responsible for lower-extremity paresis under all circumstances except for the rare ACA territory stroke, stroke type (large vessel, lacunar, or hemorrhagic), locus, and extent should have no differential effect on outcome when ACA territory strokes are excluded and baseline severity of paresis is a control parameter. Alternatively, it might be reasoned that hemorrhages, by virtue of the toxic effects of hemoglobin products, might adversely affect neuroplasticity. Population-based studies of rehabilitation outcomes report no difference between patients with hemorrhages and patients with infarcts; however, in studies of patients judged to be good rehabilitation candidates, those who have experienced hemorrhages ultimately demonstrate better outcomes, even though they are, on average, more severely impaired at onset. 15 On the other hand, when the time course of recovery is examined, it seems that over the first 10 weeks poststroke, patients with hemorrhages do demonstrate faster recovery, but thereafter, between 10 and 26 weeks, patients with infarcts tend to demonstrate a steeper recovery curve. 16 It is during this 10- to 26-week epoch that the toxic effects of blood products, such as free iron, may generate free radicals and inflammatory cytokines. 17
Hypothesis 2. Damage to the basal ganglia may affect the function of the cerebral cortex (particularly motor and premotor cortex and the supplementary motor area [SMA]), to which basal ganglia output is projected via the thalamus. 18 Extensive infarction of the basal ganglia, particularly the putamen, as a result of occlusion of the proximal (M1) portion of the middle cerebral artery, causing striatocapsular infarction, may therefore have a negative effect on cortical neuroplasticity, and hence, recovery of function and response to therapy. On the other hand, projections from vetrolateral nucleus pars oralis (VLo) and ventral anterior nucleus (VA) nuclei of the thalamus, the major recipients of basal ganglia efferent fibers, ascend through the posterior limb of the internal capsule and into the corona radiata at approximately the same location 19 as descending corticospinal/corticobulbar fibers. 20 This being the case, basal ganglia infarction might have no additional negative impact on motor recovery.
Hypothesis 3A. Patients with right-hemisphere large-vessel-distribution infarcts are more likely to have hemispatial neglect 21 and commonly associated anosognosia (denial or unawareness) 22 or anosodiaphoria (indifference—not well studied) for hemiparesis. In the study by Pedersen et al, 21 23% of 602 acute patients with acute stroke had hemispatial neglect, and in 85% of these, the lesion was in the right hemisphere. Prevalence of anosognosia is 32% at 3 days poststroke, 18% at 1 week poststroke, and 5% at 6 months poststroke. 23 Hemispatial neglect24 -32 and anosognosia33,34 have been linked in many studies to longer hospital stays, reduced likelihood of returning to independent living, lower scores on measures of functional recovery, and poorer rehabilitation outcomes. One very-high-quality study that adequately controlled for baseline motoric impairment failed to replicate this finding, 21 but the measure of hemispatial neglect used may not have been sufficiently comprehensive. Most of these studies have reported impact on outcome at the end of rehabilitation, but several have reported impact at up to 1 or even 2 years poststroke.24,26,28,31,32,35 Therefore, participants with right-hemisphere large-vessel-distribution infarcts might be expected, on average, to demonstrate less gain with treatment than participants with left-hemisphere cortical lesions.
Hypothesis 3B. Furthermore, because walking was not part of the home-based LEAPS therapy, it might be anticipated that recipients of this therapy would show lesser gains in walking speed because they were presumably left on their own to a greater extent in any walking they did. This would lead to a Side × Therapy type interaction effect.
Hypothesis 4. Patients with large-vessel-distribution strokes, particularly on the right side, often have a distorted sense of the postural vertical, which is uniformly perceived as tilted toward the side contralateral to the lesion.36,37 Contralesional deviation of the postural vertical is strongly associated with lateral pulsion and, when severe, is associated with the “pusher syndrome,” in which patients strongly tilt themselves against resistance as they seek to align their body axis with their own perception of the true vertical. There is a strong association between disordered perception of the postural vertical and hemispatial neglect, 38 but the relationship between this syndrome and anosognosia and anosodiaphoria is unknown. In our study of predictors of treatment response in the LEAPS trial, we found that poor balance at baseline, as measured by the Berg Balance Scale (BBS), 39 was predictive of less improvement in walking. 40 Therefore, to the extent that lateral pulsion contributes to poor balance and is more prevalent with right-hemisphere strokes, there may be a hemispheric difference in treatment outcome.
Hypothesis 5. Leukoaraiosis, presumably in our population reflecting ischemic demyelination, will have a negative impact on recovery, either by its effect on alternative ipsilesional pathways (eg, pathways from the premotor cortex, SMA, and cingulate motor areas), uncrossed contralesional pathways, connectivity between the SMAs on the 2 sides, or recrossing pathways at the level of the spinal cord from the contralesional side. Worse outcome after acute hospitalization, defined by the modified Rankin Scale score, has been correlated with severity of leukoaraiosis. 41
Hypothesis 6. Given that lesions from prior large-vessel-distribution strokes were focal, and LEAPS excluded those with residual neurological deficits from old strokes, the presence of prior strokes should not affect outcome.
In all our analyses, we controlled for severity of impairment, as measured by gait speed at baseline (2 months poststroke), and age, and in all but one, we controlled for baseline BBS score. Age and BBS score were found to be the major predictors of outcome (12-month walking speed) in our prior analysis. 40 Given the evidence of the particular impact of right-hemisphere cortical lesions on perception of the postural vertical, our testing of Hypothesis 4 included analysis without BBS score as a covariate.
Methods
Study Design
The LEAPS trial was a multicenter, single-blind, randomized controlled trial targeting adults who had hemiparesis, as a result of a stroke, severe enough to require inpatient rehabilitation, followed by discharge home. 14 Participants had to be able to walk 10 feet with no more than 1-person assistance and to have a self-selected 10-m walking speed of less than 0.8 m/s. They were stratified by walking impairment level at 2 months after onset of stroke (severe, <0.40 m/s; moderate, 0.40 to <0.80 m/s). Interventions were the following: (1) a progressive, task-specific locomotor training program (LTP) that included walking on a treadmill with partial body weight support and overground practice and (2) a progressive strength and balance exercise program delivered in the home—that is, a home exercise program (HEP). LTP and HEP were delivered at 2 months (early) poststroke in addition to usual care. A delayed LTP group received the intervention at 6 months poststroke. Participants were randomized 2 months poststroke to the 3 protocol intervention groups: early LTP, late LTP, and HEP (proportions 7:7:6). Contrary to our original hypothesis, the task-specific LTP program provided early or late was not superior in improving 1-year walking speed compared with the impairment-targeted HEP exercise program, and early LTP was not superior to late LTP. With both interventions, more than 50% of the study population improved walking ability at 1 year, as defined by a transition to a higher functional walking level, regardless of severity of impairment. These results enabled us to use data from all the LEAPS participants who had diagnostic images in the present study.
The LEAPS protocol has been reported. 13 Ethics review boards at all participating centers approved the protocol. All participants provided written informed consent. An independent medical monitor and a data safety monitoring board appointed by the National Institutes of Health oversaw the conduct, safety, and efficacy of the trial and monitored adverse events. The 12-month primary outcomes have been reported. 14
Interventions
The LTP and HEP programs were controlled for exercise frequency (90-minute sessions, 3 times per week) and duration (12 to 16 weeks), for a total of 30 to 36 exercise sessions. LTP included stepping on a treadmill with partial body weight support for 20 to 30 minutes at 2.0 mph, with manual assistance as needed, followed by a progressive overground walking program sustained for 15 minutes provided by a physical therapist and rehabilitation technician(s) (0-2) in the clinic. HEP included progressive flexibility, joint range of motion, upper- and lower-extremity strength, coordination, and static and dynamic balance exercises provided by a physical therapist in the home. In addition to the LTP and HEP interventions, all participants were allowed to receive any prescribed usual and customary care during the intervening periods.
Lesion Definition
Brain imaging studies (computed tomography [CT], 127; magnetic resonance imaging [MRI], 264) were available for 391 participants. All imaging studies had been obtained pursuant to the acute clinical care of the participants. Interpretation of MRI scans was based on fluid-attenuated inversion recovery sequences, in most cases supplemented by diffusion-weighted images. We did not document whether or not MRIs included diffusion-weighted image sequences.
Images failed to demonstrate a lesion in 31 participants, and 12 participants had ACA territory infarcts, leaving 348 who provided the basis for the present analysis. Each image was read by 1 of the 2 neurologists on the study (BD, SEN) using a standard template (Table 1). Lacunes were defined as deep infarcts, roughly the shape of inverted cones, tracking a single vessel (usually a lenticulostriate artery) through multiple axial cuts, typically <1.5 cm in maximal axial diameter. Mild leukoaraiosis was defined as up to several 2- to 3-mm diameter lesions in the deep or periventricular white matter. Moderate leukoaraiosis was defined by multiple white matter lesions, up to several millimeters in diameter, but none confluent except in the region posterior to the atria of the lateral ventricles. Severe leukoaraiosis was defined by multiple white matter lesions, many up to several millimeters in diameter, with multiple regions of confluence. Prior large-vessel-distribution stroke was defined by imaging abnormalities indicative of infarction in the territory of a named cerebral artery or one or more of its branches. Potential LEAPS participants who had residual motor deficits relatable to prior stroke were excluded, thereby minimizing the number of participants who had preexistent lesions of motor pathways. Prior lacunar infarctions were not assessed in this study, and their existence was only relevant to the extent of their association with leukoaraiosis.
Image Interpretation Template.
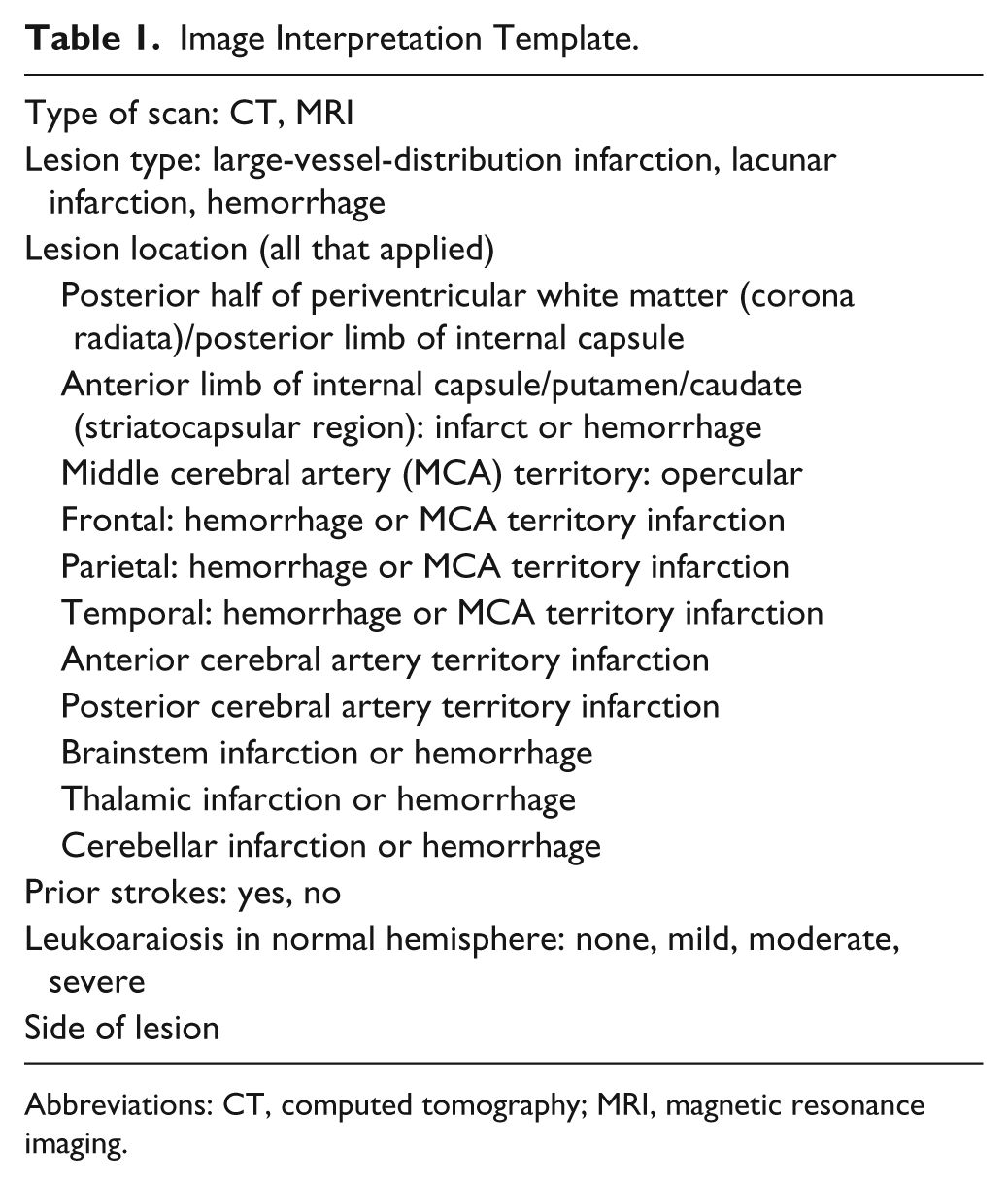
Abbreviations: CT, computed tomography; MRI, magnetic resonance imaging.
Statistical Analysis
We tested our hypotheses using a series of general linear models. For all models, the dependent variable was change in self-selected walking speed from 2 months to 1 year poststroke. All models but one (see below) included age, baseline walking speed, and BBS score 39 at 2 months as covariates. The first model tested the impact of stroke type (hemispheric large-vessel-distribution infarction, hemispheric lacunar infarction, brainstem infarct or hemorrhage, hemispheric hemorrhage). The second model, limited to the 150 participants with large-vessel-territory infarcts, tested the effect of presence or absence of basal ganglia involvement, defined by infarction in the striatocapsular territory. The third model, also limited to the 150 participants with large-vessel-territory infarcts, compared the effects on recovery of side of lesion to determine if there might have been a deleterious effect of hemispatial neglect, anosognosia, or anosodiaphoria associated with right-hemisphere cortical infarcts. We did not test for the presence of these disorders. Depression, as defined by Patient Health Questionnaire-9 score, was entered as an additional covariate in this model as it too could have affected motivation, independent of site of lesion. We then replicated this model (model 3B), adding HEP treatment to test the hypothesis that right-sided large-vessel-distribution infarcts, which are more likely to be associated with hemispatial neglect, anosognosia, or anosodiaphoria, would have a particularly negative effect on the recovery of these participants because they may have been, to a greater extent, left to their own initiative (plus the support of their families) to walk. This differential treatment effect would be manifested as a Treatment × Side interaction effect. The fourth model, also limited to the 150 participants with large-vessel-distribution infarcts, tested the impact on outcome of the potential differential effect of right-hemisphere strokes on balance by virtue of distortion in perception of the postural vertical. Consequently, BBS score was not included as a covariate. The fifth model tested the effect on outcome of moderate to severe leukoaraiosis compared with no or mild leukoaraiosis. The sixth model tested the potential impact of presence of prior large-vessel-distribution infarcts on outcome.
The last-observation-carried-forward method was used to handle missing data. Because we tested 7 different models, we applied a Bonferroni adjustment and used P < .007 as the criterion for statistical significance. All statistical analyses were performed using SAS software, version 9.2 (SAS Institute, Cary, NC).
Results
Of the 408 participants in the study, CT scans were obtained in 127 (31.1%) and MRI scans in 264 (64.7%). Scans were unavailable in 17 (4.2%). Scans demonstrated the acute stroke in 360 participants. Lesion loci are detailed in Table 2, and gait speed changes (uncontrolled) for each of the contrasts involved in hypothesis testing are detailed in Table 3. The results of our regression analyses are presented in Table 4.
Hypothesis 1. Type of lesion, controlling for baseline gait speed, BBS score, and age, had an impact on 2- to 12-month change in gait speed, which was nearly statistically significant (P = .008). The major contributors to this appeared to be the relatively lesser improvement in gait speed change (so-controlled) observed in participants with lacunar infarctions and the relatively greater improvement in participants with hemorrhages.
Hypothesis 2. Controlling for baseline gait speed, BBS score, and age among participants with large-vessel-distribution infarcts, basal ganglia involvement caused by striatocapsular infarction was associated with a significantly worse outcome at 1 year (P = .005).
Hypothesis 3. Among participants with large-vessel-distribution infarcts, side of stroke, controlling for baseline gait speed, age, and baseline BBS score, had no relationship to gait speed change (Hypothesis 3A). Furthermore, there was no evidence of a Side × Treatment interaction effect (Hypothesis 3B).
Hypothesis 4. BBS score at 2 months poststroke was 36.71 ± 13.22 in participants with left-hemisphere large-vessel-distribution infarcts and 30.15 ± 16.22 in those with right-hemisphere infarcts (P = .015), consistent with the well-established differential association between right-hemisphere large-vessel-distribution infarcts and altered sense of the postural vertical. However, notwithstanding our reported finding of a direct association between BBS score and gait speed at 1 year, 40 the poorer balance of participants with right-hemisphere large-vessel-distribution strokes did not predict less 2- to 12-month gait speed improvement.
Hypothesis 5. There was a trend for moderate to severe leukoaraiosis at baseline to be negatively associated with gait speed change, but the finding did not reach significance by the standards of this study.
Hypothesis 6. The presence of prior strokes was associated with a significantly reduced gait speed change (P = .002).
Lesion Locus and Type.
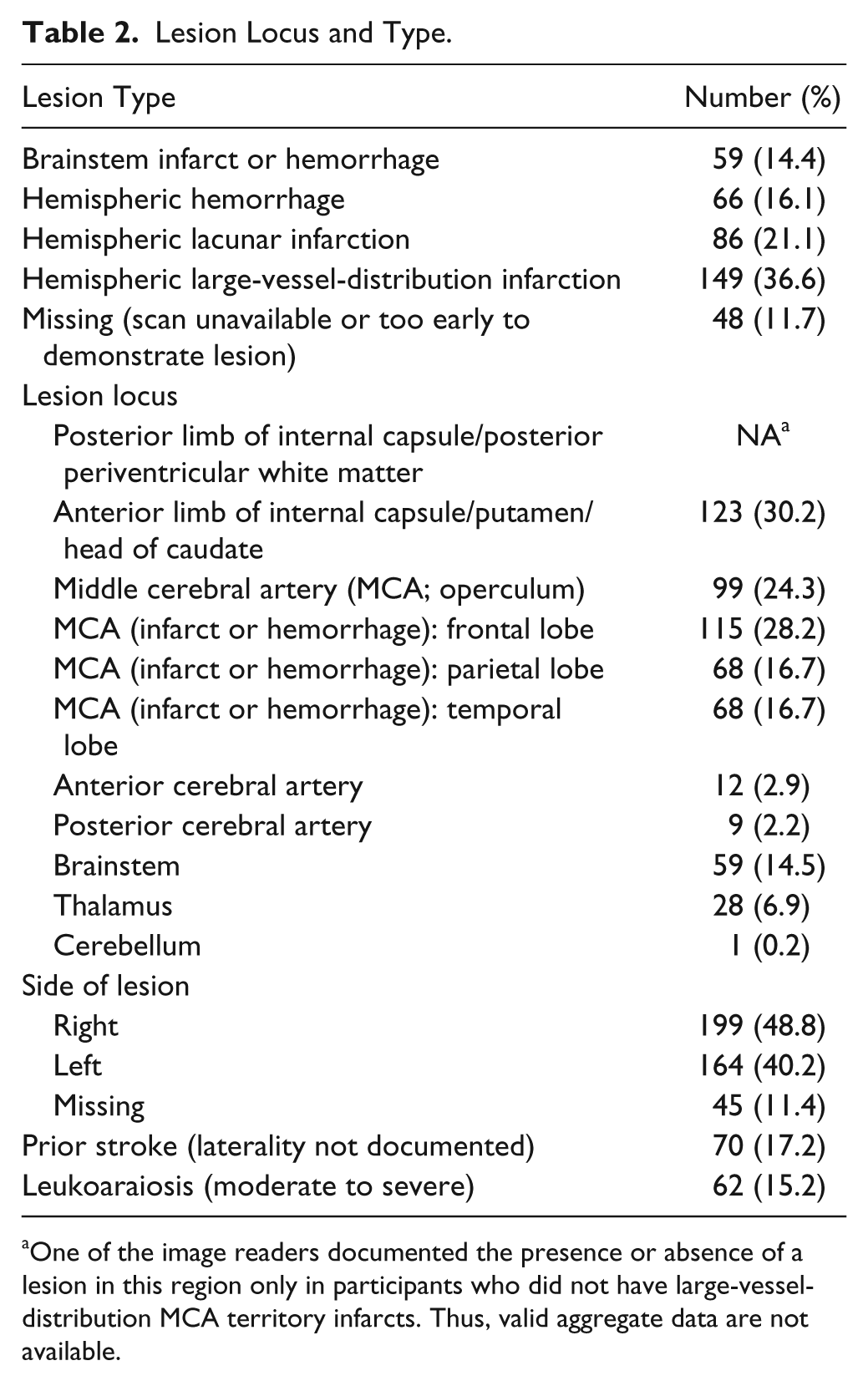
One of the image readers documented the presence or absence of a lesion in this region only in participants who did not have large-vesseldistribution MCA territory infarcts. Thus, valid aggregate data are not available.
Gait Speed Changes by Key Variables (ACA Territory Infarcts Excluded), Uncontrolled.
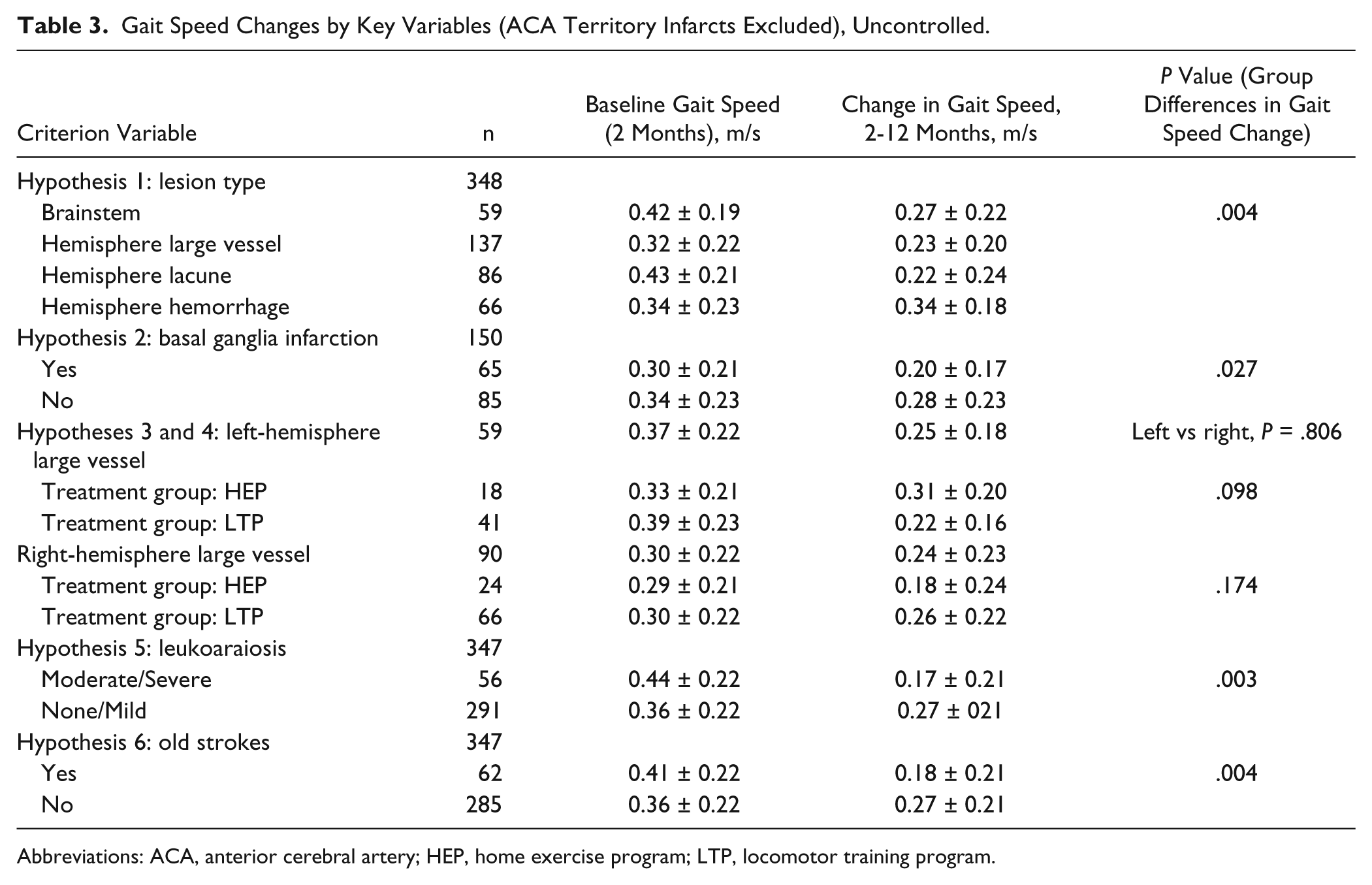
Abbreviations: ACA, anterior cerebral artery; HEP, home exercise program; LTP, locomotor training program.
Results of Regression Analyses.
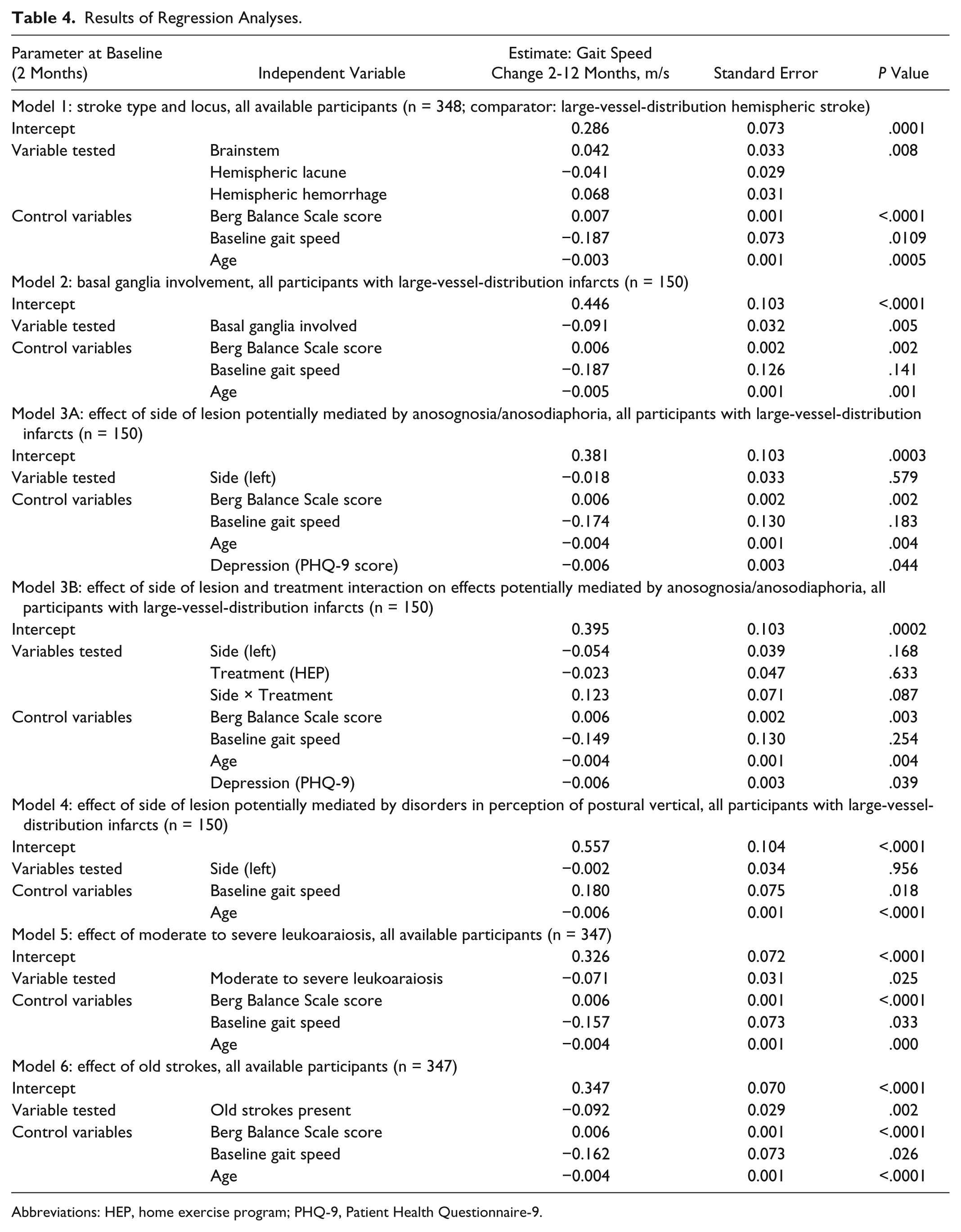
Abbreviations: HEP, home exercise program; PHQ-9, Patient Health Questionnaire-9.
Discussion
In this hypothesis-driven secondary analysis of the results of the LEAPS trial, in which we controlled for key baseline variables, including gait speed, BBS score, and age, we found a trend (P = .008) toward effect of lesion type on the primary outcome measure of the LEAPS trial—gait speed at 1 year—compounded of the relatively worse outcome for participants with lacunar infarction and the relatively better outcome for participants with hemispheric cerebral hemorrhage. We also found that basal ganglia involvement (striatocapsular infarctions) and the presence of prior stroke had negative effects on the primary outcome measure of the LEAPS trial—gait speed at 1 year. We did not find a significant relationship between right-hemisphere large-vessel-distribution infarction and 2- to 12-month change in gait speed—a relationship posited to exist because of the well-established association of such strokes with hemispatial neglect and anosognosia, and distorted perception of the postural vertical. We also did not find an association between moderate to severe leukoaraiosis and 1-year outcome.
Results of analyses of the impact of stroke type—that is, lacunar infarction, large-vessel-distribution cerebral infarction, brainstem infarction or hemorrhage, intracerebral hemorrhage, extent of stroke (basal ganglia involvement), and presence of moderate to severe leukoaraiosis or prior infarcts—can be interpreted with the most confidence. However, results related to hypotheses regarding impairment of specific functions as a result of lesions—for example, hemispatial neglect, anosognosia, anosodiaphoria, or disorders of perception of the postural vertical differentially associated with large-vessel-distribution right-hemisphere infarcts—are least secure. This is because these behavioral disorders were inferred and not directly measured.
Lesion Type
The apparently deleterious effect of lacunar infarction came as a surprise, particularly given the widely held view that lacunes are associated with a better prognosis. We suspect that this impression derives from the fact that lacunes often are not centered in the posterior periventricular white matter (the locus of descending corticospinal and corticobulbar pathways). Initially, motor function may be at floor levels, but with modest spontaneous recovery, improvement of paresis ensues. In contrast, with large-vessel-distribution infarcts, in which posterior periventricular white matter involvement is often extensive and paresis is very severe initially, even with the benefits of long-term spontaneous recovery, motor function may remain at floor levels. Only when there has been substantial opportunity for spontaneous recovery (2 months in the LEAPS trial) and analysis is controlled for the baseline clinical deficit, does the prognostic significance of lacunes become apparent. With large-vessel-distribution infarctions, many factors other than damage to corticospinal and corticobulbar pathways may contribute to motor impairment, including damage to other brain pathways that contribute to motor function (see the section Prior Stroke, below), as well as behavioral deficits, including deficits in motivation. However, with lacunar infarctions, motor impairment is solely attributable to a discrete lesion of descending corticospinal and corticobulbar pathways. It may be that, given the variety of factors contributing to paresis with large-vessel infarctions, there is somewhat greater opportunity for recovery, provided patients are not at floor levels of motor function to start with. Consistent with this concept, Sterr et al 12 found that in a study of 22 participants (at least 8 with large-vessel-distribution infarctions), who underwent constraint-induced movement therapy, severity of deficit, as measured by the Wolf Motor Function Test and the Motor Activity log, was correlated with extent of damage to the descending corticospinal tract, whereas response to treatment was not (see also Riley et al 42 ). We suggest that with lacunar infarctions, because neurological impairment is solely defined by the white matter lesion, recovery is limited by the capacity for recovery from that lesion, which may be less than that for other factors influencing paresis and engagement in therapy, such as damage to other cerebral pathways contributing to motor function (see below) and behavioral deficits, including deficits in motivation, which could affect participation in therapy.
Participants with hemispheric hemorrhages tended to have relatively higher gains in gait speed, suggesting that potential neurotoxic effects of brood products may not have major clinical consequences for recovery of walking. The trend toward relatively worse prognosis in participants with lacunar infarctions and relatively better prognosis in participants with hemorrhages may reflect a different time course of recovery from these 2 types of lesions. 16
Basal Ganglia Infarction
Our finding of a significant deleterious effect of striatocapsular infarction on outcome supports our hypothesis that the loss or corruption of basal ganglia input to the SMA and premotor and motor cortex (via VA and VLo nuclei of the thalamus) may have a negative impact on neuroplasticity.
Right-Hemisphere Large-Vessel-Distribution Infarction
Our failure to find a negative association between right-hemisphere large-vessel-distribution infarction and 1-year outcome raises a number of possibilities: (1) candidates with significant hemispatial neglect, anosognosia, or anosodiaphoria were substantially excluded for various reasons, not the least being lack of motivation and refusal of informed consent, during the screening process; (2) to the extent that neglect, anosognosia, and anosodiaphoria were present, they had substantially improved or even resolved by 2 months, eliminating them as adverse prognostic factors or so reducing their prevalence that their effect was undetectable; (3) to the extent that neglect, anosognosia, and anosodiaphoria were present, their impact was minimized by the intensive therapeutic environment created by the LEAPS study; and (4) despite a sizable literature linking hemispatial neglect and often concomitant anosognosia and presumptive anosodiaphoria (all differentially associated with right-hemisphere cortical infarction) to worse prognosis, our large and carefully controlled study provides evidence that right-hemisphere cortical infarction does not have the negative prognostic implications that might have been anticipated.
The potential reasons for failure to find a deleterious effect of right-hemisphere large-vessel-distribution stroke mediated via distortions in perception of the postural vertical are substantially similar: (1) such impairments simply might not have had the expected negative effect on gait recovery and gait rehabilitation; (2) candidates with severe deficits may have been largely excluded during screening; (3) deficits may have substantially improved by 2 months; and (4) therapists may have been able, to some extent, to enable participants to effectively compensate, even as imbalance and falls persisted as major problems in the LEAPS study, 43 improvements in gait speed notwithstanding. It is noteworthy that BBS scores in participants with right-hemisphere large-vessel-distribution infarcts were significantly lower than in those with left-hemisphere infarcts (P = .015), a finding that suggests that many participants with right-hemisphere lesions with impaired balance, plausibly in part a result of disorders of perception of the postural vertical, were included in our study but that this imbalance did not significantly affect gains in walking speed.
Leukoaraiosis
The absence of any evidence of a negative effect on outcome by leukoaraiosis (which presumably predominantly reflects ischemic demyelination in this population) may simply indicate that even in participants rated as having moderate to severe leukoaraiosis, the lesion burden was still quite modest.
Prior Stroke
The negative impact of prior strokes on outcome was unexpected because patients were excluded if there were residual neurological deficits related to such strokes. One possible explanation is that there exists extensive latent connectivity within the brain—white matter pathways culminating in very weak synaptic connections, which become stronger in the context of injury and thereby contribute to recovery. Prior stroke might, therefore, reduce some of this “connectivity reserve.” For example, in macaques years after surgical severing of the cervical dorsal roots for one arm, the erstwhile completely deafferented arm portion of the somatosensory cortex was found to have extensive afferents from the angle of the jaw just below the region of innervation by the trigeminal nerve. 44 It is possible that these novel afferents reflected new growth from the thalamus, but it is also possible that they represented existing latent connections that were engaged through synaptic modification in the wake of the injury. Diffusion tensor imaging tractography studies have demonstrated extensive connectivity between different regions of the human premotor cortex. 45 These connections could have functional significance related to coordination of movements between different parts of the body, but it is also possible that many of them represent latent connections as we have defined them. Such latent connections may be damaged with large-vessel-distribution strokes, which are associated with at least transient occlusion of the parent vessel. 46 In this setting, much of the vascular territory is likely to suffer some ischemic damage, even as imaging reveals outright infarction of only the least well-collateralized regions—the desert zones.
Applicability of Findings
A number of particular attributes of the LEAPS study and this particular analysis need to be borne in mind when comparing our results with those of other studies: (1) our studies focused on a specific time interval poststroke (60 to 365 days), thereby eliminating intersubject variability in time to recover; (2) the period of study is substantially later than that of prior studies of acute stroke outcome,47 -53 and outcome measures of interest were assessed at 1 year poststroke, a time point when rate of ongoing recovery has become very small; (3) LEAPS uniquely incorporated treatments of proven efficacy relative to customary and usual care, 54 hence proven neuroplastic effect; (4) patients recruited to LEAPS were able to ambulate postrehabilitation hospital discharge but had moderate to severe gait impairment; (5) the primary outcome measure in LEAPS was a specific functional measure, gait speed, not a global measure of functionality, such as the Functional Independence Measure, the Modified Rankin Scale, or the Barthel Index; (6) contrasts in the present study involve groups of participants with appropriately homogeneous lesion classifications—for example, large-vessel-distribution ischemic infarcts with versus without basal ganglia involvement; right-hemisphere versus left-hemisphere large-vessel-distribution infarcts (excluding lacunar infarcts); (7) the independent variables tested could have mediated their effects via their direct mechanistic impact on either reactive or experience-dependent plasticity, their effect on individual participation in the rehabilitation process, and their effect on participant activities after completion of the LEAPS protocol; our methodology does not enable us to distinguish these individual factors.
Limitations
This study is susceptible to the intrinsic risk of type I error associated with secondary analyses in general, even though our analyses were hypothesis driven and we set a Bonferroni-corrected benchmark for statistical significance. We do not have data on interrater reliability of the 2 neurologists who read the images. Both have more than 30 years of experience, but this does not preclude potentially important differences. However, most of the hypotheses tested in this study involved imaging abnormalities that are easily observed and seldom controversial: type of lesion, presence or absence of striatocapsular infarction, and side of infarction. Although we found that prior stroke adversely affected outcome, we are not able to qualify that finding in terms of the side of prior stroke relative to that of the index event.
Because the imaging studies we used were obtained at a large number of hospitals, they reflect hospital-to-hospital variability in imaging parameters. This variability is unlikely to have had any significant impact on identification of lesion type or locus, but it may have affected the degree to which leukoaraiosis was apparent. The relative insensitivity of CT for early infarction accounts for the studies that failed to demonstrate evidence of the acute stroke. The lesser sensitivity of CT for early infarction would also have led to underestimation of the size of lesions visualized on CT. However, none of our imaging variables were dependent on measures of lesion size. We have not been able to find studies demonstrating the relative sensitivity of MRI and CT for leukoaraiosis, but clinical experience suggests that MRI is more sensitive. There are more sensitive measures of leukoaraiosis—for example, quantification of fractional anisotropy from diffusion-weighted MRI sequences, but such measures are not yet used clinically, and our scans are likely to be representative of those obtained in common clinical practice.
Conclusion
Our study suggests that, although damage to corticospinal and corticobulbar pathways in the subcortical white matter is the major cause of paresis in stroke, type, locus, and extent of lesion, as well as prior stroke without residual motor deficits, may affect long-term outcome of rehabilitation of gait impairment when baseline factors such as severity of impairment, age, and imbalance are controlled for. Whether this is mediated through effects on reactive neuroplasticity or experience-dependent neuroplasticity cannot be said. Replication of our findings in prospective studies will be necessary to consider our results conclusive. None of our findings is of sufficient magnitude to influence clinical practice or inclusion criteria for clinical trials.
Footnotes
Authors’ Note
The contents of this article do not represent the views of the US Department of Veterans Affairs or the United States Government. The LEAPS database is publicly available through PubMed Central. Further information on research materials may be obtained from the first author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from National Institute of Neurological Disorders and Stroke and the National Center for Medical Rehabilitation Research (RO1 NS050506) and by the Department of Veterans Affairs (Rehabilitation R&D grant B6793C); Clinicaltrials.gov NCT00243919.