
Abstract
The current review develops a rationale and framework for examining the independent and combined effects of exercise training and cognitive rehabilitation on walking and cognitive functions in persons with multiple sclerosis (MS). To do so, we first review evidence for improvements in walking and cognitive outcomes with exercise training and cognitive rehabilitation in MS. We then review evidence regarding cognitive–motor coupling and possible cross-modality transfer effects of exercise training and cognitive rehabilitation. We lastly present a macro-level framework for considering mechanisms that might explain improvements in walking and cognitive dysfunction with exercise and cognitive rehabilitation individually and combined in MS. We conclude that researchers should consider examining the effects of exercise training and cognitive rehabilitation on walking, cognition, and cognitive–motor interactions in MS and the possible physiological and central mechanisms for improving these functions.
Introduction
Multiple sclerosis (MS) is a prevalent, nontraumatic disease of the central nervous system (CNS). This disease has a prevalence of 1 per 1000 persons in the United States.1,2 There are an estimated 2.5 million persons living with MS worldwide, and nearly 400 000 cases in the United States. 3 Of note, some recent epidemiological studies suggest a trend of increasing prevalence and incidence of MS worldwide, 4 and this disease occurs most often among young and middle-aged women of European descent. 3 MS typically begins with intermittent episodes of multifocal inflammation in the CNS,5-7 and this is characteristic of relapsing–remitting MS (RRMS). The inflammation can result in demyelination and transection of axons.5-7 There are neurodegenerative processes resulting in neuroaxonal loss (ie, atrophy) that can occur early in the disease, but are more prominent during the latter course of the disease5-7; this is characteristic of primary and secondary progressive MS. The CNS damage often accumulates over time and results in the progression of neurological disability8,9 as well as walking and cognitive dysfunction.10-12 Walking and cognitive dysfunctions are common, life-altering, and co-occurring (ie, coupled) consequences of MS.13,14
Walking dysfunction has been identified as a primary feature of MS in early historical accounts of the disease. 15 An estimated 75% of persons with MS have reported mobility problems based on population-based studies. 16 Data from an online survey of 1011 people with MS indicated that 41% of the sample reported difficulty walking and 13% reported an inability to walk 2 or more times per week. 17 Another recent study of 436 European MS patients indicated that nearly 50% of patients reported experiencing mobility impairments within the first month of diagnosis, and over 90% of patients reported experiencing mobility impairments within 10 years of diagnosis. 18 There is consistent evidence that performance on the timed 25-foot walk (T25FW) and 6-minute walk (6MW) as well as gait parameters are compromised in MS compared with controls. 19
Walking is a fundamental and valued part of our everyday life, regardless of the presence or absence of disease or chronic conditions. Ambulation represents one of the most valued functions among people with MS17,20 and has direct relevance for physical function, independence, quality of life (QOL), and activities of daily living.18,20 One study of 100 patients with MS reported that walking or gait function was rated as the most important domain of function compared with 12 other functions such as vision, thinking and memory, and mood. 21 Another study reported that persons with MS identified feelings regarding mobility impairment as limiting, frustrating, and challenging. 18 Relatedly, one study indicated that 70% of persons with MS who had difficulty walking rated it as the most challenging aspect of MS. 5 Walking difficulty further is disruptive of one’s daily life and has been associated with outcomes such as unemployment,17,22 physical function, QOL, and activities and participation. 19
Deficient cognition has been identified in early accounts of the disease, but was subsequently debated during the first half of the 20th century. 23 It is now recognized that 40% to 65% of MS patients demonstrate cognitive dysfunction based on poor performance on neuropsychological tests (eg, 1.5 standard deviations below normative test values). 24 Cognitive dysfunction primarily manifests as slowed information processing speed, deficits in learning and memory, perceptual skills and executive function, but less so as impaired intellectual functions and language skills.10,25 One meta-analysis reported moderate-sized reductions in overall cognitive function (g = −0.59), as well as in the cognitive domains of attention and executive function (g = −0.56), and learning and memory (g = −0.61) in persons with RRMS compared with controls; there were smaller differences in verbal and language functions (g = −0.44). 25 Another review indicated that processing speed, learning and memory, and executive function were more impaired in persons with progressive MS compared with RRMS. 26
Cognitive dysfunction is a highly disabling consequence of MS. Dysfunctions of information processing speed, learning and memory, and executive functions have been associated with depression in MS.27,28 Cognitive dysfunction further has been associated with unemployment and loss of employment in persons with MS,24,29 as well as reduced social functioning, 26 loss of driving abilities,30,31 and using the Internet for conducting activities of daily living (eg, purchasing an airline ticket). 32
The prevalence and burden of walking and cognitive dysfunction underscore the importance of managing these co-occurring consequences of MS. To that end, the current review develops a rationale and framework for examining the independent and combined effects of exercise training and cognitive rehabilitation on walking and cognitive functions in persons with MS. We focus on approaches for rehabilitation (ie, factors that could help a person with MS achieve and maintain maximal physical, psychological, social, and vocational potential, and quality of life, consistent with physiological impairment, environment, and life goals 33 ) as these have been identified as the best, and perhaps only, methods for restoring function in MS.33,34 Exercise training and cognitive rehabilitation, in particular, represent the rehabilitative approaches with the largest and most convincing bodies of literature for improving, restoring, and maintaining walking and cognitive functions, respectively, in MS. We do not review pharmacological treatments as these do not fall within the classical purview of rehabilitation, and there are existing reviews on extended-release, oral administration of dalfampridine (4-aminopyridine or 4-AP) for improving walking in MS.35,36 This article further is not a comprehensive, systematic review on the efficacy or effectiveness of exercise training and cognitive rehabilitation in MS, as there have been several recent reviews on this for exercise training 41 and cognitive rehabilitation. 58 Our rationale and framework are based on (a) evidence supporting exercise training and cognitive rehabilitation as behavioral approaches for rehabilitation of walking and cognitive function in MS, (b) cognitive–motor coupling, and (c) potential cross-modality transfer effects in this population. Accordingly, we first review evidence for improvements in walking and cognitive outcomes with exercise training and cognitive rehabilitation in MS. We then review evidence for cognitive–motor coupling and possible cross-modality transfer effects of exercise training and cognitive rehabilitation. We lastly present a macro-level framework for considering mechanisms that might explain improvements in walking and cognitive functions with exercise and cognitive rehabilitation individually and combined in MS. We conclude that researchers should consider examining the effects of exercise training and cognitive rehabilitation on walking, cognition, and cognitive–motor interactions in MS and identifying the possible physiological and central mechanisms for improving these functions.
Exercise Training
This section provides an overview of exercise training as a behavioral approach for improving walking and cognitive functions in MS. We first highlight evidence from meta-analyses and reviews for the efficacy of exercise training for improving walking and cognitive performance in MS. We further include recent, exemplar randomized, controlled trials (RCTs) that examine exercise training effects on walking and cognitive outcomes in MS. Exercise training is a chronic type of planned, structured, and repetitive physical activity undertaken over time that is designed for improving aspects of physical fitness (ie, characteristics of a person that are relevant for performing physical work). 37 For example, aerobic exercise training such as walking, cycling, or jogging should improve cardiorespiratory fitness (ie, peak oxygen consumption), whereas resistance training (ie, weight training with machines or free-weights) should improve muscular aspects of fitness (ie, maximal muscle strength or endurance). The importance of identifying fitness adaptations with exercise training is that such outcomes provide a manipulation check on compliance with exercise training protocols and represent possible causal mechanisms for improvements in walking and cognitive outcomes in MS.38,39
Exercise training has been considered the single most effective nonpharmacological type of symptomatic treatment in MS and represents a highly effective part of many MS rehabilitation programs. 40 There is robust evidence for improvements in walking outcomes with exercise training in MS.41,42 but the evidence for improvements in cognitive outcomes is in its infancy and is limited by small studies and methodological flaws.39,43 One meta-analysis included 22 published studies (either nonrandomized or randomized controlled trials) of 600 persons with MS, and reported an improvement of 0.19 standard deviations in walking outcomes after exercise training. 42 Another meta-analysis included data from 13 RCTs of 655 people with MS who engaged in exercise training compared with nonexercise control conditions, and reported clinically meaningful improvements in 10-meter walk time (10mWT) (16.5% improvement) and 2-minute walk (2MW) distance (19% improvement), as well as nonclinically meaningful improvements in T25FW performance (0.6 second improvement), 6MW distance (34.5 meter improvement), and timed-up-and-go (TUG) time (1.1 second improvement). 41 By comparison, one literature review reported inconsistent evidence from RCTs for the effects of exercise training on cognition in MS, 39 and this was confirmed in a separate systematic review of exercise and cognitive function in adults with neurological diseases, including MS. 43 Of note, 2 recent trials have demonstrated improvements in some domains of cognition after aerobic exercise training in MS.44,45 We now review evidence from exemplar and existing RCTs examining the effects of aerobic, resistance, and combined exercise training on walking and cognitive outcomes in MS.
Aerobic Exercise Training
Overall, there is promising evidence supporting aerobic exercise training for improving various outcomes, including walking and cognition, in MS. 46 One study, of note, adopted an RCT design for comparing treadmill training (ie, aerobic exercise) with yoga training (ie, nonaerobic exercise) and a waitlist control condition for improving ambulatory function as well as balance, fatigue, and mood in persons with MS. 47 The sample included 31 sedentary women with MS (mean Expanded Disability Status Scale [EDSS] score = 2.2, range = 1.0-4.0) who were randomly assigned into 1 of 3 groups, namely, treadmill training, yoga, or waitlist control (ie, passive control). The treadmill training group completed supervised walking on a motor-driven treadmill 3 times per week over an 8-week period. The duration was 30 minutes per session, and the intensity was between 40% and 75% of age-predicted maximum heart rate. The yoga condition involved Hatha yoga and was performed 3 times per week for 60 to 70 minutes per session over an 8-week period. There was a statistically significant improvement in 10mWT in the treadmill training group (18.5% decrease), whereas there was no change on this measure for yoga or control. By comparison, both treadmill training (16.2% increase) and yoga (10.0% increase) yielded improvement in 2-minute walk test (2MWT) distance, whereas there was no change in the control condition. This study did not include an attention control comparison condition that accounted for social contact and did not report on blinding of outcome assessors. However, this study provides promising evidence that aerobic exercise training is capable of improving both walking speed and endurance in MS.
One noteworthy pilot study adopted an RCT design for comparing 3 aerobic exercise training conditions with a waitlist control condition for improving walking endurance and various domains of cognition (ie, attention, processing speed, long-term memory, executive function) in persons with progressive MS. 44 The sample included 42 MS patients with a secondary progressive clinical disease course (EDSS = 4.0-6.0) who were randomly assigned into 1 of 4 groups, namely, supervised cycle ergometry, arm ergometry, or rowing, and waitlist control (ie, passive control). The exercise groups meet 2 to 3 times per week over 8 to 10 weeks. The duration steadily increased across the program from 15 to 45 minutes per session, and the intensity was between 120% and 130% of anaerobic threshold. There was a statistically significant improvement in 6MWT distance in all 3 exercise training groups, whereas there was no change with waitlist control. There seemingly were no differential improvements in 6MWT distance across exercise conditions. All 3 exercise conditions, but not control, further improved verbal learning and delayed recall on the Verbal Learning and Memory Test (VLMT), whereas there were selective changes in alertness (ie, Test Battery of Attention alertness subtest scores) for primarily cycle ergometry. There were no intervention effects for information processing speed (Symbol Digit Modalities Test [SDMT]), executive function (Achievement Testing System), or verbal fluency (Regensburg Verbal Fluency Test). There were significant associations between changes in aerobic capacity (ie, cardiorespiratory capacity or VO2peak) and 6MW and VLMT performance. This suggests that increasing cardiorespiratory capacity might be a potential mechanism for improvements in endurance walking performance and verbal memory with aerobic exercise training in persons with progressive MS.
We are aware of one intriguing case study that collected data from 2 ambulatory, memory-impaired persons with MS who were randomly assigned into nonaerobic (ie, stretching or active control) and aerobic (stationary cycling) exercise training conditions. 45 The 2 conditions involved exercising 30 minutes per session 3 times per week for 12 weeks. Aerobic exercise training resulted in a 16.5% increase in hippocampal volume, 55.9% increase in verbal memory, and 53.7% increase in nonverbal memory, as well as increased hippocampal resting-state functional connectivity. There were no significant changes in overall cerebral gray matter (+2.4%), non-hippocampal deep gray matter structures (thalamus, caudate: −4.0%), or in nonmemory cognitive functioning (executive functions, processing speed, working memory: changes ranged between −11% and +4%). The nonaerobic exercise condition demonstrated minimal change in hippocampal volume (2.8%), no changes in verbal or nonverbal memory (0.0%), and no change in hippocampal resting-state functional connectivity. This suggests that aerobic exercise training might improve domains of cognitive performance through neuroplasticity in MS.
Resistance Exercise Training
Overall, the evidence is promising for improving walking function with resistance exercise training in MS. 46 By comparison, there is no evidence from an RCT examining the effects of resistance exercise training on cognition in this population. 46 One study using a single-blind RCT design examined the effect of supervised progressive resistance training (PRT) on ambulatory outcomes and muscle strength in persons with MS. 48 The sample included 38 patients with definite RRMS (EDSS = 3.0-5.5) who were randomly assigned into PRT or waitlist control. PRT consisted of 5 lower body exercises (eg, leg press, knee extension, hamstring curl) performed twice per week over 12 weeks. The waitlist control group did not participate in any intervention during the 12-week period (ie, passive control), and was offered the PRT program posttrial. There was a statistically significant improvement in functional capacity based on a composite score and individual scores from the 10mWT, 6MWT, stair climb, and chair stand test following PRT (21.5% increase) compared with no change in the waitlist control. Improvements were further observed in maximum voluntary contraction (MVC) assessments of the knee extensors and flexors after PRT (15.7% to 21.3% increase) compared with no change in the waitlist control. There were significant associations between changes in MVC for the knee extensors with the composite and individual measures of ambulatory performance. This suggests that resistance exercise training might improve walking function through increases in muscle strength.
Another recent study using an RCT design examined the immediate and long-term effects of a 24-week period of supervised PRT on ambulatory functional outcomes and neuromuscular function in persons with MS. 49 The sample included 35 patients with clinically definite RRMS (EDSS = 2.0-5.5) and stable interferon therapy who were randomly assigned into PRT or waitlist control (ie, passive control). PRT was based on American College of Sports Medicine recommendations and met 2 times per week over 24 weeks. PRT consisted of 4 lower body exercises (eg, leg press, leg extension) and 2 upper body exercises (eg, triceps extension). The PRT group further performed community-based self-guided training for 24 weeks following the intervention, whereas the controls then underwent the PRT program. There was a statistically significant improvement in T25FW (0.2 m/s increase), 2MWT (0.1 m/s increase), stair climb (1.9 second decrease), and self-reported walking impairment (7.3 point decrease on the Multiple Sclerosis Walking Scale–12 [MSWS-12]) following PRT, whereas there was no change with waitlist control. Those improvements were maintained during the 24-week period following PRT. There further were improvements in MVC of the knee extensors and flexors after PRT that were sustained during the 24-week follow-up period. There were significant associations between changes in MVC for the nondominant knee extensors and flexors with measures of ambulatory performance. This further supports the possibility that resistance exercise-induced increases in strength might account for improvements in ambulation.
Combined Exercise Training
There has been a recent and expanding interest in combining modes of exercise as a comprehensive training program and examining the effects on outcomes in persons with MS. 50 Several recent studies have adopted this approach for improving walking performance in MS. To date, there are no studies examining the effects of combined exercise training on cognitive outcomes in this population. One study adopting a pretest/posttest design examined the effect of combined exercise training consisting of aerobic, resistance, and balance activities on walking outcomes in persons with MS who had onset of gait impairment. 51 The sample included 13 participants with significant disability (EDSS range = 4.0-6.0) who completed the MSWS-12, T25FW, and TUG before and after an 8-week training period. The training program was designed by a physical therapist and was performed 3 days per week under the supervision of an exercise specialist. The exercise program was generic and not individualized per participant. Session durations were increased by approximately 5 minutes per week up to a maximum of 60 minutes in week 8 (ie, 20 minutes of each mode of exercise). The combined exercise program was associated with significant improvements in MSWS-12 scores (d = 0.56) as well as T25FW (d = 0.90) and TUG (d = 0.71) performance. Although this was not an RCT design and is limited by the absence of a control comparison condition, this study does provide preliminary evidence for combined exercise as an approach for improving walking in persons who have substantial ambulatory disability.
One recent study adopted an RCT design for comparing combined exercise training with a waitlist control condition (ie, passive control) for improving walking and other secondary endpoints in MS. 52 The sample initially included 84 patients with MS (EDSS = 0-4.0) who were randomly assigned into 1 of 2 groups, namely, combined exercise training or control (avoid engaging in planned physical or rehabilitation activity over 10 weeks). The combined exercise program included aerobic (cycle ergometer or treadmill), resistance (lower extremity), balance (seated exercise on physiotherapy ball), and stretching (whole-body) exercises and met 3 times per week over 10 weeks. The duration steadily increased across the program from 60 to 90 minutes per session. Of the 42 people randomized into the exercise group, there were 39 who completed the program, whereas only 20 completed in the control group; this suggests attrition in the control condition as a possible source of bias. Nevertheless, there was a statistically significant improvement in 6MW distance in the combined exercise group compared with control (mean difference = 137 m). These studies suggest that a comprehensive exercise training program might be associated with improvements in walking, but do not isolate the independent contributions of each exercise modality for such improvements. This could be accomplished in future RCTs that examine the effects of single versus multimodal exercise training programs on walking and cognitive outcomes in MS.
Cognitive Rehabilitation
This section addresses cognitive rehabilitation as a behavioral approach for improving cognitive dysfunction in persons with MS. We are unaware of research that examines the effects of cognitive rehabilitation on walking outcomes in MS, and thus this section only focuses on cognitive outcomes (ie, performance on neuropsychological tests). However, in the aging literature, there is evidence that cognitive rehabilitation can improve walking parameters, 53 and preliminary work reporting stronger effects for cognitive rehabilitation on cognition than physical exercise. 54 We first highlight evidence from meta-analyses and reviews for the efficacy of cognitive rehabilitation for improving cognitive performance in MS. We then review exemplar RCTs that involve different characteristics of cognitive rehabilitation interventions on cognitive performance. Cognitive rehabilitation refers to interventions that aim to directly improve cognition and/or develop strategies to compensate for cognitive impairment. Such interventions tend to be multifactorial (ie, using several approaches for improving cognition),55,56 given that cognitive impairment is multifaceted and there is no single overarching model for guiding cognitive rehabilitation interventions. To that end, cognitive rehabilitation interventions can include cognitive training (ie, planned, structured, repetitive cognitive activities) to directly improve impaired domains of cognitive functioning and teaching of compensatory strategies to help patients cope with cognitive impairment, thereby aiming to improve cognition.24,57,58 Importantly, cognitive rehabilitation is not a purely psychological approach for treating mood disorders, enhancing self-efficacy, and reducing stress associated with cognitive impairment; however, some interventions may include a psychotherapy element for addressing issues that can indirectly affect cognitive impairment (eg, depression, personality difficulties).24,57,58 Although many cognitive rehabilitation interventions involve outcomes beyond cognitive performance (eg, self-efficacy), the current section of the review focuses on the effects of cognitive rehabilitation on neuropsychological test performance, given the importance of neuropsychological testing in detecting cognitive impairment in MS. 10 The direct mechanisms for how cognitive rehabilitation improves cognition in MS are not well understood, although it has been proposed that specific interventions might stimulate alternate neural pathways for specific cognitive functions (ie, compensation through neuroplasticity). 59
Research on cognitive rehabilitation in MS is in its infancy. Reviews have highlighted that results from studies examining the effects of cognitive rehabilitation in persons with MS have yielded generally mixed results, and suffer from many methodological flaws.24,57,60 The effect of neuropsychological rehabilitation on cognitive performance in MS was recently quantified in a Cochrane review with a meta-analysis. 58 That paper examined 20 studies that included 966 persons with MS and reported statistically significant effects of cognitive rehabilitation (vs any control) on memory span (effect size [ES] = 0.54) and working memory (ES = 0.33), but not executive function (ES = 0.35), immediate verbal memory (ES = 0.20), information processing speed (ES = 0.15), or attention (ES = 0.06). The heterogeneous effects on neuropsychological performance were primarily associated with variation across interventions (ie, single vs multiple targeted cognitive domains, various control comparison conditions), and noteworthy methodological limitations (eg, small sample sizes, lack of blinding, selection biases). 58
There have been several well-designed RCTs that may be of particular importance for contextualizing research on cognitive rehabilitation in MS. These RCTs have adopted 3 distinct cognitive rehabilitation interventional approaches for improving cognition in this population. For example, interventions selectively target a single domain of cognition (eg, memory), multiple domains of cognition concurrently (eg, attention and executive function), or are tailored whereby participants receive cognitive training tailored to the individualized domain(s) of cognitive impairment. We review exemplar RCTs for each of these.
Specific Interventions for Rehabilitating a Single Cognitive Domain
The majority of successful cognitive rehabilitation interventions in MS have targeted learning and memory as a single domain of cognition. 57 One particularly promising approach for selectively improving learning and memory involves the modified Story Memory Technique (SMT). This training program, originally developed for those with traumatic brain injury, uses imagery and context to aid new learning in those with memory impairments. 61 Several small RCTs in memory-impaired persons with MS reported that those who received 5 weeks of modified SMT training demonstrated statistically significant improvements on self-report (ie, Memory Functioning Questionnaire) and objective (ie, California Verbal Learning Test-2 [CVLT-2]) memory outcomes relative to a social-contact control group (ie, active control).61,62 There is further evidence that persons who underwent SMT training demonstrated increased activation of frontal and parahippocampal brain regions as well as increased functional connectivity during a functional MRI (fMRI) memory task compared with those who underwent a social-contact control condition.62,63 Recently, the modified SMT paradigm was included in a larger double-blind, placebo-controlled RCT that examined the immediate and long-term effects of cognitive rehabilitation on objective and everyday memory in 86 learning-impaired persons with MS. 64 Participants were randomized to a 5-week cognitive rehabilitation intervention condition (ie, modified SMT paradigm) or social-contact control. Participants in the intervention condition completed two, 45- to 60-minute training sessions per week over a 5-week period, whereas those in the control condition met with a therapist and completed reading comprehension exercises (ie, without using imagery and context techniques) at the same frequency and duration as the intervention condition. 64 Those who underwent modified SMT training demonstrated moderate-sized, statistically significant improvements on CVLT-2 learning slope (d = 0.54) and a small, statistically significant improvement on the Rivermead Behavioural Memory Test (d = 0.37) compared with the control condition. Importantly, those effects were maintained 6 months postintervention. 64 Another interesting finding from that study was that among those who underwent the intervention, participants with better processing speed demonstrated significantly larger improvements in CVLT-2 learning slope. 65 The primary results from this study provide strong support (ie, class I evidence) for the modified SMT as a targeted cognitive rehabilitation approach for selectively improving learning and memory in MS, particularly among memory-impaired persons with intact processing speed.
The evidence supporting targeted cognitive rehabilitation interventions for specifically improving single domains other than memory in MS is less convincing. 57 By comparison, there are no published RCTs that have specifically improved cognitive processing speed or executive function in MS, as highlighted by one recent review. 57 There is RCT evidence regarding cognitive rehabilitation effects on those cognitive functions, whereby interventions target multiple cognitive domains at once—those studies will be described in the next section. Nevertheless, one recent well-designed RCT examined the effects of home-based, computerized cognitive rehabilitation for specifically improving aspects of attention in 88 persons with MS. 66 Participants with attention dysfunction (ie, impairment on at least 2 neuropsychological tests of attention) were randomized into a specific intervention condition or nonspecific intervention condition (ie, control condition). The specific intervention involved the computerized Attention Processing Training (APT) program, which consisted of 5 modules that hierarchically targeted focused, sustained, selective, alternating, and divided attention. APT exercises increased in difficulty over the course of the intervention. The nonspecific intervention condition involved newspaper and text-based reading comprehension exercises (ie, no attentional training). Each intervention condition was home-based and was designed to involve two, 60-minute sessions per week over the 3-month period. 66 Those who received APT training demonstrated statistically significant improvements in Paced Auditory Serial Addition Test (PASAT) 2′ and 3′ performance (ie, sustained attention) compared with those in the nonspecific intervention. Such improvements were maintained 3 months later. SDMT performance did significantly improve relative to baseline for both conditions, but those improvements did not significantly differ based on condition (ie, specific vs nonspecific). There were no significant intervention effects on tests other than sustained attention, such as tests of memory or selective (ie, Visual Search) or alternating/divided attention (Trail Making Tests A and B). 66 This study does seemingly identify sustained attention as a potential target for specific cognitive rehabilitation interventions, but it does not overwhelmingly support APT for rehabilitating multiple aspects of attention in MS.
Multifaceted Interventions for Rehabilitating Multiple Cognitive Domains
There have been several well-designed RCTs that attempt to rehabilitate multiple cognitive functions simultaneously, oftentimes using computerized cognitive training. There is limited support for this approach, as results from studies that adopt multifaceted cognitive rehabilitation interventions have been conflicting. For example, one double-blind, RCT examined the effects of a computerized training program on attention and executive function in 20 persons with MS who had impaired attention and executive function. 67 Participants were randomly assigned to the computerized cognitive rehabilitation intervention condition or a control condition that involved no rehabilitation. The intervention involved the “Plan A Day” and “Divided Attention” modules of the RehaCom cognitive training package. This program trains planning and organizing ability, using realistic scenarios, as well as the ability to selectively attend to important visual stimuli in the presence of distractors, using a locomotive-driving simulation. Those who underwent the intervention completed three, 60-minute training sessions per week, over a 3-month period. Those who received cognitive rehabilitation demonstrated statistically significant improvements in attention and executive function, based on PASAT 2′, 3′, and Wisconsin Card Sorting Test scores, compared with the nonrehabilitation control, 67 and the results were maintained at 6-month follow-up. 68 Those authors reported that relative to healthy controls, MS participants in the treatment group demonstrated significant bilateral increases in dorsolateral prefrontal cortex activation using fMRI, which correlated with improved performance and improved functional connectivity in various brain networks.69,70 However, other studies using computerized approaches to rehabilitate attention and working memory simultaneously have not yielded positive results.71,72
Other computerized interventions have targeted a broader array of cognitive functions by adopting a more generalized approach to cognitive rehabilitation. For instance, one recent single-blind RCT examined the effects of computer-assisted cognitive rehabilitation on memory, attention, executive function, and problem-solving skills in 61 persons with MS who self-reported cognitive deficits. 73 Participants were randomized into a multifaceted cognitive rehabilitation intervention condition or waitlist control. The intervention condition involved a once-weekly group-based efficacy enhancement class as well as home-based computerized cognitive training. The cognitive training involved completing computerized cognitive exercises targeting attention, executive function, memory, and problem-solving skills that increased in difficulty over the course of the intervention. Participants engaged in three, 45-minute sessions per week over an 8-week period, and were exposed to computerized cognitive exercises that targeted a new cognitive domain each of the first 4 weeks, and had access to computerized cognitive exercises targeting all 4 domains for the remainder of the intervention. 73 Those who received cognitive training demonstrated moderate-sized, statistically significant improvements on CVLT-2 scores, and large, statistically significant improvements in self-reported use of memory strategies (ie, Multifactorial Memory Questionnaire scores) compared with the waitlist control condition. However, there were no statistically significant effects of the intervention on other neuropsychological outcomes (ie, tests of attention, executive function, problem solving). 73 Taken together, despite some positive results, it remains unclear which cognitive domains actually improve following multifaceted cognitive rehabilitation, and how such interventions might improve those cognitive functions.
Tailored Interventions Based on Individual Cognitive Impairments
The third category of cognitive rehabilitation interventions involves tailoring the cognitive training based on the domain(s) of cognitive impairment of individual participants. Such interventions aim to optimize the impact of cognitive rehabilitation by including generalized cognitive training (ie, targeting multiple domains of cognition) that is individualized based on the pattern of cognitive impairment. For example, one RCT examined the effects of a computerized cognitive rehabilitation intervention compared with a noncognitive rehabilitation (ie, speech therapy, occupational therapy) control condition in 19 persons MS who had general cognitive deficits. 74 The intervention involved teaching cognitive compensation strategies for everyday living, alongside administration of the learning and memory, attention, and problem-solving modules of the RehaCom cognitive training program. Participants completed twelve, 60-minute sessions per week of computerized exercises that targeted the participants’ 2 most impaired domains of cognition over 4 weeks. Those who underwent the cognitive training program demonstrated statistically significant improvements on German-language neuropsychological tests of executive function and spatial-constructional ability compared with the control condition; the improvements were seemingly maintained for 3 months postintervention. There were no statistically significant intervention effects on other cognitive domains relative to the noncognitive rehabilitation control. 74 Of note, this small study did not report the results of the tailored intervention based on subgroups of persons who underwent training on separate domains of cognition.
One recently published RCT adopted a similar tailored approach in a larger sample of persons with MS. 75 That study examined the effects of a multicenter, computerized cognitive rehabilitation intervention and a social-contact control in 41 cognitively impaired persons with MS who were receiving a similar disease-modifying treatment regimen. The computerized intervention condition targeted executive function, memory, and attention. Executive function training involved the “Plan A Day” procedure from the RehaCom cognitive training program, 67 memory training involved completing computerized reading comprehension exercises, and the attention training component involved repeated administration of the modified PASAT. Participants received training according to individualized patterns of cognitive impairment and all computerized cognitive exercises increased in difficulty over the course of the intervention. If participants were impaired in more than one domain, training was balanced equally across impaired cognitive domains. The computerized training itself consisted of two, 60-minute sessions of cognitive training per week, for 15 weeks. Those in the social-contact control condition met with a psychologist at the same frequency and duration as the intervention condition and discussed perceptions of the impact of MS and related difficulties at work. Those who received cognitive rehabilitation failed a significantly fewer number of neuropsychological tests in Rao’s Brief Repeatable Battery than those in the social-contact control condition. Those who underwent cognitive rehabilitation, regardless of the cognitive domain trained, further demonstrated statistically significant improvements on the Selective Reminding Test (SRT)-delayed recall and 10/36 Spatial Recall Test (SPART). Interestingly, the authors further analyzed the selective effects of the tailored intervention based on the domain of cognitive training. Of those who completed the intervention, 50% completed executive function training, 72% completed memory training, and 55% completed attention training. Those who underwent memory training demonstrated significant improvements on the SRT-delayed recall and 10/36 SPART, and those who underwent attention training demonstrated significantly improved SDMT scores, respectively, compared with the control condition. There were no significant effects of executive function training on executive outcomes compared with the control condition. 75 This provides additional support for targeted cognitive rehabilitation for improving specific cognitive functions, in particular, memory and attention, within the context of a tailored approach. Although few published cognitive rehabilitation RCTs have included tailored interventions, this recent study is promising, given that this cognitive rehabilitation approach can selectively target multiple cognitive domains in parallel. This can potentially optimize cognitive rehabilitation in MS by simultaneously delivering targeted interventions to persons with a broader range of cognitive dysfunction.
Cognitive–Motor Coupling and Cross-Modality Transfer Effects in MS?
One intriguing and recent observation is the coupling of cognitive and motor functions in persons with MS, and this might have implications for considering cross-modality transfer effects of exercise training and cognitive rehabilitation on cognitive and walking outcomes. For example, researchers reported associations between performance on neuropsychological tests of processing speed and executive function with upper (ie, 9-hole peg test) and lower (ie, T25FW) motor function in MS. 13 Others have reported statistically significant associations between tests of processing speed and multiple measures of walking performance (ie, MSWS-12, T25FW, 6MW, spatiotemporal gait kinematics). 14 There is further experimental evidence that performing a cognitive task concurrently while walking is associated with a reduction in walking performance compared with walking alone. 76 This has been termed the dual-task cost (DTC) of walking and represents cognitive–motor interference (ie, another indication of cognitive–motor coupling). The presence of coupling makes logical sense considering the overlap in brain regions associated with cognitive and motor functions, and the recognition that walking is not a simple motor task devoid of cognitive input. 77 The DTC of walking further has been associated with outcomes in MS, such as fall risk. 78 This underscores the importance of examining approaches for reducing cognitive–motor interference in MS and highlights the possibility of cross-modality transfer, for example, wherein cognitive rehabilitation could influence walking performance. 53 Some researchers have further suggested that we should consider combining cognitive rehabilitation and exercise training and examining the effect on cognitive and motor outcomes individually and together (DTC of walking) compared with single modes of rehabilitation.54,79
There is some preliminary evidence for cross-modality transfer effects regarding exercise training in MS. For example, previously reviewed studies of aerobic exercise training and other published studies of physical activity interventions have reported co-occurring improvements in cognitive and motor outcomes.44,80 We are unaware of research that has examined the effect of cognitive rehabilitation on both walking and cognitive outcomes in MS, but there is preliminary evidence that cognitive rehabilitation might have effects on walking in healthy older adults.53,81,82 For example, one RCT reported that older adults who underwent 10 weeks of cognitive rehabilitation, using the highly successful ACTIVE program, 83 demonstrated significantly better TUG performance (d = 0.73) than a waitlist control (ie, passive control); this study did not examine the effects of the ACTIVE program on cognitive outcomes. 81 We further are unaware of research on combining cognitive tasks with exercise training (ie, dual task training), and examining the effects on walking and cognitive outcomes alone and combined in MS, although this has been done successfully in healthy and cognitively impaired older adults.54,79,84,85 One recent systematic review of 8 RCTs summarized that combined cognitive and exercise training (ie, either delivered sequentially or as dual-task training) can be efficacious for improving everyday functioning, gait, and cognitive outcomes in healthy and cognitively impaired older adults.79,86 However, there is limited evidence that supports exercise and cognitive training combined when compared with cognitive or exercise training alone in those populations.54,79 The combined approach should seemingly translate into the largest improvements in co-occurring cognitive and motor deficits, and this might translate into large effects on the DTC of walking and associated real-world metrics such as street-crossing, as an example. There are many unanswered questions regarding the temporal sequence of such a combined intervention in MS, whereby each phase (ie, exercise and cognitive rehabilitation) might be more efficacious in different patient samples. For example, the efficacy of exercise training and cognitive rehabilitation interventions on walking and cognition might differentially depend on clinical characteristics, such as disability status 80 or domain of cognitive impairment.65,75 Nevertheless, there is much that can be learned from the gerontology literature and applied in a novel manner for managing cognitive and motor outcomes independently and collectively using exercise training and cognitive rehabilitation in MS.
Framework for Explaining Mechanisms of Exercise and Cognitive Rehabilitation
The possibility of cross-modality transfer effects for exercise and cognitive rehabilitation on cognition and walking should coincide with a framework for possible mechanisms. One proposed framework that has been recapitulated for identifying mechanisms of exercise training and physical activity effects on walking outcomes in MS focuses on improvements in physiological functioning.38,87 This model posits that physical inactivity initiates a cycle of deconditioning, and when a threshold of deconditioning is reached, physical inactivity results in walking dysfunction. 38 Such a model suggests that exercise training and behavioral interventions that target physical activity can stop, slow, or reverse walking dysfunction through improvements in physiological functioning, namely, aerobic capacity, muscle strength, and postural control, as a mechanism.38,88 There is evidence that better aerobic and muscular fitness are associated with better walking performance (eg, T25FW and 6MW) and spatiotemporal gait kinematics in MS, 89 and there is other evidence that those domains of fitness are associated with cognitive outcomes.90,91 There further is evidence from RCTs of exercise training that changes in fitness are correlated with changes in walking performance 48 and cognition 44 in MS. This suggests that the model of physiological mechanisms has some traction for explaining improvements in walking and cognition with exercise training in MS.
Another framework for examining mechanisms of exercise training and cognitive rehabilitation effects involves adaptations in CNS structures and connectivity for explaining improvements in walking and cognitive outcomes in MS. 92 For example, researchers have adopted the World Health Organization’s International Classification of Functioning (ICF) model for identifying entry points and mechanisms for explaining exercise training benefits in MS. 92 One of the entry points that is poorly understood involves exercise training effects on CNS structures, and how this might have downstream effects on other outcomes. There is cross-sectional evidence for cardiorespiratory fitness, as a marker of aerobic exercise training, being associated with information processing speed, brain structure (ie, grey/white matter integrity), and brain function (ie, greater activation of the right middle and inferior frontal gyri, and decreased activation of the anterior cingulate cortex during an executive function fMRI task) in MS.93,94 There are recent data indicating that cardiorespiratory fitness is associated with volumes of the thalamus, hippocampus, and basal ganglia nuclei in MS. 95 We further note that aerobic exercise training has improved the structure and connectivity of the hippocampus in memory-impaired persons with MS. 45 Collectively, this evidence combined with the extensive evidence in older adults 96 and emerging evidence in persons with psychiatric conditions (eg, schizophrenia 97 ) suggests CNS adaptations as an important mechanism for exercise training effects in MS, and perhaps for cognitive rehabilitation. Indeed, several studies in MS have reported improvements in brain structure 69 and function62,70,98 as potential mechanisms for the efficacy of cognitive rehabilitation.
Those 2 frameworks should be combined into a comprehensive model as has been done in aging. 99 That model, outlined in Figure 1, includes risk factors that are modifiable (eg, lifestyle behaviors, physical activity, 80 cognitive reserve100,101) as entry points for exercise training and cognitive rehabilitation interventions individually and combined (ie, interactions). Such entry points influence the CNS and other peripheral systems (ie, cardiopulmonary and musculoskeletal systems) independently and interactively. The CNS and peripheral systems influence the outcomes of mobility disability and cognitive dysfunction considering cognitive–motor coupling and associated overlap in regions of brain atrophy. There are further bidirectional paths in this model such that walking and cognitive consequences of MS could influence one another and lifestyle behaviors as well as CNS and physiological outcomes. Such a model could guide future interventions considering that it suggests possibly overlapping mechanisms for exercise and cognitive rehabilitation, as well as cross-modality transfer effects of exercise and cognitive rehabilitation on cognition and motor outcomes (ie, walking). We note that such an intervention would be limited to ambulatory persons with MS, given the emphasis on walking behavior. However, this approach might not be limited among those with RRMS, given evidence that exercise training improved walking and cognitive performance in persons with progressive MS. 44
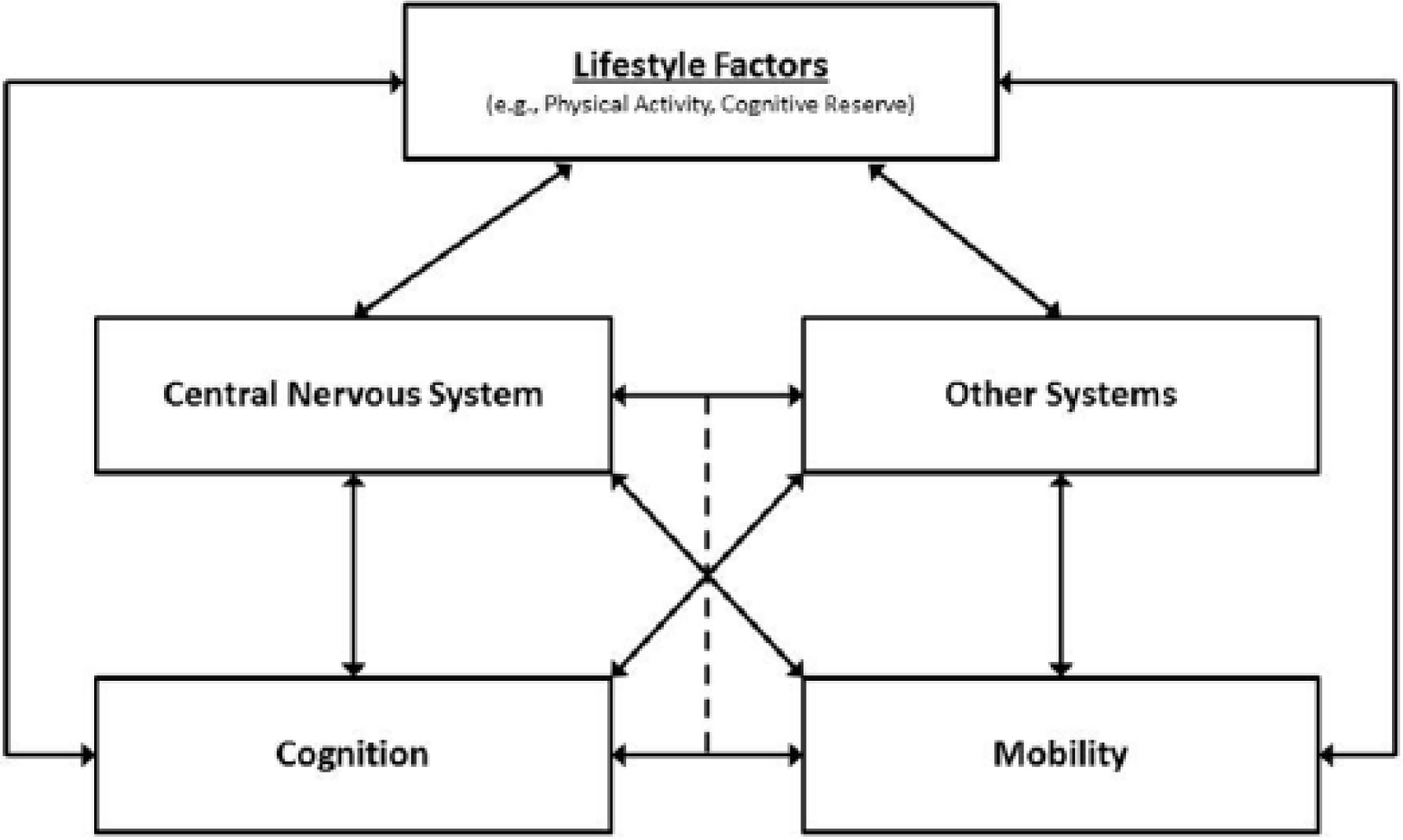
Model for possible cognitive and exercise rehabilitation effects on cognition and walking in multiple sclerosis.
Summary and Future Directions
Walking and cognitive dysfunction are both prevalent and disabling consequences of MS, and seemingly can be managed with rehabilitation. There are growing bodies of literature on exercise training and cognitive rehabilitation effects on walking and cognition. Classically, researchers have evaluated exercise training as an approach for improving walking function and cognitive rehabilitation as an approach for improving cognitive function, separately. Overall, there is promising evidence for aerobic and resistance exercise improving walking performance, and preliminary evidence supporting aerobic exercise for improving cognitive performance in MS. Although there is overall mixed evidence for cognitive rehabilitation improving cognitive performance in MS, recent evidence seemingly suggests that specific interventions for rehabilitating a single cognitive domain might exert particularly beneficial effects. There further have been no studies examining the effects of cognitive rehabilitation on walking outcomes in this population. However, there is burgeoning evidence that walking and cognitive functions co-occur, giving rise to the prospect that walking and cognitive dysfunction can be simultaneously improved through an individual or combined rehabilitation intervention, perhaps due to cognitive–motor coupling and/or cross-modality transfer effects. There is preliminary evidence supporting physical activity and exercise training as possible intervention approaches that improve both functions. Based on evidence from other populations, we highlight dual-task training and cognitive rehabilitation as other potential approaches to improve both walking and cognitive functioning in MS. This potentially symbiotic relationship warrants further study for optimizing rehabilitation research that targets walking and cognition as interrelated consequences of MS, rather than as separate constructs. To that end, we propose a framework for considering possible mechanisms whereby rehabilitation might exert beneficial effects on both ambulation and cognition and the interaction in this population. Researchers should consider examining the individual and combined effects of exercise training and cognitive rehabilitation on walking, cognition, and cognitive–motor interactions in MS, as well as the potential role of disability status and clinical course of MS on those effects. Researchers should particularly be aware that positive outcomes in progressive courses of MS might involve a stable level of function rather than an improvement in outcomes, per se. Such research should address possible physiological and central mechanisms for improving those functions, as well as cross-modality transfer effects and dual- versus single-task training effects on walking and cognition as two of the most common and burdensome outcomes of MS.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research described in this article was funded in part by Grants RG 4491A3/1 (Robert W. Motl) and CA 1069-A-7 (John DeLuca), both from the National Multiple Sclerosis Society.