
Abstract
Background. Converging evidence suggests that the amount of stepping practice is an important training parameter that influences locomotor recovery poststroke. More recent data suggest that stepping intensity and variability are also important, although such strategies are often discouraged early poststroke. Objective. The present study examined the efficacy of high-intensity, variable stepping training on walking and nonwalking outcomes in individuals 1 to 6 months poststroke as compared with conventional interventions. Methods. Individuals with unilateral stroke (mean duration = 101 days) were randomized to receive ≤40, 1-hour experimental or control training sessions over 10 weeks. Experimental interventions consisted only of stepping practice at high cardiovascular intensity (70%-80% heart rate reserve) in variable contexts (tasks or environments). Control interventions were determined by clinical physical therapists and supplemented using standardized conventional strategies. Blinded assessments were obtained at baseline, midtraining, and posttraining with a 2-month follow-up. Results. A total of 32 individuals (15 experimental) received different training paradigms that varied in the amount, intensity, and types of tasks performed. Primary outcomes of walking speed (experimental, 0.27 ± 0.22 m/s vs control, 0.09 ± 0.09 m/s) and distances (119 ± 113 m vs 30 ± 32 m) were different between groups, with stepping amount and intensity related to these differences. Gains in temporal gait symmetry and self-reported participation scores were greater following experimental training, without differences in balance or sit-to-stand performance. Conclusion. Variable intensive stepping training resulted in greater improvements in walking ability than conventional interventions early poststroke. Future studies should evaluate the relative contributions of these training parameters.
Keywords
Introduction
Despite substantial recovery of locomotor function in the first 6 months poststroke, 1 many patients continue to walk at slow speeds and over limited distances in the home and community. 2 Numerous therapeutic interventions designed to accelerate walking recovery have been investigated, although their relative efficacy remains unclear. Converging evidence suggests that the specificity and amount of task practice are critical determinants of locomotor recovery following neurological injury.2-4 For example, providing large amounts of stepping practice using weight-supported treadmill training has been shown to improve specific measures of walking function poststroke.5-7 However, equivalent gains have recently been observed following conventional strategies involving limited stepping practice. 8
Another training parameter that may be important is the intensity of stepping activities. Consistent with the field of exercise physiology, 9 intensity is defined as the rate of work performed (ie, power or workload) during locomotor activities and is estimated indirectly through metabolic and cardiorespiratory measures.9,10 Higher-intensity stepping training is performed by walking at faster speeds on a treadmill or overground2,11,12 or by increasing task demands 10 (eg, added weight to limbs/trunk). Such activities increase the neuromuscular and metabolic power generated during training and can lead to greater improvements in walking distance or aerobic capacity. Unfortunately, previous studies investigating the effects of high-intensity training in patients poststroke often utilize forward treadmill stepping as their primary intervention and often do not demonstrate gains in important locomotor outcomes, such as self-selected walking speed.2,11,12 Moreover, providing only forward stepping practice on a treadmill or overground leads to very small improvements in other functional tasks, including transfers and postural stability,2,11,13 which are essential to many activities performed in the home and community. As such, implementation of such training may be limited by the need to practice these other tasks.
One training parameter that has received less attention is the variability of stepping training. Recent data from animal models of spinal cord injury indicate greater stepping recovery following training in different directions (backward or sideways), overground or over stairs, as compared with forward treadmill training.14,15 These gains in locomotor function were observed despite substantially less stepping practice than forward stepping and with little regard for normal gait kinematics. Allowing variability and increasing task difficulty during locomotor training, particularly at high intensities, deviates considerably from traditional rehabilitation strategies that direct their attention toward “normalizing” gait patterns and minimizing errors during stepping.16-18 Long-standing data in motor control research indicate that introducing variability into a specific task increases the number of errors performed during practice,19,20 although performance on retention tasks is improved. If patients can adjust their locomotor strategies to correct errors during task performance, allowing or augmenting errors has the potential to improve task performance, as observed previously.21-23
Practice of only high-intensity stepping training with variable contexts is rarely performed in patients with subacute stroke. Our recent preliminary data from individuals 1 to 6 months following a single stroke suggest that a training strategy to maximize stepping practice in multiple, variable contexts and performed at high intensities was feasible and resulted in significant improvements in locomotor function and symmetry 24 as well as in nonwalking tasks (balance and transfers). 25 Such training emphasized progressive increases in the difficulty of variable walking tasks in different environments, with focus only on task completion (ie, continued stepping) and with minimal focus on normalizing gait patterns. This strategy contrasts sharply from conventional clinical interventions, which focus on ameliorating impairments and provide practice of multiple functional tasks, 26 performed at reduced cardiovascular intensity, 27 with attention toward normalizing movement patterns. 16 Despite these preliminary data, the superiority of this high-intensity, variable stepping training as compared with more conventional strategies on recovery of walking function is not clear.
The primary aim of this assessor-blinded randomized trial is to examine the efficacy of high-intensity, variable stepping training on walking and nonwalking outcomes in individuals with subacute stroke as compared with conventional interventions. Information from this study may provide insight regarding the potential importance of specific training parameters to improve walking and other functional tasks.
Methods
The present study was conducted over 2 years; all procedures were approved by the local ethics committee with written informed consent and medical clearance required to participate.
Study Sample and Design
Individuals with a single, unilateral, supratentorial stroke in the previous 1 to 6 months were recruited consecutively from surrounding inpatient and outpatient clinics. All participants were required to walk 10 m overground with minimal or moderate physical assistance from a therapist or without physical assistance but at speeds ≤0.9 m/s at self-selected speeds (SSSs) with assistive devices and below-knee bracing as needed. Exclusion criteria included the following: previous central or peripheral nervous system or orthopedic injury that may limit independent ambulation, uncontrolled cardiorespiratory disease, or inability to follow 3-step commands. Participants were stratified into 4 groups according to the amount of physical assistance and gait speed (requiring moderate assistance, requiring minimal assistance, <0.5 m/s without assistance, between 0.5 and 0.9 m/s without assistance). Patients were randomized to control versus experimental groups using a blocked design (4 per block), with allocation generated by computer software and concealed by a research assistant not involved in the study. Preliminary outcomes following experimental 24 training performed in patients with subacute stroke (0.32 ± 0.20 m/s) and less-intensive control (0.15 ± 0.09 m/s) 28 interventions indicated that 16 individuals in each group would provide 95% power (pooled standard deviation = 0.13 m/s).
Intervention
Patients randomized to either training group received up to 40 training sessions of 1 hour each over 10 weeks (4-5 sessions/wk). Both groups were asked to wear validated, reliable accelerometers 29 (StepWatch, Modus, Inc) on their paretic ankle throughout each day of study enrollment, including during training sessions and outside of training sessions. Days with <10 steps recorded were excluded from analysis in both groups and assumed to be artifacts (ie, not worn by the participant). Participants were also asked to wear step monitors ~2 weeks before the start of training sessions, throughout training, and 2 weeks following posttraining (POST) and follow-up (F/U) testing.
The experimental training protocol has been described previously in detail 24 and was delivered by 1 of 5 therapists in the laboratory, with previous training and discussion of the training protocol. 24 During training sessions, the research physical therapist’s primary goals were to maximize the individual’s stepping activity at high intensities, in variable contexts described below, for up to 40 min/session. Therapists would focus on a patient’s individual gait deficits with tasks and in simulated environments that the participant would encounter in the home and community. During the first week, only forward treadmill training was performed (speed-dependent treadmill training), with a goal to maintain heart rate (HR) within 70% to 80% of HR reserve or ratings of perceived exertion (RPE) ≥14. The targeted training zone of 70% to 80% HR reserve was calculated using age-predicted maximum HR (ie, HRmax = 208 − [0.7 × age] 30 ) and the Karvonen formula, 9 where 70% HR reserve = 0.7 × (HRmax − HRrest) + HRrest, and was recorded using pulse oximeters (Rad-57, Masimo Corp). Limb swing assistance, body weight support, and nylon straps stabilizing the pelvis were provided as necessary to ensure successful stepping, as characterized by positive step lengths, lack of stance-phase limb collapse, and sagittal/frontal plane stability. 24 Research therapists did not focus on lower-extremity kinematics if individuals could continue stepping according to the above criteria. Ankle foot orthoses or posterior knee braces were allowed to minimize orthopedic concerns.
Training at high cardiovascular intensities over the remaining sessions was focused on variability of stepping tasks and divided into ~10-minute increments between speed-dependent treadmill training (described above), skill-dependent treadmill training, overground training, and stair climbing. Skill-dependent treadmill training was performed by applying perturbations to challenge postural stability, propulsion, and limb swing and included walking in multiple directions, over inclines and obstacles, and/or with weighted vests and leg weights with limited handrail use as tolerated. Perturbations were applied such that 2 to 5 different tasks were randomly alternated and repeated within 10-minute periods. The difficulty of tasks was reduced when participants were not successful for 3 to 5 consecutive stepping attempts. Overground training focused on high speeds or variable tasks as described, with use of a gait belt or overhead mobile or rail suspension system for safety. Stair climbing was performed over static or rotating stairs (Stairmaster, Vancouver, WA) using reciprocal gait patterns with progression to higher speeds and reduced hand rail use. If specific tasks were not practiced during individual sessions, subsequent sessions focused on missed tasks.
Patients allocated to the control group were encouraged to continue concurrent physical therapy as possible, with details of the timing and types of therapeutic activities extracted from medical records, as available. Clinical physical therapists were not asked to alter practice patterns. Control therapy sessions were supplemented by research therapists in an effort to achieve 40 sessions over 10 weeks. Interventions during supplemented sessions were performed away from other experimental sessions by the research therapists. The supplemental sessions focused explicitly on practice of multiple therapeutic tasks consistent with conventional physical therapy activities as described in a multisite observational study. 26 The amounts and types of specific lower-extremity activities from this study included (mean repetitions [confidence intervals]) the following: active exercises (75 [58-93]); passive/stretching exercises (12 [9-16]); transfers (11 [9-13]); balance activities (27 [19-35]); gait (357 [296-418]), and stairs (3 episodes [2-4]). These values were used as targets during control training sessions. Steps/session were augmented during supplemental sessions to achieve stepping activities as observed in a separate observational study (mean ± standard deviation = 886 ± 852 steps/session). 2 Data from this latter study were reanalyzed, and a significant relation between stepping activity and gait speed was observed as follows: Steps/session = 200 + 1500 × Initial SSSs. For the present protocol, we calculated the targeted steps/session for each person based on their gait speed to ensure that stepping activity was consistent with the largest estimates available. Steps were recorded during supplemental control sessions by the accelerometers for later analysis, and targeted stepping amounts were approximated using hand-held step counters during sessions.
Stepping practice was delivered both on the treadmill and overground and without restrictions on cueing and feedback. Intensity of all activities was targeted at 30% to 40% of their HR reserve, consistent with data from observational reports of conventional physical therapy in subacute stroke. 27 Therapists could focus on kinematic tasks as deemed appropriate, particularly at these lower intensities. The treating research therapist progressed patients with assistive devices and bracing as deemed appropriate to progress functional independence.
Outcomes
All clinical and walking laboratory outcome measures were performed by blinded raters at baseline assessments (BSLs), midtraining (MID), and POST, with a 2-month F/U. Primary outcomes included walking speed at SSS and fastest-possible speeds (FSs) over short distances using a pressure-sensitive walkway (GaitMat, Chalfont, PA) and walking distance during the 6-minute walk test (6MWT) performed at SSS. 24 If participants required physical assistance, speed and distance were documented, with 0 m/s documented for SSS and FS and 0 m for 6MWT. 24 Data on daily stepping (steps/day) in the home and community were collected at BSL, POST, and F/U, with data averaged over a minimum of 5 days up to 14 days as available, where ≥3 days is sufficient to reliably estimate stepping activity. 31 We also asked participants to wear step monitors/accelerometers at all times throughout the entire training period, including during and outside of therapies, to evaluate stepping activity both within sessions (steps/session) and outside of sessions (steps/day during training). Stepping activity was not recorded by blinded assessors.
Secondary gait measures included indicators of spatiotemporal symmetry. Temporal symmetry was evaluated as percentage gait cycle paretic single-limb stance at SSS and FS. Spatial symmetry was determined using step-length symmetry 24 as follows:
where 100% indicates perfect symmetry. Given the variability in this measure, 24 we also calculated absolute differences in step lengths (0 cm = perfect symmetry) across assessments.
Secondary clinical measures included the Berg Balance Scale (BBS) and the timed 5-times sit-to-stand (5XSTS) transfer task. 25 Self-reported measures included the Activities-Specific Balance Confidence (ABC) Scale 32 and the Physical Subscale of the Medical Outcomes Short-Form 36 (Physical SF36). 8
Additional measures included baseline assessment of the lower-limb Fugl-Meyer assessment 33 and the Patient Health Questionairre-9 8 for depressive symptoms. Furthermore, the number of adverse events during or outside of interventions throughout training was tabulated, including major events such as fall incidence, fractures, or cardiorespiratory or neurological events requiring hospitalization, as well as minor events of skin breakdown, joint or back pain, or complaints of increased spasticity.
Analysis
Baseline characteristics and training parameters were compared between treatment groups using unpaired t tests, Mann-Whitney U, and χ2 comparisons as appropriate, with ratio data tested for normality. Data were utilized for all participants who met inclusion and were tested at BSL, with data imputed for any missing assessments from the last testing period. All participants were evaluated at least once at MID, POST, or F/U. All data are presented as means ± standard deviations in tables and text, with means ± 95% confidence intervals in figures. All parametric measures were analyzed using a 2-way repeated-measures ANOVA, with main factors of treatment (experimental vs control), and repeated for time (assessments). Post hoc t tests at each time were performed for primary outcomes only with significant interactions. Significance was set at α = .0125 with Bonferroni corrections made for the 4 primary repeated-measures ANOVA comparisons, and α = .05 for post hoc and secondary measures. Secondary exploratory analysis also included correlation and stepwise multiple linear regression analysis to evaluate the contributions of training parameters (steps/session, steps/day, and stepping intensities) on primary locomotor outcomes at POST assessments, with α = .05.
Results
Screening evaluations were performed on 151 individuals, of whom 33 individuals met all inclusion criteria and were subsequently enrolled (Figure 1) and randomized to experimental (n = 16) or control interventions (n = 17). For 1 experimental participant, an assessor could not be blinded for any outcome assessment, and these data are excluded from the final analysis (n = 15), with results not statistically different with inclusion. Of this final group, 2 individuals were nonambulatory, and 4 could not perform the 5XSTS in the experimental group at BSL. In the control group (n=17), 1 person was nonambulatory, and 3 could not perform the 5XSTS. Also, 4 participants in the experimental group and 1 in the control group could not attend the F/U session, and their data from POST assessments were imputed. Table 1 provides the demographic characteristics and baseline impairments of the participants who initiated the study protocol, indicating no differences between training groups.
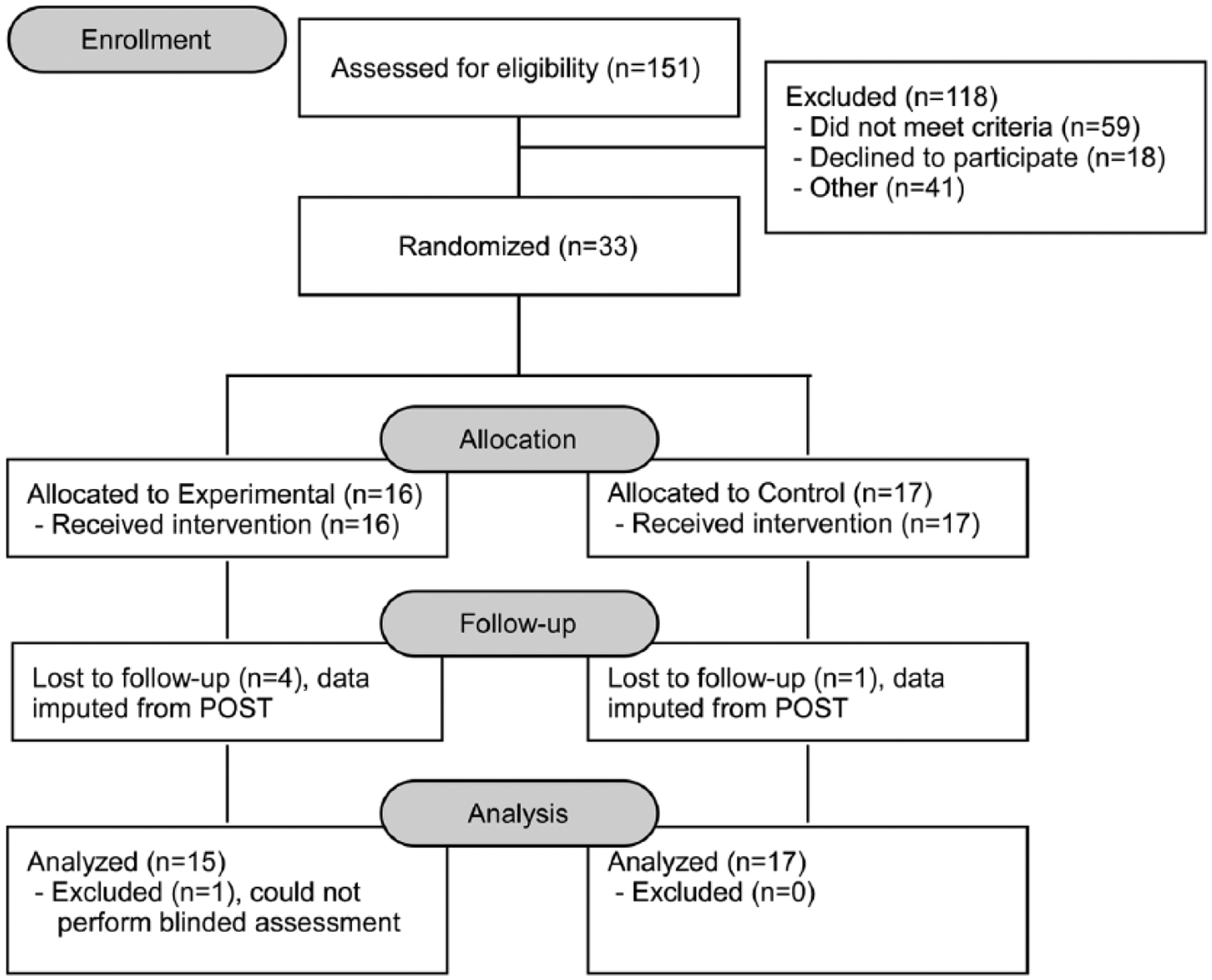
CONSORT diagram.
Demographics and Clinical Characteristics.
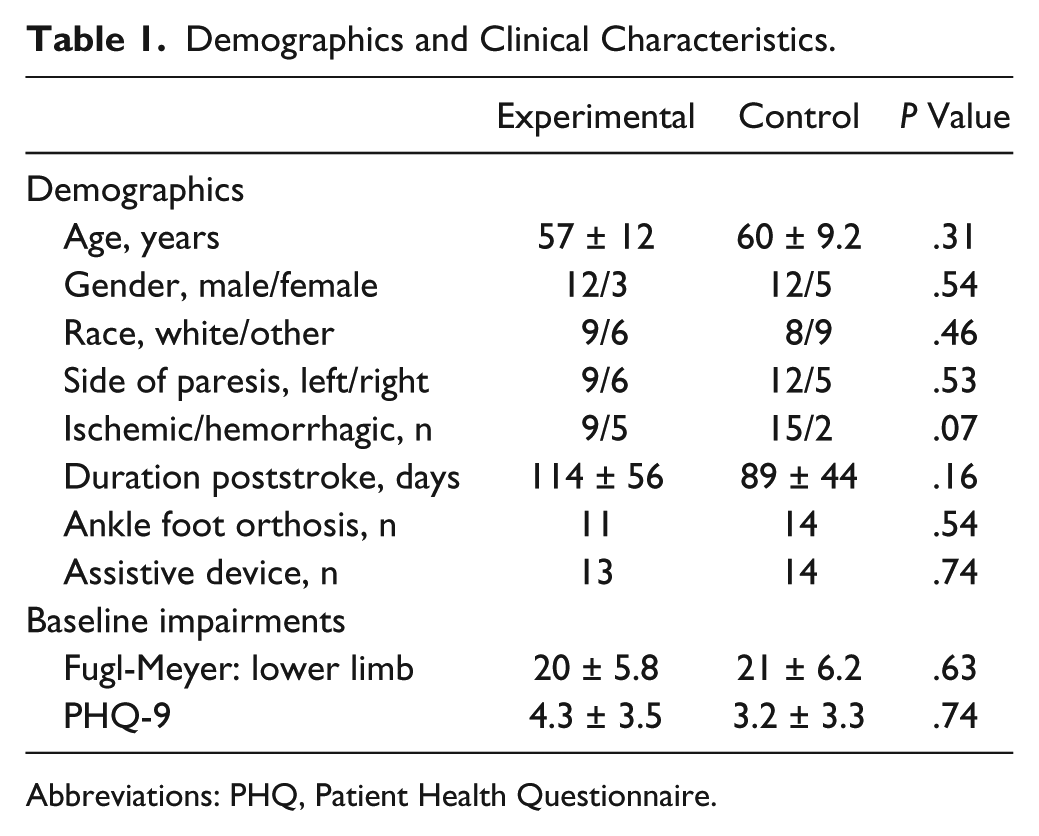
Abbreviations: PHQ, Patient Health Questionnaire.
Details of the training interventions are provided in Table 2. There were no between-group differences in number of sessions, with details of within-session activities available for all experimental training. For control therapies, a mean of 26 ± 7.6 supplemental sessions per participant were provided to control participants by research staff. For within-session activities, we were able to collect steps/session in 76% of control sessions and details of the types of activities in 68% of sessions. Barriers to obtaining these details from remote rehabilitation centers included difficulty accessing therapy notes and accurate determination of start time of therapy despite use of the accelerometers throughout the day, including during therapy sessions. Of the available sessions, significant between-group differences of ~1500 steps were observed for steps/session and for steps/day during the training period. Significant differences were also observed for intensity measures of peak HR reserve and peak RPE achieved during sessions, with intensity data for control interventions available only for supplemented sessions. There was a significant correlation between steps/session and mean peak HR reserve (r = 0.76; P < .01) but not RPE achieved (r = 0.29; P > .05).
Training Interventions.
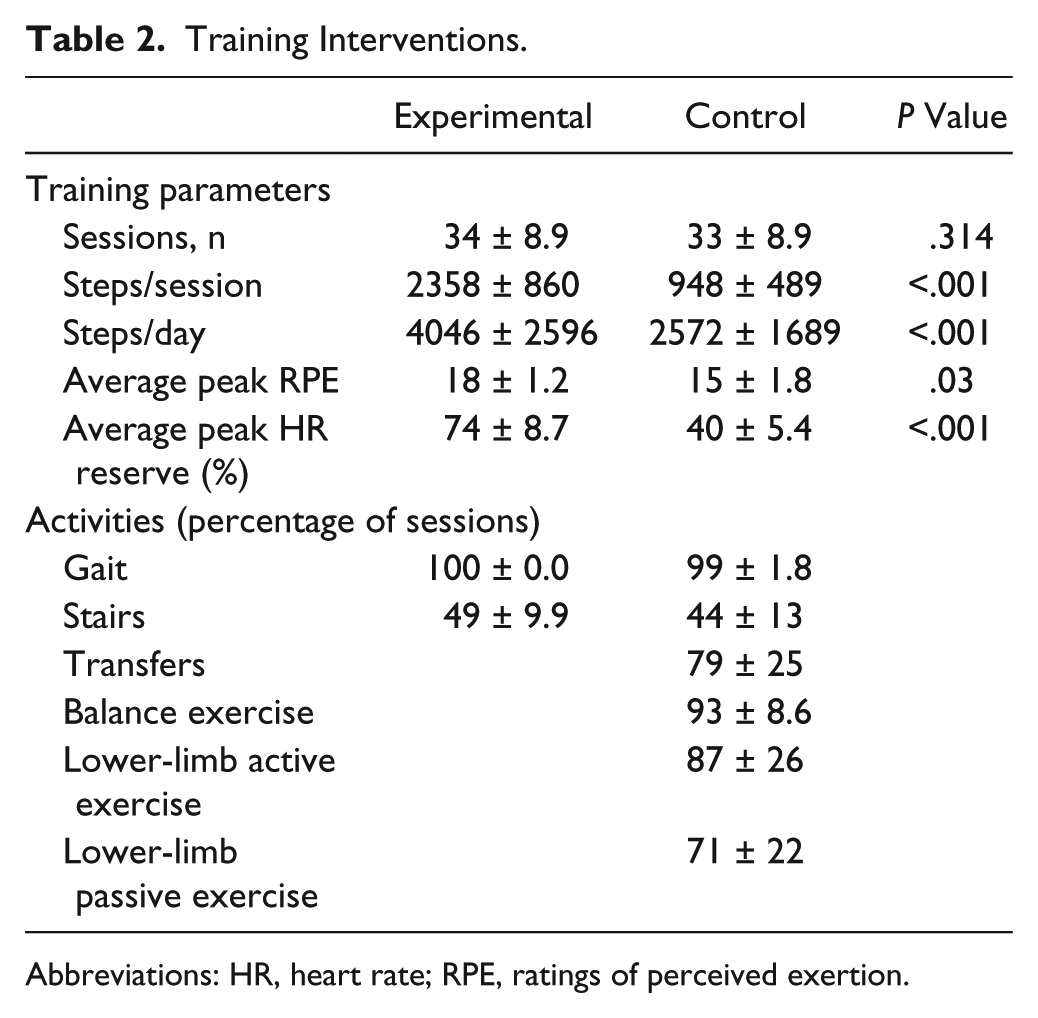
Abbreviations: HR, heart rate; RPE, ratings of perceived exertion.
Primary outcomes (Table 3) were not different between groups at BSL. During and following training, however, repeated-measures ANOVAs revealed significant interactions of treatment and time between groups for SSS, FS, and 6MWT, with no differences in daily stepping activity at BSL, POST, and F/U. Exclusion of patients whose data were imputed from POST to F/U revealed similar, significant gains from BSL to POST in both experimental and control interventions for laboratory gait measures. Figures 2A and 2B demonstrate the changes in SSS and 6MWT during the study, with significant between-group differences in MID, POST, and F/U. Comparisons at POST indicate 3- to 4-fold greater improvements in the experimental group for ΔSSS (experimental, 0.27 ± 0.22 m/s, vs control, 0.09 ± 0.09 m/s) and Δ6MWT (119 ± 113 m vs 30 ± 32 m).
Outcomes: P Values for Interaction Effects of Time and Group.
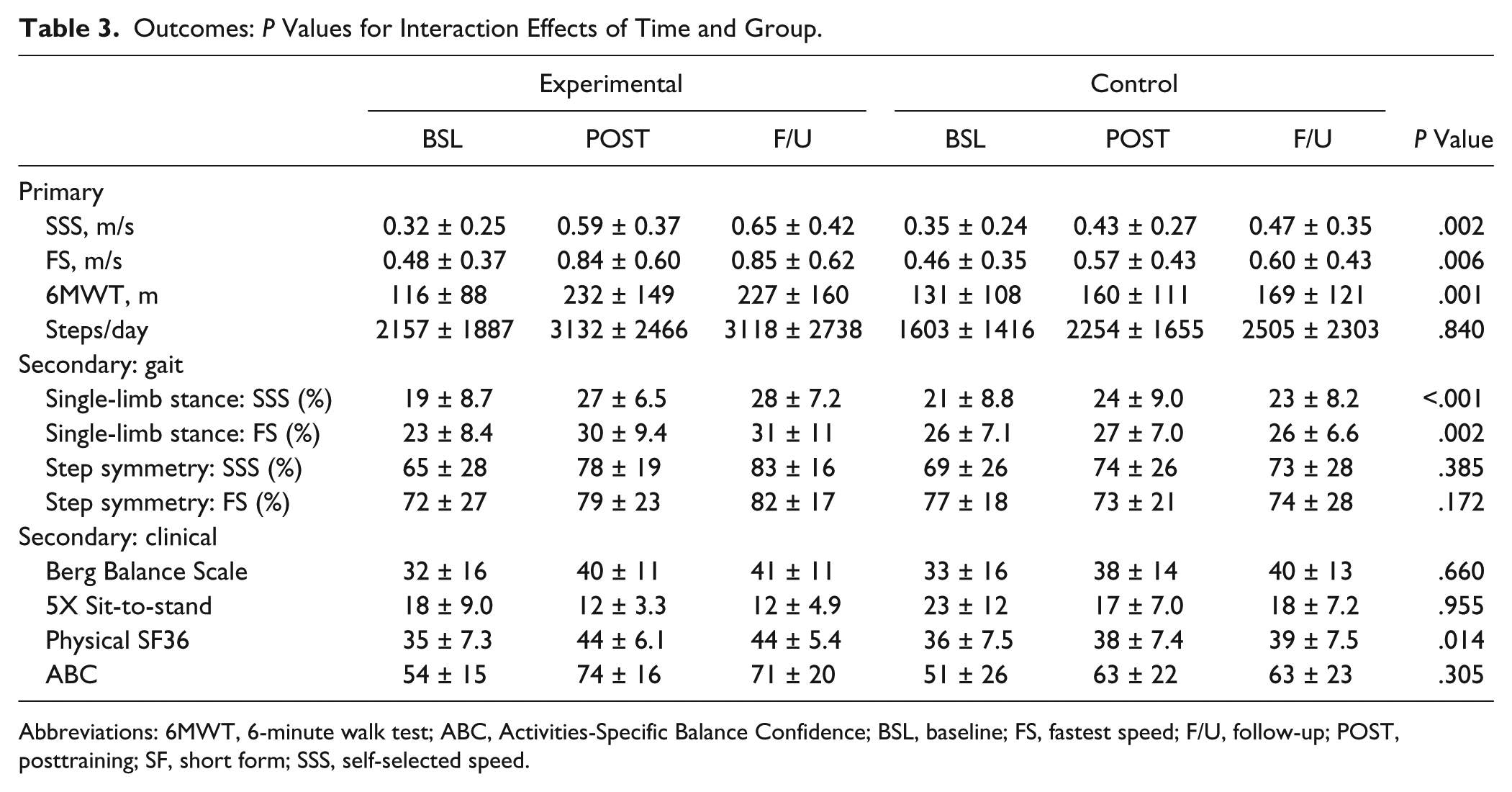
Abbreviations: 6MWT, 6-minute walk test; ABC, Activities-Specific Balance Confidence; BSL, baseline; FS, fastest speed; F/U, follow-up; POST, posttraining; SF, short form; SSS, self-selected speed.
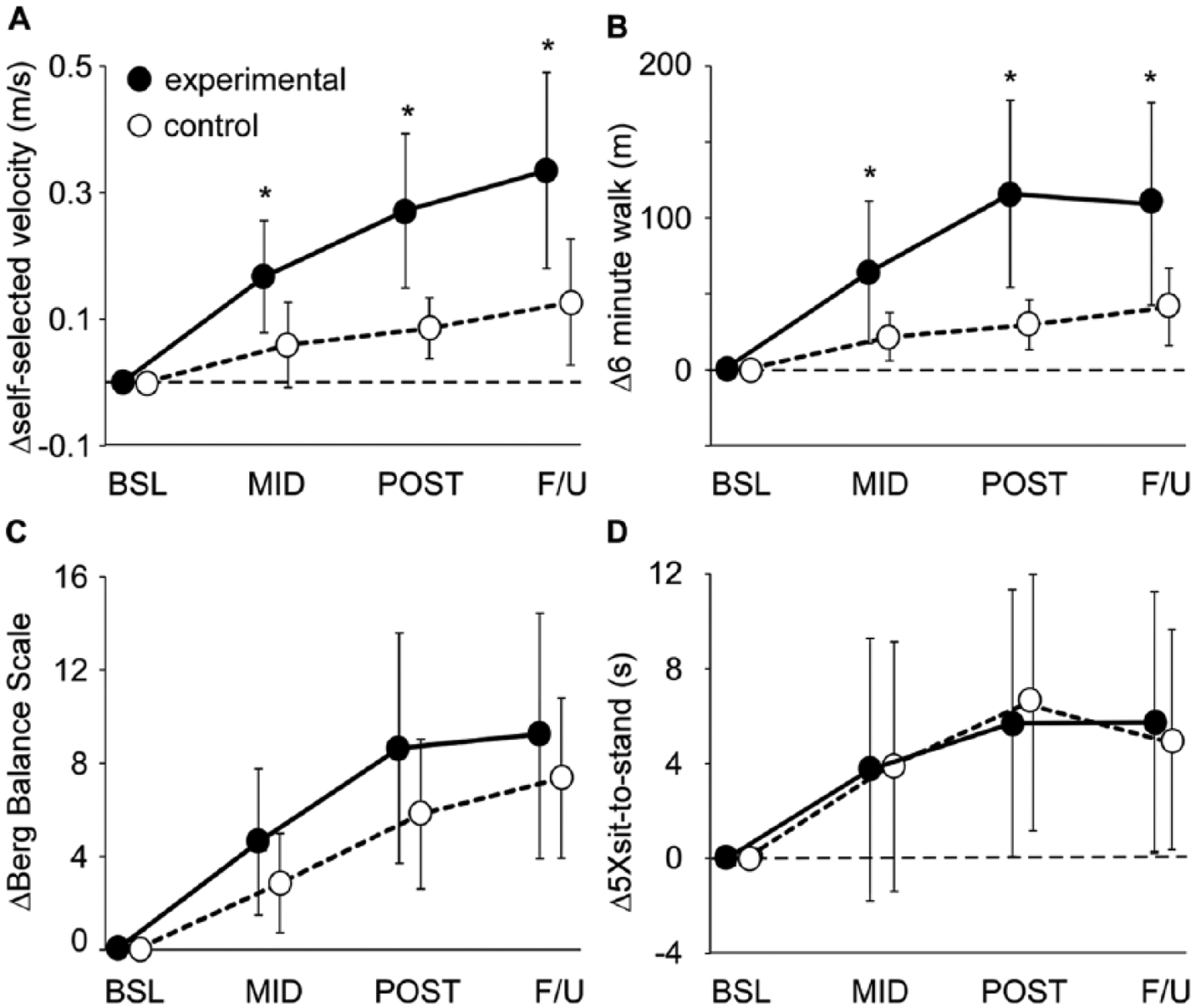
Changes in primary outcomes of self-selected speed (A) and 6-minute walk test (B) in training groups at baseline (BSL), midtraining (MID), posttraining (POST), and follow-up (F/U), with post hoc significance denoted by asterisk (*). Changes in Berg Balance Scale (C) and 5X sit-to-stand (D) were not significant.
Secondary gait measures of spatiotemporal symmetry demonstrated significantly greater improvements in paretic single-limb stance in the experimental versus control groups at SSS and FS. Specific changes in the experimental group at POST included mean improvements of 6% to 8% in single-limb stance closer to normative values (~40%), with improvements of only 1% to 3% in the control group. For step length symmetry, mean changes of 7% to 13% were observed in the experimental group, with more inconsistent changes following control interventions (−4% to 5% changes). However, between-group differences in step length symmetry were not significant, and reanalysis of absolute step length differences also indicated no differences between groups (eg, Δstep length differences at SSS from BSL to POST: 1.9 ± 10 vs 1.8 ± 9.3 cm).
Secondary clinical assessments revealed large differences between Physical SF36 scores between training groups and POST and F/U. There were, however, no between-group differences in improvements in BBS (Figure 2C), 5XSTS (Figure 2D), or ABC. Improvements in BBS were different from BSL to POST in both experimental and control groups (8.5 ± 9.5 and 5.4 ± 6.5; both P < .01). For 5×STS, significant improvements from BSL to POST were observed in the control group (6.5 ± 9.5s, P < .05), with gains in the experimental group approaching significance (5.6 ± 8.7s, P = .056). Of the patients who could not perform 5XSTS at BSL testing, 3 of 4 experimental participants and 2 of 3 control participants were able to complete the task at POST.
Correlation analyses revealed significant associations between mean steps/session and changes in selected primary outcomes. Correlations for SSS and 6MWT are demonstrated in Figures 3A and 3B (both P < .01), with smaller but significant correlations with FS (r = 0.48, P < .05, not shown). Similar or slightly lower correlations were observed between steps/day throughout all training and including sessions (r values = 0.39-0.65) and primary laboratory-based outcomes. There was no correlation between steps/session with changes in stepping activity from BSL to POST assessments (r = 0.22; P > .05).
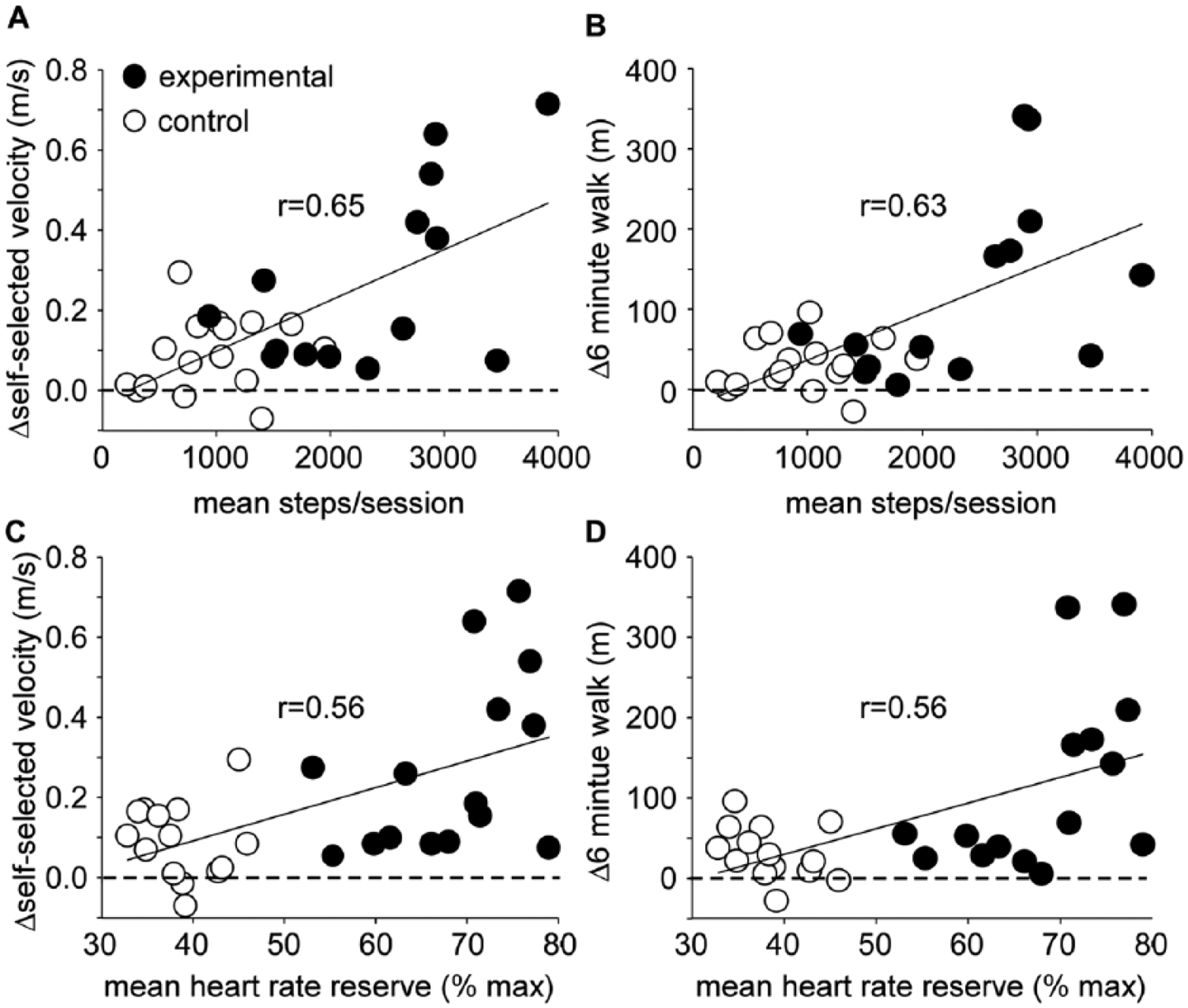
Significant correlations between steps/session (A-B) and average peak heart rate reserve (C-D) with self-selected speed and 6-minute walk test at posttraining assessments.
Significant associations were also observed with training intensity, as depicted with HR reserve (Figures 3C and 3D), but not peak RPEs during training (r values < 0.10, not shown). However, stepwise linear regression using steps/session and HR reserve as independent predictors revealed that only steps/session was related to changes in SSS (r2 = 0.42; P < .01) or 6MWT (r2 = 0.36; P < .01).
Adverse events were observed in both groups, including equivalent number of falls outside of therapy without injury (8 in experimental, 9 in control). No cardiovascular events occurred in the control group, although 2 occurred in the experimental group requiring brief hospitalization, including elevated blood pressure prior to a training session and aspiration at home; both participants resumed training following medical reclearance. In addition, 2 individuals in the control group experienced seizures (which occurred outside of training), both of whom resumed training following discharge. Other minor events included skin breakdown (3 experimental/3 control), joint or back pain (3/1), and increased report of spasticity (1/0). When patients reported joint/back pain and increased spasticity, training activities were modified to mitigate symptoms.
Discussion
The present data extend upon preliminary assessments of variable, high-intensity stepping training24,25 with comparisons to outcomes following conventional physical interventions in participants with subacute stroke. The types, amounts, and intensities of stepping practice performed during experimental training were similar to our published data, 24 although such training is rarely performed in patients early poststroke. Rather, traditional rehabilitation models 16 and current physical therapy texts17,18,34 focus on impairment-based approaches and attempt to normalize kinematics, particularly in the initial stages after injury. Available data of activities performed during clinical treatment of patients poststroke are consistent with these models, with practice of multiple tasks2,26 at low exercise intensities, 27 consistent with our control training paradigm. Direct comparison of the effects of high-intensity variable stepping paradigm with conventional strategies utilized in control training revealed 3- to 4-fold greater improvements in walking function in the experimental group. These between-group differences were above thresholds for minimally clinically important differences (SSS: 0.10 m/s; 6MWT: 50 m), 35 which were maintained at F/U. The potential importance of amount and intensity of stepping practice was further highlighted by the significant associations between these training variables with primary clinical walking measures.
Between-group differences in secondary measures of paretic limb stance and step-length symmetry are of specific interest, given the minimal focus on gait kinematics during variable stepping practice. Significant improvements in paretic limb stance time were observed following experimental versus control interventions, whereas no differences were observed in step-length symmetry. Our variable stepping training incorporated tasks of increasing difficulty with applied perturbations to augment errors, which has been utilized in neurologically impaired populations during studies targeting specific locomotor tasks (limb swing or step symmetry).21-23 Despite disruption or potential worsening of gait kinematics during application of these specific perturbations, improvements in locomotor performance are observed following their removal. The present data are consistent with these latter studies and may help clinicians understand the importance of errors and variability during walking training, even in patients early following injury.
The findings of equivalent changes in BBS and 5XSTS between training groups are of further interest because the experimental group did not focus on these tasks. Significant gains were observed for both groups, with mean changes above thresholds for minimal detectable changes (~6 points 36 ) in patients with acute stroke. Similar improvements above the minimal detectable changes for 5XSTS (3.6 s 37 ) were also observed, consistent with our preliminary data. 25 Notably, very small changes in BBS (<2 points) and 5XSTS (< 3 s) are typically observed following interventions that utilize only forward treadmill training.2,11-13 Why these measures improve with the present experimental protocol and not forward treadmill training are not entirely clear, although a previous suggestion is that the biomechanical demands of the stepping tasks practiced (eg, stairs, multidirectional stepping) are similar to the demands of the BBS and 5XSTS. 25 Repeated practice of these variable stepping tasks may facilitate improvements in neural circuitry and volitional activation of muscle groups subserving these nonwalking tasks. 25 Whereas future studies may explore potential mechanisms underlying these improvements, the present data suggest that these training strategies may increase the efficiency of rehabilitation sessions by improving function in multiple mobility domains. 25
Despite these combined gains, there were no significant differences in improved stepping activity between intervention groups. Conversely, however, significant differences in Physical SF36 scores were observed favoring experimental training. These data present a disconnect between self-reported and objective measures of physical activity, as reported previously in this patient population. 38 Further research may be required to provide interventions directed toward patients’ understanding of their limited stepping activities and to increase daily stepping activity, which is critical to minimize secondary complications poststroke.
Although the experimental training elicited large amounts of stepping activity during training, steps/session were still 1000 to 1500 steps lower than that achieved during only treadmill stepping. 2 However, the present gains compare favorably with published data detailing the effects of forward stepping activities with limited variability.8,11,12 For example, the LEAPS study 8 comparing treadmill and limited overground stepping with strength and balance exercise in patients earlier poststroke (~60 days) demonstrated smaller differences in 6MWT than observed here. In another recent study using patients with subacute stroke, 39 comparisons of variable stepping to forward treadmill training elicited no differences between groups, although their improvements were markedly smaller than those observed here. Both studies did not emphasize training intensity,8,39 which could contribute to the differences between studies. Long-standing data suggest that greater alterations in cardiorespiratory2,12 and neuromuscular40,41 function can contribute to selected walking changes following high-intensity training on a treadmill, although changes in self-selected walking speed are still limited.2,11,12
Why these experimental strategies elicited the observed gains in locomotor function as compared with other stepping strategies28,39 is uncertain but are consistent with our preliminary reports.3,24,25 Our goals of focusing the applied interventions to increase variability and encourage errors for specific biomechanical stepping tasks, particularly at high intensities, is quite different from variable training described in the aforementioned study. 39 The error-enhancing strategies used here were modeled after published studies directed toward specific gait components.21-23 Those strategies are very focused, however, whereas the present strategy targeted patients’ multiple gait deficits during training. The present training strategy bears some similarity to recent animal studies detailing the improvements in forward locomotion with variable stepping training (ie, sidestepping, backward, and stairs).14,15 Those authors hypothesized that variability of stepping training may recruit more expansive neural circuitries underlying different stepping tasks while still focusing on the fundamental task of walking. Repeated recruitment of these different neural circuits, particularly at high intensities, could allow greater performance of tasks that engage more limited circuitries (ie, forward stepping). The differential and combined contributions of intensity and variability of stepping tasks on walking recovery should be identified in future work to provide specific recommendations of the key variables necessary to maximize locomotor function.
An advantage of the present study is our monitoring of stepping activities in participants throughout the study. Such monitoring can provide greater insight into how practice both within and outside of research or clinical interventions are related to outcomes; this is not often performed in research studies. Despite these recordings, the difficulty in obtaining therapy records from remote rehabilitation centers limited our ability to accurately delineate the type, amount, and times of all therapies delivered in approximately 24% to 32% of control intervention sessions. These missing data may have contributed to the correlations presented of steps/session versus outcomes. However, recording of total steps/day throughout training was available, revealing associations between steps/day and steps/session that were similar to primary walking outcomes. We are, therefore, not certain that these missing data influenced the main outcome of differences between groups. More stringent control of other therapy sessions will be necessary to better determine the amounts, intensities, and types of practice received during all therapies.
A related limitation of this study is the lack of ability to remotely monitor other pertinent training parameters during clinical therapies, including performance of tasks other than walking 42 or measures of intensity, which can be related to motor recovery. Future advances in remote sensor technology may facilitate better understanding of tasks performed both within and outside of scheduled therapy sessions.
Additional limitations of the present study include the inability to achieve 40 sessions for each patient and a relatively small sample size. For scheduling therapies, all research staff worked with participants to attempt to achieve all sessions, and our preliminary data suggest that participants were able to achieve an average of 90% of sessions. Despite attendance of only ~83% to 85% in the present study, similar numbers of sessions between groups suggest that this was not a factor contributing to our results. For sample size, initial power analyses based on preliminary data suggest a relatively small sample would be required to see differences between the distinct training interventions. Such samples were based on previous investigations of the efficacy of training interventions on similar patient populations, without the constraints of additional physical therapy that may contaminate functional outcomes. Larger sample sizes in future studies will be needed to validate these findings.
Conclusions
Focused variable stepping training at high intensities elicits significantly greater gains in walking function and participation as compared with conventional interventions. The magnitudes of the differences in SSS and 6MWT between groups were also above clinically significant thresholds. Differences were also observed in temporal gait symmetry, whereas standing balance or STS performance demonstrated equivalent gains. Future studies should continue to delineate the relative contributions of specific training parameters to maximize locomotor recovery in this patient population.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by National Institute of Disability and Rehabilitation Research H133B031127 and H133B140012, the Chicago Blackhawks Foundation, and the Bullock Foundation.