
Abstract
Background. The velocity of reaching movements is often reduced in patients with stroke-related hemiparesis; however, they are able to voluntarily increase paretic hand velocity. Previous studies have proposed that faster speed improves movement quality. Objective. To investigate the combined effects of reaching distance and speed instruction on trunk and paretic upper-limb coordination. The hypothesis was that increased speed would reduce elbow extension and increase compensatory trunk movement. Methods. A single session study in which reaching kinematics were recorded in a group of 14 patients with spastic hemiparesis. A 3-dimensional motion analysis system was used to track the trajectories of 5 reflective markers fixed on the finger, wrist, elbow, acromion, and sternum. The reaching movements were performed to 2 targets at 60% and 90% arm length, respectively, at preferred and maximum velocity. The experiment was repeated with the trunk restrained by a strap. Results. All the patients were able to voluntarily increase reaching velocity. In the trunk free, faster speed condition, elbow extension velocity increased but elbow extension amplitude decreased and trunk movement increased. In the trunk restraint condition, elbow extension amplitude did not decrease with faster speed. Seven patients scaled elbow extension and elbow extension velocity as a function of reach distance, the other 7 mainly increased trunk compensation with increased task constraints. There were no clear clinical characteristics that could explain this difference. Conclusions. Faster speed may encourage some patients to use compensation. Individual indications for therapy could be based on a quantitative analysis of reaching coordination.
Introduction
Impairment of upper-limb motor control is a major cause of disability in patients with stroke-induced cerebral lesions. It is well known that reaching and grasping movements in hemiparetic patients are slow and segmented,1,2 but the mechanisms that cause the slowness are still unclear. Movement slowness may be the direct consequence of the weakness which occurs after a brain lesion.3,4 The impairment of coordination due to the lack of corticospinal control likely contributes through impairment of individual joint control5,6 and disruption of agonist-antagonist muscle coordination 7 and interjoint coordination.8,9 In addition, excessive muscle contractions due to spasticity,10,11 spastic co-contraction, 12 and pathological synergies13,14 have all been suggested to potentially slow movement with segmented and irregular trajectories. 15
Recently, several studies demonstrated that hemiparetic patients were able to perform faster movements when required to do so and that a faster speed of execution improved movement quality, as appreciated by smoothness.16-19 However, the impact of faster speed instruction on movement extent and coordination has not yet been investigated. Voluntary increases in reach velocity may influence movement execution across joints and may also lead to inappropriate muscle activity in hemiparetic patients.
In healthy subjects, Gottlieb et al 20 examined the regulation of movement velocity in a single joint and proposed two modes of pulse step control. In the default mode (speed insensitive strategy) the automatic changes in velocity according to target distance would be regulated by the duration of the pulse step, while in the speed-sensitive strategy, when the velocity is related to an explicit speed instruction, it could be regulated by pulse intensity. 21 These principles have also been identified during planar 2-joint movements in healthy subjects 21 and hemiparetic patients. 22
In hemiparetic patients, the control of the velocity of a single joint is complicated by spasticity-related inappropriate muscle activity, which can limit range of motion.10,23 Recent studies have demonstrated that spasticity is characterized by a decrease in the stretch reflex (SR) threshold that occurred within the anatomical limits of joint motion.7,24 Thus, the slow stretching of muscles beyond the static reflex threshold triggers a contraction of the muscle, limiting movement. When the muscle is stretched faster, the threshold of activation for the length change is progressively reduced, further limiting range of motion.5,25 It is generally agreed that spasticity contributes to the reduction of maximum reaching velocities, but this has not been clearly demonstrated.26-30 More generally, the relationships between force, active range of motion, and spasticity are still debated6,31 although it has been proposed that they all could result from limitations in the central specification of SR thresholds.7,32
During unconstrained multijoint reaching movements, hemiparetic patients generally use the redundancy of the body, increasing trunk flexion in order to compensate for the impairment of elbow extension.33,34 Trunk flexion increases reachable distance in both healthy subjects and hemiparetic patients. When reaching to distant targets, trunk flexion occurs earlier and is of greater amplitude in hemiparetic patients than in healthy subjects, suggesting that it is triggered at a lower threshold of elbow extension. 35 In addition, the involvement of the trunk increases the velocity of the hand. 36 However, it has been shown that patients are actually able to increase range of motion in the shoulder and elbow and use better coordination to reach a distant target when trunk flexion is blocked by a restraining belt. 37 This suggests that the patients spontaneously use trunk compensation, rather than using their full potential of upper-limb motion, probably to reduce effort.
The aim of the present study was to analyze the impact of increased reaching speed condition on both hand kinematics and arm-trunk coordination in patients with stroke-related hemiplegia. The first aim was to investigate the combined effects of reaching distance and speed condition on the coordination of trunk and paretic upper-limb motion. The working hypothesis was that range of elbow extension motion and/or velocity would be limited by the loss of motor control and/or inappropriate muscle activity and that the patients would thus increase trunk motion in order to achieve a faster reach. The analysis focused on elbow extension (indicative of the quality of arm motion33,38) and trunk movement (indicative of a compensatory strategy 39 ). The second aim was to investigate the ability of the patients to perform faster reaching movements when the trunk was restrained.33-37,40 The working hypothesis was that trunk restraint would reveal the limits of the patients’ capacity to adapt reaching movements to more difficult (increased distance and/or speed) conditions.
The overall aim of this single session study was to test the hypothesis that faster speed would favor the use of unsuitable compensatory motor behavior. This is clinically relevant since recent neurorehabilitation methods based on motor learning principles41-45 may favor the use of faster speed instructions as a general means to increase the intensity of therapy. 16
Methods
Subjects and Clinical Evaluation
The study was approved by the local institutional review board. Fourteen hemiparetic patients were included following signing of the informed consent form. They had all sustained a single unilateral stroke of nontraumatic origin at least 1 year previously (Table 1). All exhibited spasticity of the paretic arm and were included in a program of regular botulinum toxin injections (the recordings were made at least 12 weeks after the last injection, when the activity of the botulinum toxin had ceased). 46 Patients with hemispatial neglect, apraxia, or shoulder pain or other neurological or orthopedic conditions affecting the arm or trunk were excluded. We verified clinically that the patients were able to understand simple instructions. The clinical assessment included the following: the arm section of the Fugl-Meyer Scale (maximum score 66), which is a reliable and valid test for the assessment of arm and hand impairment in stroke patients 47 ; the Action Research Arm Test (ARAT), which scores the capacity to grasp and manipulate different sized objects (maximum score 57) and is reliable, valid, and sensitive to change 48 ; and the Motor Activity Log (MAL), which is a semistructured interview for the assessment of frequency of use and quality of use of the affected limb in daily life. This test is a reliable and valid tool for the measurement of arm and hand activity. 49
Patients’ Characteristics.
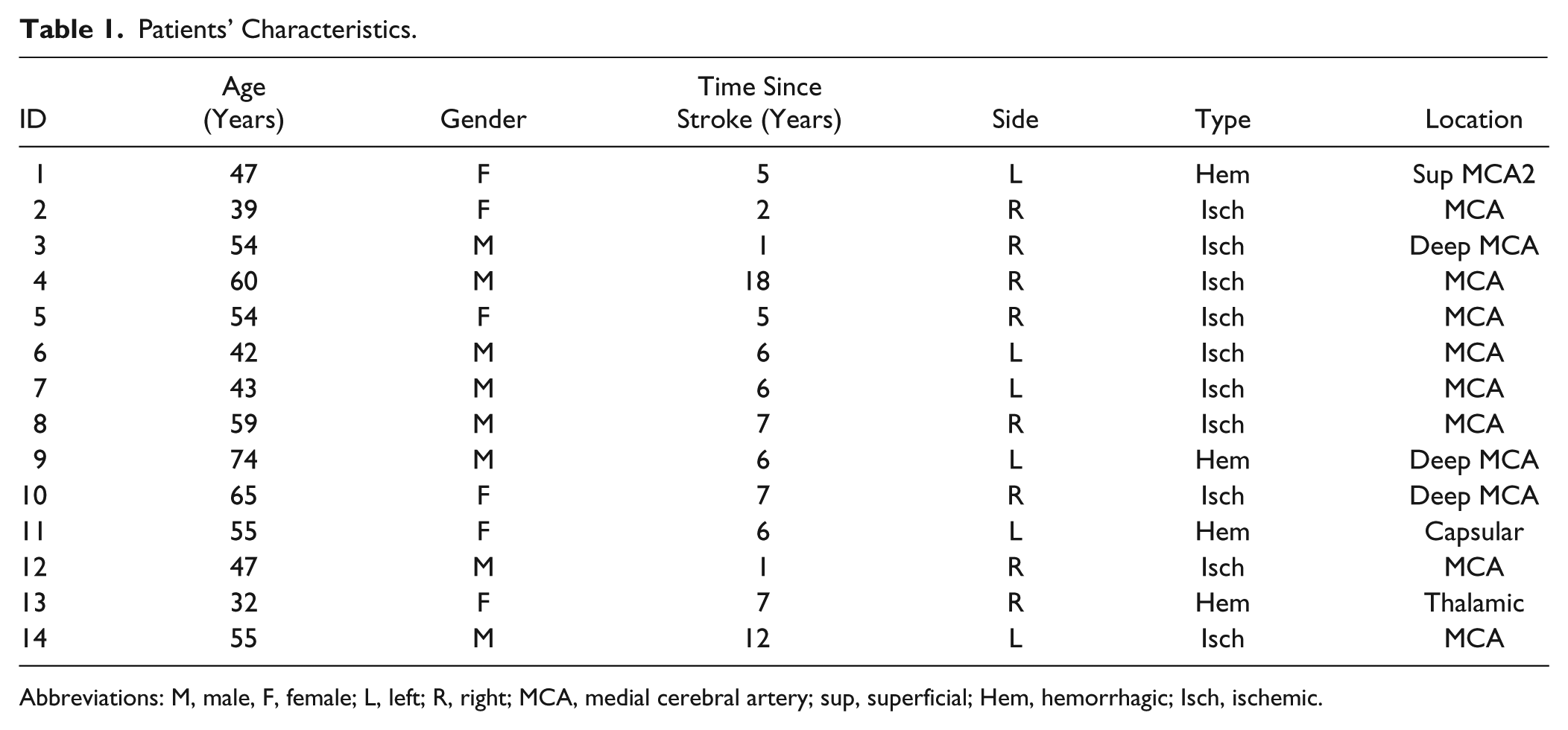
Abbreviations: M, male, F, female; L, left; R, right; MCA, medial cerebral artery; sup, superficial; Hem, hemorrhagic; Isch, ischemic.
Spasticity of the paretic elbow flexors was rated using the modified Ashworth Scale. Passive range of motion of the main paretic upper-limb joints was measured using a manual goniometer and strength of the main upper-limb muscle groups was evaluated using the MRC scale.
Reaching Task
Participants were seated in a chair with their hand placed on the table in line with the shoulder (elbow approximately at 90°). The starting position was marked for each patient. The task was to reach forward with the paretic hand to touch a target (colored spot, 1-cm diameter) placed on a table in the mid-sagittal plane at 60% and 90% of his or her nonparetic arm length (measured from the acromion process to the mid-palmar crease). The instruction was to touch the target with the ulnar border of the hand formed as a fist and then return to the initial position. This task was chosen so that it would be possible even for patients with severe impairment, and was independent of hand and finger function. Two speed conditions were assessed: preferred speed (patients’ spontaneous speed) and fast speed (patients were instructed to reach “as fast as possible”). The order of the tasks was not randomized: the easiest conditions were performed first in order to record the most “spontaneous” behavior and to avoid excessive fatigue. Throughout the text the word “speed” is used to specify the condition and the word “velocity” refers to the measured movement.
The trials were performed initially with the trunk free (trunk-free condition) and were then repeated with the trunk restrained (trunk-restrained condition) by a large strap across the chest.
Five trials were recorded for each of the 8 conditions: target distance (close and far) × speed condition (preferred and fast) × trunk (free and restrained).
Data Recording and Analysis
Movement kinematics were recorded using 8 optoelectronic cameras (Motion Analysis Corporation, sampling frequency 100 Hz) that measured the 3-dimensional coordinates of 5 reflective markers positioned on the proximal interphalangeal joint of the index finger, the radial styloid process of the wrist (RS), the lateral epicondyle of the humerus (LE), the acromion processes (AC), and the upper part of the sternum (ST). 34 The experimenter triggered the recording then asked the patient to perform the movement.
All data were processed using customized algorithms developed using Labview 8.5 (National Instruments). The data analysis focused on 3 types of movement variables: kinematics of the hand in space (measured using the RS marker since the finger marker was not always exploitable), amplitude of elbow joint rotations, functional arm length, and trunk movements.
Position data were filtered (low-pass cutoff, 20 Hz) plotted in 3 dimensions (3D) and the tangential velocity profile of the RS marker was computed. The reach was analyzed from the initial to the final hand position on (or near) the target. The onset and offset times of the reaching movement were automatically determined for each trial (with a threshold of 0.05 m/s) and then visually checked. Peak velocity, reach duration (difference between onset and offset times) and reach distance (3D distance covered by the RS marker) were calculated. A curvature index was computed as the ratio between total end point path length and a straight line joining the initial and final positions. 50 Trajectory smoothness was calculated as the number of velocity peaks: the thresholds (greater than one-tenth of peak velocity and longer than 90 ms) were chosen on an empirical basis after visual monitoring of the trajectories.
Elbow angle was computed using vectors which, respectively, joined the AC and LE markers and the LE and RS markers. The amplitude of extension during the reach and the maximum velocity of elbow rotation were calculated. The 3D displacements of the ST and AC markers were computed to estimate the respective contribution of trunk flexion and associated trunk and scapula rotations. Functional arm length was calculated as the 3D distance between the RS and AC bony landmarks; arm lengthening during reach was also computed.
All movement trials were considered, whether or not the patients reached the target. Statistical analysis was performed on the mean of the 3 to 5 trials recorded in each condition for each participant (some trials had to be excluded due to technical problems, mostly hidden markers). A nonparametric Friedman test was used to test the effect between the conditions (8 different conditions) and then a Wilcoxon test was used for paired comparisons. The significance level of the Wilcoxon test was set at P < .006 following Bonferroni correction for 8 comparisons. A Mann-Whitney test was used to analyze differences between subgroups of patients. Two regression analyses were performed with reach distance (3D displacement of the RS marker) as the independent variable and elbow extension and 3D displacement of the AC marker as dependent variables, respectively.
Tables with further data and supplementary figures will be available in the online data supplement.
Results
The results of the clinical evaluation are presented in Table 2.
Clinical Assessment of the Patients. a
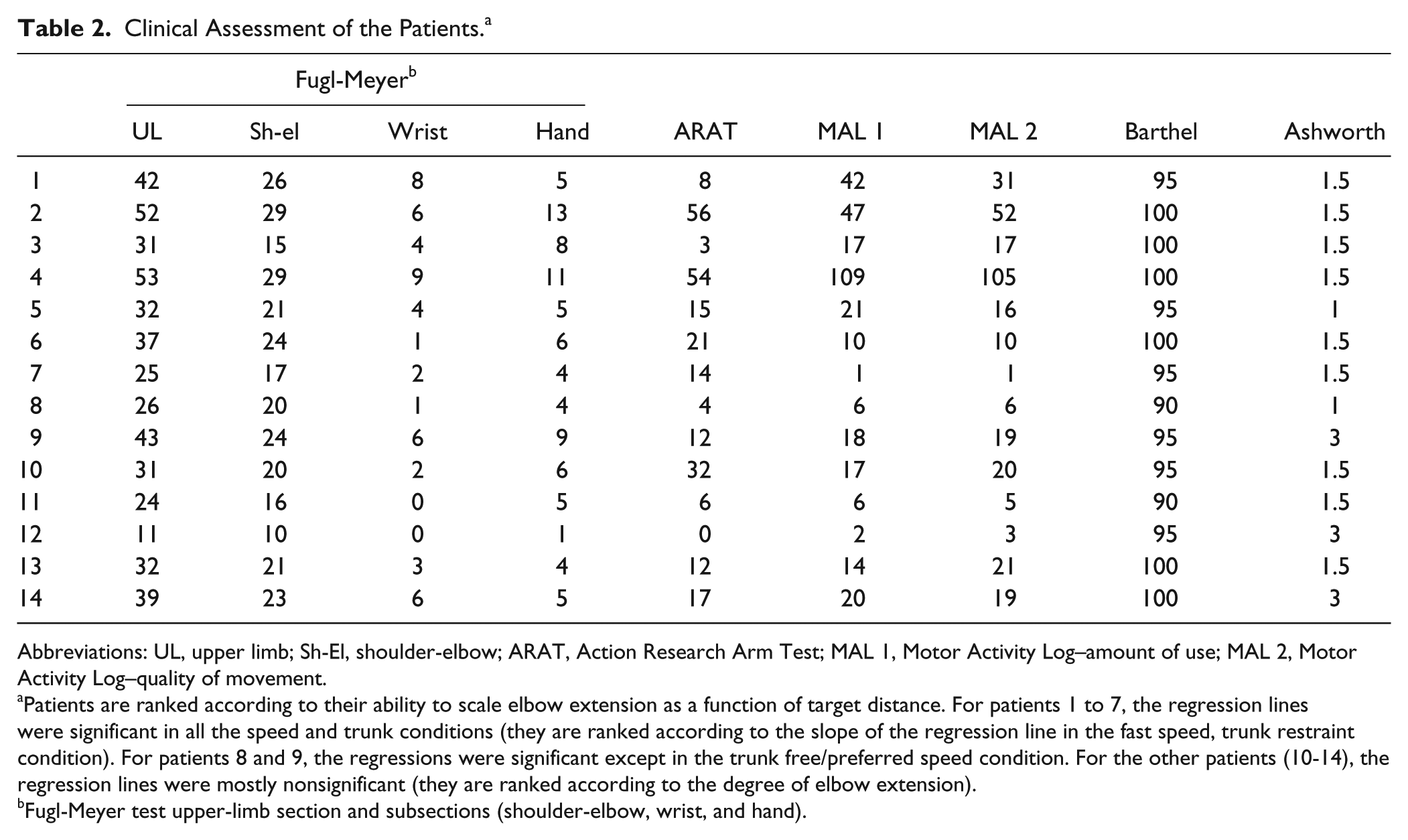
Abbreviations: UL, upper limb; Sh-El, shoulder-elbow; ARAT, Action Research Arm Test; MAL 1, Motor Activity Log–amount of use; MAL 2, Motor Activity Log–quality of movement.
Patients are ranked according to their ability to scale elbow extension as a function of target distance. For patients 1 to 7, the regression lines were significant in all the speed and trunk conditions (they are ranked according to the slope of the regression line in the fast speed, trunk restraint condition). For patients 8 and 9, the regressions were significant except in the trunk free/preferred speed condition. For the other patients (10-14), the regression lines were mostly nonsignificant (they are ranked according to the degree of elbow extension).
Fugl-Meyer test upper-limb section and subsections (shoulder-elbow, wrist, and hand).
Effect of Speed Condition on Hand Kinematics
All the patients were able to perform the reaching movements in the different experimental conditions, although they did not always reach the target.
Variables relating to the end point kinematics are presented in Figure 1. The Friedman test showed that all the variables varied with the conditions, the asterisks in Figure 1 indicate significant paired differences between conditions (Wilcoxon test).
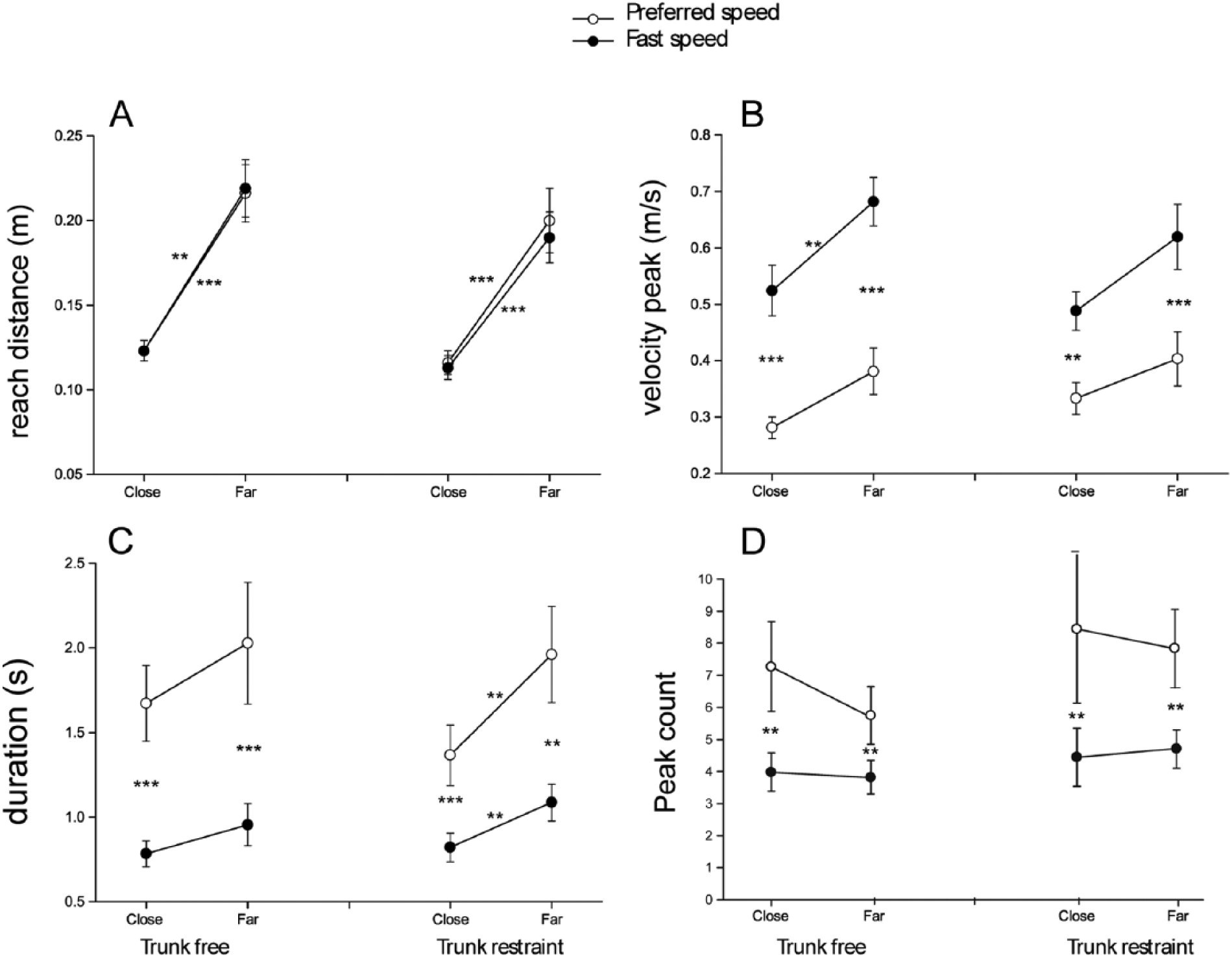
Effect of speed condition on hand kinematics. (A) Reach distance. (B) Maximum peak velocity. (C) Reach duration. (D) Peak count. The effect of target distance (close, far) and trunk condition (free, restrained) are represented on the abscissa of each panel. Open circles indicate the preferred speed condition and black circles the fast speed condition. Each point represents the mean of the 14 subjects. The standard error of the mean is indicated. The asterisks indicate the level of statistical significance with a Wilcoxon paired test, for the effect of target distance, speed condition, and trunk restraint. **P < .006; ***P ≤ .001.
The most spontaneous motor behavior was performed with the trunk free at preferred speed. In this condition, reach distance was 0.216 ± 0.017 m (mean ± standard error of the mean) for the far target and 0.120 ± 0.006 m for the close target (Figure 1A). Peak velocity was 0.40 ± 0.05 m/s for the far target and 0.33 ± 0.03 m/s, for the close target (not significantly different, Figure 1B; see Supplementary Table S1 for individual data). Reach duration was not significantly different between targets (2.03 ± 0.36 and 1.67 s ± 0.22 s for the far and close targets, respectively, Figure 1C). Peak count did not vary with target distance (Figure 1D).
In the fast condition, the peak velocity of the hand increased and duration decreased significantly compared with the preferred speed condition. The reach distance was not significantly different than in the preferred speed condition. There was a significant effect of target in the fast condition: peak velocity was greater for the far (0.68 ± 0.04 m/s) than for the close target (0.52 ± 0.04 m/s). Reach duration was similar for the far (0.95 ± 0.12s) and the close target (0.78 ± 0.76s). Peak count was significantly lower in the fast condition than in the preferred speed condition.
The effect of the trunk restraint is illustrated in the right-hand sections of Figure 1A-D. Reach distance was not significantly modified by the trunk restraint but tended to decrease for the far target-fast speed condition. Peak velocity was not significantly modified by the trunk restraint compared with the trunk free conditions and varied in a similar way with target and instruction. Reach duration increased with target distance, but the mean values were not significantly different than in the trunk free condition. The variations of the peak count were similar in the trunk free and restraint conditions.
The curvature index varied little with the condition, except that in the fast conditions it was greater for the close than the far target (P < .05).
To summarize, endpoint kinematics were modulated by target distance and speed condition but were little affected by trunk restraint.
Effect of Speed Condition on Trunk Contribution to the Reaching Movement
The contribution of the trunk to the reaching movement is shown by the 3D displacement of the ST marker (which relates to trunk flexion) and that of the AC marker (which relates to a combination of trunk and scapula rotations) (Figure 2A and B). In the trunk free–preferred speed condition, the trunk contribution was relatively small for the close target (0.04 ± 0.01 and 0.07 ± 0.01 m for ST and AC, respectively) and increased significantly with target distance (to reach 0.08 ± 0.01 and 0.12 ± 0.02 m for the far target for ST and AC, respectively). In the trunk free–fast speed condition, trunk movement was greater than in the preferred speed condition reaching 0.10 ± 0.02 and 0.16 ± 0.02 m for the far target for ST and AC, respectively. The difference between speed conditions was significant for the far but not the close target.
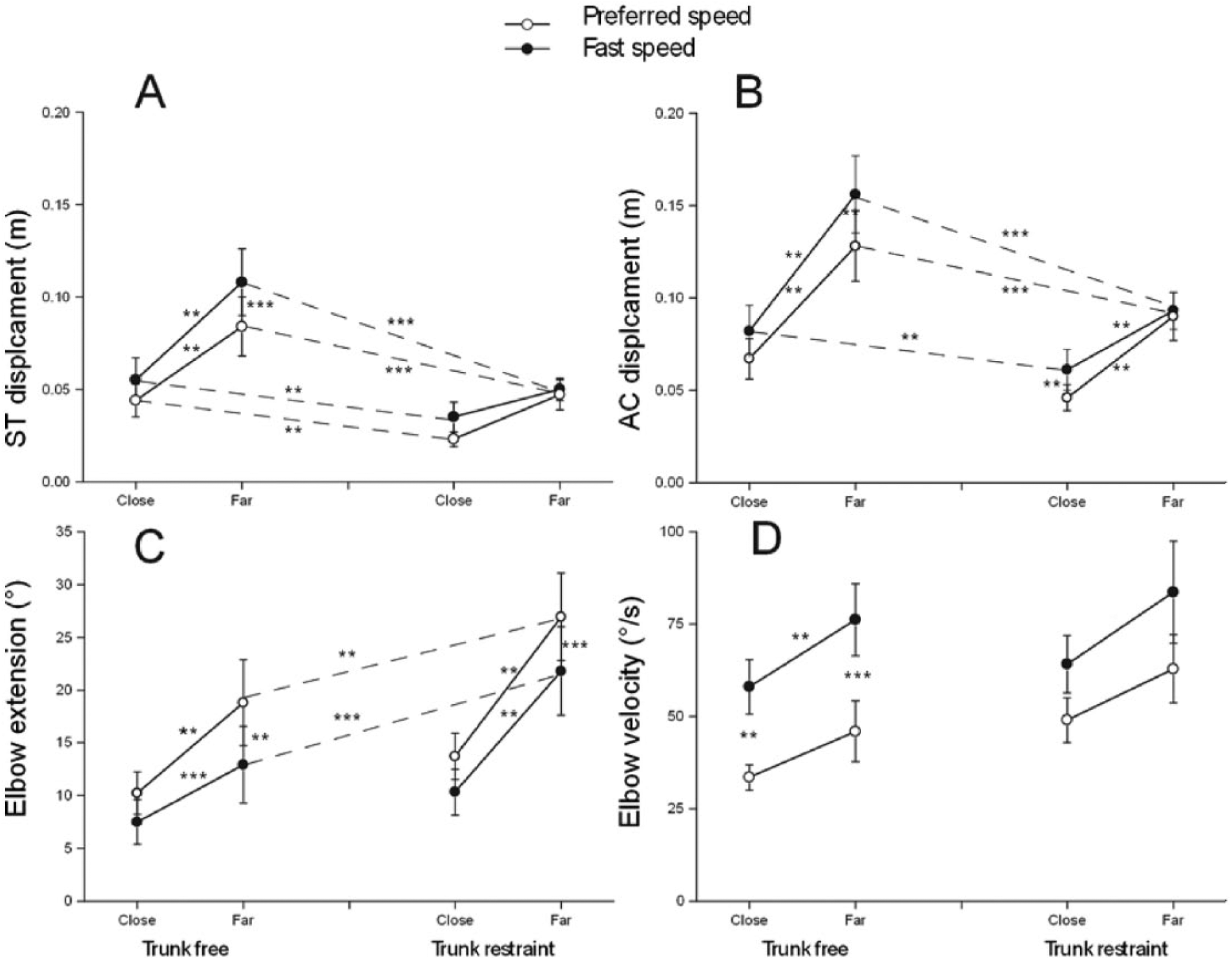
Effect of speed condition on elbow extension and trunk movement. (A) Displacement of the sensor fixed on the sternum. (B) Displacement of the sensor fixed on the acromion. (C) Elbow extension amplitude. (D) Elbow extension velocity. Same legend as in Figure 1.
In the trunk-restrained condition, the strap limited, but did not completely prevent, trunk movement. ST displacement was always less than 0.05 m even for the far target, but AC displacement increased with target distance (0.04 ± 0.01 and 0.09 ± 0.01 m for the close and far targets, respectivlely). In the fast condition, ST displacement did not change, but AC displacement increased for the close but not for the far target. This suggests that the physical limit of the strap allowed a maximum displacement of 0.05 m for ST and 0.09 m for AC, probably because associated trunk and scapula rotations were less blocked than flexion.
Effect of Speed Condition on Elbow Extension
In the trunk-free condition, elbow extension (Figure 2C) increased significantly with target distance (10.2° ± 2.0° and 18.8° ± 4°, respectively, for the close and far targets). Maximal elbow extension was less in the fast compared with the preferred speed condition and was scaled to reach distance (7.5° ± 2.1° and 12.9° ± 3.6°, respectively, for the close and far targets). The difference between the preferred and fast speed conditions was significant for the far but not the close target. Elbow extension velocity (Figure 2D) increased significantly in the fast condition. Extension velocity was scaled to target distance in the fast (58.0° ± 7.3° and 76.2° ± 9.7°, respectively, for the close and far targets) but not in the preferred speed condition (33.5 ± 3 and 45.9 ± 8 deg/s for the close and far targets, respectively).
Trunk restraint increased elbow extension compared with the trunk-free condition (significantly for the far but not the close target). In the trunk-restrained condition, maximal elbow extension was significantly scaled to target distance and was significantly lower in the fast than in the preferred speed condition (close preferred 13.7° ± 2.1°; far preferred 26.9° ± 4.1°; close fast 10.3° ± 2.1°; far fast 21.7° ± 4.1°). Elbow extension velocity was not significantly greater in the trunk-restrained than in the trunk-free condition, and there was no significant difference between the fast and preferred speed conditions.
Individual Analysis of the Scaling of Elbow Extension and AC Displacement to Reach Distance
Regression analysis was used to investigate the relationship between elbow extension (dependent variable) and reach distance (independent variable) for each participant (Figure 3A and B, see Supplementary Table S2). The regression analysis was significant in most cases. In 7 patients, it was significant in all 4 trunk and speed conditions (r2 = 0.612-0.995); in the 7 others it was not always significant (or was significantly toward flexion in one patient), see Supplementary Table S2.
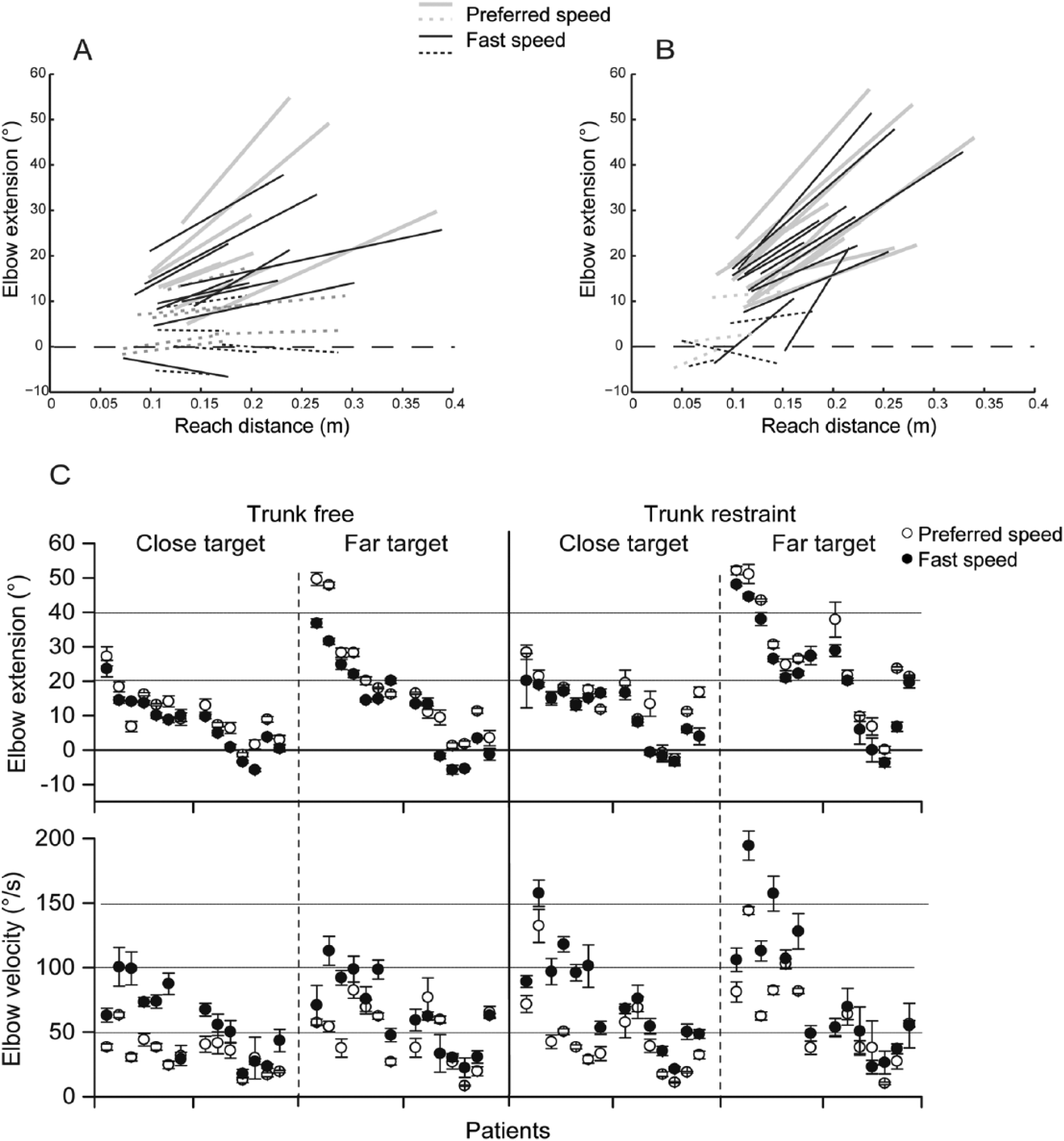
Scaling of elbow extension in individual patients. (A) Effect of reach distance (independent variable) on elbow extension (dependent variable) in the trunk-free condition. Each line indicates the regression of the 6 to 10 samples recorded for one patient in one experimental condition. The extremities of each line relate to the shortest and longest reach distances observed within these trials. Full lines indicate significant regressions and dotted lines indicate nonsignificant regressions. The stippled line represents zero extension. Gray lines indicate the preferred speed condition and black lines the fast speed. (B) Effect of reach distance (independent variable) on elbow extension (dependent variable) in the trunk restrained condition. Same legend as (A). (C) Effect of speed condition (preferred in grey and fast in black) on elbow extension amplitude (upper part) and velocity (lower part) for the close and far targets in the trunk-free and trunk-restrained conditions. The patients are ranked as in Tables 1 and 2 according to their ability to scale elbow extension to movement distance (the regressions of elbow extension to movement distance were significant for the beginning 7 patients, whatever the condition).
The individual values of elbow extension and elbow extension velocity are shown in Figure 3C. The patients are ranked according to their ability to scale elbow extension to movement distance. The first 7 patients who regularly scaled elbow extension to movement distance were able to increase the velocity of elbow extension when the instruction was to go faster. This was not the case for the 7 other patients. Elbow extension velocity was significantly different between these 2 subgroups (Mann-Whitney, P < .0001).
The amount of AC displacement (dependent variable) increased significantly with reach distance (independent variable, see Supplementary Figure S1 and Table S3). In the trunk-free condition, the slope of this relationship varied between 0.28 and 1.08 in the preferred speed condition and between 0.15 and 1.4 in the fast condition (a slope of 1 or more indicates that hand displacement is entirely the result of trunk movement). In the trunk-fixed condition, the amount of AC displacement was also significantly related to reach distance in most patients, despite the strap. The slope of this relationship varied between 0.17 and 0.9 in the preferred speed condition and between 0.24 and 0.97 in the fast condition.
Coordination Between the Trunk and Upper Limb
The reach distance is ensured by the added contribution of the lengthening of the arm (increase in the functional arm length) and AC displacement (see Supplementary Figure S2). The relative contributions of the trunk and upper limb for each individual are illustrated in Figure 4 in the trunk-free condition. The direction of the vectors indicates the difference between preferred and fast speed conditions. Figure 4 shows that fast speed associates an increase in AC displacement corresponding, with a few exceptions, to a decrease of arm lengthening. In 4 cases, the effort required to make faster reaches resulted in a decrease of functional arm length characterized by a negative value of arm lengthening.
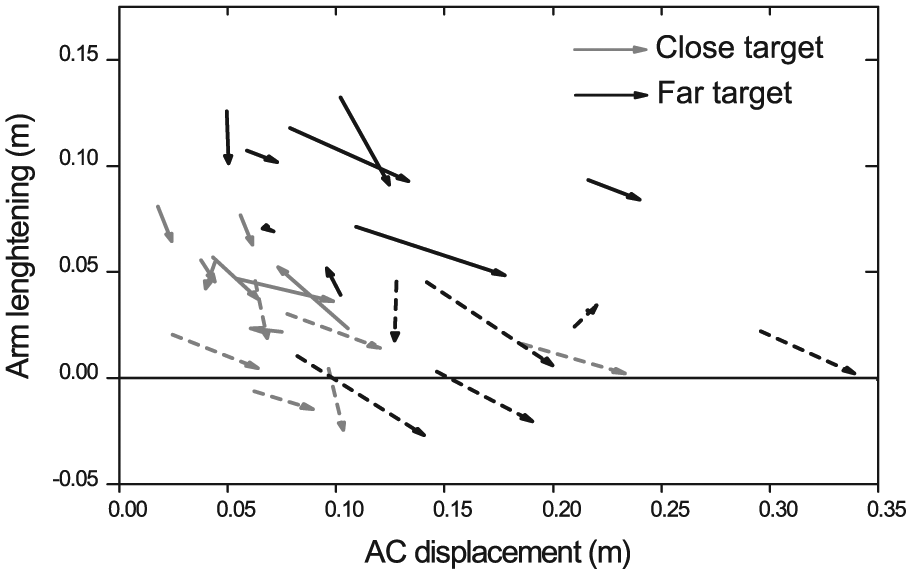
Effect of movement velocity on the contribution of trunk movement and arm lengthening to reach distance in individual patients. Influence of the speed condition on the relative contributions of AC displacement (in abscissa) and arm lengthening (in ordinate) in the trunk-free condition. Each vector represents one subject and points from preferred speed to fast speed values. Close targets are represented in gray and far targets in black. The dotted lines indicate patients who did not scale elbow extension as a function of reach distance.
Comparison With Clinical Data
The individual patients in Tables 1 and 2 are presented in the same order as in Figure 3C. The analysis of individual results and the comparison of clinical and kinematic data did not show clear cut clinical differences between the patients who were able or not to scale elbow extension to movement distance. For example, the Fugl-Meyer scores were 25 to 53 versus 11 to 46, respectively. However, it is noteworthy that the patients with the most severe spasticity (MAS 3) were among the least able to regulate elbow extension to target distance.
Discussion
In healthy subjects, it is well known that hand velocity increases with target distance 51 and with the instruction to move faster. As suggested by Gottlieb et al, 20 these factors correspond to independent organizing principles, respectively, called speed-insensitive and speed-sensitive strategies. 21 The present study confirms that hemiparetic patients are able to voluntarily increase movement velocity.16-19 The effect of target distance was significant in the fast condition but not in the preferred speed condition, in contrast with the results of several previous studies23,36,52 which showed that hand velocity increased with movement distance in hemiparetic patients.
Faster movements were also smoother as shown by a lower number of peaks. 53
The main result of the present study was that faster hand velocity affects arm-trunk coordination, in contrast with what had previously been claimed. 17
Because of the large redundancy of the body and limb segments, 54 hand movement can be generated by an infinity of arm and trunk coordination patterns. The present observations in the preferred speed condition confirmed that hemiparetic stroke patients take advantage of this redundancy and use greater trunk flexion34-36 and rotations 40 to compensate for the impairment of elbow extension. Both trunk movements and elbow extension were scaled to reach distance. 35 The present study also confirmed that when the participation of the trunk was limited by a restraining strap, the patients were able to increase elbow extension amplitude so that the displacement of the hand was not altered. 37
The voluntary increase in movement velocity in the fast speed condition had 2 consequences. On one hand, some patients were able to increase elbow extension velocity and to scale it to movement distance, which is consistent with the observation of single joint planar movements in healthy subjects.20,21,55,56 On the other hand, the faster movement strongly affected arm-trunk coordination. First, the increase in elbow extension velocity was performed at the expense of elbow extension amplitude, which was consistently decreased. Second, trunk movement increased consistently: This was observed both when the trunk was free and also, within the limits of the strap, in the restrained condition. Third, the instruction to go faster altered the relative contribution of the trunk and upper limb to the distance reached: In most patients, the trunk movement became the main (or even the only) source of hand displacement for reaching. The individual analysis showed that the patients who were able to increase elbow extension when the target distance was increased were also able to increase the velocity of elbow extension when the instruction was to go faster. In contrast, the other patients relied mainly on the trunk to adapt to harder task constraints: increased target distance or faster speed. Unfortunately, the role of trunk participation on the reaching movement was not completely demonstrated since the trunk restraint was not tight enough. It is likely that a complete trunk restraint would have reduced movement extent in the far target-fast speed condition.
The alteration of arm-trunk coordination with increased reaching speed contrasts with the constant extension range51,55,56 and arm coordination57-60 generally reported in healthy subjects, although a recent study demonstrated small differences. 61 The reduction in elbow extension amplitude with increased reaching speed may be due to spasticity, defined as a velocity dependent increase in the stretch reflex. 10 The patients recruited in this study had different degrees of spasticity. The analysis of individual data did not evidence clear relationships between the clinical and kinematic data except that 3 of the 7 patients with the most severe limitation of elbow extension also had severe spasticity. The velocity of elbow extension observed in the present study was low, less than 85 deg/s in average, in most patients is was well below the maximum voluntary velocity observed in healthy subjects during horizontal planar movements (500-700 deg/s)62,63 and reaching movements (100-180 deg/s). 64 Experiments involving passive stretching of the wrist and elbow flexors in patients with spasticity demonstrated that less than 100 deg/s velocities could trigger a spastic response.7,32,65 The relative reduction in elbow range of motion at faster speed could be due to the triggering of a spastic reflex resulting from the impaired regulation of the stretch reflex threshold 7 ; however, the weakness caused by the lesions of the corticospinal pathway may also be involved. Muscle hypoextensibility probably also contributes to the reduction in elbow extension. The further reduction of elbow extension with increased movement velocity is more likely to be due to spastic co-contractions, 12 which increase with effort and may induce a reversal of the torque produced at the joint 66 or to the triggering of pathological synergies, an involuntary elbow flexion accompanying the effort of shoulder flexion.13,14 The main limitation of the present study is that it lacks electromyography data that could demonstrate this point.
The alteration of arm-trunk coordination observed in the present study contradicts the previous conclusions that “movement quality improves” with faster task performance.16,17,19 Previous studies were based on different tasks and analyses. During reach to grasp movements, increasing movement speed lead to a straighter movement path and larger finger aperture16,17,19 (however, elbow joint rotation and trunk movements were not measured). Another study involving alternating cyclical movements showed that both elbow extension and trunk movement were reduced at faster speeds. 18 In addition, all previous studies were carried out in patients with a higher level of function (ARAT scores of 20-53) 16 and no or little spasticity. In the present study, the patients were more impaired, had higher levels of spasticity and some were not able to grasp.
Limitations
Further studies are needed to confirm the immediate effect of the faster speed condition. The main limitation of this study is that fatigue or learning effects may have influenced the results since the order of the conditions was not randomized. Another limitation is that because of technical problems, the precision of the reaches was not measured. This important determinant of movement quality2,6,8 was not assessed in the present study. In addition, the lack of electromyography data is a strong limitation for a better understanding of the mechanisms limiting elbow extension velocity (to detect spasticity or to qualify the coordination strategies according to the instruction20,21).
Conclusion and Perspectives
The present results demonstrate that faster movement speed incites patients to use a motor schema involving compensation 39 rather than faster elbow extension. Compensation may help patients to perform tasks in the short term but is associated with long-term problems 67 and can lead to a pattern of learned nonuse, limiting subsequent recovery.68,69 Although it is speculative to infer a possible evolution from a single session study, the present study suggests that training at faster speeds should be used with caution in order to avoid the risk of imposing useless or potentially harmful therapy. The quantitative analysis of reaching coordination presented in the present study could be used to select patients before entering into intensive therapy. Training at faster speeds should be carefully reserved for patients who are able to spontaneously modulate the range and velocity of elbow extension as a function of target distance. It may be contraindicated (or used with caution) in patients who do not spontaneously scale elbow extension but instead use increased trunk compensation. Trunk restraint, which is already recommended for training elbow extension70,71 is particularly recommended if a fast speed training protocol is envisaged. Finally, similar studies are now required on the combined effects of target distance and speed instruction on the trunk and upper-limb reaching coordination during and after a rehabilitation intervention involving fast and/or intense therapy such as robotic interventions.41,44,45
Footnotes
Acknowledgements
The authors are grateful to the patients who participated in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: L. Mandon was supported by SOFMER (Société Française de médecine physique et réadaptation).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.