
Abstract
Background. Parkinson’s disease (PD) is associated with stooped postural alignment, increased postural sway, and reduced mobility. The Alexander Technique (AT) is a mindfulness-based approach to improving posture and mobility by reducing muscular interference while maintaining upward intentions. Evidence suggests that AT can reduce disability associated with PD, but a mechanism for this effect has not yet been established. Objective. We investigated whether AT-based instructions reduce axial rigidity and increase upright postural alignment, and whether these instructions have different effects on postural alignment, axial rigidity, postural sway, and mobility than effort-based instructions regarding posture. Method. Twenty subjects with PD practiced 2 sets of instructions and then attempted to implement both approaches (as well as a relaxed control condition) during quiet standing and step initiation. The “Lighten Up” instructions relied on AT principles of reducing excess tension while encouraging length. The “Pull Up” instructions relied on popular concepts of effortful posture correction. We measured kinematics, resistance to axial rotation, and ground reaction forces. Results. Both sets of experimental instructions led to increases in upright postural alignment relative to the control condition. Only the Lighten Up instructions led to reduced postural sway, reduced axial postural tone, greater modifiability of tone, and a smoother center of pressure trajectory during step initiation, possibly indicating greater movement efficiency. Conclusion. Mindful movement approaches such as AT may benefit balance and mobility in subjects with PD by acutely facilitating increased upright postural alignment while decreasing rigidity.
Keywords
Introduction
Parkinson’s disease (PD) is a progressive neurological disease that includes a range of symptoms related to control of posture. These symptoms include increased postural sway during quiet stance 1 and a tendency to stand with a forward-stooped postural attitude, 2 which may negatively affect postural stability. 3 PD symptoms also include high and unadaptable axial tone (rigidity), which has been associated with difficulty turning, 4 and reduced ability to shift weight in preparation for step initiation. 5 These problems are likely to contribute to falls 6 and decreased quality of life for people with PD.
Although medication often alleviates Parkinsonian motor symptoms, it does not eliminate them, and it may even make some aspects of postural control worse.1,7,8 Therefore, additional complementary approaches are needed. Approaches based on mindful movement, also called “movement based embodied cognitive practices,” 9 have shown promise in this regard. Mindful movement approaches have in common attention not only to the outcome of the movement, but also to the quality of the movement itself. Some data suggest that mindful movement approaches such as tai chi,10-13 ballroom dance, 14 and Alexander Technique (AT)15,16 may be helpful for improving mobility and overall well-being in people with PD, but the evidence is equivocal 17 and the mechanisms by which the improvement might occur are unknown. Practitioners of mindful movement maintain specific intentions regarding the quality of movement and/or posture, and these intentions differ across approaches. Thus, one important question is whether different qualitative intentions regarding posture and movement have different effects on posture and movement in PD.
One possible way that mindful movement may improve Parkinsonian motor symptoms is by increasing core stability. Some evidence suggests that increasing strength in the muscles of the trunk may improve stability. 18 It is possible that simply bringing focused attention to stabilizing the trunk may provide similar benefits. However, other research sheds doubt on the value of trunk stabilization methods. 19 Furthermore, intentionally engaging trunk muscles may have a particularly detrimental effect on people with PD, who already tend to have excessive activity in their trunk musculature. 20 It is possible that overactivation of trunk muscles associated with axial postural tone decreases their responsiveness, which could decrease postural stability.
Another possible way that mindful movement may improve motor symptoms is by reducing excessive axial tone. High axial tone, as measured by resistance to axial rotation in the hips, trunk, and neck, is associated with deficits in functional mobility in subjects with PD. 4 Axial tone may be amenable to modification: evidence indicates that a course of lessons in AT reduces excessive axial tone in adults with back pain, and that long-term practice reduces it even further while also making it more adaptable. 21
The AT is unique among mindful movement approaches in that it is not defined by a particular set of postures (as in yoga) or movements (as in tai chi or tango), but rather by postural instructions that are maintained during everyday movement such as standing, sitting, walking, and talking. 22 According to its proponents, students of AT learn to prevent unconscious postural habits, especially excessive muscular activity in the neck and trunk, that interfere with easy carriage and movement.23-25 (Cacciatore et al have written an excellent description of AT pedagogy. 26 ) The approach has been shown to be helpful for alleviating chronic back pain, 27 increasing functional reach, 28 and reducing postural sway 29 in older adults, increasing breathing capacity, 30 and decreasing disability associated with PD.15,16 The prevalence of unconscious postural habits and excessive rigidity in PD provides a logical justification for why AT might be particularly helpful for this population.
The goal of this study was to determine the effects of different instructions on axial rigidity, postural sway, postural alignment, and step initiation in patients with PD. Following the approach of Jones, 25 2 opposing sets of instructions were tested as experimental conditions. Both approaches drew attention to posture and used intention to influence background muscle activity in the trunk and neck (axial tone), but in opposite ways. The “Pull Up” instructions were based on the idea of increasing effortful trunk stabilization, and the “Lighten Up” instructions were based on reducing excessive muscular activity while maintaining an upward intention. A “Relax” condition was used as a control. By testing all subjects in all conditions, we aimed to distinguish between changes in posture and movement due simply to increased attention to the body and increased uprightness (factors that both experimental conditions should have in common) from changes due to specific ways of thinking about posture.
We hypothesized that both sets of experimental instructions would increase uprightness of posture and efficiency of step initiation relative to the Relax condition. In contrast, we hypothesized that the intention to decrease excessive activity in axial musculature (Lighten Up) would decrease postural rigidity and sway, whereas effortfully increasing activation of axial muscles to stabilize the trunk (Pull Up) would increase postural rigidity and sway. More detail about these hypotheses is included below under the Tasks and Measures subsection.
Method
Participants
Twenty participants with Parkinson’s disease (PD) were referred by the Parkinson’s Center of Oregon at Oregon Health & Science University (OHSU). All participants were screened for the following exclusion factors: previous deep brain stimulation surgery, neuropathy, and inability to stand independently for 20 minutes. Participants were tested in the “ON” state to maximize external validity. All comparisons were within-group. See Table 1 for demographic characteristics of participants.
Demographic Attributes of Participants.
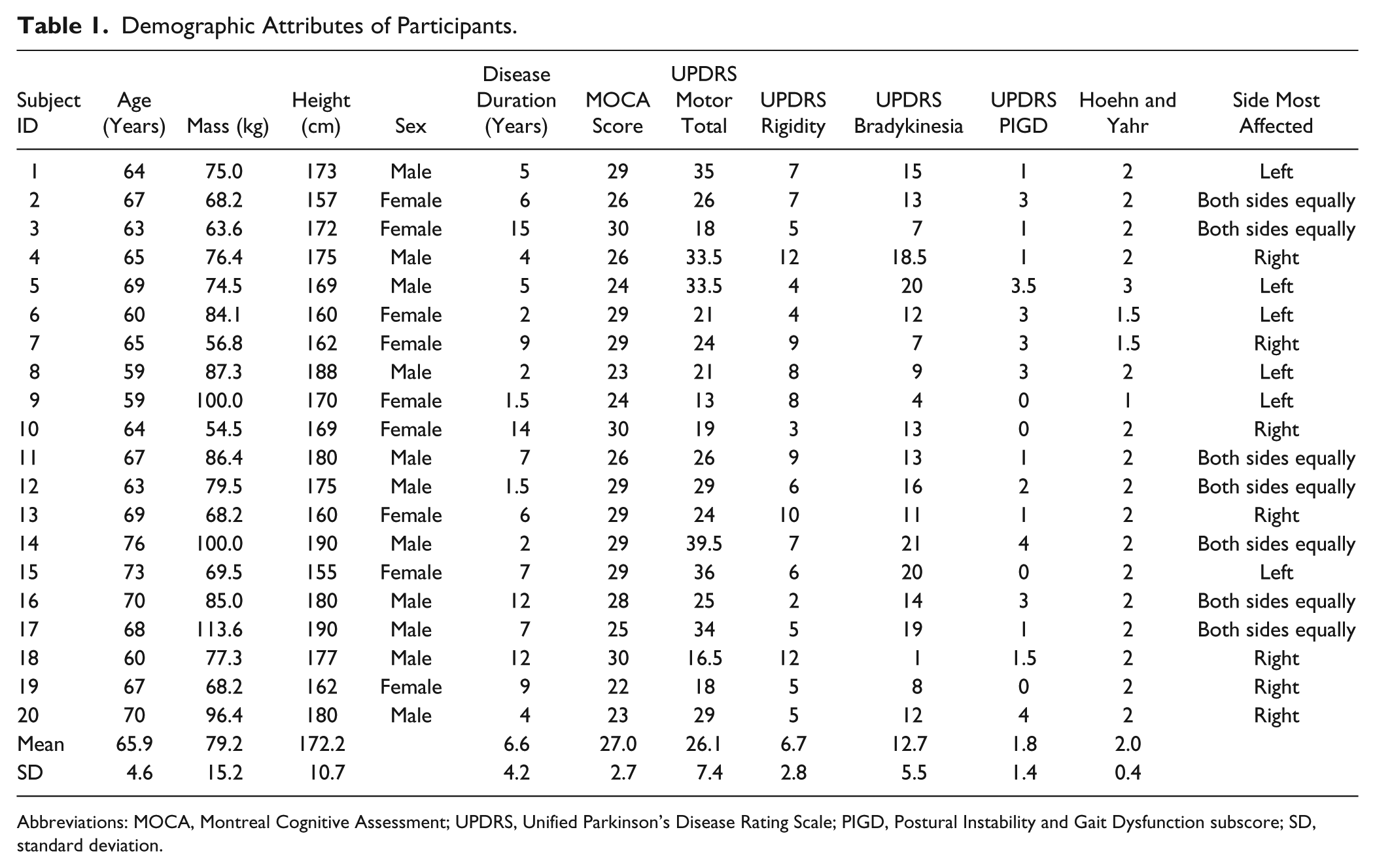
Abbreviations: MOCA, Montreal Cognitive Assessment; UPDRS, Unified Parkinson’s Disease Rating Scale; PIGD, Postural Instability and Gait Dysfunction subscore; SD, standard deviation.
Procedure
After participants signed consent forms approved by OHSU’s Internal Review Board, experimenters administered the Montreal Cognitive Assessment (MOCA), 31 United Parkinson’s Disease Rating Scale (UPDRS), 32 and a preliminary assessment of expectations about the effects of the instructions. Experimenters then provided more detailed instruction regarding the different conditions, which participants would be asked to implement during the measurements.
Participants were given instructions and a few minutes of practice in 3 postural conditions: AT-based (Lighten Up), effort-based (Pull Up), and a control condition (Relax), followed by the completion of 3 tasks for each postural condition. Tasks and collected measurements were as follows: (1) axial tone—5 minutes of axial rotation with measurement of resistance between shoulders and pelvis; (2) quiet stance—30 seconds of quiet stance with inertial sensors located on the wrists, ankles, lumbar, and sternum to measure 3-dimensional acceleration and rotation; and (3) step initiation—3 self-initiated steps off of a force platform, with reflective markers on bony landmarks of the body, including the head, shoulders, and pelvis.
Pull Up and Lighten Up conditions were counterbalanced such that odd-numbered subjects completed the conditions in the following order: [Relax, Lighten Up, Relax, Pull Up]; and even-numbered participants completed the conditions as: [Relax, Pull Up, Relax, Lighten Up]. During analysis, the initial Relax conditions were excluded. For each task, participants completed 3 successive trials for each condition, with a total of 12 trials for each task before moving on to the next task. The experimenter gave a single-sentence reminder of the instructions before each trial. A research assistant stood near the participants to catch any incipient falls. After all trials were completed, participants filled out a debriefing questionnaire.
Expectations
Participants were asked to anticipate the effects of the different ways of thinking about posture before beginning. The experimenter presented written descriptions of both experimental conditions and asked participants to check boxes indicating how helpful each one would be to their symptoms while standing quietly or stepping. The order of presentation of the descriptions was counterbalanced across participants. The Lighten Up condition was described as follows:
Whatever our condition, we make matters worse by pulling ourselves down, and especially by tightening the neck and pulling the head down. For the next few minutes I would like you to focus on allowing an upward direction.
The Pull Up condition was described as follows:
Parkinson’s makes you weaker, so it is important to activate your core muscles to pull yourself up to your full height. For the next few minutes I would like you to focus on feeling your neck and trunk muscles work strongly to pull you up.
The 5-point rating scale was as follows: [Would make things worse; Would have no effect; Would help a little bit; Would help somewhat; Would help a lot].
Posture Instructions
Before the measurements, subjects were given time to practice changing between the baseline condition (Relax) and the 2 test conditions (Pull Up and Lighten Up). Instructions for the Relax (control) condition were
Imagine that it is the end of a long day and you feel tired and lazy; allow your head to feel heavy and sink slightly forward and down; relax your shoulders and allow them to hang heavily.
Instructions for the Pull Up condition were
Use your core muscles to pull yourself up to your fullest height; engage the muscles in your abdomen and lower back; feel your neck and trunk muscles working to pull you up; pull your stomach in, your head and chest up, and your shoulders back.
Instructions for the Lighten Up condition were
Notice that you are pulling yourself down and give yourself permission to stop doing it; let your head balance easily at the top of your spine; allow your spine to be uncompressed and your torso to open effortlessly; let your shoulders and chest be open and light.
Subjects practiced until they stated that they could clearly distinguish between the 3 conditions.
Tasks and Measures
Axial tone
Axial tone (called “trunk stiffness” in some previous studies) was measured during active standing without external support, using a device built specifically for this purpose.4,21,33,34 Subjects stood on a horizontally rotating platform with their feet in a comfortable position, wearing a shoulder harness and a hip belt. The hip belt was attached to the platform, and the shoulder harness was attached to the unmoving, upper part of the device that allows frictionless sway but no rotation. Participants were instructed to stand quietly with their eyes closed and allow the machine to move them. The platform rotated back and forth at 1 deg/s with a maximum deviation of 10° from center in each direction, pausing for 3 seconds before reversing direction. Each trial proceeded as follows: [left, center, right, center]. In each condition, subjects completed three consecutive trials without stopping or opening their eyes. Between conditions, subjects opened their eyes and were encouraged to move as desired for about 2 minutes while remaining in the harness and hip belt. After breaks, subjects returned their feet to their original positions. Strain gauges measured continuous resistance to rotation, and the peak resistance in each cycle was used as the primary outcome measure.
Previous work showed that axial tone adapts in anticipation of external body rotation in healthy subjects but not in PD. 20 Therefore, we measured the phase lead between the axial resistance and the platform rotation, with a higher phase lead indicating greater adaptability.
Equipment malfunction prevented us from collecting postural tone data from 3 subjects, and 1 subject was not able to complete this task because he got dizzy standing with his eyes closed, leaving an N of 16 for these measures.
Postural sway
Subjects wore an APDM Opal inertial sensor around their waists as they stood quietly, with arms crossed over their chests, for 30 seconds. Amplitude (root mean square acceleration) and frequency of sway (Hz) in the mediolateral (ML) and anteroposterior (AP) dimensions were the primary outcomes. 35 Reliable data were obtained for 19 subjects.
Postural uprightness
Subjects stood for about 5 seconds ready to initiate walking. Outcome measures were the vertical and horizontal distances between the markers just in front of the ears and the markers on the acromia of the scapulae while standing and during step initiation. Reliable data were obtained from 17 subjects.
Step initiation
Subjects stood on 2 force plates (sampled at 480 Hz) with their weight evenly balanced and with a comfortable stance width. Foot position was standardized across conditions. Subjects were instructed to initiate stepping with their most affected leg, to begin whenever they were ready, and to stop after 3 steps. Outcome measures were the peak excursion of the center of pressure (CoP) in AP and ML axes during the initial weight shift and the smoothness of the CoP trajectory from the start of the trial to the moment when the first foot came off the force plate. Previous work indicates that subjects with PD are less able to move the CoP backward during step initiation (due to an inability to adequately activate tibialis, 5 deactivate soleus, 36 or both), and that they may compensate by increasing the lateral shift of CoP. 37 Movement smoothness is a commonly used indicator of improved control and is quantified by jerk, the integral of the squared 3rd time derivative of the AP and ML CoP traces. 38 Therefore, improved postural-motor control would be indicated by an increase in backward CoP displacement relative to lateral CoP displacement and by a smoother (less jerky) CoP trajectory. Reliable data were obtained for 16 subjects.
Subjective assessment
Afterwards, subjects answered written questions about the amount of mental and physical effort each set of instructions required, how each set of instructions affected their feeling of stability, and the familiarity of the instructions, using an 11-point scale.
Statistics
Because medians are more robust to outliers than means, and we only had 3 trials in each condition, we selected median values from each condition for analysis. For each outcome measure, we ran a 1-way analysis of variance and followed significant results with paired t tests. In order to reduce the likelihood of type I errors, we used the Holm-Bonferroni sequentially rejective test 39 (rather than the more common Bonferroni tests, which increase the chances of type II errors) 40 to compare the effects of the different instructions. To implement this, we rank-ordered the P values for the t tests on all 3 comparisons (Lighten Up vs Relax, Relax vs Pull Up, and Lighten Up vs Pull Up). The smallest P value was compared against α/k (where k = the number of tests), the middle P value was compared against α/k − 1, and the largest P value was compared against α/k − 2. Therefore, the significance thresholds for the smallest, middle, and largest P values (based on a standard α of .05) were .05/3 = .0167, .05/2 = .025, and .05/1 = .05, respectively.
For our subjective measures, which compared only the 2 experimental conditions, we used the same method, grouping the 2 questions asked in the expectations survey separately from the four questions asked in the subjective assessment.
Results
Expectations
Subjects expected that both sets of experimental instructions would bring about slight to moderate improvement in symptoms relative to the relaxed condition (P < .00001), with no difference between the experimental instructions for either quiet standing (P = .42) or stepping (P = .24).
Axial Tone
Axial tone was affected by instructions, F(2, 30) = 3.7, P = .036 (Figure 1A). Resistance was significantly lower with Lighten Up instructions than Relax instructions, t(15) = 3.4, P = .004, and marginally lower under Lighten Up instructions than Pull Up instructions, t(15) = 2.1, P = .048.
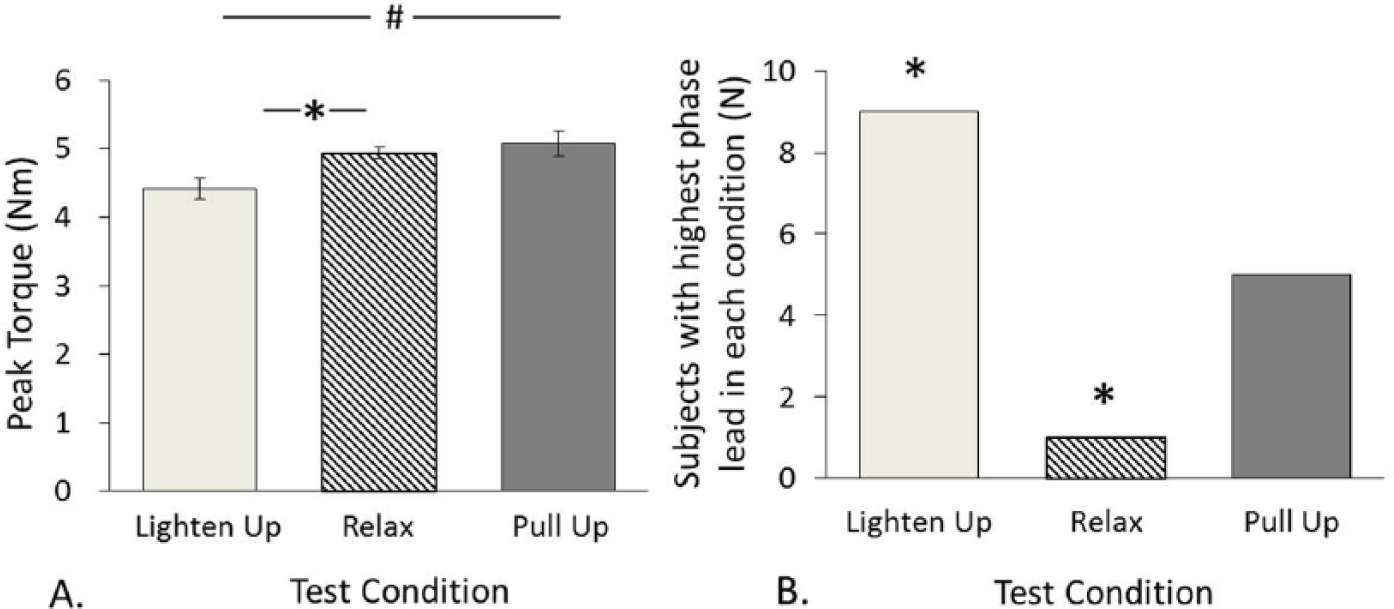
(A) Peak torque (N m) in the 3 conditions. Error bars indicate ±1 standard error after grand mean differences among subjects were removed. * Indicates significant difference after correcting for multiple comparisons. # Indicates significant differences before correcting for multiple comparisons. (B) Number of subjects with highest phase lead in each condition. * Indicates significant difference from expected proportion.
Phase leads were not normally distributed, so t tests were not appropriate. Phase lead was highest for most subjects in the Lighten Up condition and for fewest subjects in the Relax Condition (Figure 1B). According to a χ2 test, this was a significant deviation from expected proportions, χ2(2) = 6.11, P = .047.
Postural Sway
Amplitude
Instructions affected amplitude in both AP and ML axes, F(2, 36) = 5.6, P = .007 and F(2, 36) = 5.0, P = .011, respectively. AP sway amplitude in the Lighten Up condition was significantly lower than both the Relax, t(18) = 2.8, P = .013, and Pull Up, t(18) = 2.7, P = .015, conditions (Figure 2A). ML sway amplitude in the Lighten Up condition was lower than both the Relax, t(18) = 2.6, P = .017, and Pull Up, t(18) = 2.7, P = .015, conditions (Figure 2B).
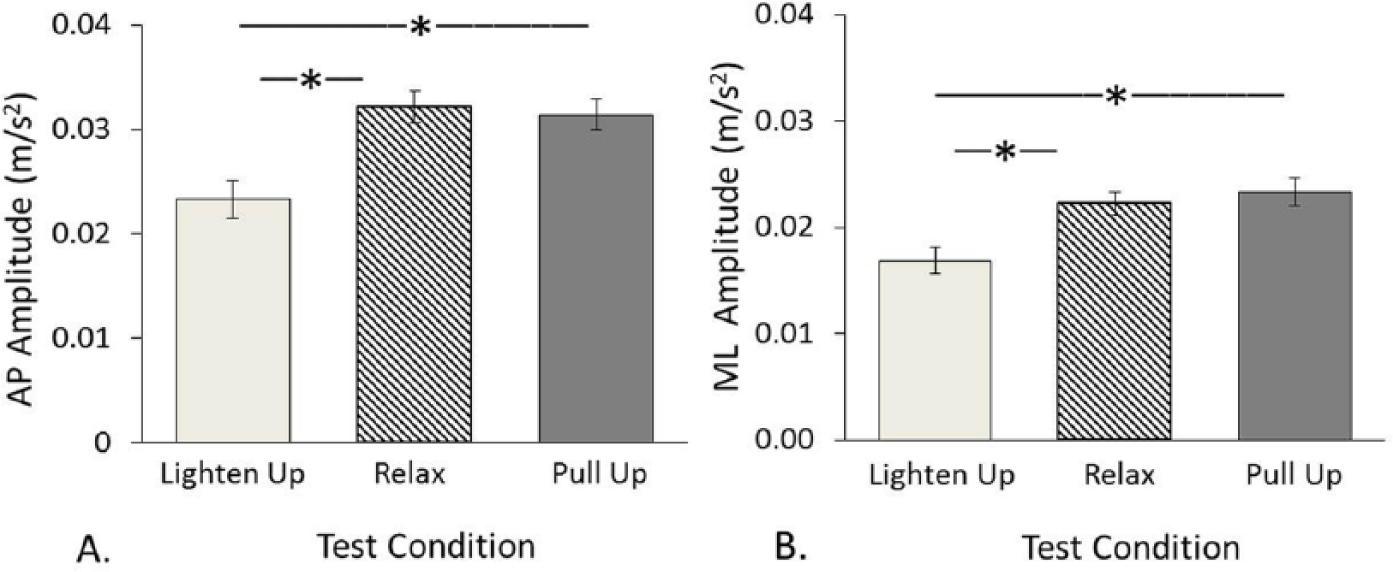
Postural sway in the 3 conditions. Error bars indicate ±1 standard error after grand mean differences among subjects were removed. * Indicates significant difference after correcting for multiple comparisons. (A) Anteroposterior amplitude (m/s2). (B) Mediolateral amplitude (m/s2).
Frequency was not affected by instructions. Mean frequencies for the Lighten Up, Relax, and Pull Up conditions, respectively, were 1.03, 1.02, and 1.01 Hz in the AP axis (P = .69) and 1.23, 1.28, and 1.21 Hz in the ML axis (P = .20).
Postural Uprightness
Standing vertical distance was affected by instructions, F(2, 32) = 4.4, P = .021. The vertical distance between the head and shoulders was marginally greater in the Lighten Up condition than in the Relax condition, t(16) = 2.7, P = .017 (Figure 3A and B).
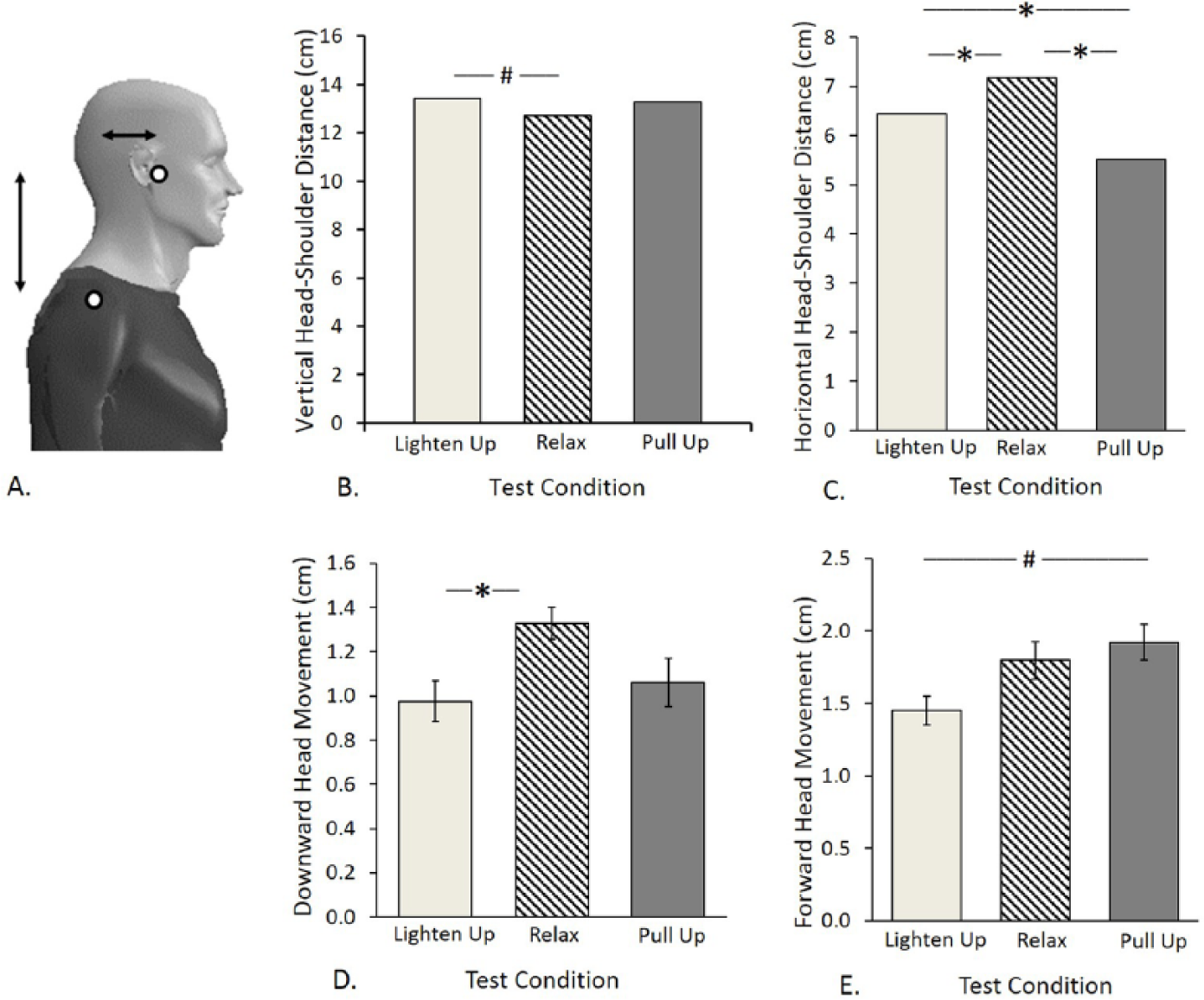
(A) Placement of reflective markers on head and shoulders, from which vertical and horizontal distances were computed. (B-D) Postural alignment in the 3 conditions. Error bars indicate ±1 standard error after grand mean differences among subjects were removed. Error bars are not shown in (B) and (C) because they were too small to see. * Indicates significant difference after correcting for multiple comparisons. # Indicates significant difference before correcting for multiple comparisons. (B) Anteroposterior amplitude (m/s2). (C) Mediolateral amplitude (m/s2). (D) Anteroposterior velocity (m/s). (E) Mediolateral velocity (m/s).
Standing horizontal distance was affected by instructions, F(2, 32) = 13.2, P < .0001. The head was farther forward in the Relax condition than in both the Lighten Up condition, t(16) = 2.5, P = .024, and the Pull Up condition, t(16) = 4.5, P = .0004. The head was farther back in the Pull Up condition than in the Lighten Up condition, t(16) = 3.1, P = .007 (Figure 3A and C).
Downward head movement was affected by instructions, F(2,32) = 7.1, P = .003. During step initiation, the head moved farther down relative to the shoulders in the Relax condition than in the Lighten Up condition, t(16) = 2.9, P = .011 (Figure 3D).
Forward head movement was affected by instructions, F(2, 32) = 9.6, P = .0005. During step initiation, the head moved marginally farther forward relative to the shoulders in the Pull Up condition than in the Lighten Up condition, t(16) = 2.6, P = .019 (Figure 3E).
Step Initiation
Anteroposterior CoP displacement during the initial phase of weight shift was not affected by instructions, F(2, 32) = 1.7, P = .20 (Figure 4A). Mediolateral CoP displacement was affected by instructions, F(2, 32) = 5.4, P = .01 (Figure 4B). Lighten Up instructions produced less lateral CoP displacement than either Relax, t(15) = 4.7, P = .0003, or Pull Up, t(15) = 2.5, P = .025, instructions. The effect of instructions on the ratio between AP and ML CoP displacement approached significance, F(2, 32) = 2.8, P = .07 (Figure 4C).
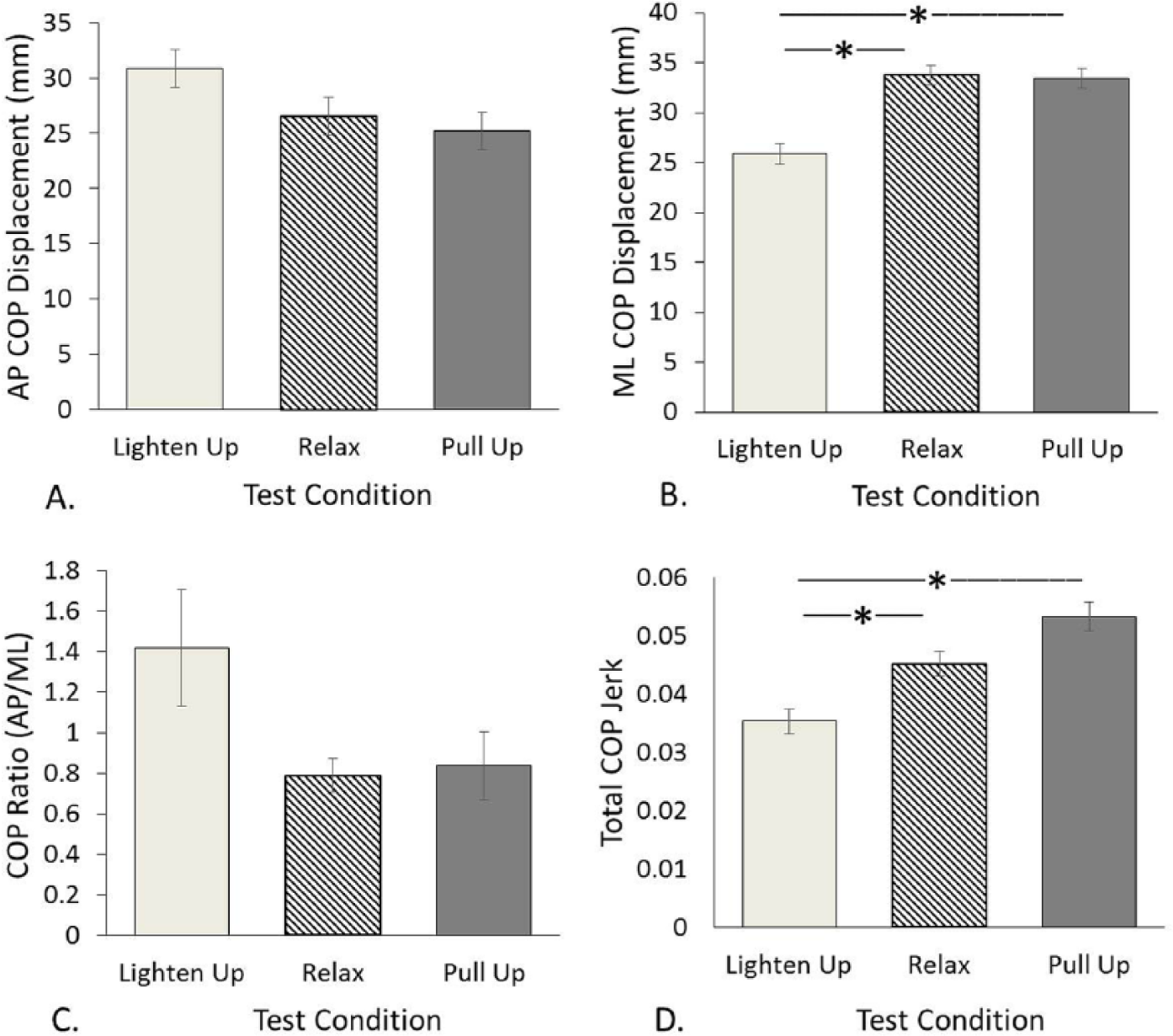
Step initiation. (A) Peak backward displacement of center of pressure (CoP) during initial weight shift. (B) Peak lateral displacement of CoP during initial weight shift. (C) Ratio of A to B. (D) Total jerk of CoP trace during step initiation (see method section for detail). Error bars indicate ±1 standard error after grand mean differences among subjects were removed. * Indicates significant difference after correcting for multiple comparisons.
Smoothness was affected by instructions, F(2, 30)=7.0, P = .003. The CoP trajectory was smoother in the Lighten Up condition than in either the Relax, t(15) = 3.4, P = .004, or the Pull Up, t(15) = 3.0, P = .01, conditions (Figure 4D).
Subjective Assessment
During the postexperiment debriefing, subjects reported that the Lighten Up instructions were significantly less familiar than the Pull Up instructions, t(19) = 2.8, P = .001, and required marginally less physical effort, t(19) = 2.2, P = .04. There was no difference in how subjects perceived the effects of the 2 sets of instructions on their stability or in how much mental effort they required (Figure 5).
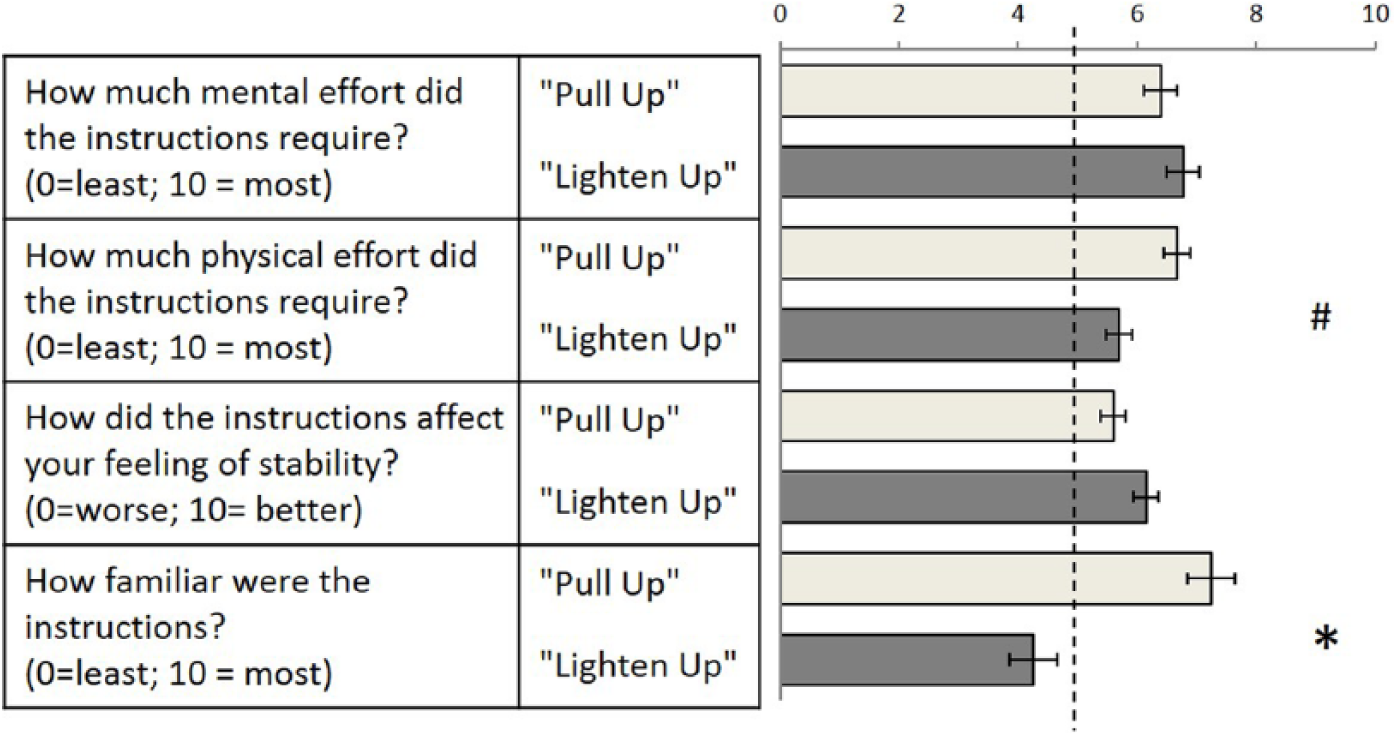
Subjective reports. Error bars indicate ±1 standard error after grand mean differences among subjects were removed. * Indicates significant difference after correcting for multiple comparisons. # Indicates significant difference before correcting for multiple comparisons.
Discussion
Summary of Findings
This study investigated the effects of 2 sets of instructions on posture and mobility: Lighten Up, based on AT principles of reducing excess tension while encouraging length, and Pull Up, based on popular concepts of effortful posture correction. We hypothesized that both sets of experimental instructions would increase postural uprightness and step efficiency relative to the Relax condition, that Lighten Up instructions would decrease postural rigidity and sway, and that Pull Up instructions would increase postural rigidity and sway. We found that during upright standing, only Lighten Up instructions increased head height, while both sets of experimental instructions (especially Pull Up) decreased forward head carriage. During step initiation, Lighten Up instructions reduced lateral CoP displacement and increased smoothness of CoP path relative to both other conditions. Both axial rigidity (peak torque) and postural sway amplitude (AP and ML) were lower with Lighten Up instructions than in either other condition. Tone was most adaptable with Lighten Up instructions and least adaptable in the Relax condition.
Interpretation
Distinct effects of the Lighten Up versus Pull Up instructions were apparent in several measures. First, axial rigidity was lower under Lighten Up instructions than in both other conditions. Lower axial rigidity is consistent with improved postural control and mobility, as previous work has shown that high axial rigidity is associated with turning difficulty in PD. 4 The difference in axial tone observed was relatively modest (0.7 N m, around 14%). However, an earlier study using the same measurement device found a difference of 0.84 N m (16%) between control subjects and PD subjects OFF medication and a difference of 0.47 N m (10%) between control subjects and PD subjects ON medication. 20 Therefore, a difference of 14% is likely to be clinically significant. This result supports the idea that excessive and inflexible muscular contraction in PD may contribute to stooped posture, reduced postural stability, and mobility limitations. 41 It also suggests that the beneficial effects of a series of AT lessons previously reported for subjects with PD 15 may be due, in part, to the axial muscles becoming more adaptable and less rigid.
Second, sway amplitudes were smaller under Lighten Up instructions than under Pull Up instructions. Given the abundant evidence associating large sway amplitude with postural instability in PD, 6 this result suggests that Lighten Up instructions may be of greater benefit for postural stability in PD than Pull Up instructions, perhaps because of the reduction in stiffness they encourage. Lower stiffness may allow subjects with PD to more quickly deactivate previously activated muscles, improving postural control.
We also observed a smaller horizontal distance between the head and shoulders under Pull Up instructions than under Lighten Up instructions, without a corresponding difference in vertical distance. Stooped posture in PD brings the head forward and down and is associated with postural instability, 3 so to some extent, bringing the head up and back relative to the “Relax” condition is probably advantageous. However, if the head comes back more than it goes up, this could indicates a further compression of the spine (as the total distance between head and shoulders decreases), rather than an improvement. In support of this interpretation, Jones25,42 found that when healthy people practiced what they considered to be their “best” posture, they pulled their heads back, and this led to twice as much electromyographic activity in their sternomastoid muscles compared with an AT-based posture.
Step initiation was also different between the 2 experimental conditions. The ML CoP displacement during the initial weight shift before step initiation was smaller under Lighten Up instructions than under Pull Up instructions. Parkinson’s disease has been associated with both smaller 43 and larger 37 lateral CoP shifts, making this result difficult to conclusively interpret. However, considered along with the reduced stiffness and the (nonsignificant) tendency for both AP CoP displacement and the ratio of AP to ML CoP displacement to be highest in the Lighten Up condition, this result is consistent with the idea that the Lighten Up instructions facilitated the deactivation of soleus and/or tibialis muscles, allowing step initiation to proceed with less lateral displacement of CoP, and thus promoting more efficient movement. In addition, the CoP trajectory was smoothest during the Lighten Up condition, suggesting more sophisticated control. Future studies should control movement timing and measure EMG during step initiation in order to shed more light on this issue.
Limitations and Future Directions
It is thought that PD reduces the ability to appropriately generate and inhibit motor commands 44 and to generate effective motor imagery. 45 Therefore, the ability of subjects with PD to apply these rather subtle instructions was somewhat surprising. However, this study only included subjects with mild to moderate PD and only tested subjects in the ON (medicated) state. Given the documented deficits in proprioception and body schema associated with PD,45,46 it is possible that severe PD (and its associated cognitive deficits) would interfere with the ability to direct focused intention to the body in this way. Future studies should investigate whether Lighten Up instructions (or Pull Up instructions) can benefit people with more advanced PD.
Further work is also needed to determine whether subjects with PD can maintain the instructions over longer time periods. While the instructions in this study were based on AT, they were extremely brief and primarily verbal. In contrast, a traditional course of AT study comprises a series of 30-minute (or longer) lessons, each of which includes considerable manual contact during movement. Previous research indicates that a course of 24 AT lessons is helpful for mobility in PD, and that the benefits can be retained for at least 6 months.15,16 Future studies should investigate whether the mechanisms seen here are retained after longer-term training. Repeated exposure to AT principles might also eliminate differences in familiarity between the 2 sets of instructions, which would remove another potential confound.
AT principles are meant to be applied to everyday movements such as standing, sitting, and walking. Thus, they are well-suited for combining with activity-based approaches. Given the success of combining AT with exercise for improving mobility and reducing discomfort in patients with back pain, 27 an approach combining AT instruction with exercise or other physical therapy methods47,48 may be worth pursuing for patients with PD.
Summary and Conclusions
Stooped posture is a particular problem in PD. 49 Dominant approaches to correcting postural alignment generally focus on actively doing something, such as tucking the pelvis, pulling back the shoulders, and so on. 50 However, among mindful movement practices there is precedent for a more subtle approach. In this study, subjects with PD briefly practiced different ways of standing upright, one of which was based on the AT. Our findings suggest that brief postural instructions can have acutely beneficial effects on motor problems associated with PD. Because the 2 sets of instructions we used had markedly different effects on postural sway, alignment, and movement smoothness, we conclude that the effects were not due to attention to the body, per se, or even solely to the increase in standing height. These results are consistent with previous results indicating that long-term training in the AT improves subtle control of axial tone and of coordination between the legs and torso,21,51 and they suggest that how one conceives of postural uprightness affects how one stands and moves, and that this influence can be harnessed for rehabilitative purposes.
Footnotes
Acknowledgements
We thank Catherine Kettrick and Tim Cacciatore for invaluable conversation.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Cohen is a certified teacher of the Alexander Technique and a member of the American Society for Alexander Technique. Oregon Health & Science University (OHSU) and Dr Horak have a significant financial interest in ADPM, a company that may have a commercial interest in the results of this research and technology. This potential institutional and individual conflict has been reviewed and managed by OHSU.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health (grants AG-006457, T32-NS045553, and T32-AT002688); Medical Research Foundation of Oregon; and University of Idaho College of Letters, Arts, and Social Sciences.