
Abstract
Introduction
Repetitive, task-related walking training is commonly identified as a key component of stroke rehabilitation following stroke.1,2 Task-related training, also referred to as task-oriented or task-specific training, is based on the premise that to learn to walk, one should practice walking. Despite the apparent simplicity of the concept, there is significant variability in the specific focus, treatment content, and outcomes achieved with the various walking-task training interventions in the literature.3-6 Given that a primary concern of poststroke physical therapy is the reacquisition of motor skills, we propose that motor-learning science offers a sound theoretical framework to develop a more coherent and effective task-related walking training intervention.
The goal of motor-learning science is to understand how people acquire motor skills through practice or experience. 7 From the literature, we know that individuals learn motor skills optimally under specific conditions. In recent years, practice conditions shown to elicit behavior changes have also been associated with changes in the activity and structure of the brain. 8 According to motor-learning principles (MLPs), learning is optimized when practice is abundant, engaging, challenging, and progressive. 9 We also know that learning is typically improved when practice is variable and random in order; practice conditions resemble the expected performance conditions; continuous tasks such as walking are practiced as a whole task; and feedback and guidance are provided in a manner that encourages error experience, self-evaluation, and self-correction.7-9
On review of community-based walking-training literature, application of these MLPs is arguably incomplete. Although most interventions incorporate some whole-task walking practice, adherence to other principles has been less consistent. Circuit-training interventions include variable-task practice; however, task stations frequently focused on part-task practice (eg, heel raises and step-ups) and were blocked in order, and authors failed to describe how feedback was provided.10-15 In studies rooted in a central pattern generator (CPG) theory of gait control and recovery, participants typically underwent whole-task practice of the gait cycle through body-weight-supported treadmill training (BWSTT), where practice was constant, guided, and usually had limited inclusion of overground walking.16-19
In addition to uneven application of MLPs, many outpatient-based walking training studies fail to compare the experimental intervention with an alternative approach to task-oriented training. For example, circuit training interventions have been compared with seated activities or standard physical therapy care,10,11,13 whereas in outpatient BWSTT studies, one BWSTT protocol was compared with another BWSTT protocol or with a nonwalking activity.17,18 In the Locomotor Experience Applied Post-stroke (LEAPS) trial, 20 BWSTT was compared with a supervised, home exercise program. In this study, the BWSTT and the home exercise programs were found to be equally effective. 19 On first read, this study seems to indicate that there is no added value of task-oriented walking training over non-task-oriented training; however, the inclusion of walking-specific goal setting, 20 instructions to walk daily, frequent supervision, and the context-specific home environment 21 may have led to a substantial amount of walking-specific practice by the comparison intervention group. As the home therapy intervention was not explicitly based on any particular theoretical framework nor intentionally designed to include task-related practice, interpreting the implications of these results is challenging.
In summary, the literature is still not clear whether one approach to task-oriented walking-skill training is superior to another. More research is required to identify the essential ingredients of an optimally effective, poststroke walking-skill training intervention for individuals living in the community. We propose that a systematic, motor-learning-science–framed research approach would lead to an increased understanding of crucial treatment components and subsequently result in improved patient outcomes.
The purpose of this randomized controlled trial was to evaluate the impact of the Motor Learning Walking Program (MLWP) in community dwelling individuals within 1 year of stroke onset. The MLWP is an intensive, varied, task-specific, overground walking training program organized to be consistent with key MLPs. In an effort to assess the relative value of motor-learning science as a theoretical framework, the MLWP was compared with BWSTT, an approach rooted in the CPG theory of gait control and recovery.
Methods
All study activities were approved by the Research Ethics Boards of St Joseph’s Healthcare Hamilton (SJHH; #6-2753); the Hamilton Health Sciences (#07-054), Hamilton, Ontario; and Joseph Brant Memorial Hospital, Burlington, Ontario. The study was registered at ClinicalTrials.gov (#NCT00561405). A detailed description of the study methods, including rationale and content of the interventions, can be found in the previously published protocol article. 22
This study was a randomized, parallel-group (1:1) trial with stratification by baseline comfortable gait speed (<0.5 m/s, and ≥0.5 m/s). A gait speed of 0.5 m/s represents the velocity required to safely cross a street at a marked crosswalk. 23 Design included concealed allocation during screening and randomization, rater-blinded outcome assessment, and intention-to-treat analysis.
Between January 1, 2007, and August 31, 2010, participants were recruited through clinician referrals from inpatient acute and rehabilitation units and outpatient rehabilitation programs at 3 teaching hospitals in the neighboring cities of Hamilton and Burlington, Ontario. Some participants were recruited through newspaper advertisements and local stroke survivor groups. Referred patients were screened by a research coordinator and underwent written informed consent and baseline assessment. A permuted block (block sizes 2, 4, and 6) randomization schedule was created and administered by a central randomization service (SJHH Biostatistics Unit). On completion of the screening, consent, and baseline assessment, group assignment was communicated by e-mail to the research coordinator. In an effort to minimize expectation bias, participants and therapists in both groups received information that promoted the rationale and potential benefits of their assigned intervention and were blinded to the study hypotheses.
Participants
Inclusion criteria were as follows: (1) ≥40 years old, (2) living in the community, (3) <12 months since onset of ischemic or hemorrhagic stroke, (4) able to walk 10 m without assistance (gait aid allowed), (5) able to follow a 2-step verbal command, and (6) independent community ambulation prior to stroke. Individuals were excluded if they presented with (1) cognitive impairment (ie, Mini Mental Status Exam score less than age and education norms) 24 ; (2) severe visual impairment; (3) lower-extremity amputation; (4) unstable cardiac, medical, or musculoskeletal conditions that would limit treatment participation (determined by physician screening and baseline interview); or (5) comfortable gait speed >1.0 m/s without a gait aid.
Interventions
Participants were assigned to the experimental MLWP or the comparison BWSTT intervention. The aim of the MLWP was to engage participants in the practice of a variety of overground walking tasks relevant to community mobility. 25 Under the supervision of one physical therapist, participants in the MLWP group practiced 7 core walking activities at every session: (1) short walks; (2) longer distance (≥50 m); (3) steps, curbs, and slopes; (4) obstacle avoidance; (5) transitions (eg, sit to stand and walk); (6) changes in centre of gravity (eg, pick up an object off floor); and (7) changes in direction. Within each session, an approximately equal amount of time was spent practicing each of the core tasks. When a participant was observed to consistently perform a specific task without physical assistance, the challenge level was adjusted through the addition of concurrent verbal or physical tasks, reduced time constraint, altered terrain and/or lighting, increased duration, reduced predictability, and/or performance in a mobile environment. In addition to variable practice and task-related practice, sessions were organized in a manner consistent with MLPs related to guidance, feedback, and order of practice. 7
The comparison BWSTT was structured to provide participants with the opportunity to practice high repetitions of a near-normal gait pattern while supported over a treadmill and assisted by one or more physical therapy staff. This approach to training is rooted in the CPG theory of gait control and recovery 26 and based on protocols described in the literature.17,27
Both intervention groups were offered 15 sessions over 5 weeks in an outpatient clinic setting. Sessions were 1 hour long, including setup, vital sign assessment, and rest periods. Refer to Table 1 for a comparison of the 2 interventions. To minimize risk of contamination, each intervention was provided by a separate group of physical therapists trained in their respective interventions (MLWP, n = 4; BWSTT, n = 4). Therapist training was delivered by the Principal Investigator (VDP) and included reading and discussion of selected literature and intervention protocol documents, role-playing practice, and cotreatment of at least 1 participant. Ongoing treatment fidelity was facilitated through regular (at least once per month) observation sessions, case discussions, and review of training documentation by the principal investigator.
Description of Experimental and Comparison Interventions.
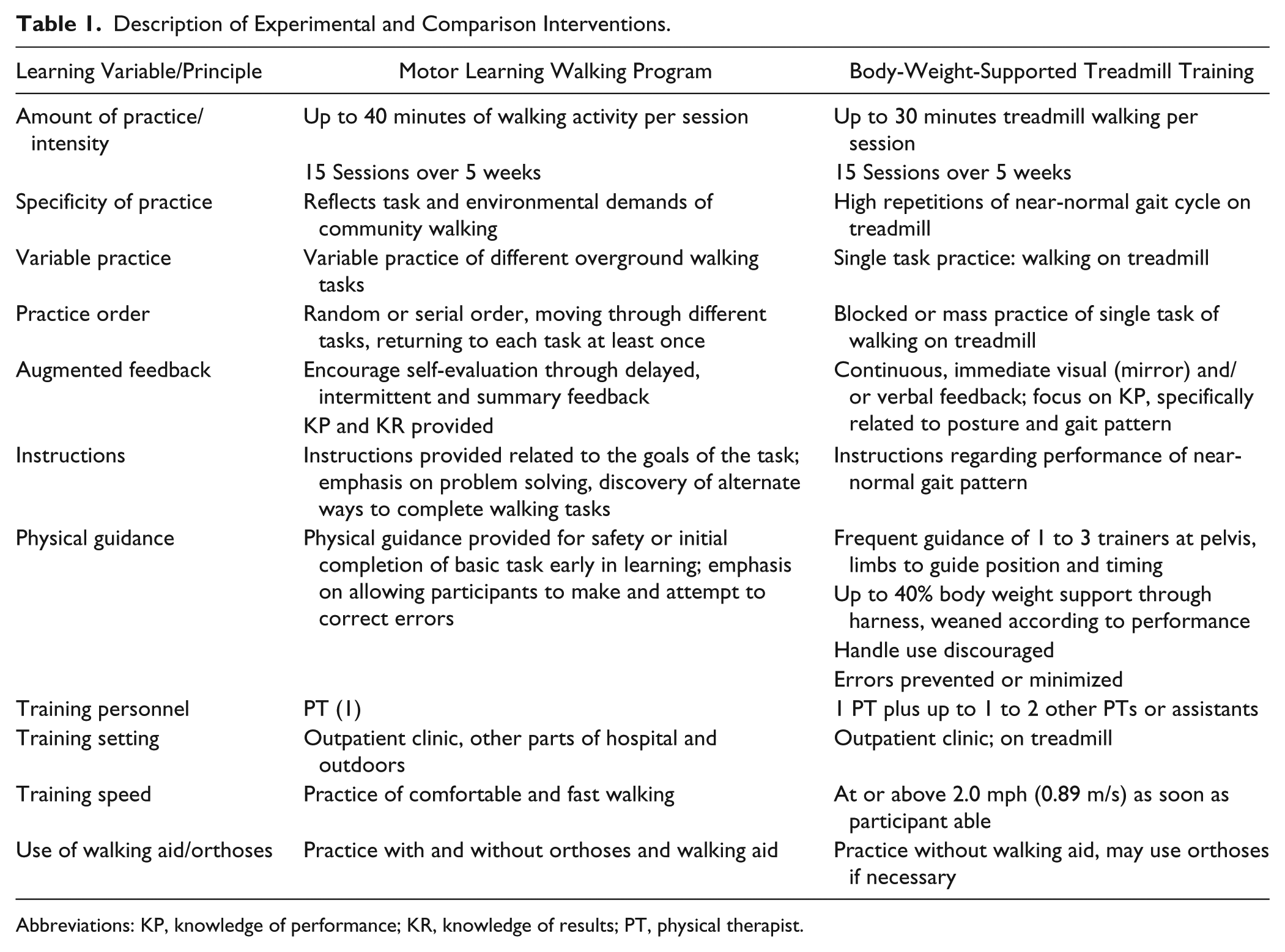
Abbreviations: KP, knowledge of performance; KR, knowledge of results; PT, physical therapist.
Outcomes
The primary outcome for this study was comfortable gait speed measured following treatment completion (T2). Gait speed, measured using the 5-m walk test28,29 has been shown to be reliable (r = 0.94), responsive to change, and significantly related to independent community ambulation in individuals with stroke. 30 Patients were also assessed using the following outcome measures, all shown to be reliable and valid in individuals with stroke: 5-m Walk Test (maximum pace)28,29; 6-Minute Walk Test 29 ; the Functional Balance Test (FBT), 31 a test of higher level balance and walking control; the Activities-specific Balance Confidence Scale 32 ; the modified Functional Ambulation Categories 33 ; and the Stroke Impact Scale 3.0. 34 Community mobility participation was measured using the Life Space Assessment, 35 which has been shown to be reliable, valid, and responsive to change in older adults. All outcomes were measured by a blinded physical therapist assessor within 1 week prior to initiating training (T1), within 1 week following completion of training (T2), and 2 months after training (T3). At every visit, participants were asked to recall whether they had a fall, how many falls, and if they required medical care for the fall or any other reason since their last visit. In a convenient sample of participants from both intervention groups, step activity during treatment sessions was collected using StepWatch 3.0 step activity monitors (Orthocare Innovations, Oklahoma City, OK). 36
Analysis
Descriptive statistics were used for baseline characteristics and outcomes scores (means with standard deviation [SD], or median with first [Q1] and third quartile [Q3]) for continuous variables and counts (percentage) for categorical variables. Intention-to-treat analysis with multiple imputation technique for missing values 37 was used for between-group comparisons for primary and secondary outcomes. For primary analysis, postintervention (T2) comfortable walking speeds for the intervention groups were compared using analysis of covariance with group (MLWP or BWSTT) and baseline speed stratum (ie, slow or fast) as factors. Secondary analysis included between-group comparisons of gait speed at the 2-month follow-up (T3) and all other outcomes at T2 and T3 using analysis of covariance. For each outcome, 2 covariates were used: baseline comfortable gait speed and the baseline value of the outcome of interest. In addition, an odds ratio of the frequency of participants in the MLWP group achieving a meaningful change in gait speed at T2 (≥0.14 m/s) 38 compared with participants receiving BWSTT was calculated using χ2 statistics. All statistical tests were 2-sided with a 0.05 level of significance. The Bonferroni correction method was used to adjust the level of significance for testing for secondary outcomes. Analysis was performed using IBM SPSS Statistics 20.0 for Windows (Somers, NY) and SAS 9.2 (Cary, NC).
The sample size estimate was based on review of previously reported poststroke gait rehabilitation studies. To reliably detect a meaningful between-group difference of 0.14 m/s 38 in gait speed (assuming a SD of 0.19 m/s,11,16,17 with 80% power at a 2-tailed significance level of 0.05), the sample size was calculated to be 29 participants per treatment group. Considering the loss to follow-up rates reported in the literature, which ranged from 7% 11 to 20% 17 , a 17% loss was allowed, resulting in a total recruitment target of 70 participants.
Results
A total of 186 individuals within 1 year of stroke were referred for screening. Of these, 71 participants met inclusion and exclusion criteria, consented, and were randomized (MLWP, n = 35; BWSTT, n = 36). The mean age of participants was 67.3 (SD = 11.6) years, with a mean of 20.9 (SD 14.1) weeks since stroke onset. One participant from each group withdrew for personal reasons after baseline assessment and before beginning training. A total of 64 participants were assessed at posttreatment (T2: MLWP = 30; BWSTT = 34); 58 participants were assessed at follow-up (T3: MLWP = 26; BWSTT = 32). Participant flow is presented in Figure 1.
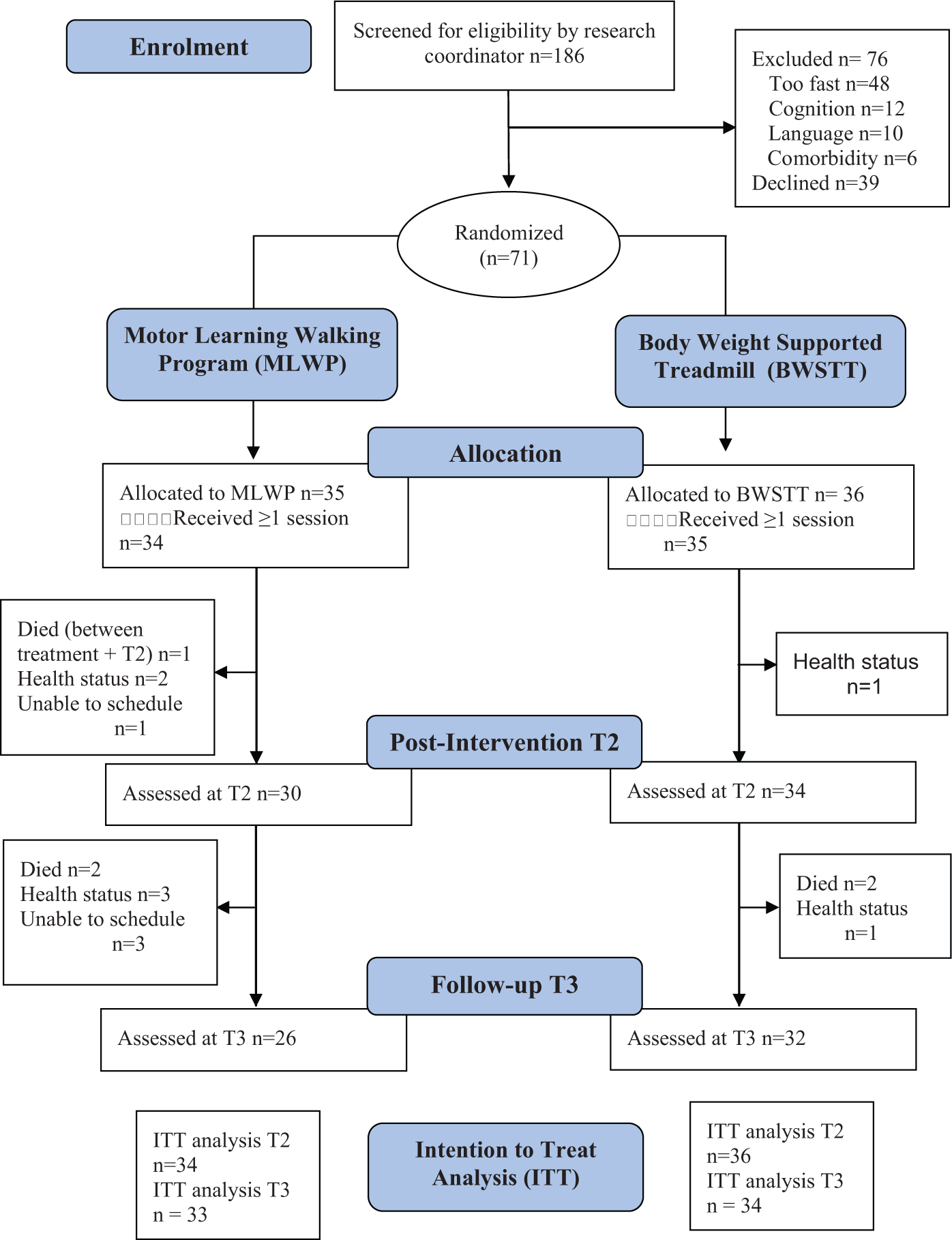
Consort diagram depicting participant flow during study.a
The 69 participants who undertook at least 1 treatment completed an average of 13 training sessions (MLWP, 13.29 [SD 4.33]; BWSTT, 13.50 [SD 3.87]). In a sample of convenience, there was no significant between-group difference for number of steps per treatment session (P = .61), with 1620 (SD = 624) steps taken during MLWP (n = 19) and 1712 (SD = 487) steps taken during BWSTT (n = 21).
Groups were balanced on baseline characteristics (see Table 2). In Table 3, the observed data have been summarized using mean scores for primary and secondary outcomes at baseline, postintervention, and follow-up. In Table 4, the differential effects of the MLWP over BWSTT for primary and secondary outcomes at T2 and T3 are presented for intention-to-treat and adjusted analysis.
Baseline Characteristics of Study Participants.
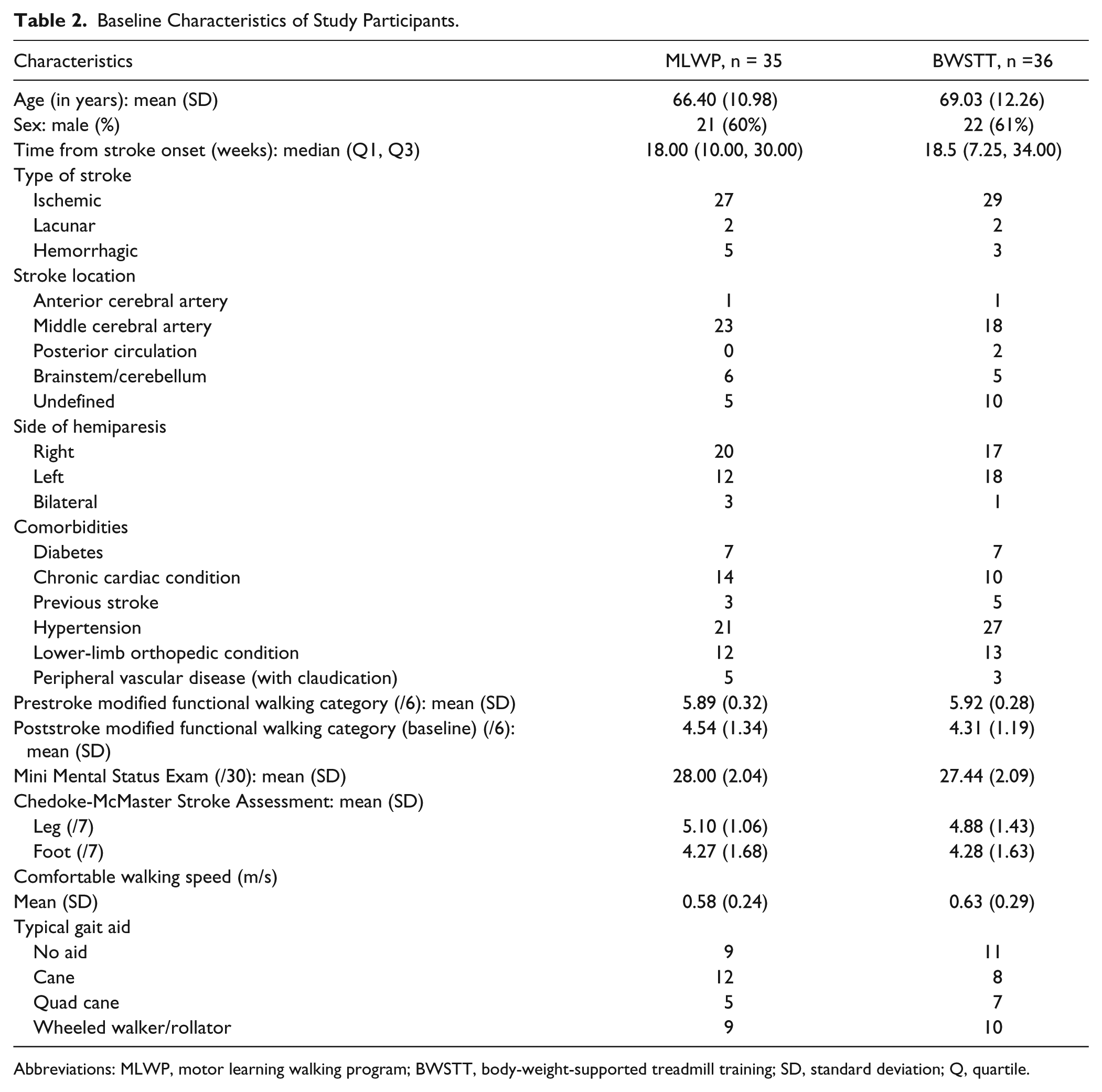
Abbreviations: MLWP, motor learning walking program; BWSTT, body-weight-supported treadmill training; SD, standard deviation; Q, quartile.
Observed Primary and Secondary Outcomes at T1, T2, and T3.
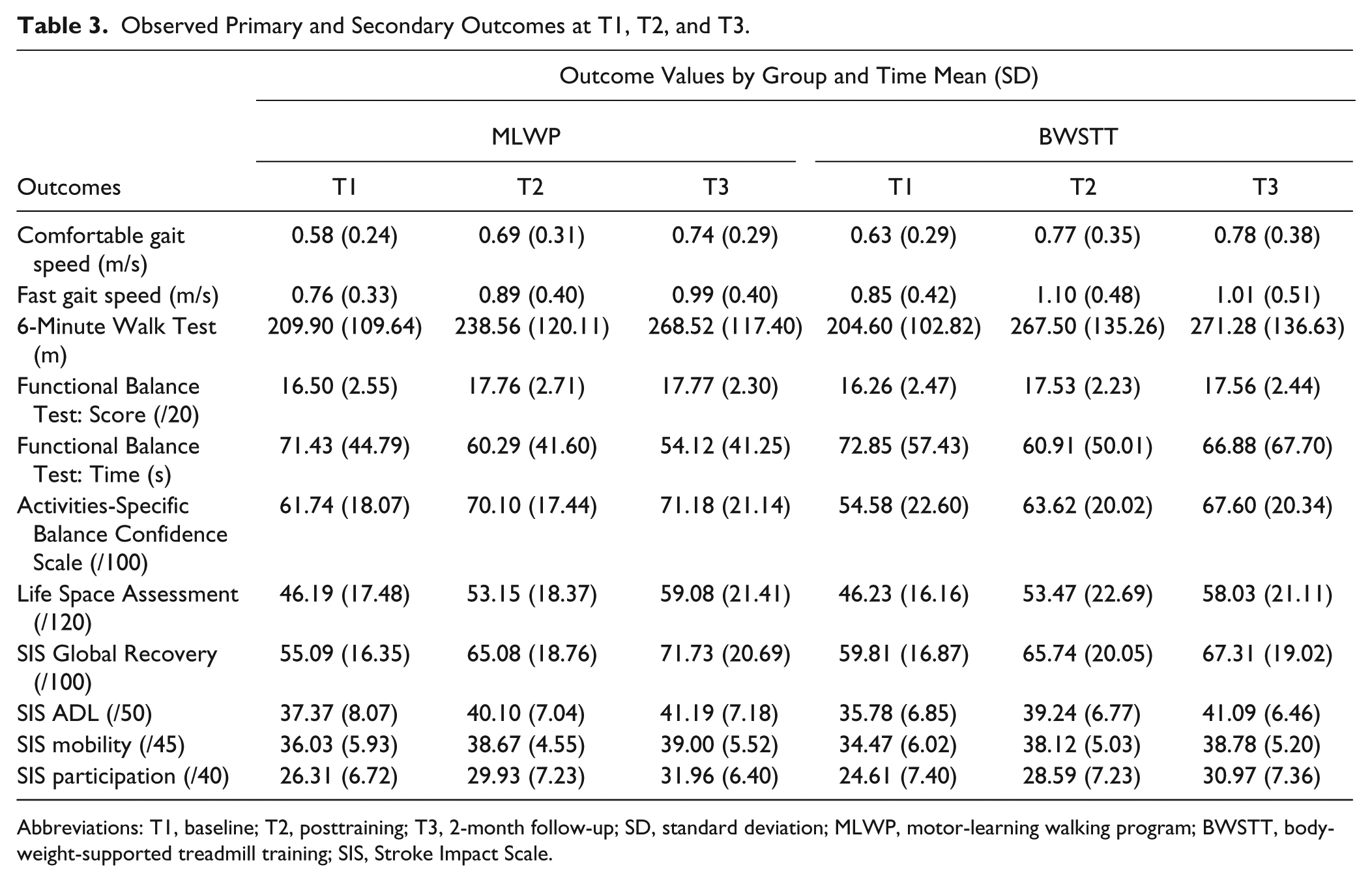
Abbreviations: T1, baseline; T2, posttraining; T3, 2-month follow-up; SD, standard deviation; MLWP, motor-learning walking program; BWSTT, body-weight-supported treadmill training; SIS, Stroke Impact Scale.
Adjusted Differential Effect of MLWP Over BWSTT at T2 and T3 Using Intention-to-Treat Analysis. a
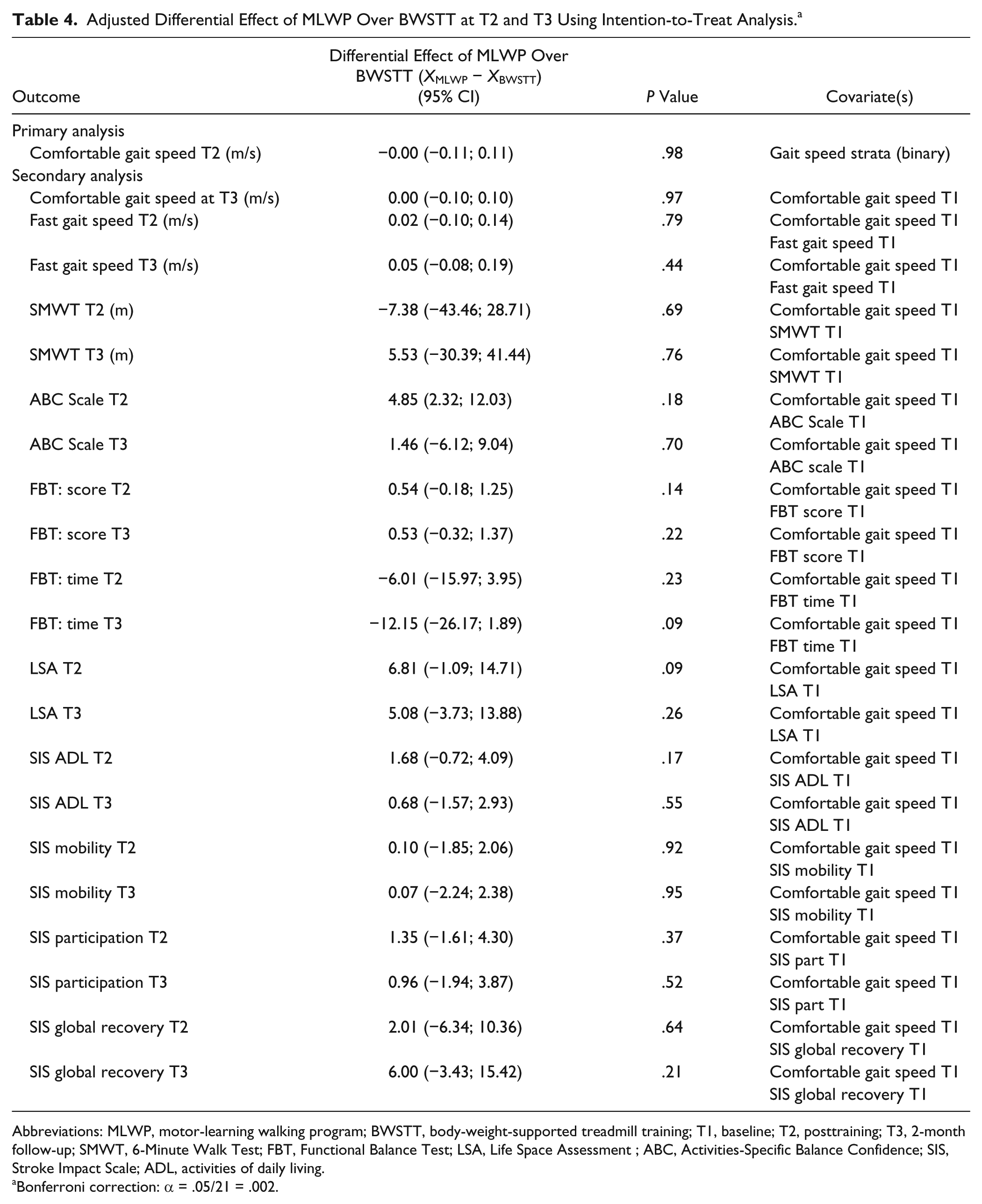
Abbreviations: MLWP, motor-learning walking program; BWSTT, body-weight-supported treadmill training; T1, baseline; T2, posttraining; T3, 2-month follow-up; SMWT, 6-Minute Walk Test; FBT, Functional Balance Test; LSA, Life Space Assessment ; ABC, Activities-Specific Balance Confidence; SIS, Stroke Impact Scale; ADL, activities of daily living.
Bonferroni correction: α = .05/21 = .002.
Primary Outcome
There was no significant between-group difference in comfortable gait speed at T2. Mean between-group difference was 0.002 m/s (95% CI = −0.112, 0.117; P > .05). Both groups improved comfortable gait speed following treatment. Based on the primary adjusted analysis, including multiple imputation, the change in gait speed at T2 in the MLWP group was 0.14 m/s (95% CI = 0.09, 0.19) and 0.14 m/s (95% CI = 0.08, 0.20) in the BWSTT group.
Secondary Outcomes
There were no significant between-group differences in any of the secondary outcome measures at T2 or follow-up (T3). Although effect sizes did not reach statistical significance, participants in the MLWP group tended to perform the FBT, a test of higher level balance and walking, 31 more quickly than participants in the BWSTT group at T2 (between-group difference = −6.01 s; 95% CI = −15.97, 3.95) and T3 (between-group difference = −12.15 s; 95% CI = −26.17, 1.89).
Participants in both groups demonstrated gains in all functional performance outcome measures (gait speed, 6-Minute Walk Test, and FBT) from T1 to T2. From T2 to T3, scores in both groups improved or were maintained on all outcomes, except the FBT in the BWSTT group, where performance deteriorated between T2 and T3.
When gait speed data were dichotomized, at T2, 50% (15 of 30) of MLWP participants improved their gait speed by 0.14 m/s or more between T1 and T2, compared with 32% (n = 11 of 34) of the BWSTT group. On χ2 analysis, the between-group difference was not statistically significant (odds ratio = 2.10; 95% CI = −0.58, 3.98; P = .143).
Falls and Adverse Events
There were no between-group differences in rates of falls over the entire study period. Based on interview data at T2 and T3, 11 of 30 (36.7%) participants in the MLWP, and 10 of 32 (31.3%) in the BWSTT group reported at least 1 fall between T1 and T3. Only 2 (6.6%) participants in the MLWP and 4 (12.5%) in the BWSTT group reported multiple falls. Regarding other serious adverse events, a total of 3 patients (4.5%; 2 [6.2%] MLWP, 1 [2.7%] BWSTT) reported a new stroke or transient ischemic attack over the study period; also, 2 participants had cardiac events requiring hospitalization, both in the BWSTT group. A total of 4 participants died during the study period; 1 person in the MLWP group died following a new stroke 1 week after completing the 15 intervention sessions and just prior to the postintervention assessment (T2); 3 participants died between assessments at T2 and T3 (MLWP, 1; BWSTT, 2). It is important to note that no participant died, had a cardiac event, or stroke during or between treatment sessions.
Discussion
The intention of this randomized controlled trial was to compare the impact of 2 different approaches to task-related walking training in ambulatory, community-dwelling individuals within 1 year of stroke. We hypothesized that the MLWP, a walking training intervention designed to adhere to key MLPs, would be more effective than BWSTT, an intervention based on a CPG theory of gait control. The failure to detect a significant difference between these 2 interventions challenges us to reevaluate our original assumptions.
The principal assumption underlying this trial was that consistent adherence to MLPs would increase the effectiveness of task-related walking training. Borrowing Whyte’s analogy of a recipe, 39 each of these learning “ingredients” (ie, intensity, specificity, whole-task practice, variability, order, feedback, and guidance) were assumed to be active, potent factors in improving walking skill. On reflection, it is likely that in this patient cohort, some motor learning ingredients are more important, or potent, than others. When step activity was measured during treatment sessions, both MLWP and BWSTT groups took more than 3 times the mean number of steps (507, SD = 64) observed by Lang et al 40 during standard outpatient stroke physical therapy sessions. Perhaps, as observed in animal models, 41 as long as an individual practices walking in some manner, amount or intensity of practice becomes the most potent treatment ingredient. This premise is consistent with previous reviews of gait training literature that fail to find a difference in treatment effect between different approaches to intensive walking-focused training in neurorehabilitation populations.21,42,43 Notwithstanding our primary conclusions that the 2 walking-focused interventions were equally effective, results on the FBT remain intriguing. The FBT is a novel timed test of dynamic balance during walking. 31 Participants perform a continuous circuit of walking-related tasks (ie, stand up from a chair and walk, walk up and down a step, pick up an object off floor while walking, turn and walk back to chair) on a 9-m track. Although the between-group comparison of times did not reach statistical significance (P = .09), participants in the MLWP group improved their time from T1 to T2 and again at T3, whereas the BWSTT group improved their performance from T1 to T2 but seemed to deteriorate at T3. As the demands of this test more closely resemble the practice items within the MLWP, this result may be cautiously interpreted as support for the principle of specificity of practice. 7 Alternately, they may reflect a potentially beneficial effect of the variable practice within the MLWP. According to the schema theory of motor control, variable practice of a particular skill helps the learner develop a stronger, more flexible schema for that skill, leading to an increased ability to perform that skill in different environments and task conditions. 44 It is possible that the 5-m walk test was not optimally suited to detect such a benefit.
Based on motor learning science, the MLWP was specifically designed to encourage cognitive effort and problem solving during training. 9 Practice tasks were random or serial in order, and feedback and guidance was delayed or limited in frequency to allow self-evaluation and correction of errors. Although these strategies have been associated with improved outcomes after stroke,45-47 there is evidence that the degree of benefit is influenced by the complexity of the skill being learned and the experience of the learner.48-50 In an effort to standardize application of these principles, the study protocol did not allow for patient-specific adjustments in terms of feedback provision or practice order to match the characteristics of the learner and the task. It is possible that this protocol rigidity may have limited the overall effectiveness of the intervention.
In their challenge-point framework, Guadagnoli and Lee 51 propose a task- and person-specific approach to structuring practice. When individuals practice a motor skill, they receive a certain amount of information about their performance from their internal feedback systems or from external sources such as a therapist. This information represents challenge, where too little or too much information can limit learning. The optimal information level, or challenge point, depends on the skill and experience of the learner/patient, combined with the difficulty level of the task. The role of the therapist is to adjust the task challenge level by adjusting variables such as practice order, frequency of feedback, and provision of guidance, ultimately finding the optimal challenge point for a particular patient. There is emerging evidence to support the use of a challenge point framework in arm and hand rehabilitation in Parkinson’s disease 52 and reactive balance training after stroke. 53 Future research should explore the application of this framework in walking retraining poststroke.
Despite a lack of between-group differences in the primary outcome, it is important to note that both interventions resulted in a clinically meaningful change (0.14 m/s) in comfortable gait speed. 38 In addition, the magnitude of change in this study was comparable to the change previously reported for patients of similar functional status and stroke chronicity undergoing task-related training.10,11,16 Although participants in the LEAPS study 19 made larger gains in gait speed (0.25 m/s), interventions began almost 3 months earlier, and the magnitude of change has been shown to diminish with time poststroke onset. 54 In addition, the interventions in our study included only 15 sessions compared with 36 sessions in the LEAP protocol. 19 It is possible that the impact of the MLWP and the BWSTT programs in our study would have been greater if these interventions were initiated sooner after stroke and for a longer duration. Use of repeated-measures design over an extended training period could help identify optimal timing, duration, and frequency of walking training in this population.
In the literature, between 37% and 73% of individuals with stroke report at least 1 fall, and 20% to 55% report repeated falls. 55 In our study, both the MLWP and BWSTT groups had a relatively low rate of at least 1 fall (37.7% and 31.3%) and multiple falls (6.6% and 12.5%) over the study period. In addition, in the LEAPS, fall rates were highest in the early BWSTT group compared with the home exercise group. 19 The authors hypothesized that the difference may be related to the lack of balance-specific training in the BWSTT intervention compared with the home exercise program. Considering that the MLWP intervention included dynamic balance challenges within the context of walking, it is somewhat surprising that the MLWP group did not report fewer falls in our study. The overall low fall rates and no between-group differences may be related to the short follow-up time or a difference in data collection methods (retrospective vs prospective). Future research should ensure prospective collection 56 of falls over prolonged time periods (eg, 6-12 months) and an adequate sample size to detect between-group differences in this important outcome.
Without definitive evidence in support of MLWP over BWSTT, clinicians may base treatment decisions on practical considerations such as patient preference, treatment setting, and equipment and human resources availability. BWSTT required an average of 1.4 staff per session compared with 1 therapist for the MLWP. Assuming the median hourly rates for a physical therapist is $37.00/hour and $25.00/hour for a physical therapy assistant (PTA), 57 15 one-hour sessions of MLWP supervised by 1 therapist would cost $555.00, whereas the same dose of BWSTT supervised 1 one therapist and assisted by a PTA (on 40% of the sessions) would cost $705.00. In addition, BWSTT requires specialized equipment, whereas the MLWP incorporates objects found in any therapy department, or home and could be delivered in a community or clinical setting. Although this trial did not include a formal economic analysis, clinicians and administrators may consider MLWP to be a cost-effective, flexible treatment option for ambulatory, community-dwelling individuals with history of stroke.
Limitations
Unfortunately, 2 participants withdrew from the study prior to training (MLWP, 1; BWSTT, 1), 5 participants were lost to follow-up at T2 (MLWP, 4; BWSTT, 1), and 11 participants were lost to follow-up at T3 (MLWP, 8; BWSTT, 3; see Figure 1). Participants in the MLWP group were more likely to be lost for reasons other than death. Because session attendance was equal between groups, and treatment was typically completed before the loss, it is unlikely that this imbalance reflects a specific intolerance to the MLWP intervention. Despite this loss, we reached the target sample size for the primary outcome. In addition, lost data were imputed to retain the benefits of random allocation. In this study, we intentionally compared 2 intense, task-related walking interventions. Because neither of these interventions represents standard practice, we cannot be certain that the observed changes were greater than expected with active, standard physical therapy care. We expect that the increased focus on walking would lead to better outcomes; however, this needs to be confirmed through further research. To amplify the difference between interventions, the MLWP did not include treadmill walking, and BWSTT did not include overground training. Combined interventions may be more typical of clinical practice and have been associated with some positive outcomes.58,59 The field would benefit from further evaluation of novel treatment combinations that target walking-skill reacquisition. Finally, this trial represents a comparison of 2 relatively complex, principles-driven interventions. We are confident that the interventions differed substantially in terms of mode of walking, variability of practice, and provision of physical guidance; however, fidelity to principles related to feedback provision and cognitive engagement were less easily documented. Although we believe that therapists were adequately trained and mentored regarding these motor learning variables, failure to document actual adherence limits our ability to comment on the relative impact of these principles on our findings.
Conclusion
In this randomized controlled trial, we compared 2 intensive, task-related walking-skill training programs that were different in theoretical rationale and level of adherence to specific MLPs. Both interventions were associated with a clinically meaningful improvement in walking performance in this group of community dwelling individuals within 1 year of stroke. There were no significant between-group differences on primary outcome of comfortable gait speed. Clinical decisions may be informed by pragmatic considerations such as equipment and staff availability and patient preference. Further experimental and clinical research is required to determine the individual impact of and interactions between specific motor-learning variables on walking retraining outcomes after stroke.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was completed through funds received by the Ontario Stroke Network, Ministry of Health and Long Term Care, ON (Grant #06356), and from the Father Sean O’Sullivan Research Centre, Hamilton, ON, Canada. This research was conducted as a component of VDP’s doctoral studies for which he received a Canadian Institutes of Health Research Doctoral Student Award.
Authors’ Note
Trial Registration: ClinicalTrials.gov no. NCT00561405.