
Abstract
Background. Impaired trunk motor control is common after stroke. Combining transcutaneous electrical nerve stimulation (TENS) with task-related trunk training (TRTT) has been shown to enhance the recovery of lower limb motor function. Objective. This study investigated whether combining TENS with TRTT would enhance trunk control after stroke. Methods. Thirty-seven subjects with stroke were recruited into a randomized controlled clinical trial. Subjects were randomly assigned to any one of the three 6-week home-based training groups: (1) TENS + TRTT, (2) placebo TENS + TRTT, or (3) control without active training. The outcome measures included isometric peak trunk flexion torque and extension torque; forward seated and lateral seated reaching distance to the affected and unaffected side; and Trunk Impairment Scale (TIS) scores. All outcome measures were assessed at baseline, after 3 and 6 weeks of training, and 4 weeks after training ended at follow-up. Results. Both the TENS + TRTT and the placebo-TENS + TRTT groups had significantly greater improvements in isometric peak trunk flexion torque and extension torque, lateral seated reaching distance to affected and unaffected side, and TIS score than the control group after 3 weeks of training. The TENS + TRTT group had significantly greater and earlier improvement in its mean TIS score than the other 2 groups. Conclusions. Home-based TRTT is effective for improving trunk muscle strength, sitting functional reach and trunk motor control after stroke in subjects without somatosensory deficits. The addition of TENS to the trunk augments the effectiveness of the exercise in terms of TIS scores within the first 3 weeks of training.
Keywords
Introduction
An increasing number of intervention studies have focused on improving the trunk motor control of subjects with stroke.1-4 Trunk motor control refers to the ability of the trunk muscles to hold the trunk upright, adjust to weight shifts, and perform selective movements during static and dynamic postural adjustments.2,5 Numerous studies have documented how trunk motor control is impaired in subjects with stroke.1,2,5,6 A longitudinal study 6 comparing the recovery of trunk motor control in 32 subjects after a stroke revealed that the majority still presented mild to severe trunk impairment after 6 months. Trunk motor control is important for functional skills such as dressing, transfers, and walking, 7 and it is correlated with functional balance 2 and functional mobility.2,8
Muscle weakness following stroke is well documented. 9 Studies revealed that both isometric and isokinetic trunk muscle strength was lower in patients with stroke when compared with healthy controls.5,10 In addition, electromyography activities of trunk muscles on the affected side of the body were reduced and delayed relative to the unaffected side during self-initiated voluntary flexion and extension of trunk, 11 and during rolling from supine to side lying in patients with stroke. 12 A significant positive correlation was found between trunk muscle strength and sitting balance, 13 and functional balance performance in patients with stroke. 10
Sensory input is required for motor performance and skill acquisition. 14 Transcutaneous electrical nerve stimulation (TENS) has been demonstrated to excite large sensory fibers, predominantly in the A-beta range. 15 Through the cutaneous stimulation of muscles, it increases the excitability of the sensorimotor cortex. 16 Levin and Hui-Chan 17 demonstrated that 3 weeks of 60-minute TENS sessions applied to the common peroneal nerve improves the ankle dorsiflexor strength of stroke survivors. Ng and Hui-Chan 18 have reported that subjects with chronic stroke receiving TENS followed by task-related training had significantly earlier and greater improvement in ankle dorsiflexion torque after 2 weeks of treatment than matched controls receiving TENS alone, placebo-TENS with task-related training or no treatment. In a subsequent study, 19 these authors further demonstrated that combining TENS with task-related training could significantly improve gait speed and walking endurance in subjects with stroke when compared with placebo stimulation or no treatment.
There is growing evidence supporting the effectiveness of task-related training in stroke rehabilitation. 20 Subjects with stroke whose practiced seated reaching tasks for 10 sessions over 2-week period could significantly improve the sitting balance with longer seated reaching distance than the subjects whose practiced upper limb tasks. 3 Recent studies have demonstrated that 10 to 15 hours of task-related trunk training (TRTT) significantly improves trunk motor control of subjects with stroke as measured by the Trunk Impairment Scale (TIS).1,2 With the previous reports showing that combining TENS with task-related training can improve motor control in the lower limbs,18,19 it is plausible that TENS applied to the trunk muscles during TRTT could augment the motor output of trunk muscles during the training. This study was designed to test that idea by comparing the effectiveness of 3 treatment protocols—(1) TENS + TRTT, (2) placebo-TENS + TRTT, and (3) no active treatment—for subjects with chronic stroke. The output measures focused on trunk muscle strength, functional seated reaching distance, and trunk motor control.
Methods
Study Design
The study was an assessor-blinded, stratified, randomized, placebo-controlled clinical trial. As no previous study has investigated the effect of electrical stimulation on trunk motor control with stroke subjects, the power analysis was based on a meta-analysis examining the effect of functional electrical stimulation on force production in stroke survivors. 21 The sample size was calculated using the Power Analysis and Sample Size software package (version 8 for Windows). An average effect size for the outcome measures of 0.59 was adopted on the basis of the meta-analysis. The estimated sample size for each group was 11. Four additional subjects were recruited in anticipation of a drop-out rate of 10% during the course of the study. The confidence level for statistical significance was set at 5% (α = .05) with power equal to 80% (β = 0.2).
Randomization
After obtaining the written consent of those recruited, an initial assessment of eligibility was performed. A research assistant gave those who fulfilled the inclusion and exclusion criteria a baseline assessment involving all of the outcome measures. After that baseline assessment, concealed randomization was conducted by a clerical worker who was not involved in the study. In order to achieve a nearly even distribution of important parameters among the groups, the randomization was stratified using Minimize computer software. 22 The stratification was based on age (≤60 or >60 years), gender (male or female), and the hemiplegic side (left or right), because age, gender, and hemiplegic side have been shown to have known effects on the outcome measures.23,24
Subjects
Forty-six subjects were initially recruited for the study. Subjects were included if they had been diagnosed with single stroke more than 6 months previously, had impaired sitting balance as indicated by a balance score of 3 to 5 out of 6 on the Motor Assessment Scale, 25 had been discharged from all rehabilitation services for more than 3 months, and could get support by a caregiver for the home-based program. Potential subjects were excluded if they had medical comorbidities such as unstable blood pressure, used a cardiac pacemaker, had cognitive impairment indicated by scoring less than 7 out of 10 on the Abbreviated Mental Test, 26 had unilateral neglect as indicated by a star cancellation test score of less than 47, 27 or showed severe sensory deficits in the pin prick test. 28 Subjects were asked to close their eyes. Subjects were then asked whether he or she could feel the needle pricks when the tip of a sterile safety pin was pressed perpendicularly to the bare skin of the trunk. Subjects were excluded because of severe sensory deficits, using cardiac pacemakers, or having unstable blood pressure. Thirty-seven subjects met the inclusion criteria. A flow diagram of the recruitment is shown in Figure 1.
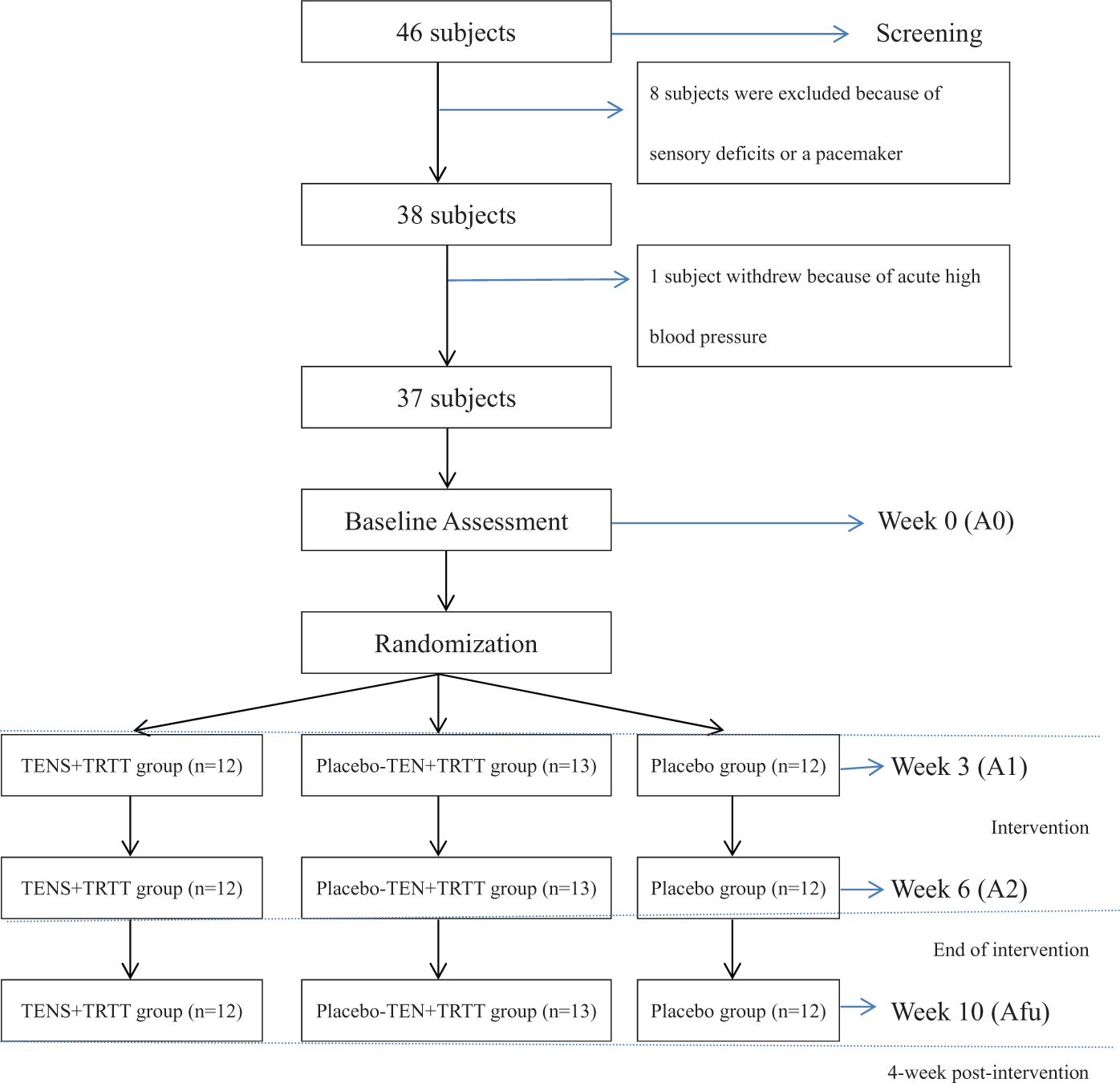
Flow diagram of subjects being recruited to the study.
Ethical Considerations
All the candidates were informed about the objectives of the study, and they were required to sign consent forms before the assessment. The protocols were approved by the Ethics Review Committee of the Hong Kong Polytechnic University. The clinical trial was reported to the US National Institutes of Health for international reference (ClinicalTrials.gov identifier: NCT01200030).
Intervention
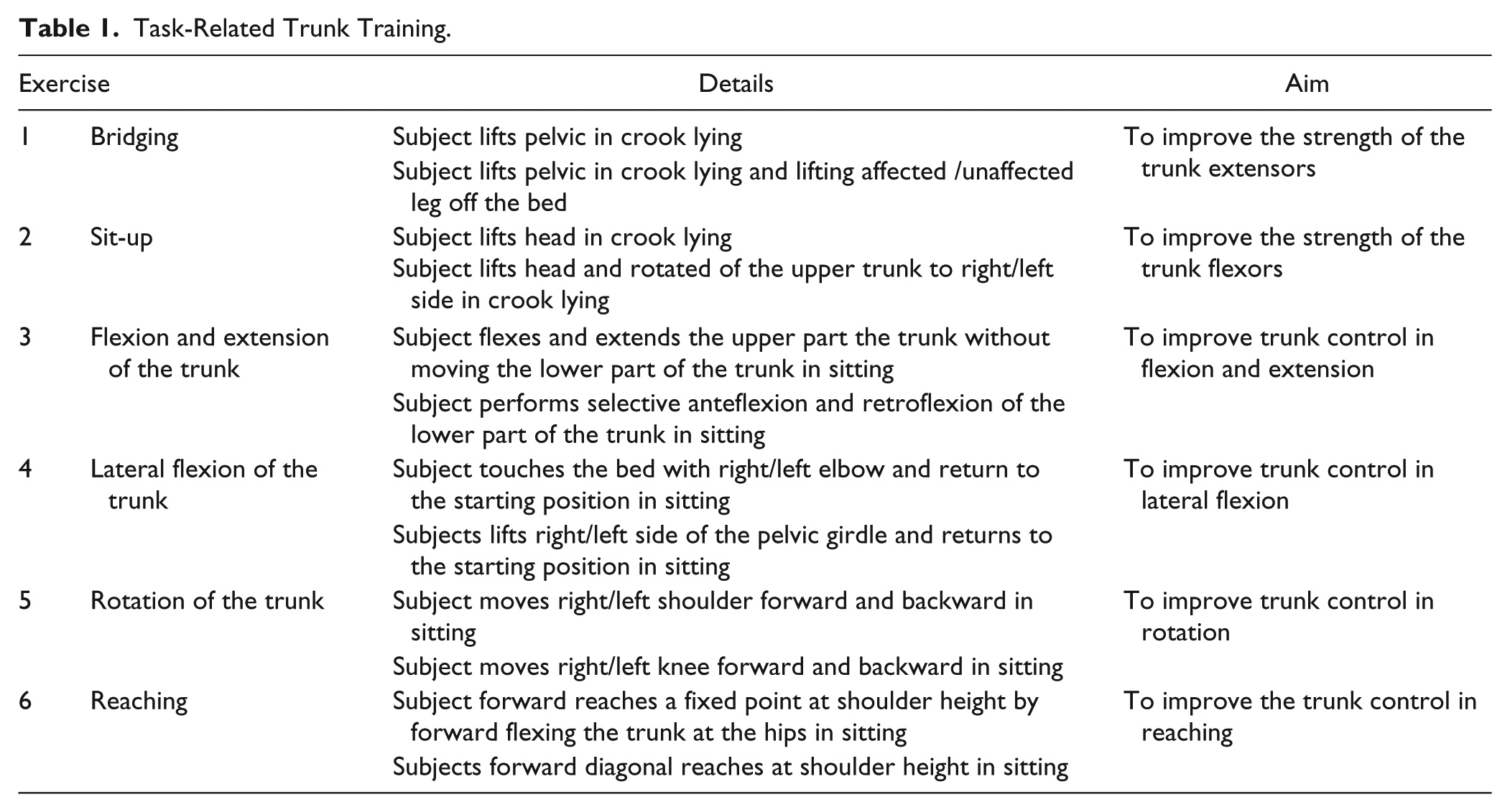
Task-related training is a rehabilitation strategy that involves practice of goal-directed, functional movements in a natural environment to help patients derive optimal control strategies for alleviating movement disorders. 23 The TRTT protocol was developed based on that used in previous studies which related to functional task.1-2 The components of the TRTT were grouped into 6 sets of exercises: (1) pelvic bridging, (2) sitting up, (3) trunk flexion and extension, (4) trunk lateral flexion, (5) trunk rotation, and (6) reaching. Each TRTT session consisted of 6 exercises with each taking 10 minutes to complete, for a total of 60 minutes. Table 1 describes the details and the aims of the exercises. The subject was allowed to rest if they felt tired during the training. The physical therapist applied standard progression of the exercises as the muscle strength of the subjects improved, increasing the number of repetitions, increasing the range of movement, adjusting the speed of movement and decreasing the rest time between exercises.
Task-Related Trunk Training.
The TENS + TRTT group received TENS simultaneously with the TRTT at home under the instruction of a physical therapist. Each subject in the TENS + TRTT and placebo-TENS + TRTT groups was provided with their own model ITO 120Z dual channel TENS stimulator. Pairs of electrodes were placed on the skin over the latissimus dorsi (lateral to T9 over the muscle belly) and the external abdominus obliquus (aligned 45° to the vertical, 15 cm lateral to the umbilicus, anterior to the axillary line) on the affected side. Those muscles were chosen because they are large, superficially located, and easily identified. Dickstein et al 11 reported that there was reduced and delayed in latissimus dorsi muscle activities in the affected side during trunk movement when compared with nonaffected side. Kafri and Dickstein 12 studied 17 subjects with stroke and reported that the external abdominus obliquus muscles activity of the affected side was reduced when move from supine to a side lying position when compared with normal subjects. High-frequency TENS (frequency 100 Hz; pulse width 0.2 ms) was used. The intensity of stimulation was set at twice the sensory threshold (the minimum intensity the subject could feel), which was barely below the motor threshold. The stimulation parameters were chosen based on the results of previous studies combining TENS with task-related training, which aimed at improving lower limb motor function after stroke.18,19
For the placebo stimulation, the electrical circuitry inside the TENS machine had been disconnected. An LED light blinked when the stimulator was switched on, but no electric current was delivered to the subject. The physical therapist told all subjects before the intervention that “You might or might not feel any sensation or muscle contraction during the stimulation.”
The intervention involved 5 training sessions per week for 6 weeks, for a total of 30 sessions. Within the 6-week intervention period the physical therapist conducted 6 home visits and 6 telephone follow-ups with each subject in all 3 study groups in order to ensure their treatment compliance. During each home visit the physical therapist checked whether the electrodes were being correctly applied over the different muscles, and recommended the progressions of the TRTT if necessary. The subjects were required to fill in an exercise log to record their daily exercise compliance, and this was checked by the physical therapist during the home visits. The subjects in the control group did not receive any active training except health education on measuring their blood pressure and monitoring the incidence of falls.
Outcome Measurements
All subjects were assessed by a research assistant who was blinded to their grouping. The subjects were assessed at baseline (A0), after 3 weeks (A1) and after 6 weeks of training (A2). They were then followed up 4 weeks after the intervention had ended (Afu).
The isometric peak trunk flexion torque and extension torque were measured using a Cybex NORM isokinetic dynamometer. This instrument has demonstrated good test–retest reliability for measuring peak torque in isometric trunk flexion (intraclass correlation coefficient [ICC] = 0.97) and extension (ICC = 0.93). 29 The subject was secured to the machine in a standing position as recommended by the manufacturer. The axis of rotation was set at the L5/S1 level. Vertical alignment was taken as the intersection of the mid-axillary line and L5/S1. The subject was asked to perform 3 trials of isometric trunk flexion and then isometric trunk extension in the neutral position, each involving 5 seconds of contraction with 60 seconds of rest between the recordings. Verbal encouragement (“harder and harder, and hold it” in Cantonese) was given to promote maximal contraction of the trunk muscles. The maximum value among the three readings was used in the statistical analysis.
Sitting functional reach 30 was also measured. This test has good test–retest reliability (ICC = 0.90-0.97), 31 interrater reliability (ICC = 0.98) 32 , and intrarater reliability. 32 The subject was seated with the hips, knees, and ankles positioned at 90° of flexion and the feet flat on the floor. Forward seated reaching distance was measured with the subject sitting with the unaffected side near a wall and reaching forward with the unaffected hand. The placement of the fifth finger of the unaffected hand was recorded with a tape measure in centimeters. Lateral seated reach distance was taken as the distance the acromion moved when the subject, seated with the back to the wall, reached to the unaffected and affected sides. The standardized verbal instruction (in Cantonese) was, “Keep your eyes looking forward, and reach out as far as you can.” After a practice trial, 3 measurements were performed with 15 seconds of rest between trials. The values of the 3 trials were averaged for analysis.
Trunk motor control was quantified using the TIS, 5 which has good interrater reliability (ICC = 0.85-0.99) 5 and internal consistency 5 (Cronbach’s α = .65-.89). Its construct validity has been demonstrated using Barthel index scores (r = .86) and trunk control test scores (r = .83). 6 The TIS is a 2-, 3- or 4-point ordinal scale, which evaluates static sitting balance, dynamic sitting balance, and coordination. The maximum scores on the static sitting balance, dynamic sitting balance, and coordination scales are 7, 10, and 6 points, respectively. The total score ranges between 0 and 23 points, with a higher score indicating better trunk control. The static sitting balance components evaluated whether a subject could keep a seated position with both feet on the floor and with the legs crossed compensating both passively and actively with the trunk. The dynamic sitting balance components evaluated the ability to perform selective lateral flexion initiating from the shoulder to the pelvic girdle and from the pelvic girdle to the shoulder. The coordination components evaluated the ability to selectively rotate the upper and lower parts of the trunk with normal timing and symmetry of trunk movement.
Statistical Analysis
The statistical tests were conducted with the help of version 17 of the Statistical Package for the Social Sciences. Descriptive statistics were computed for the relevant subject characteristics. A Kolmogorov–Simirnov test was used to test the normality of data. The intention-to-treat assumption was used in the data analysis. Any change in the outcome measures was quantified by subtracting the pretreatment scores from the posttreatment scores. Differences in each outcome measure from the baseline were analyzed with repeated-measures analysis of variance followed by post hoc tests with the significance level set at 5%. The between-subjects factor was the grouping, and the within-subject factor was the assessment time. All P values were corrected using Bonferonni’s adjustment to maintain the overall type I error at 5%.
Results
The 37 subjects included 27 males and 10 females with a mean age of 57.8 ± 9.4 years and an average time poststroke of 44.2 ± 28.3 months. Tables 2 and 3 present the full demographic data and motor function of the participants, respectively. There was no significant differences among 3 groups at baseline, including demographic data, mean isometric peak trunk flexion torque and extension torque, forward and lateral seated reaching distance, and TIS scores (Table 4). All the subjects completed at least 85% of the treatment protocol (≥26 hours of the training) according to the records in the exercise log books. Tables 5 and 6 compare the outcome measurements and TIS subscales, respectively, among the 3 groups.
Comparison of Subject Demographic Data of Subjects With Stroke Among 3 Intervention Groups.
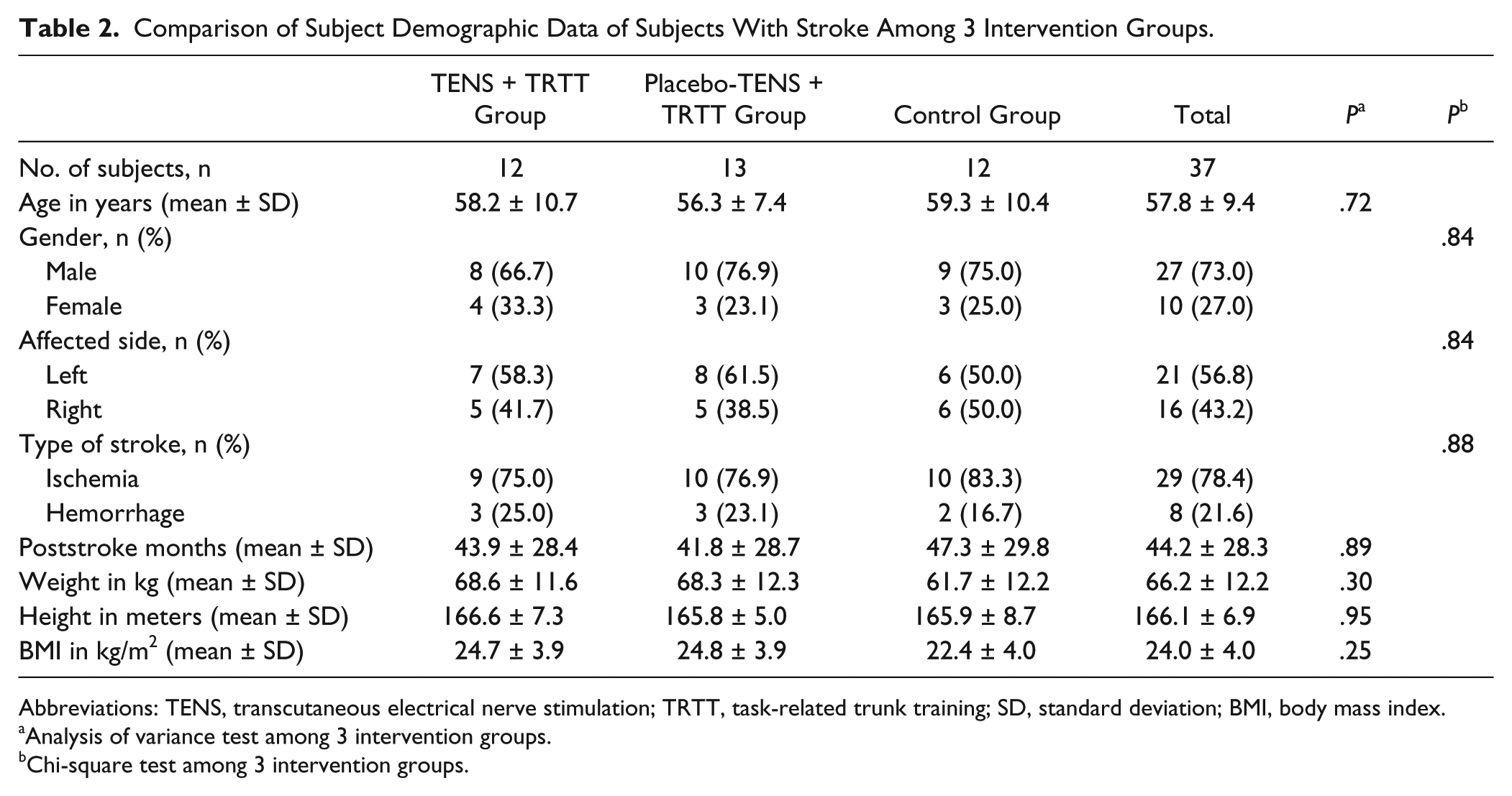
Abbreviations: TENS, transcutaneous electrical nerve stimulation; TRTT, task-related trunk training; SD, standard deviation; BMI, body mass index.
Analysis of variance test among 3 intervention groups.
Chi-square test among 3 intervention groups.
Motor Assessment Scale of the Subjects With Stroke Among 3 Intervention Groups. a
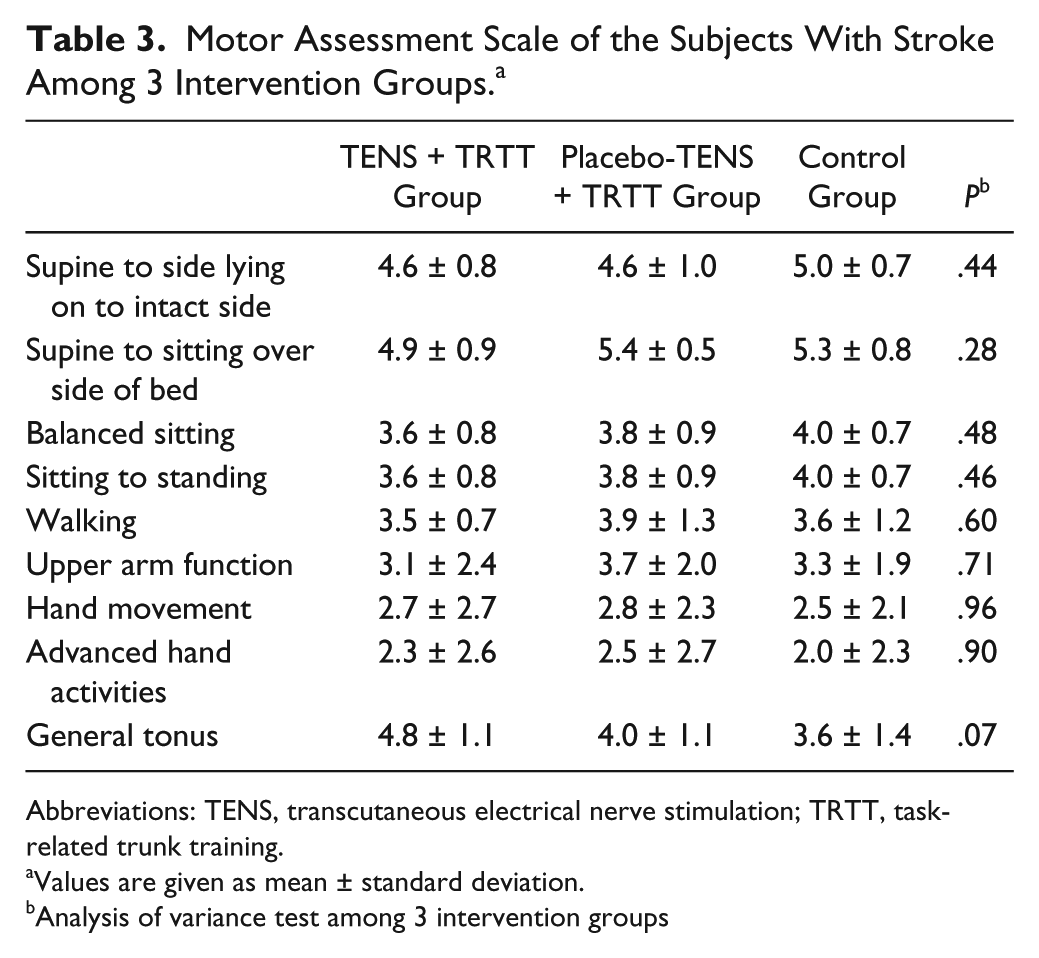
Abbreviations: TENS, transcutaneous electrical nerve stimulation; TRTT, task-related trunk training.
Values are given as mean ± standard deviation.
Analysis of variance test among 3 intervention groups
Baseline Characteristics of the Subjects With Stroke Among 3 Intervention Groups. a
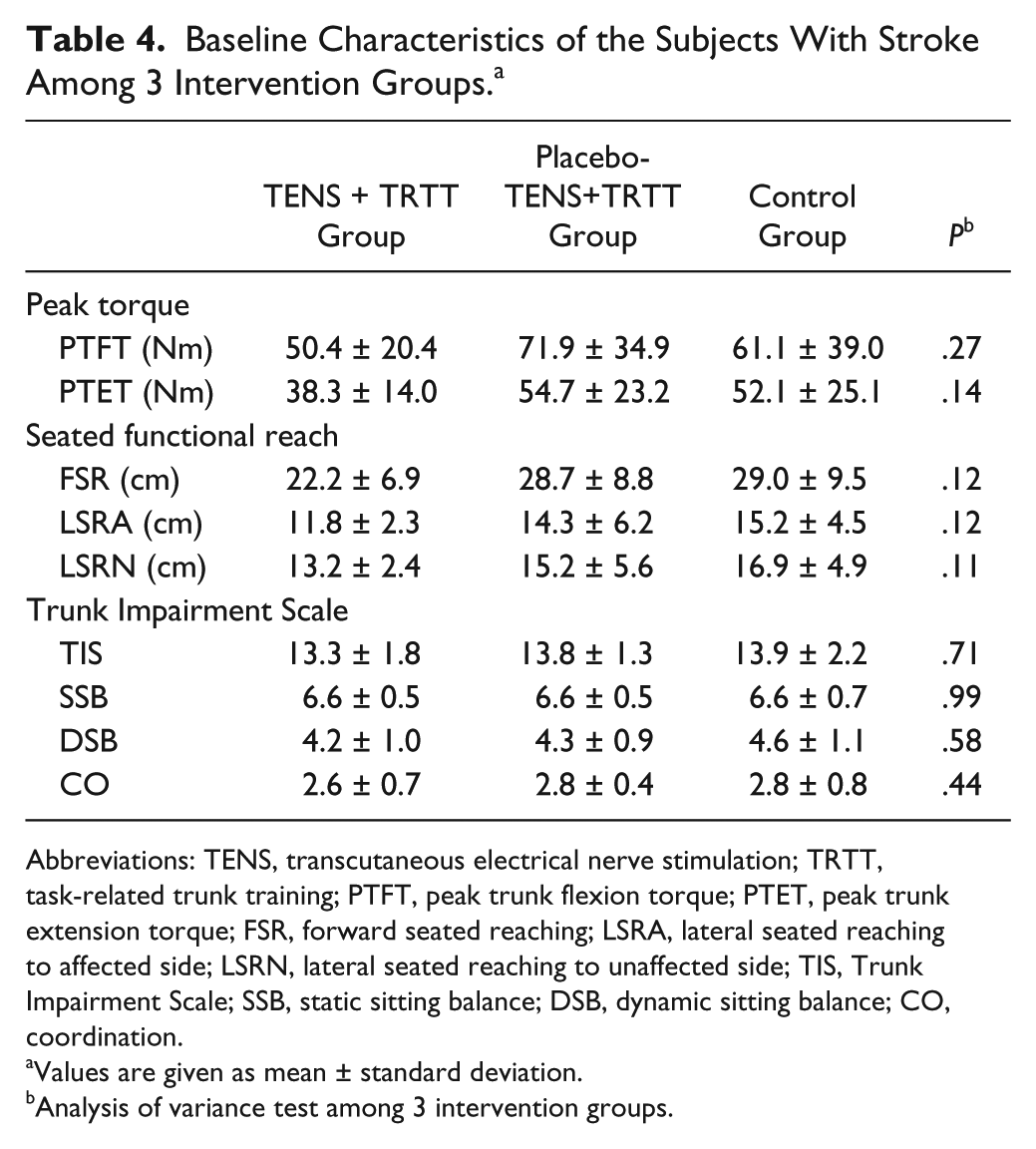
Abbreviations: TENS, transcutaneous electrical nerve stimulation; TRTT, task-related trunk training; PTFT, peak trunk flexion torque; PTET, peak trunk extension torque; FSR, forward seated reaching; LSRA, lateral seated reaching to affected side; LSRN, lateral seated reaching to unaffected side; TIS, Trunk Impairment Scale; SSB, static sitting balance; DSB, dynamic sitting balance; CO, coordination.
Values are given as mean ± standard deviation.
Analysis of variance test among 3 intervention groups.
Comparison of Outcome Measurements Among 3 Intervention Groups. a
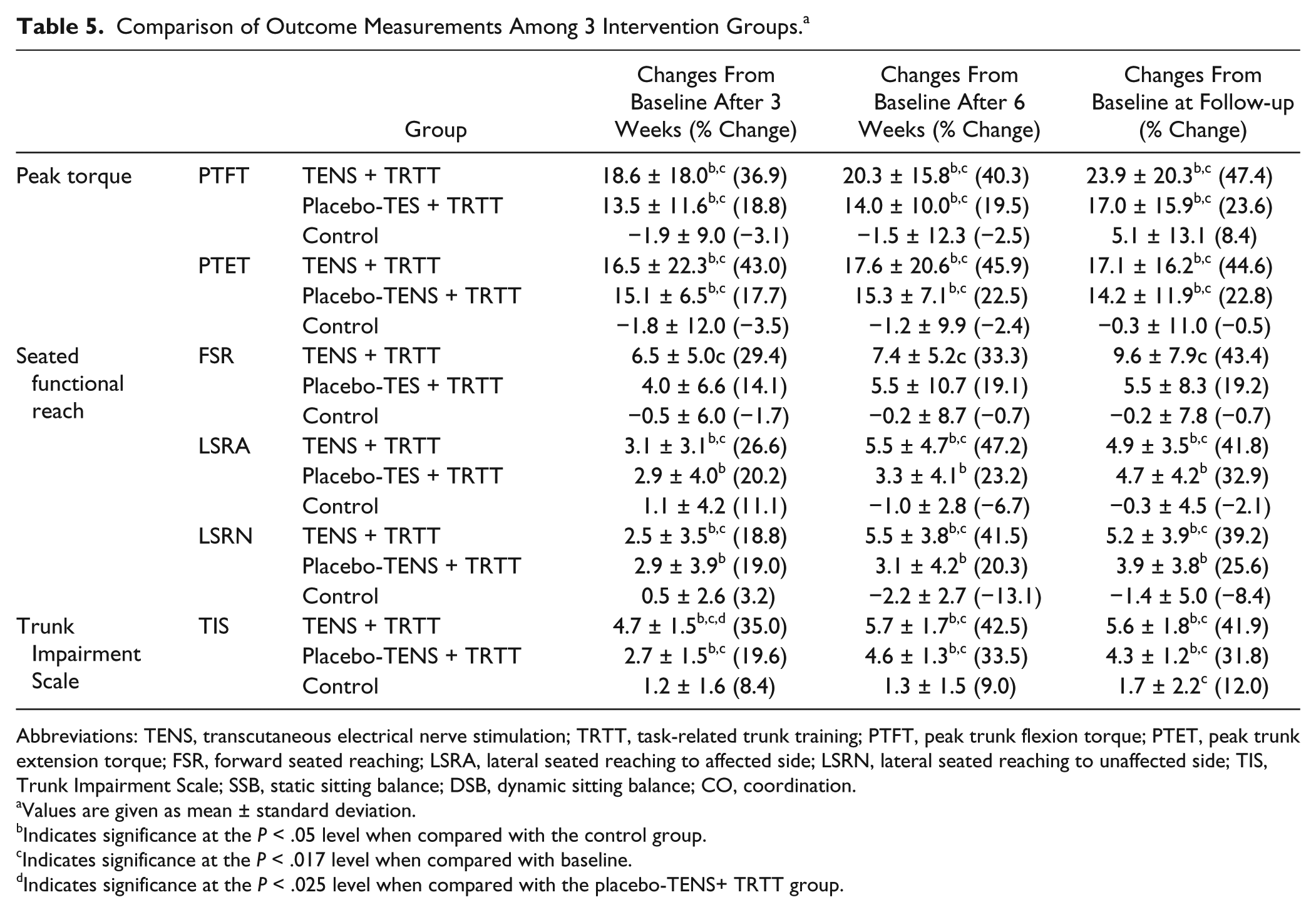
Abbreviations: TENS, transcutaneous electrical nerve stimulation; TRTT, task-related trunk training; PTFT, peak trunk flexion torque; PTET, peak trunk extension torque; FSR, forward seated reaching; LSRA, lateral seated reaching to affected side; LSRN, lateral seated reaching to unaffected side; TIS, Trunk Impairment Scale; SSB, static sitting balance; DSB, dynamic sitting balance; CO, coordination.
Values are given as mean ± standard deviation.
Indicates significance at the P < .05 level when compared with the control group.
Indicates significance at the P < .017 level when compared with baseline.
Indicates significance at the P < .025 level when compared with the placebo-TENS+ TRTT group.
Comparison of the Static Sitting Balance, Dynamic Sitting Balance, and Coordination Subscales of the Trunk Impairment Scale Among 3 Groups. a
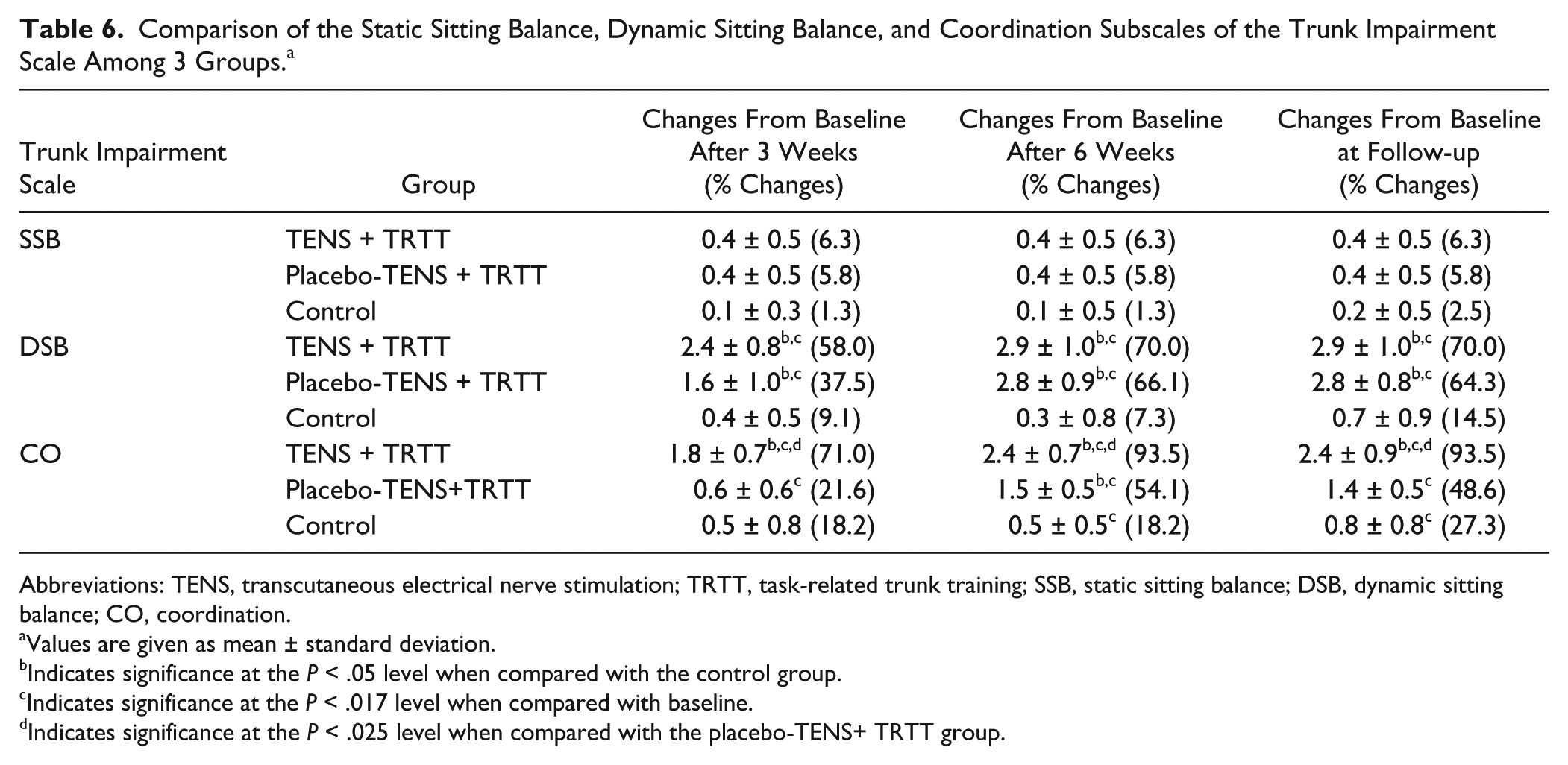
Abbreviations: TENS, transcutaneous electrical nerve stimulation; TRTT, task-related trunk training; SSB, static sitting balance; DSB, dynamic sitting balance; CO, coordination.
Values are given as mean ± standard deviation.
Indicates significance at the P < .05 level when compared with the control group.
Indicates significance at the P < .017 level when compared with baseline.
Indicates significance at the P < .025 level when compared with the placebo-TENS+ TRTT group.
Compared with the control group, both TRTT groups (with TENS or placebo-TENS) showed significantly greater improvements in their average isometric peak trunk flexion torque and extension torque, lateral seated reaching distance, and TIS scores at the A1, A2, and Afu time points (P ≤ .05). When compared with the placebo-TENS group, the TENS + TRTT group showed earlier and greater improvement in its mean TIS score at A1 (P ≤ .05), but not in the other outcomes.
When compared with the baseline values, both the TRTT groups (receiving TENS or placebo-TENS) showed significant improvements in their average isometric peak trunk flexion torque and extension torque and TIS scores at A1, A2, and Afu (P ≤ .05). However, only the TENS + TRTT group, not the placebo-TENS + TRTT group, showed significant improvements in forward and lateral seated reach distance and the TIS scores (P ≤ .05).
Post hoc calculations for the TIS subscales are presented in Table 5. When compared with the control group, neither TRTT group (receiving TENS or placebo-TENS) showed significant improvement in static sitting balance, but both showed significant improvement in dynamic sitting balance (P ≤ .05) at all time points. When compared with the control and placebo-TENS + TRTT groups, the TENS + TRTT group demonstrated significantly better coordination at all time points (P ≤ .05).
Discussion
These results confirm that TRTT can play a key role in improving isometric peak trunk torques, seated reaching distance and TIS scores. In addition, combining TENS with TRTT is generally more effective than TRTT alone for improving TIS scores. The added TENS appears to induce earlier and greater improvement in the TIS indicators.
The results of this study show that the TRTT protocol tested can be effective in improving trunk motor control. It provided sufficient stimulus to generate improvements in the stroke patients studied. The exercise program was designed according to the principles of specificity and repetition in training. It focused on the ability of the trunk muscles to hold the trunk upright, adjust to weight shifts, and perform controlled movements during certain functional tasks. Subjects in the present study practiced 30 hours of TRTT. Our training duration was substantially longer than previous studies where subjects practiced for only 10 to 12 hours.1,2 As the percentage of improvement in outcomes was greater after 6 weeks than after 3 weeks of training, longer duration (ie, 30 sessions) of TRTT probably provided sufficient training intensity and duration to improve muscle strength and enhance trunk motor control.
The mechanism by which TRTT improves muscle strength appears to be multifactorial. Enhancement of descending voluntary commands to paretic muscles, reorganization of synapses, and new cortical representation after repeated practice of functional tasks may all have played a part.33,34 Current research evidence supports the hypothesis that improvements in motor function following TRT are due, at least in part, to the neuroplasticity of the central nervous system following stroke.33,34 A study using functional magnetic resonance imaging has shown that improvements in hand function after 2 weeks of home-based rehabilitation exercises correlate with increased activity in the premotor cortex, the secondary somatosensory cortex contralateral to the affected hand, and the in superior posterior regions of the cerebellar hemispheres bilaterally. 33 Nelles et al 34 have reported that stroke survivors who had practiced task-related training had a larger bilateral activation area in the inferior parietal cortex, in the premotor areas and in the contralateral sensorimotor cortex than those without training. Since the TRTT involves bilateral movement, it is impossible to eliminate the possibility the noted improvement is due to improvements in the muscle strength of unaffected side. Further neurophysiological studies are warranted to identify the mechanisms underlying the motor improvements induced by TRTT in stroke survivors.
The present findings show that TRTT was effective in improving lateral reaching distance to both affected and unaffected side. Such improvements might be due to the specificity of the training in this TRTT program. 35 The newly gained reaching distance had been further incorporated into the subjects’ functional task-related activities in daily living. However, there was no significant improvement in forward reaching distance after TRTT training, even though previous studies have shown significant improvements.3,4 Such differences might be explained by different assessment methods and the different levels of functional ability of the subjects recruited. The subjects in this study used both hands in their reaching tasks, while subjects in previous studies used only their unaffected arm. In addition, the subjects in this study had impaired sitting balance, while the subjects in 1 previous study 4 could reach to 140% of their arm length with their unaffected arm.
The TENS + TRTT group showed earlier and greater improvement in its TIS scores starting at week 3, which was probably due to the changes in the coordination component of the TIS. TENS plays a major role in augmenting motor control of the selected shoulder and pelvis rotations, as well as in improving the symmetry of trunk movement. These findings are consistent with previous reports that TENS plus task-related training can augment lower limb motor function after stroke.18,19 Previous studies have revealed that the cortical pathways to trunk muscles are represented bilaterally while those to limb muscles are unilaterally represented in the cortical hemispheres.36,37 As the pattern of muscle weakness in the trunk might be different from that of the affected limb after stroke, the mechanism by which TENS increased the excitability of the sensorimotor cortex might be different in the trunk and the lower limbs. The neurophysiological mechanisms underlying improvement in trunk control following TENS is an area that warrants further study.
Our subjects with stroke practiced TRTT simultaneously with TENS stimulation. Khaslavskaia et al 16 have reported that repeated electrical stimulation over the common peroneal nerve could significantly increase motor evoked potentials of the tibialis anterior muscle elicited by focal magnetic stimulation of the motor cortex. We thus purported that our subjects could gain the most benefits when they practiced TRTT simultaneously with TENS stimulation.
The results show that combining TENS with TRTT was effective in improving trunk control even though there was no corresponding improvement in the peak torque generated by the trunk muscles or in the maximum seated reaching distance. This might be because of the nature of the TRTT employed. The exercises focused on trunk control and the coordination of muscle activation in task-related activities. The trunk muscles did not need to exert their maximum strength or generate maximal excursions. In addition, the fact that the TENS did not induce an enhanced increase in trunk muscle strength could be due to the ceiling effect in trunk muscle strength achieved by the TRTT alone.
The study protocol provides detailed guidelines for a 6-week, home-based rehabilitation program supported by a caregiver. All of the subjects completed more than 85% of the exercise program. Such high exercise compliance might have been due in part to the physical therapist’s surveillance, but it is probably important that the training was implemented in a home setting and that the subjects registered their compliance in an exercise log book, which also gave a record of progress.
There are several limitations of this study that should be acknowledged. It was impossible to blind the physical therapist to the application of TENS and TRTT. The therapists who delivered the intervention anticipated a treatment effect for the TENS. Indeed, even some subjects might have been aware of the hypothesis and the different interventions, which rendered a proper double-blinded, randomized, and controlled trial impossible. The physical therapist made more home visits to those in the TENS + TRTT and placebo-TENS + TRTT groups than to the control group, though the total number of home visits plus telephone follow-ups was the same. And TENS was applied only to the latissimus dorsi and the external abdominus obliquus because of the limited number of electrodes available. It is not clear whether stimulating other large muscles such as the erector spinae would yield similar results. Further study could validate the efficacy of targeting other trunk muscles and using other stimulation settings with stroke patients.
Conclusions
Home-based TRTT can improve trunk muscle strength, sitting functional reach and trunk control in subjects with chronic stroke, at least those without somatosensory deficits. The TRTT protocol tested can serve as a detailed guideline for a 6-week, home-based rehabilitation program aiming at enhancing the trunk muscle strength, sitting functional reach, and trunk control of stroke survivors. Applying TENS to trunk muscles can accelerate the benefits of exercise as measured by the TIS within the first 3 weeks of training.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.