
Abstract
Background. Thus far, most of the brain–computer interfaces (BCIs) developed for motor rehabilitation used electroencephalographic signals to drive prostheses that support upper limb movement. Only few BCIs used hemodynamic signals or were designed to control lower extremity prostheses. Recent technological developments indicate that functional near-infrared spectroscopy (fNIRS)-BCI can be exploited in rehabilitation of lower limb movement due to its great usability and reduced sensitivity to head motion artifacts. Objective. The aim of this proof of concept study was to assess whether hemodynamic signals underlying lower limb motor preparation in stroke patients can be reliably measured and classified. Methods. fNIRS data were acquired during preparation of left and right hip movement in 7 chronic stroke patients. Results. Single-trial analysis indicated that specific hemodynamic changes associated with left and right hip movement preparation can be measured with fNIRS. Linear discriminant analysis classification of totHB signal changes in the premotor cortex and/or posterior parietal cortex indicated above chance accuracy in discriminating paretic from nonparetic movement preparation trials in most of the tested patients. Conclusion. The results provide first evidence that fNIRS can detect brain activity associated with single-trial lower limb motor preparation in stroke patients. These findings encourage further investigation of fNIRS suitability for BCI applications in rehabilitation of patients with lower limb motor impairment after stroke.
Introduction
Reduced gait performance is a common residual deficit in hemiplegic patients after stroke. The recovery of walking ability is generally observed in only 50% to 60% of patients. At the time of discharge from rehabilitation and therapy clinics, approximately 5% of patients are independent in stair climbing; 9% and 14% are able to walk outside and inside, respectively; 27% to walk with cane or other aid; and 45% remain in a wheelchair. Although some patients can walk independently, their gait disturbance limits performance of daily activities and makes them more susceptible to injury. 1
None of the existing gait rehabilitation techniques based on physiotherapy treatments has shown convincing evidence of effective recovery of lower limb functions in chronic patients after stroke. Top-down strategies using brain–computer interfaces (BCIs) that use neurophysiologic or metabolic brain activity to drive external devices may represent a promising approach to modulate brain reorganization and motor behavior in stroke survivors.2-5 BCI training is anticipated to induce brain plasticity and recovery by providing contingent afferent feedback to sensorimotor cortex. Good recovery is often associated with returning activity to the cortical areas near the lesion, 6 and the stimulation and reinforcement of activity in the perilesional areas through BCI training demonstrated beneficial effects for motor rehabilitation after stroke.7-9
Most of the BCIs developed for motor rehabilitation used electroencephalographic signals to drive prostheses that support upper limbs movements. However, only few BCIs used hemodynamic signals or were designed to control lower extremity prostheses.10,11 Yet recent technological developments indicate that functional near-infrared spectroscopy (fNIRS)-BCIs can be exploited in the rehabilitation of lower limb movement due to their great usability and reduced sensitivity to head motion artifacts. 2
The aim of this proof of concept study was to assess to what extent fNIRS signals associated with lower limbs motor preparation can be reliably measured and classified and thus used for future applications of fNIRS-BCI in rehabilitation of lower limb movement.
Until now, BCIs have largely used the neurophysiologic brain signals associated with motor imagery, as consistent evidence has been provided in favor of close similarities between the overt and covert motor activity (motor imagery).12,13 However, motor imagery vividness can vary substantially among healthy individuals as well as in patients after stroke. In particular, motor imagery vividness of the affected side is reduced in patients with stroke. 14
The use of motor preparation and intention for BCI control is more ecological and motivating, as patients are encouraged to prepare and attempt to execute a real movement.2,3,15 This strategy could then represent an added value to promote functional recovery.
In this pilot study on chronic stroke patients, fNIRS signals were acquired during preparation of hip movement, a motor act critical for balance and posture retention during standing and walking. Based on prior literature on motor preparation and intention,16-20 frontal premotor and posterior parietal activations were expected to be detected by fNIRS on a single-trial level. Sensitivity to lower limb motor preparation activity was further explored using single-trial linear discriminant analysis (LDA)–based classification of hemodynamic signals.
Methods
Patients
Seven right-handed chronic stroke patients participated in the study (mean age = 54.7 ± 14.10; 3 females). All participants suffered from severe hemiparesis as result of a single unilateral cerebrovascular incident. The following criteria were adopted to include patients with stroke: (a) interval since stroke at least 12 months, (b) no psychiatric or neurological condition other than stroke, (c) no cerebellar lesion or bilateral motor deficit, and (d) ability to understand and follow instructions (S1). Patients’ functional mobility was assessed with the Timed Up and Go (TUG) 21 (see Supplementary Material). All recruited patients have no severe stenosis of carotid or intracranial major vessels including middle and anterior cerebral arteries. The study was approved by the ethics committee of the Faculty of Medicine of the University of Tübingen (Germany), and all procedures were in accordance with the declaration of Helsinki in its latest revision.
Task
The paradigm consisted of 2 sessions of 11 “left hip” (9 seconds, 10 seconds, 11 seconds) and 11 “right hip” movement preparation (9 seconds, 10 seconds, 11 seconds) followed by movement execution (3 seconds) either of left or right hip and interspersed with 23 periods of rest (15 seconds, 20 seconds, 25 seconds) presented in a pseudo-randomized order (Figure 1A). Random selection of duration of preparation and rest condition as well the inclusion of shorter preparation trials (1 second, 3 seconds, 6 seconds) aimed to reduce task predictability and habituation. Participants, sitting on a chair, used a mechanical device (pedals) that permitted to perform hip movements while constraining knee and ankle movements (Figure 1B). Participants were visually cued for left and right hip preparation and execution (Figure 1A).
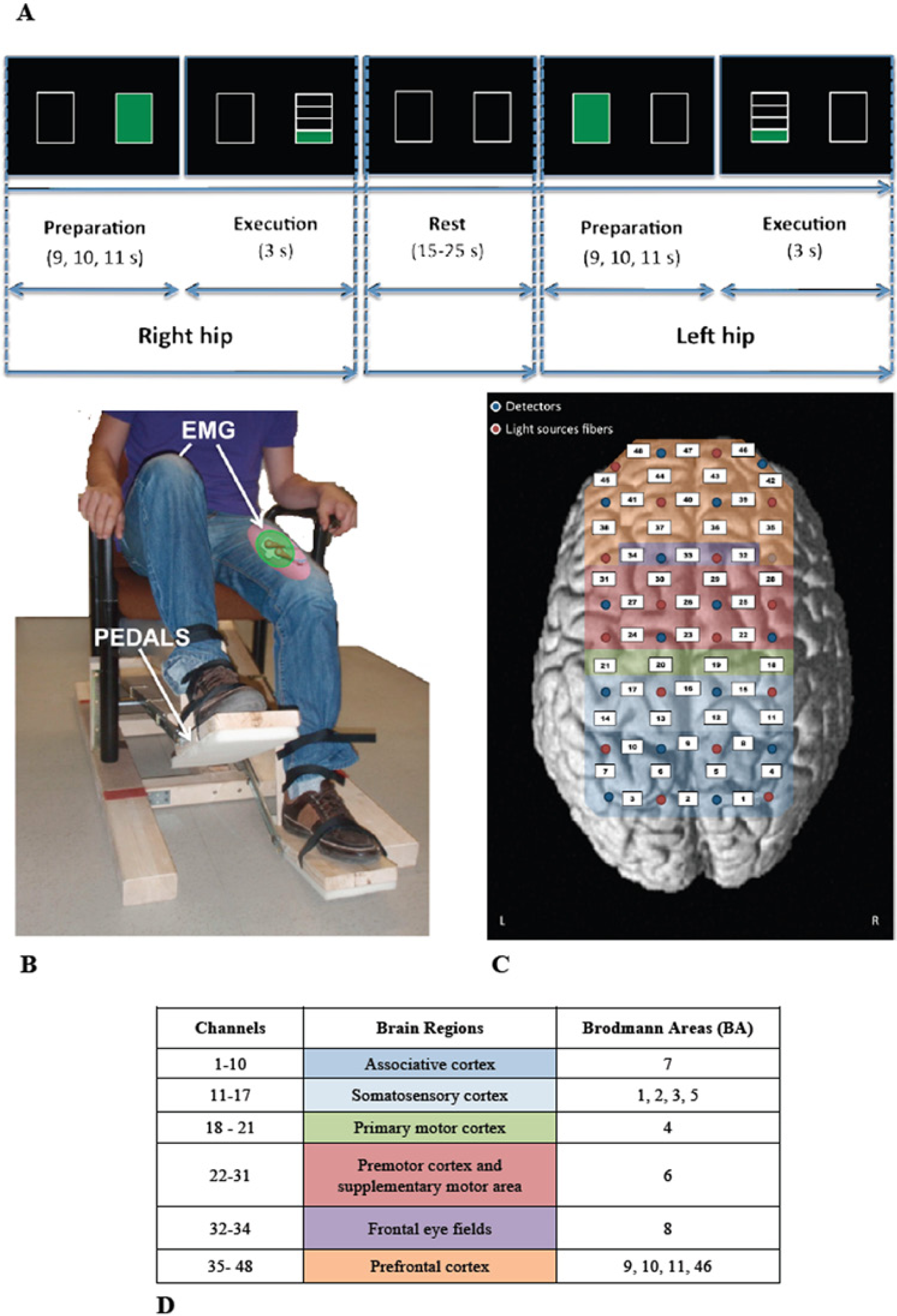
Experimental setup.
fNIRS Data Acquisition
A 48-channels ETG-4000 (Hitachi Medical Systems GmbH, Tokyo, Japan) with continuous wave laser diodes with wavelengths of 695 nm and 830 nm and sampling rate of 10 Hz was used. The optodes were applied sagittally covering the frontal regions, bilateral premotor cortex (PMC), supplementary motor area (SMA), primary and secondary motor areas, and somatosensory areas (Figure 1C and D). Based on the International 10-20 System for EEG electrode placement, Cz was used as a reference point for positioning the optodes. fNIRS channels were defined as the midpoint of the corresponding light source-detector pair (Figure 1C and D). The fixed inter-optodes distance is 3 cm. At this typical source–detector separation,22,23 the contribution of the gray matter to the light absorption has been estimated in the order of 20% to 30%. 24 The positions of the optodes were marked by means of a 3D digitizer in all patients (Fastrack; Polhemus Inc, Colchester, VT). For coregistration purposes a T1-weighted anatomical magnetic resonance (MR) image was acquired of each patient using a 3 T Siemens magnetic resonance imaging system (Siemens TIM Trio, Erlangen, Germany) with a 1 mm isotropic MPRAGE sequence and the following parameters: TR = 2300 ms; TE = 3.03 ms; TI = 1100 ms; flip angle = 8°; FOV = 256 × 256; matrix size = 256 × 256; number of slices = 176; slice thickness = 1 mm, bandwidth = 130 Hz/Px. Spatial registration of channel locations was performed using Statistical Parametric Mapping software package (NIRS-SPM; SPM5; Welcome Trust Centre for Neuroimaging, London, UK). NIRS channel positions in real coordinates obtained from a 3D digitizer were projected onto the cortex of the anatomical MR image of the 7 patients using Horn’s algorithm. 25 The cortical regions and Brodmann’s areas (BA) corresponding to each channel were defined using Automated Anatomical Labeling (AAL) available on the MRIcron software26-29 (Figure 1C and D).
EMG Data Acquisition
Electromyography (EMG) activity was recorded using a BrainVision QuickAmp amplifier (Brain Products GmbH) from 2 active electrodes on 5 patients. Bipolar EMG electrodes were placed along muscle fibers of femoris quadriceps muscle/sartorius muscle of both legs (Figure 1B) according to SENIAM recommendations. 30 Electrode impedances were kept below 5 kΩ by careful skin abrasion. We applied standard preprocessing for surface EMG with a band pass filter 10 to 400 Hz and notch filter 50 Hz. 30 The reference electrode was placed over the clavicula.
fNIRS Data Analysis
Previous studies suggested that the fNIRS signal could be contaminated by extra brain components such as skin blood flow effect and systemic physiological fluctuations. 31 This is an important general issue that until now has not been resolved. There exist no reliable signal filtering techniques to reduce a task-evoked intrinsic contaminant. Moreover, no reliable methods permit to separate the observed signal into the cerebral functional signal and other physiological fluctuations especially when there is a correlation between these components. Very recently, a novel method for separating functional and systemic signals based on their hemodynamic differences has been proposed for healthy subjects. 32 The authors assumed that cerebral functional hemodynamics in the capillaries of the local cerebral region and a systemic fluctuation in other vessels of the other tissues are characterized by their linear negative and positive correlation between oxy- and deoxyhemoglobin changes, respectively. They then provided an empirical procedure to determine the coefficients of the linear relationship between the oxy- and deoxyhemoglobin changes of the two modalities, which were used to separate functional and systemic signals. However, the computation of the coefficients is based on temporal stability of the hemodynamic modalities, and this assumption might not be appropriate in the case of patients with neurovascular alteration after stroke.
A recent study has shown that totHb signal provides better spatial specificity in cerebral activity mapping, as its variations are much less sensitive to pial vein contamination. 33
In the present study, the above-mentioned issues were addressed using the following data preprocessing and analysis. fNIRS data were preprocessed and analyzed using Statistical Parametric Mapping software package (NIRS-SPM, SPM5; Welcome Trust Centre for Neuroimaging). Statistical analyses of NIRS data are based on a mass-univariate approach derived from the general liner model (GLM). A GLM model was generated using standard hemodynamic response function (HRF) as basis function.
Data were filtered using the wavelet-minimum description length (MDL) algorithm for removing unknown global trend due to breathing, cardiac, vasomotion, and experimental noise. 34 This preprocessing step, by decomposing NIRS measurements into global trends, hemodynamic signals and uncorrelated noise, enables to reduce spurious components, though it has limited efficacy in reducing task-evoked intrinsic contaminant such as skin blood flow effect. 31 A gaussian low-pass filter with 4-second full-width-half-maximum (FWHM) was used to estimate and remove temporal autocorrelation.
The concentration changes of oxyhemoglobin (oxyHb) and deoxyhemoglobin (deoxyHb) and total hemoglobin (totHb), calculated from optical density changes, were obtained using the modified Beer–Lambert law. 35
To minimize the effect of contamination of subsequent movement execution on the hemodynamic response of preparation condition only motor preparation trials with duration of 9 seconds, 10 seconds, and 11 seconds were considered (73% of all trials).
Cortical activations related to hip movement preparation were obtained at single-patient level by separately comparing left and right hip movement preparation to rest. Single patient parametric maps were thresholded using a significance level of P < .01 corrected for multiple comparisons using Sun’s tube formula. 36 First-level contrast images relative to totHb only 33 were also entered into a second-level (random-effects) group analysis. Only stroke patients with lesions in the right hemisphere (6 out of 7) were included in the second-level random-effect analysis to avoid miscoregistration due to image flipping. The resulting parametric maps were thresholded using a significance level of P < 0.01 uncorrected due to small sample size and also because specific activations in premotor and parietal cortices were expected.
Selection of channels in the corresponding regions of interest in the hemisphere contralateral to the prepared movement was then performed anatomically and functionally, based on single-patient parametric t-maps of totHb (highest t-value) resulting from the comparisons of paretic and nonparetic hip movement preparation with respect to rest. Time-series of oxyHb, deoxyHb, and totHb changes for each trial were extracted from selected channels corresponding to PMC and PPC on each patient. Subsequently, totHb signal of each movement preparation trial (9 seconds, 10 seconds, 11 seconds) was segmented into 1-second blocks; the mean of 10 data points per block (10 Hz) was calculated for each channel in the selected regions of the hemisphere contralateral to the prepared movement, and in the corresponding channels in the ipsilateral hemisphere. Offline classification using LDA with linear kernel was then performed to discriminate paretic hip movement preparation trials with respect to nonparetic hip movements preparation trials. 37 Discrimination of left versus right movement preparation trials was considered instead of movement preparation versus rest as during gait left and right lower limbs movements are alternated in a continuous fashion.
Mean changes of totHb concentration in PMC and PPC in both hemispheres were used as discriminatory feature13,38 for classification.13,37 Only totHb signal changes were considered as feature of interest as changes of oxyHb signal are more sensitive to noise and artefacts. 33 Data samples of each patient were split into a two thirds training set to develop the patient-dependent classifier and a one third testing set to test its performance. 39
EMG Data Analysis
As for fNIRS analysis only trials with a preparation phase of 9 seconds, 10 seconds, and 11 seconds were considered. These trials were full-wave rectified and low-pass filtered at 10 Hz in Brain Vision Analyzer (Version 1.04; Brain Products GmbH, Munich, Germany), normalized with respect to maximal activation during movement and offline segmented into 12-second epochs, including 9 seconds of movement preparation (back-averaging with a start point from the movement trigger) and 3 seconds of movement execution (averaging with a start point from the movement trigger). EMG activity of each hemisphere was then expressed as a percentage of the maximal value of motor execution. A threshold of 30% was used to define the EMG activity as tonic activity. This threshold had the only purpose of discriminating voluntary from nonvoluntary activity (ie, to detect the onset of the movement). This moment can be clearly distinguished by the sudden increase in RMS value during movement performance (see Figure 4).
Results
Group analysis of paretic hip movement preparation showed extended bilateral activations—increased totHb—in SMA, premotor cortex, sensorimotor regions, and frontal areas, with a maximum peak in the ipsilesional premotor area, contralateral to the movement (Figure 2). Group analysis of nonparetic hip movement preparation showed more focal totHb changes with clusters in the PMC and PPC bilaterally, and with a maximum peak in the contralateral PMC (Figure 2). No significant changes of deoxyHb were measured during both paretic and nonparetic hip movement preparation.
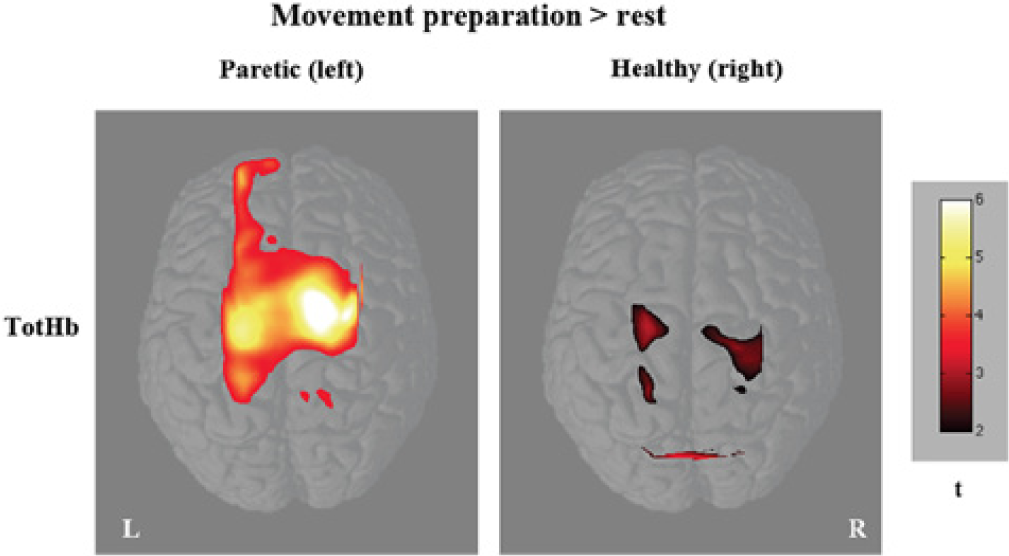
Maps of changes of totHb during paretic and nonparetic hip movement preparation trials threshold at P < .01 uncorrected.
Individual cortical activation patterns of oxyHb and totHb changes are reported in Figure 3. Despite interpatients variability, common activations in the contralateral PMC and PPC were generally observed during movement preparation in all patients (Figure 3) and, more important, in the ipsilesional hemisphere during movement preparation of the paretic limb.
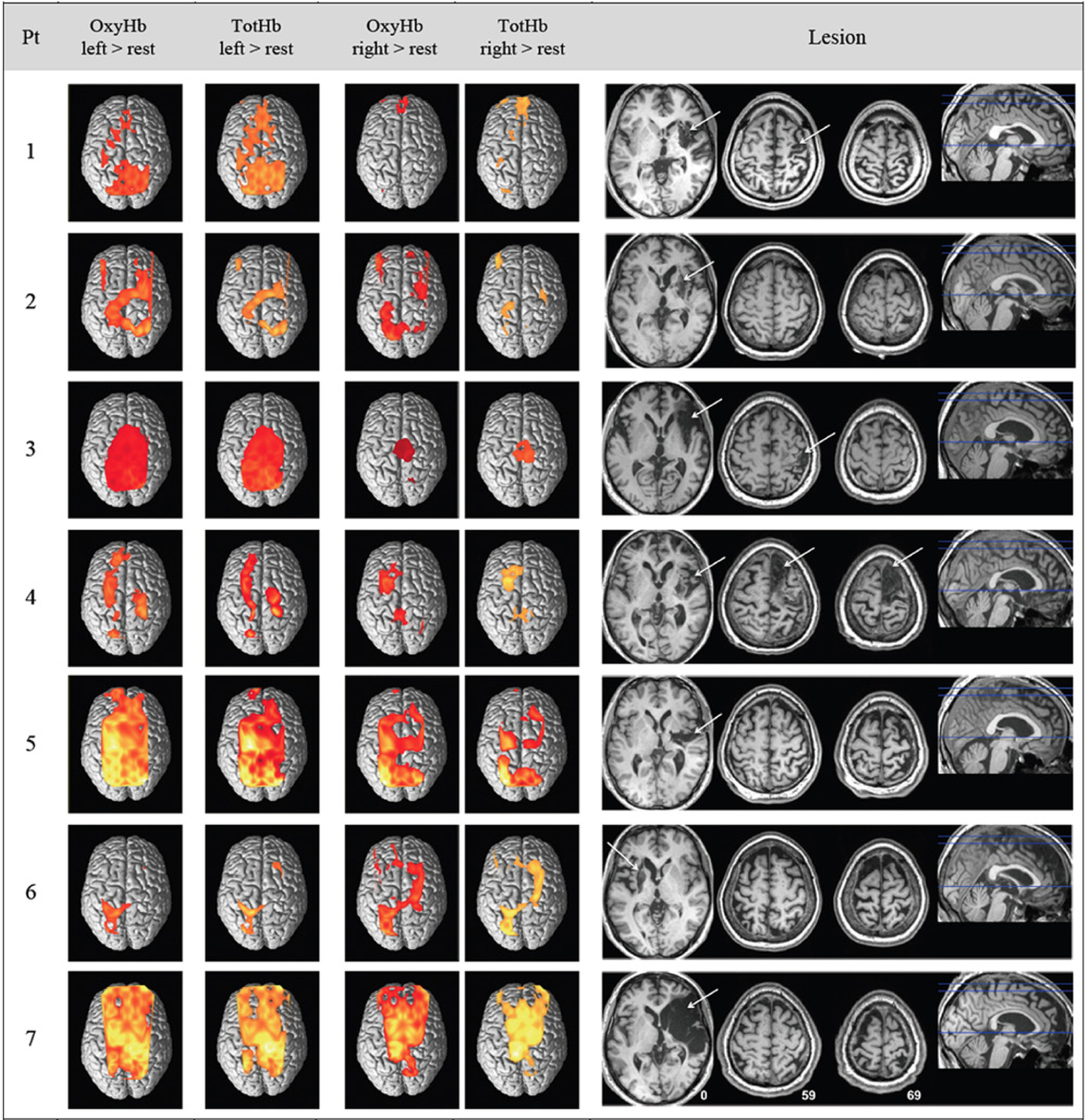
Single patients maps of changes in oxyHb and totHb of paretic and nonparetic hip movement preparation thresholded at P < .01 corrected for multiple comparisons using Sun’s tube formula. 36 On the right side are shown axial views of T1-weighted anatomical images at coordinates z = 0, 59, 69.
EMG analysis revealed only tonic activity during movement preparation trials (Figure 4). In the remaining 2 patients, in whom EMG was not acquired, visual inspection ensured no lower limb movements during motor preparation.
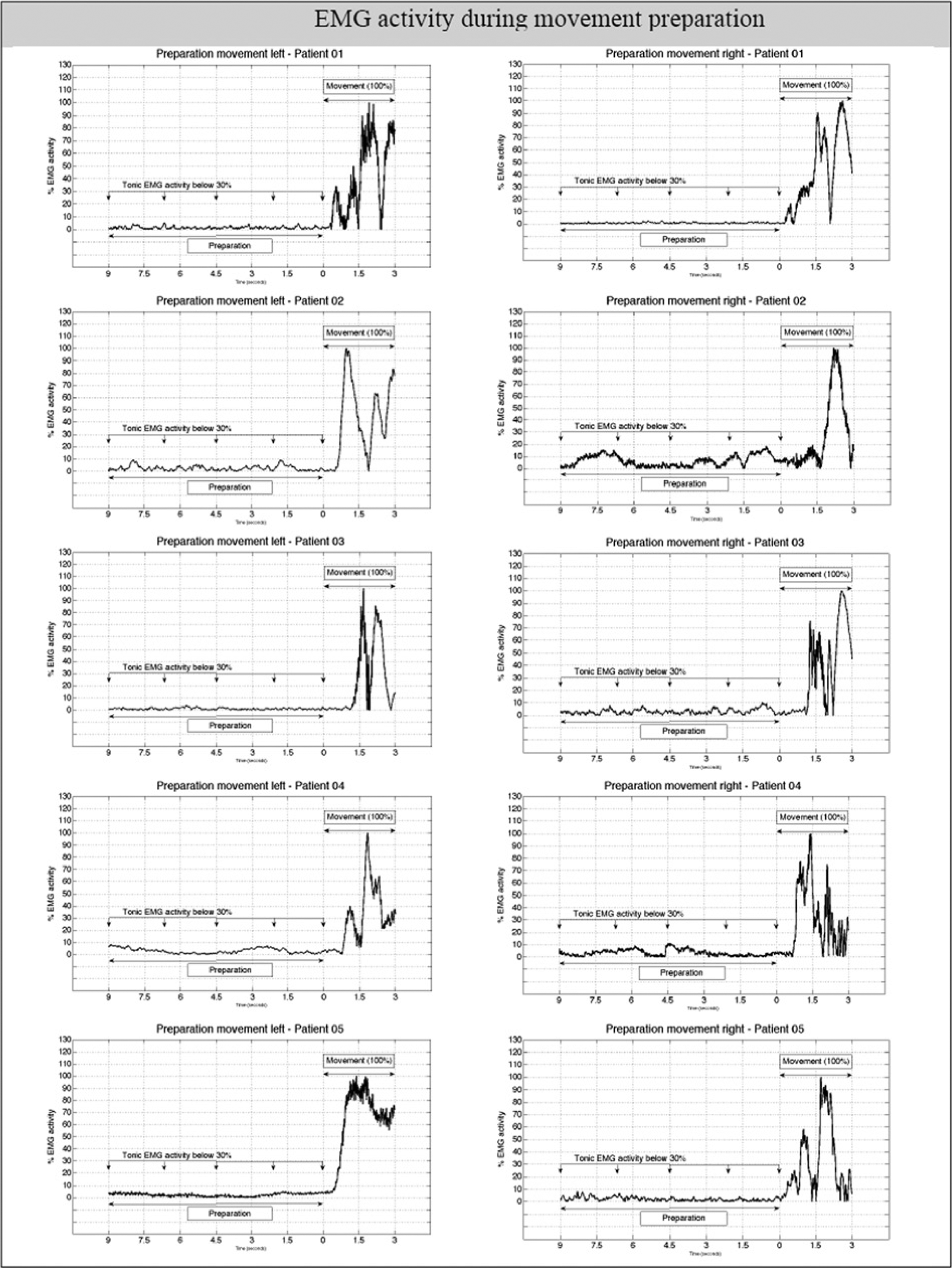
EMG activity during paretic and nonparetic hip movement preparation trials.
Time-series of averaged oxyHb, deoxyHb, and totHb changes, in the selected channels corresponding to PMC and PPC contralateral to the movement preparation, of each patient along with t values relative to changes of totHb in these channels are shown in Figure 5. Significant increases of oxyHb and totHb during paretic and nonparetic hip movement preparation in the contralateral PMC and PPC were observed. No significant changes of deoxyHb were observed during both conditions in contralateral and ipsilateral hemispheres.
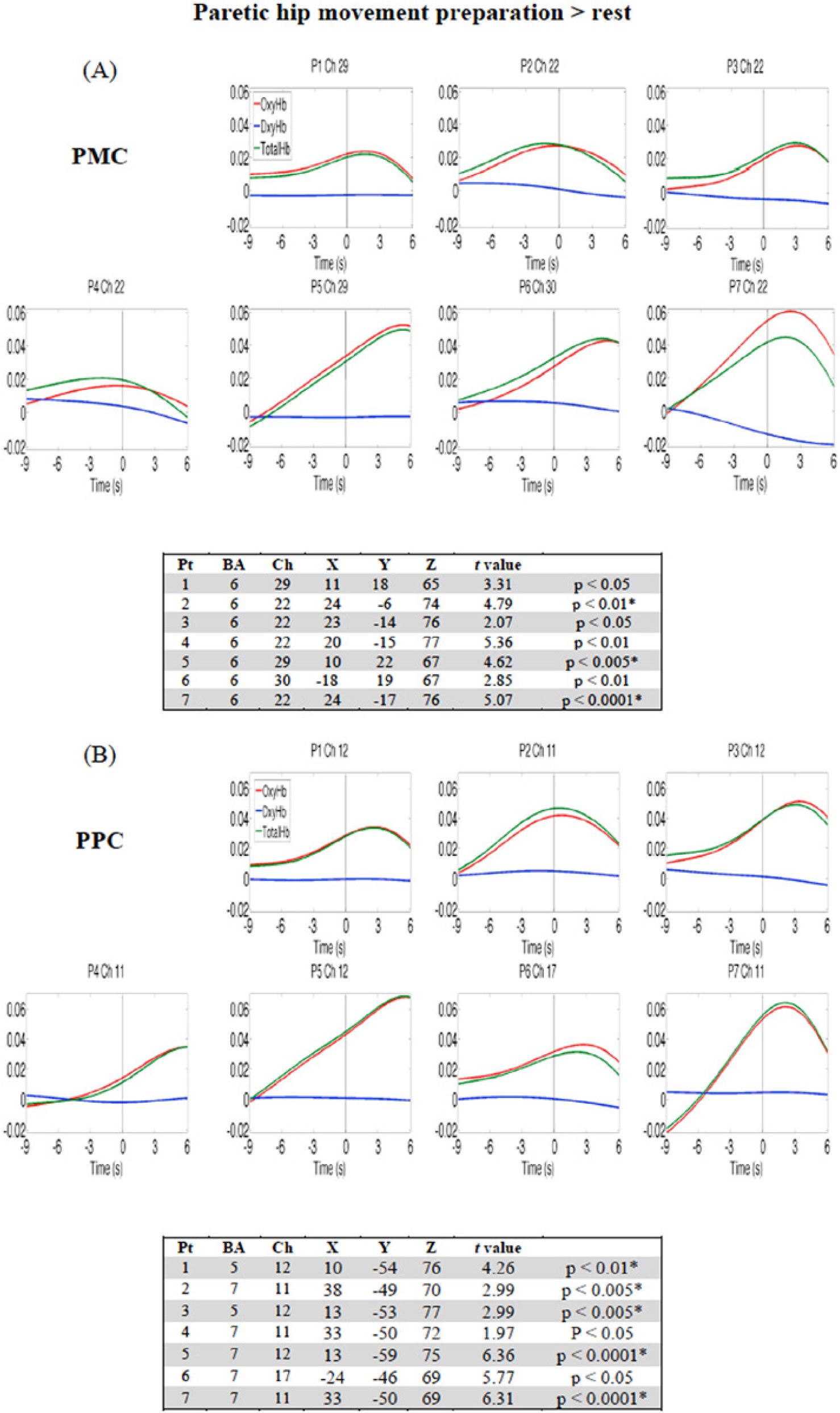
Average time-course of totHb (green), oxyHb (red), deoxyHb (blue) during paretic hip movement preparation > rest in the contralateral (ipsilesional) PMC (A) and PPC (B).
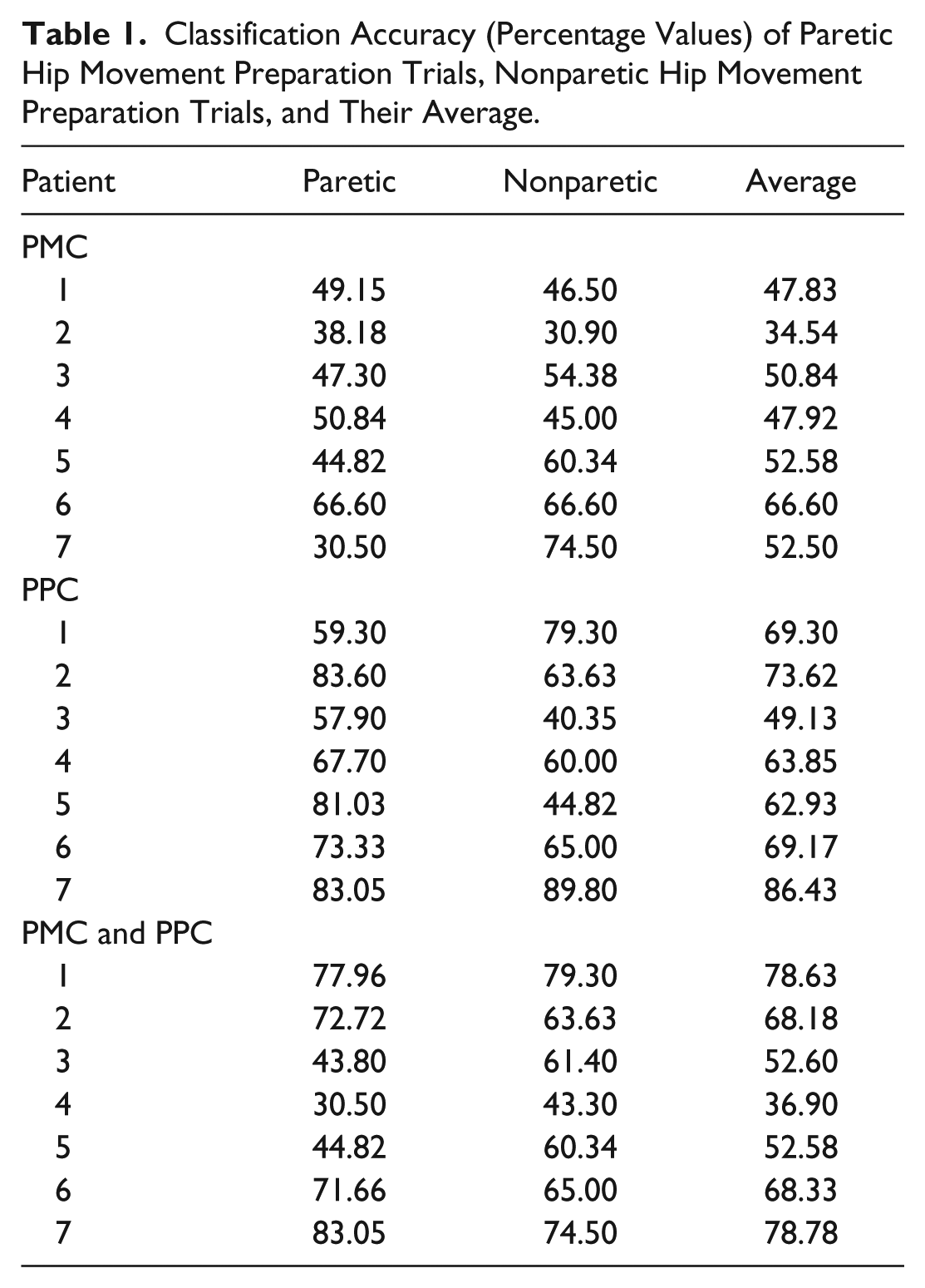
The average performance of LDA classifier when PPC channels were used as discriminant features of paretic versus nonparetic hip movement preparation trials reached 67.77 ± 11.35% accuracy (mean ± SD, t = 15.79, P < .0001; paretic = 72.27 ± 10.94%, nonparetic = 63.27 ± 17.51%); using PMC channels classification accuracy was 50.40 ± 9.45% (t = 14.10, P < .0001; paretic = 46.77 ± 11.24%, nonparetic = 54.03 ± 14.66%), whereas using combined PPC and PMC channels classification accuracy was 62.28 ± 15.51% (t = 10.63, P < .0001; paretic = 60.64 ± 20.46%, nonparetic = 63.92 ± 11.50%; see Figure 6 and Table 1). Classifier performance using PPC channels was significantly higher than using PMC only (paired t-test: t = 3.01, P = .024), but not using combined PMC and PPC channels (t = 1.25, P = .258). Average accuracy between paretic and nonparetic preparation trials was above chance in 6 out of 7 patients using either PPC channels or combined PMC and PPC channels; however, the number of subjects showing above chance accuracy of paretic and nonparetic preparation trials separately was lower considering combined PMC and PPC channels (Table 1).
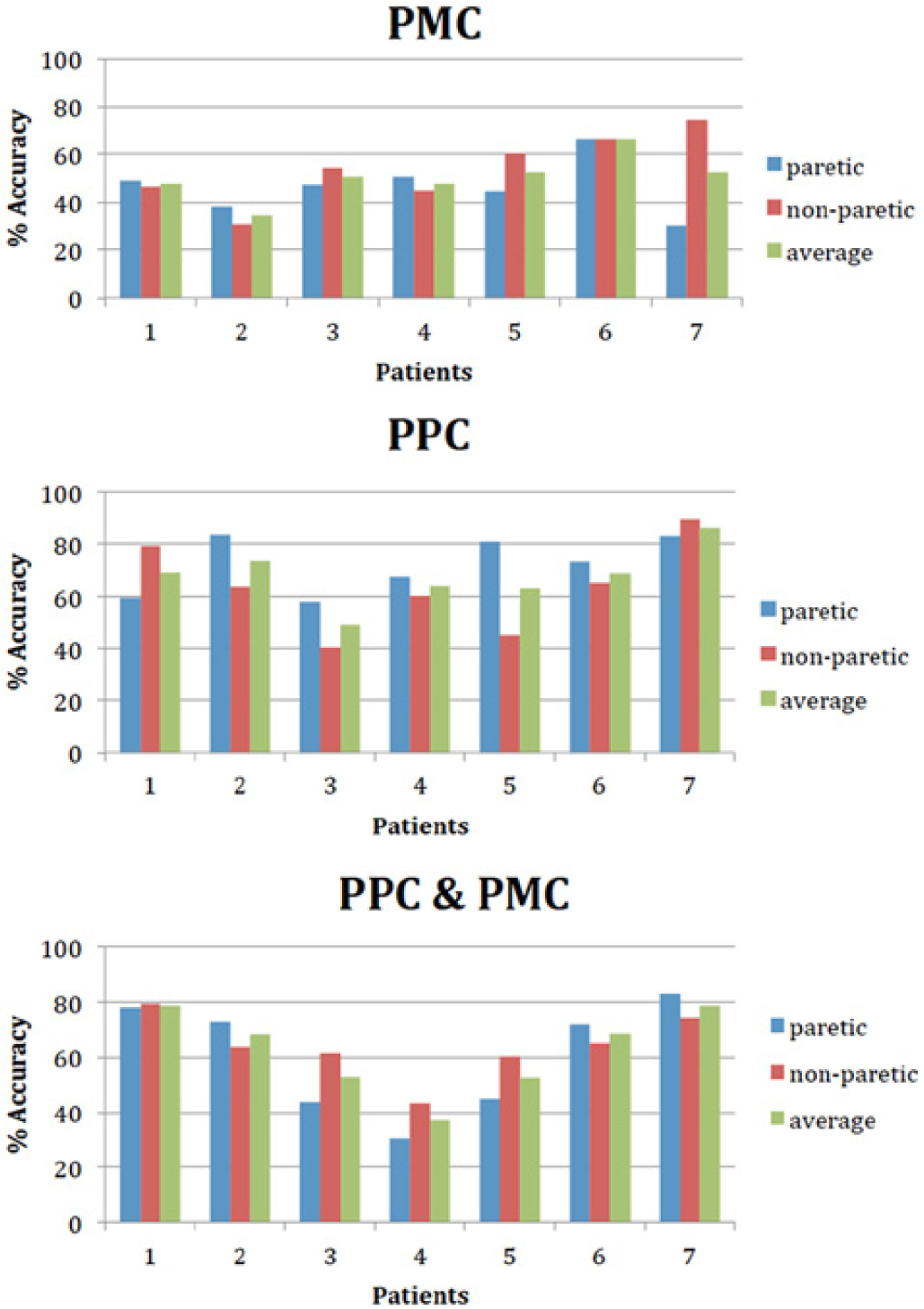
Percentage accuracy of LDA classification discriminating paretic hip movement preparation trials with respect to nonparetic hip movement preparation trials based on totHb signal changes in bilateral PMC, PPC, and combined PPC and PMC across patients.
Classification Accuracy (Percentage Values) of Paretic Hip Movement Preparation Trials, Nonparetic Hip Movement Preparation Trials, and Their Average.
Discussion
The present proof of concept study investigated the possibility to detect and classify hemodynamic signals associated with preparation of lower limb movements to assess the feasibility of an fNIRS-BCI for gait rehabilitation. Results of group and single-patient analyses during movement preparation of the paretic limb showed totHb changes in the ipsilesional premotor and sensorimotor regions contralateral to the prepared movement, as well as involvement of contralesional/ipsilateral regions. Preparation of movements with nonparetic lower limb showed as well recruitment of PMC and PPC bilaterally on single patients; at group level totHb changes were more focal and less spread. Bilateral sensorimotor activations during unilateral foot movement have been previously reported in fNIRS and magnetoencephalograpy studies in healthy participants.40,41
In patients with stroke the type of lesion (eg, cortical, subcortical, etc) might substantially affect brain reorganization and the balance of cortical activations. In a study with relatively small number of patients (n = 8), larger cortical lesions have been associated with increased cortical activation in the contralesional hemisphere during walking, whereas small subcortical lesions were associated with increased involvement of the ipsilesional hemisphere. 42 However, cortical activations during walking reflect movements of several segments of lower limbs, whereas in our study patients performed hip movements only.
Our results revealed larger activations in the ispilesional hemisphere at group level, but single-patient analysis showed region-dependent involvement of contralesional hemisphere. The contribution of contralesional activity in movement preparation and execution in stroke patients is known and commonly interpreted as compensatory mechanism, although some studies indicate that the involvement of contralesional sensorimotor regions might be unhelpful and maladaptive for motor recovery.6,43-47 Results from a combined transcranial magnetic stimulation and diffusion tensor imaging study showed greater tracking error during antiphase bilateral ankle movement for patients with strong corticospinal tract conductivity from the nonlesioned hemisphere to paretic ankle than those with weak or no conductivity. 48 Future studies including larger groups of patients with cortical and subcortical lesions will help elucidate specific gait-related cortical activations and adaptive and maladaptive mechanisms in these two groups.
Overall, our results are in line with previous studies highlighting the critical role of PMC and PPC in motor preparation of upper limb movements17,18,49 and of lower limb movements in healthy individuals. 50 Functional magnetic resonance imaging (fMRI) studies using pattern recognition methods recently reported successful decoding of action intentions from preparatory blood oxygenation level dependent (BOLD) response in multiple parietal and premotor brain areas.16,19
Additionally, our study further supports previous reports demonstrating fNIRS validity for assessing gait functions in healthy participants41,51-53 and patients with stroke.42,54,55
More important, our results suggest that discrimination of left and right lower limb movement preparation trials is possible using a trained classifier based on LDA. The best classification performance was obtained considering totHb signal changes either in PPC or in PMC and PPC combined. However, patient-specific channels’ selection might be necessary for BCI applications due to region-dependent variability on the accuracy across patients.
Overall, LDA classification performance indicates that changes of totHb signal in PPC and PMC, associated with lower limbs movement preparation in patients after stroke, can be exploited for BCI implementation despite the observed differences in interhemispheric lateralization. Successful discrimination of fNIRS activity associated with left and right lower limb movement preparation trials might be then used to drive external rehabilitative effectors (eg, Lokomat orthosis 56 ).
Higher accuracy in classifying lower limb movement or motor intention and preparation from hemodynamic patterns in patients with stroke might be achieved using more sophisticated pattern recognition methods. In healthy subjects, multivariate pattern classification of fNIRS signals reduced the latency to decode a change in finger tapping by 50% (from 4.8 to 2.4 seconds). 57 Sitaram and colleagues, 58 the first to apply pattern recognition algorithms—Support Vector Machines (SVM) and Hidden Markov Model (HMM)—for classification of fNIRS data associated with motor activity in healthy volunteers, reported an average classification accuracy of left and right hand motor imagery of 73% with SVM and of 89% with HMM.
To date, several studies indicated that despite the intrinsic low temporal resolution of hemodynamic signals, fNIRS and fMRI signals could be used for neurofeedback application and BCI.59-63 It has been shown that through real-time fMRI feedback of the difference in activity between the contralateral M1 and the ipsilateral M1 healthy participants were successful in increasing contralateral activity by suppressing activity in the ipsilateral M1. 64 A similar approach might be used for motor rehabilitation after stroke using fNIRS signals. Moreover, a recent pilot study showed that chronic stroke patients, through real-time fMRI training, were able to increase activity in the ipsilesional ventral premotor cortex, which in turn led to a decrease of intracortical inhibition. 8
Thus far, while several applications for rehabilitation have been proposed and tested based on EEG and fMRI signals only few focused on fNIRS signals. The results of the present pilot study provide important indications toward the implementation of an fNIRS-BCI for gait rehabilitation.
Footnotes
Acknowledgements
We would like to acknowledge Dr Ann-Christine Ehlis and Ramona Täglich for their technical support.
Authors’ Note
Authors Massimiliano Rea, Mohit Rana, and Andrea Caria contributed equally to the work. Senior authors Ranganatha Sitaram and Andrea Caria contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study was supported by EC grants: FP7-ICT-2009-247935—BETTER: BNCI-driven Robotic Physical Therapies in Stroke Rehabilitation of Gait Disorders; FP7-ICT-2009-231724—HUMOUR: Human Behavioral Modeling for Enhancing Learning by Optimizing Human-Robot Interaction; Italian Ministry of Health, GR-2009-1591908; FP7-ICT-2009-258749-CEEDs: The Collective Experience of Empathic Data Systems; FP7-ICT-2013-609593-BNCI Horizon 2020. The Future of Brain/Neural Computer Interaction: Horizon 2020.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.