
Abstract
Background. Hemiparesis after stroke can severely limit an individual’s ability to perform activities of daily living. Functional electrical stimulation (FES) has the potential to generate functional arm and hand movements. We have observed that FES can produce functional hand opening when a stroke patient is relaxed, but the FES-produced hand opening is often overpowered by finger flexor coactivation in response to patient attempts to reach and open the hand. Objective. To determine if stimulating both reaching muscles and hand opening muscles makes it possible to achieve useful amounts of simultaneous reach and hand opening even in the presence of submaximal reaching effort. Methods. We measured reach and hand opening during a reach-then-open the hand task under different combinations of voluntary effort and FES for both reach and hand opening. Results. As effort was reduced and stimulation generated more movement, a greater amount of reach and hand opening was achieved. For the first time, this study quantified the effect of voluntary effort for reach and hand opening on stimulated hand opening. It also showed variability in the interaction of voluntary effort and stimulation between participants. Additionally, when participants were instructed to reach with partial effort during simultaneous FES, they achieved greater reach and hand opening. Conclusions. Simultaneous reaching and FES hand opening is improved by including FES for reach and reducing voluntary effort. In the future, an upper extremity neuroprosthesis that uses a combination of voluntary effort and FES assistance may enable users to perform activities of daily living.
Introduction
Poststroke hemiparesis limits arm and hand function, making bimanual tasks difficult if not impossible. 1 Hemiparesis is worsened by disuse and involuntary coactivation patterns across multiple joints (ie, synergy patterns). 2 For example, when a stroke patient abducts and/or flexes his or her shoulder (as when reaching), the biceps and forearm flexors may involuntarily activate (flexor synergy) at the same time, preventing lifting the arm and reaching forward simultaneously. These synergy patterns have been well quantified2-4 and appear to be expressed in proportion to shoulder abduction and reaching effort.4-6
Functional electrical stimulation (FES) of paretic muscles has the potential to generate functional reach and hand opening and has been used successfully to improve function after spinal cord injury.7-9 Similarly, electrical stimulation of finger extensors in stroke10-15 produces hand opening while the participant is relaxed. However, when the user exerts effort to reach or open the hand during stimulation, the hand does not open as much as when the person remains relaxed,16,17 presumably because effort to open the hand produces involuntary finger flexor contractions.10,16,18 Voluntary hand opening effort reduces FES extension of the metacarpal phalangeal joint 16 ; therefore, maximal stimulated hand opening is achieved when the user remains relaxed. Similarly, voluntary shoulder abduction and reaching effort produces net wrist and finger flexion force and forearm co-contraction. 4 Elbow extension due to triceps stimulation is limited by both simultaneous voluntary shoulder abduction 19 and increased voluntary effort in stimulated muscles.20,21 These results strongly infer that voluntary effort for reach and hand opening will interfere with FES hand opening but do not directly quantify the effect of voluntary effort on stimulated hand opening.
Our long-term objective is to develop a neuroprosthesis that restores arm and hand function in moderate to severely impaired stroke survivors. Ideally, residual voluntary movement of the same limb would control stimulation to produce desired arm and hand movements. Considering the proportional gradation of forces at different joints produced by synergy patterns, partial effort may not completely limit the effects of stimulation, allowing useful levels of hand opening. Therefore, our aim is to achieve adequate FES-generated movement in the presence of some simultaneous effort.
This pilot study’s goal is to provide estimates of the potential hand opening achieved with an FES system if simultaneous voluntary reaching and hand opening effort are reduced. There are 2 hypotheses: (a) submaximal reaching effort combined with stimulation of reaching and hand opening muscles will result in larger hand opening and greater reaching distance than maximal voluntary reaching effort with stimulation of hand opening muscles and (b) during stimulation for hand opening and reach, zero simultaneous hand opening effort will result in greater hand opening than maximal hand opening effort. The resulting preliminary data will provide a basis for designing experiments to evaluate the interaction of voluntary effort and FES in the stroke population and provide an initial assessment of the hypotheses. If these hypotheses are true, partial voluntary effort may provide a command signal for an FES system that produces functionally relevant reach and hand opening.
Methods
Participants
Participants were recruited from an outpatient stroke clinic. Primary inclusion criteria included the following: (a) at least 6 months poststroke, (b) able to follow 3-stage commands, (c) able to reach forward at least 10 cm while the investigator supported the elbow and wrist, (d) unable to fully reach and open the hand while the arm is unsupported, (e) functional upper extremity passive range of motion, and (f) functional stimulated hand opening while relaxed. All participants provided written informed consent prior to participation in this study, which was approved by an institutional review board. An upper limb Fugl-Meyer Motor Assessment and modified Ashworth test characterized each participant’s upper limb motor impairments.
Seven participants enrolled in the study, and 5 completed the protocol. Table 1 contains participants’ demographic information. Subjects 6 and 7 did not complete the protocol for the following reasons: (a) when we stimulated the arm, subject 6 could not avoid simultaneous volitional effort to lift the arm, and (b) we could not identify electrode positions for subject 7 that produced consistent hand opening.
Participant Demographics and Settings.
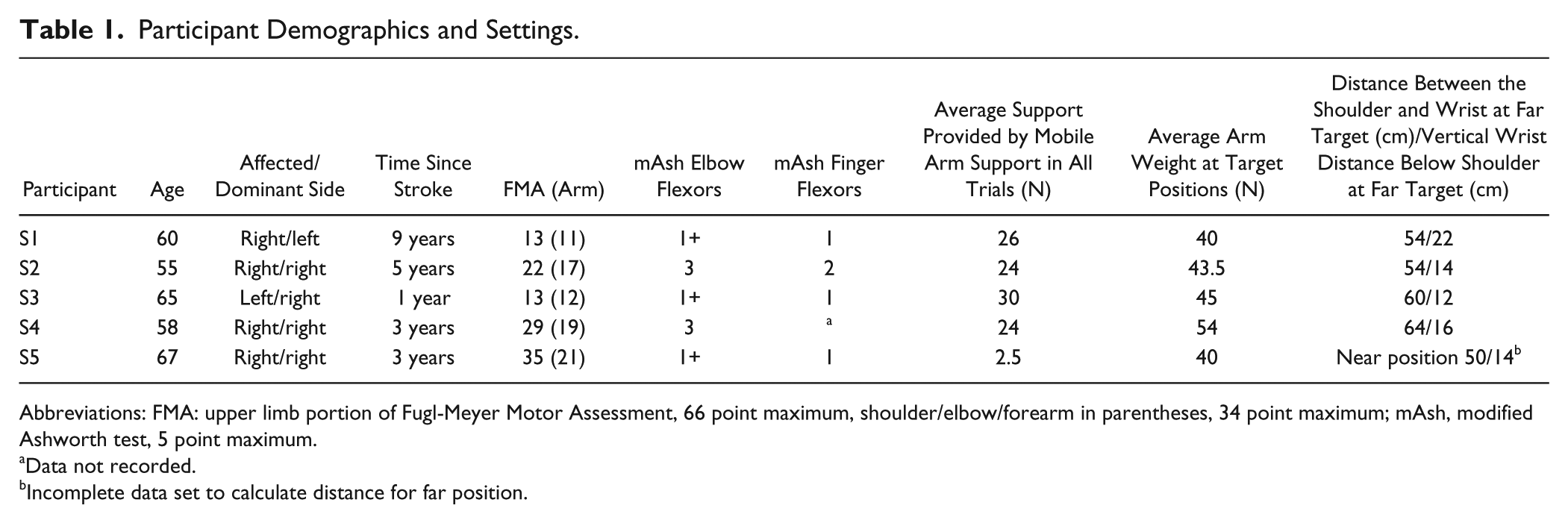
Abbreviations: FMA: upper limb portion of Fugl-Meyer Motor Assessment, 66 point maximum, shoulder/elbow/forearm in parentheses, 34 point maximum; mAsh, modified Ashworth test, 5 point maximum.
Data not recorded.
Incomplete data set to calculate distance for far position.
Setup
Participants performed a series of reach and open the hand trials, described below, with their paretic arm. Starting with the wrist positioned at the base of the sternum and the elbow flexed 90°, participants were cued to reach toward a target and attempt to open their hand under a variety of stimulation and effort conditions. A participant is shown performing the task in Figure 1A. We recorded arm position with an optical tracking system (Optotrak) and recorded surface electromyograms (EMGs) from flexor digitorum superficialis and extensor digitorum communis. A custom device recorded hand opening (measured as the distance between the fingers and tip of the thumb) and grasp force. 22
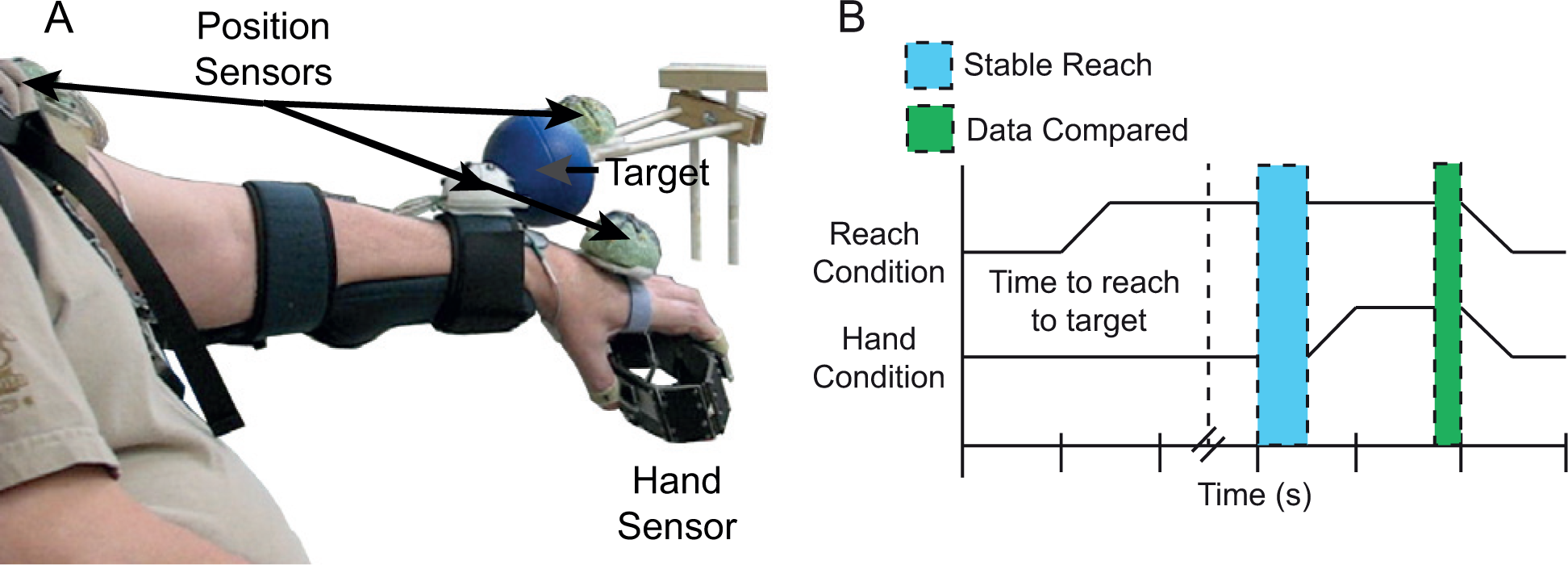
(A) Participant performing the reach and open task. (B) Graphical description of the reach and then open the hand task.
Two computer-controlled stimulators activated muscles for reach and hand opening. Surface stimulation electrode sizes ranged from 1.25 in. round to 2 in. × 5 in. rectangular. We targeted the anterior and middle deltoids for shoulder abduction and flexion and triceps for elbow extension. We also stimulated subject 4’s biceps to prevent overshooting the near target. The goal for stimulated hand opening was to produce finger extension, thumb abduction, and thumb extension by stimulating extensor digitorum communis, extensor pollicis longus, and abductor pollicis brevis.
Surface stimulation produced hand opening and elbow extension without pain, but had difficulty recruiting adequate shoulder abduction and flexion to achieve full arm elevation. Therefore, an elevating mobile arm support (Jaeco) provided an upward force at the forearm in all trials, reducing the shoulder force that FES needed to generate. The goal of the arm support was to provide participants with enough support to enable them to volitionally reach approximately halfway between their resting position and their maximum forward passive reach. Subject 4 was able to lift his arm on his own, but had difficulty independently controlling the elbow at the same time; therefore, for subject 4 the support’s purpose was to allow the stimulation to produce maximal reach.
Experimental Procedures
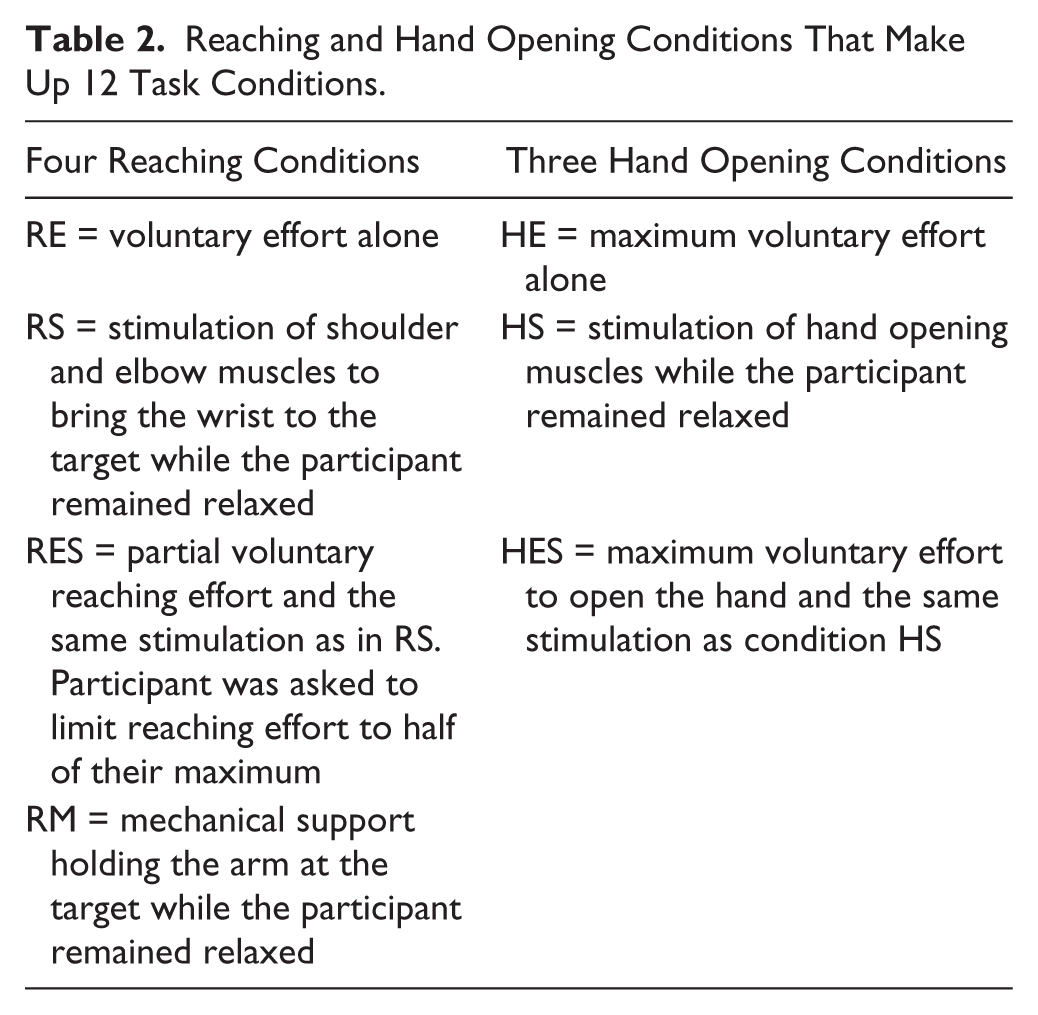
During the first experimental session, we determined electrode positions and stimulation levels that produced reach and hand opening without eliciting pain while the participant relaxed. Then, over several sessions, participants learned the reach and open tasks under 12 combinations of 4 reaching conditions and 3 hand opening conditions, which are described in Table 2. Participants were cued to reach toward a target in front of them under one of the reaching conditions (RE, RM, RS, RES). Once the arm came to a steady position, participants were instructed to maintain their reaching effort while attempting to open their hand under one of the hand opening conditions (HE, HS, HES). Trial timing is illustrated in Figure 1B.
Reaching and Hand Opening Conditions That Make Up 12 Task Conditions.
Once the participant could perform the reach and open task consistently under the 12 conditions, data (ie, amount of hand opening, reaching distance, EMGs) were collected. Two separate sessions were used to record data for the near and far targets, respectively. The near target position was half of the participant’s maximum active reach distance. The far target position was the furthest position that shoulder and elbow stimulation could achieve while the subject remained relaxed. The distance between the shoulder and the wrist and the vertical distance of the wrist below the shoulder during manual support (RM) to the far target are included in Table 2. Each participant performed at least 3 trials under each combination of conditions.
Data Analysis
The last second of each trial was used to calculate hand opening and the distance from the target to the wrist. If all of a participant’s trials of a single reach and hand opening condition had hand opening increase less than half a centimeter, the result was treated as no hand opening. This prevented passive hand movement during reach from appearing like active hand opening.
Analysis of variance (ANOVA) models were used to compare hand opening and the distance from the target. The models included subject as a random factor while reaching condition, hand opening condition, and target position were fixed factors. Interaction effects were included for the fixed effects. If factors were statistically significant, the Tukey–Kramer comparison of means was used to determine which conditions were statistically different. The distribution of residuals was statistically different from a normal distribution (P < .05, Kolmogorov–Smirnov test). Contributing factors were residual outliers and residual skewness of −0.22. A visual inspection of residuals’ normality suggests the difference from a normal distribution does not alter P values sufficiently to disbelieve the results considering that analysis repeated with outliers removed produced the same conclusions.
To assess the primary hypotheses, we compared hand opening and the distance from target in subsets of the data:
To assess the net effect of reach on the hand we compared hand closing forces and forearm EMGs. We compared hand closing forces during voluntary reaching effort (RE) under the 3 hand opening conditions (HE, HS, and HES). We compared forearm EMG generated during the combination of reaching effort plus hand opening effort (RE + HE) and during the combination of mechanical support plus hand opening effort (RM + HE). These provide insight into forearm co-activation in response to reaching effort. The 3 analysis time windows were 1 second long: (a) at the beginning of the trial while the participant was relaxed, (b) during reach prior to hand opening, and (c) during the final second of hand opening.
Results
Reducing reaching and hand opening effort and augmenting it with stimulation increased hand opening at distances that were both within and beyond participants’ voluntary reaching distance. Hand opening increased with stimulation and reduced levels of reach and hand opening effort. These findings support both hypotheses: Hypothesis 1—hand opening during stimulated reach with partial reaching effort and stimulated hand opening (RES + HS) was greater than during voluntary reaching effort and stimulated hand opening (RE + HS) (P < .05); and Hypothesis 2—hand opening was greater during stimulated reach and stimulated hand opening (RS + HS) than during stimulated reach and stimulated hand opening with maximal hand opening effort (RS + HES; P < .05). Figure 2 shows average hand opening across all participants and target positions for the 12 combinations.
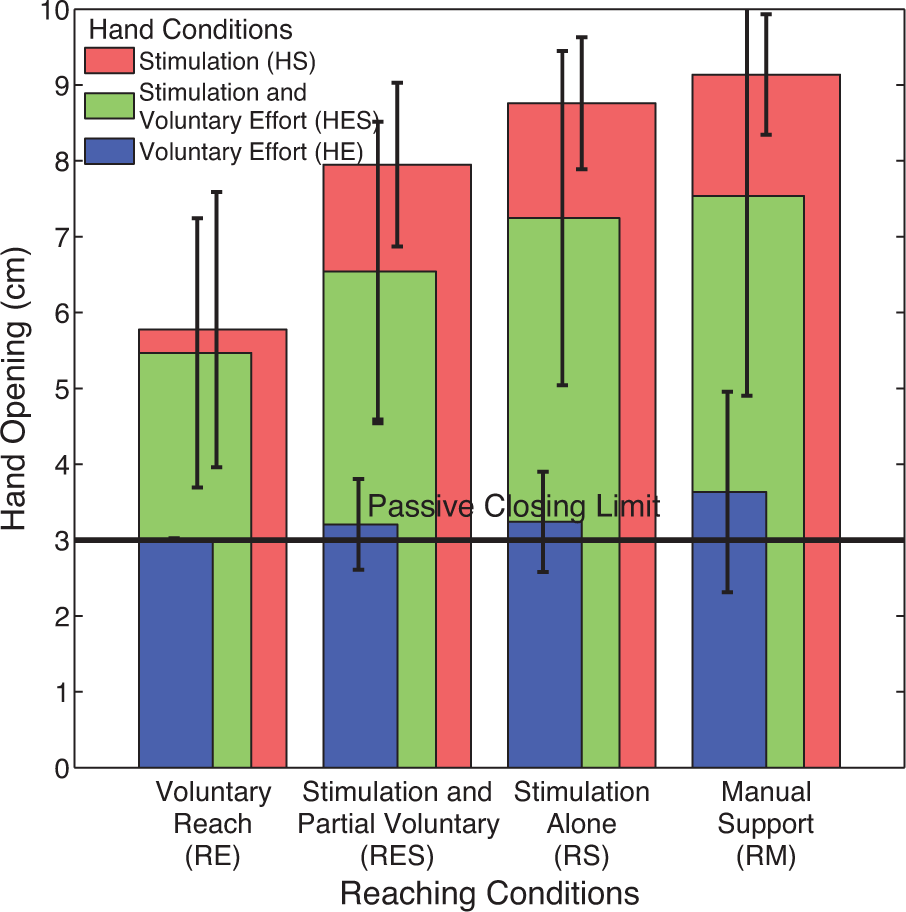
Amount of hand opening (mean ± standard deviation) averaged across all participants for all 12 task combinations. The passive closing limit (3 cm) is the smallest amount of hand opening that the hand sensor could measure.
Hand Opening
The reaching condition × hand opening condition interaction was significant (P < .001) while the other interactions were not significant: reaching condition × target position (P = .709) and hand opening condition × target position (P = .692). Significant main effects were reaching condition (P < .001), hand opening condition (P < .001), and participant (P < .001) but not target position (P = .196).
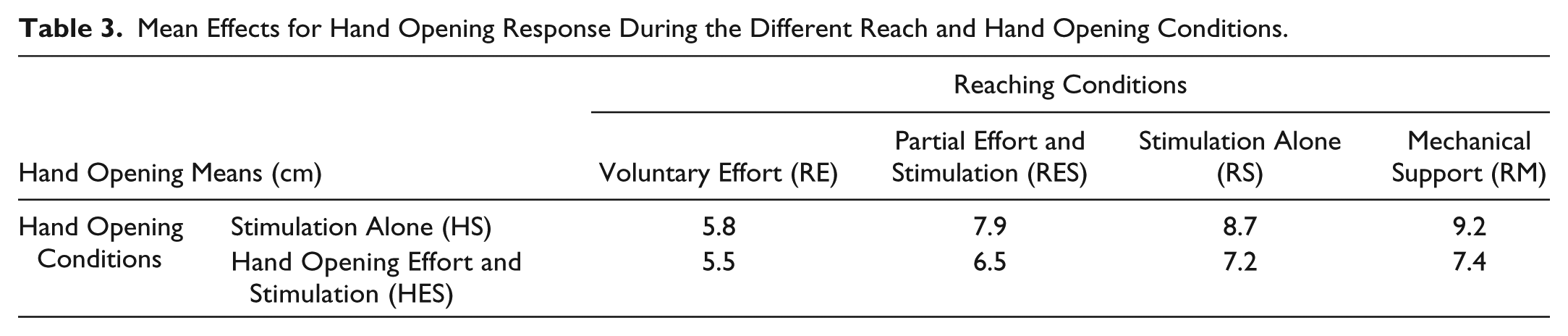
The model was simplified to calculate effect means shown in Table 3. Target position was removed from the model because it was not statistically significant in the interaction or main effects. Since there was minimal voluntary hand opening without stimulation (HE), those data were also removed from the model. The random effect of participants accounted for 2.1 cm of variance while model error variance contributed 1.5 cm.
Mean Effects for Hand Opening Response During the Different Reach and Hand Opening Conditions.
We also looked at the effects of reaching and hand opening effort in individual participants. The effects of reducing reaching effort while stimulating reach and hand opening are shown in Figure 3A. The effects of voluntary effort to open the hand during hand stimulation and stimulated reach are shown in Figure 3B. Variation between subjects is large, ranging from virtually no effect for either type of effort (S2) to large effects of voluntary reach (S1, S4, S5) and a large reduction of hand opening with voluntary hand opening effort (S1).
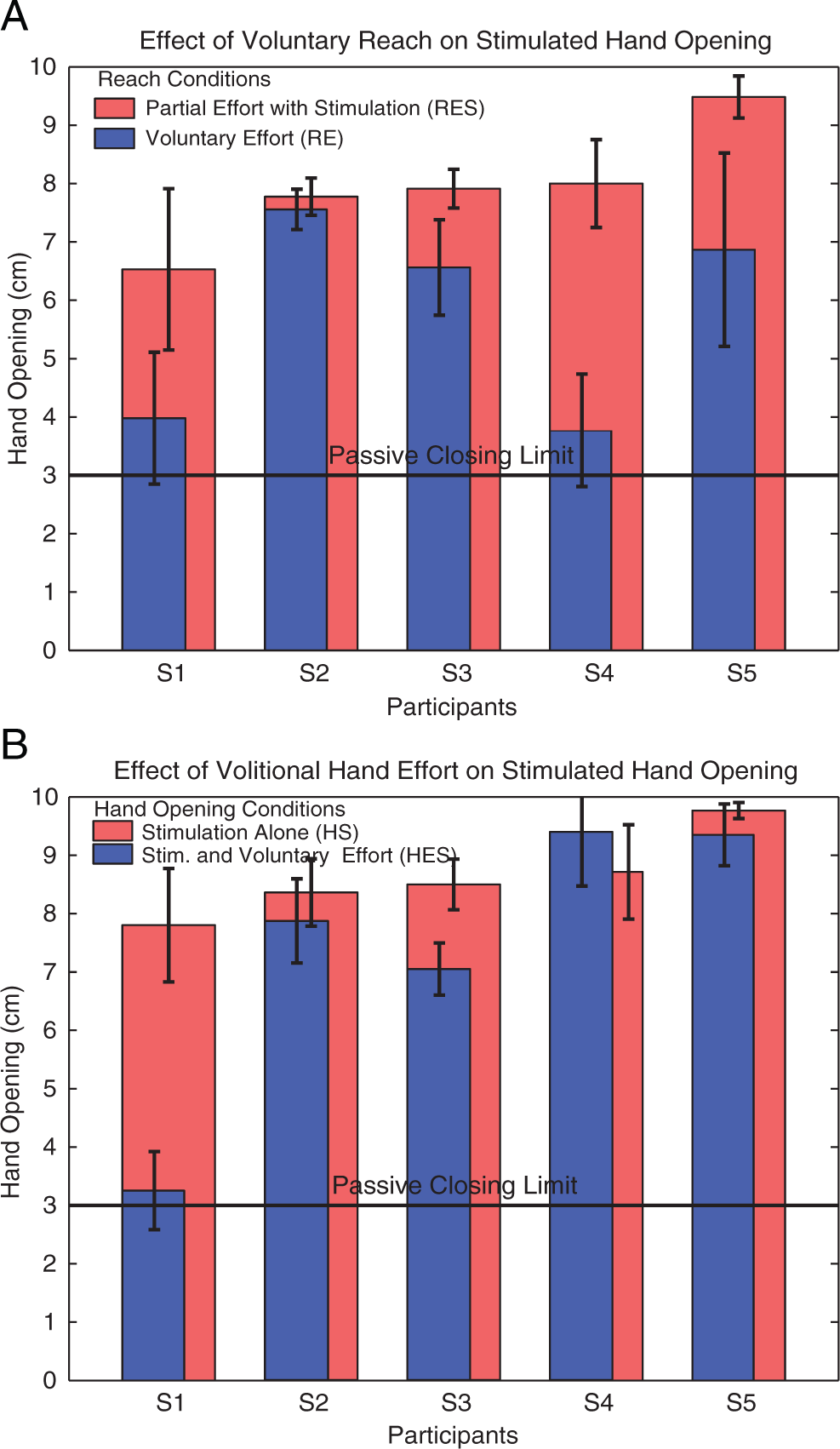
(A) Amount of stimulated hand opening (mean ± standard deviation) during RE + HS and during RES + HS for each participant. (B) Amount of hand opening (mean ± standard deviation) during RS + HS and during RS + HES for each participant.
Reaching Distance
Reaching distance was measured as the distance from the target to the wrist. To simplify comparisons across participants and sessions, we subtracted the shortest average distance from the target in any of the 12 conditions from all of the trials for that participant. The reaching condition × target position had a significant interaction (P < .001). Nonsignificant interactions included target position × hand opening condition (P = .652) and reaching condition × hand opening condition (P = .625). The primary effects had the following P values: reaching condition (P < .001), target position (P < .001), participant (P < .001), and hand opening condition (P = .477).
The primary factor that affected distance from the target was reaching condition. Distance from target is shown in Figure 4 for each participant during the different reaching conditions at the far target position. For subjects 1, 3, and 5, voluntary reaching (RE) was difficult and left them at least 15 cm further away from the far target than with stimulation (RS or RES). With stimulation (RS and RES), all of the participants were able to reach both targets. Partial reaching effort did not prevent participants from reaching the targets.
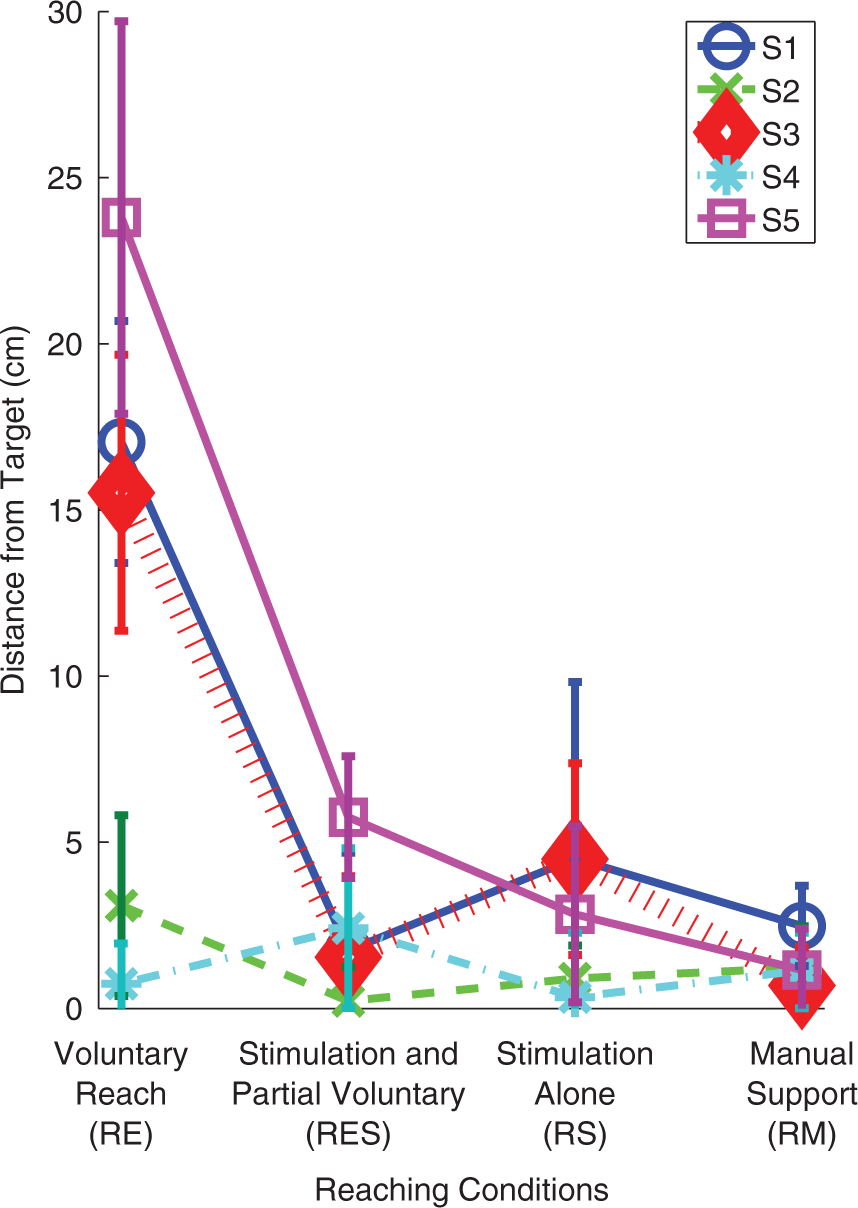
Reaching distance from the far target (mean ± standard deviation) during different reaching conditions.
Hand Closing Force
The combinations of reach and hand opening where the hand produces a compression force instead of opening provide additional insight into stimulation’s effects. Figure 5 shows the effect of reaching effort (RE) and subsequent hand opening conditions (HE, HS, HES) on hand closing force. Subjects 1, 3, 4, and 5 appear to increase hand closing force during reach before adding the hand opening condition. For subjects 4 and 5, there was no further increase in hand closing force during maximum effort to open the hand (HE). When stimulation was added at the hand (HS and HES) during voluntary reaching effort alone (RE), stimulation overpowered flexion forces and produced hand opening as shown in Figures 2 and 3A. However, for subjects 1 and 3, hand closing force increased during HE. Hand opening stimulation (HES) overpowered these forces for subject 3, but not for subject 1.
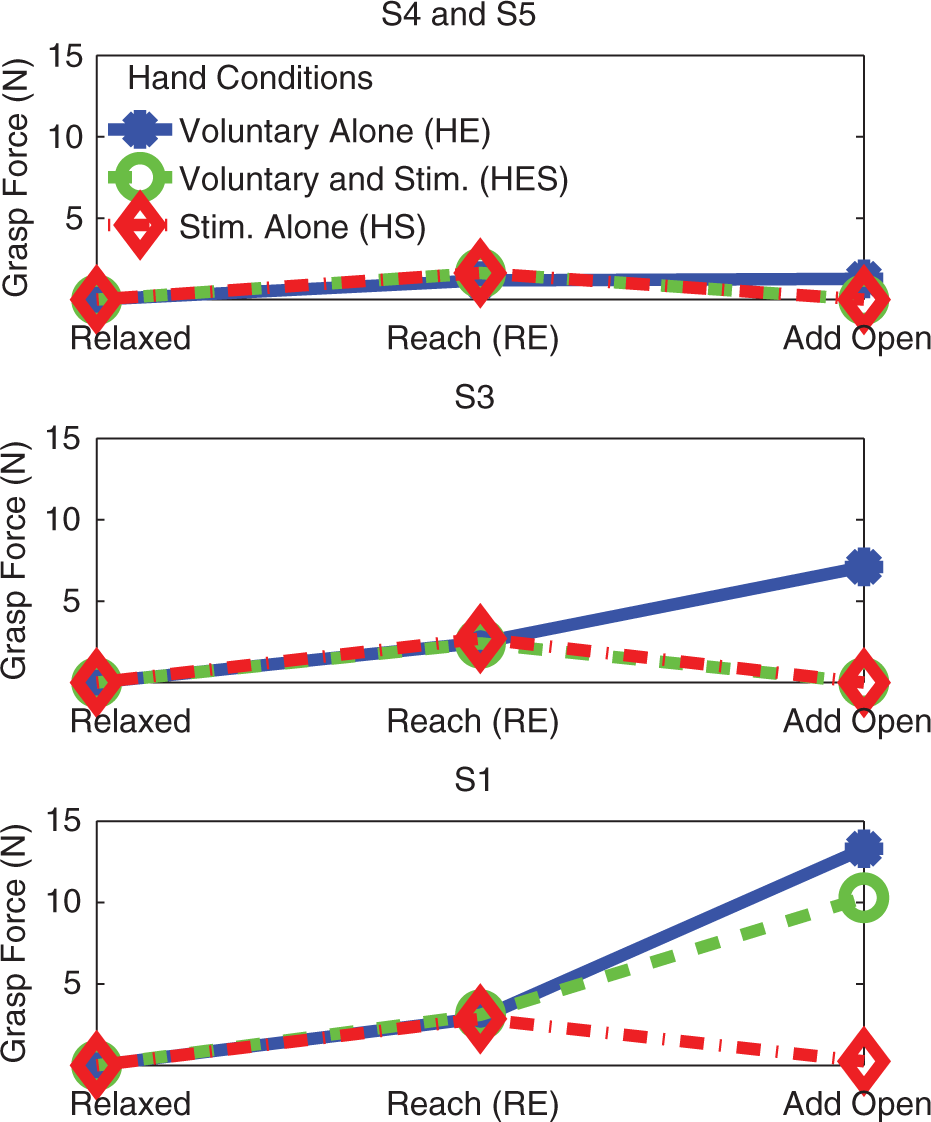
Grasp force during voluntary reaching and different hand opening conditions. The horizontal axis shows the progression from being relaxed, to reaching, to reaching while opening the hand. The different lines represent the 3 hand opening conditions. The top plot shows averaged data for subjects 4 and 5. The middle plot shows data for subject 3, and the bottom plot shows data for subject 1.
Forearm EMG
Forearm flexor and extensor EMGs showed a trend of increasing with either reaching or hand opening effort. EMG magnitudes were averaged across all of the available participants (subjects 2-5). During voluntary reach and hand opening effort trials (RE + HE), average flexor/extensor EMGs were 10 µV/8 µV while relaxed (before attempting reach), 15 µV/21 µV during voluntary reach (RE before attempted HE), and 35 µV/34 µV during reach and hand opening (RE + HE). During mechanical support and effort to open the hand (RM + HE), flexor/extensor EMGs were 10 µV/9 µV while relaxed (RM before attempted HE) and 22 µV/27 µV during hand opening (RM + HE). This suggests an increase in both flexor and extensor activation during volitional attempts to open the hand or reach.
Discussion
This study illustrates the impact of maximal effort to reach or open the hand on limiting hand opening achieved with FES. These results suggest that FES can produce functional arm movement and hand opening in the presence of partial reaching effort. Combining FES with partial effort allowed some participants to reach further and achieve greater hand opening for both near and far target locations, as hypothesized. In these experiments, we observed a general trend that decreasing voluntary effort for reach and hand opening enabled FES to have a greater effect on hand opening, although effect size varied between participants. The results support the hypotheses for a portion of the stroke population, and have implications designing neuroprostheses to augment arm and hand function in stroke survivors.
Implications for Neuroprosthetic Restoration of Arm and Hand Function
The differences in the interaction between stimulation and voluntary effort across individuals suggest multiple approaches for implementing an arm and hand neuroprosthesis for stroke survivors. For individuals in whom increased voluntary reach or hand opening effort decreases stimulated hand opening,10,16,18 it is important to limit effort exerted during stimulation. It is important to note that partial voluntary reaching effort and even maximum attempted hand opening effort in some individuals did not completely overpower the stimulated hand opening response and allowed functionally relevant levels of hand opening.
In a neuroprosthetic application, partial effort would produce arm and hand EMGs that could be useful as command signals to control stimulation without completely limiting the beneficial effects of reduced effort. Individuals that do not show a strong impact of effort on the stimulated response will require less reduction of voluntary effort. Thus, the results suggest a feasible approach to restoring functional arm and hand function through integrated voluntary and stimulated muscle activation. The combination of proximal and distal stimulation, with partial voluntary effort, will potentially restore function to a much broader group of individuals than previously described approaches that only stimulated hand opening.10,16,23 Limiting voluntary effort may have an additional benefit of decreasing the perceived level of effort, encouraging arm use, and potentially reversing learned disuse.
In addition to increasing function, a neuroprosthesis could enable people to participate in therapies that require a prescribed level of voluntary ability.24-27 If sufficient motor relearning is obtained from combined therapy and FES and persists after FES is turned off, it may be possible to discontinue use of the neuroprosthesis. However, if insufficient motor relearning is achieved, continuing use of a neuroprosthesis could provide substantial benefit indefinitely. FES during and following therapy is most likely of value in cases of moderate to severe chronic impairment, where therapeutic interventions to date have been less effective.
Mechanisms Underlying Reduced Hand Opening
Co-activation and co-contraction of finger flexors are likely contributors to the reduction of stimulated hand opening achieved during effort to reach or to open the hand. Results shown here (Figure 5) and by others4,19 show that voluntary shoulder abduction and reach effort increases wrist and hand flexion force, requiring additional extension force to open the hand. Finger flexor and extensor co-contraction in response to effort could reduce the effect of hand stimulation even if it does not change the net grasp force. Voluntarily contracting a stimulated muscle reduces the incremental force added by stimulation in both able-bodied 20 and stroke patients. 21 If electrically stimulated and volitionally activated motor units overlap, then for stimulation to increase muscle force, either inactive motor units must be recruited by stimulation or volitionally activated motor units must be stimulated at a higher frequency. 28
Reflexes might also limit hand opening. Reflex responses increase after stroke.29,30 Finger extensor stimulation can elicit finger flexor stretch reflexes 16 in individuals with stroke. In addition, electrical stimulation at a proximal joint can increase these stretch reflexes, 31 but the effects vary by muscle. Stimulation pulse width and stimulus location, nerve trunk versus muscle belly, can vary the neural contributions to force from central and peripheral pathways. 32 Our stimulation parameters are similar to parameters that do not primarily recruit motor units through reflex pathways, 29 suggesting that peripheral pathways are primarily responsible. In addition to stimulation producing and modulating reflexes, voluntary effort modulates reflexes as well. Poststroke effort generally decreases the stretch reflex threshold 33 and increases the size of the reflex response. 34 Stroke reflexes are less sensitive than controls to change in voluntary effort. 30 The overall reflex contribution to the change in hand opening is unclear because of modulation from both voluntary effort and stimulation.
Over time, FES can modulate sensory and motor responses in the sensorimotor cortex. 35 The duration of stimulation in our experiments was less than that used to produce a lasting effect in other studies, 35 but the sensory response to FES could affect volitional cortical activation in addition to producing a reflex response. The limitations with hand FES systems for stroke10,36 and experiments evaluating simultaneous voluntary effort and stimulation16,19-21 suggest that the variability in the response to FES is not simply a result of altered cortical activation.
Study Limitations and Future Work
The results provide estimates for mean effect sizes and variability due to effort for reach and hand opening. The effect sizes will help determine sample sizes for future studies that examine these interactions in further depth. While the sample size was small, the relative variability in participants’ stimulation responses during effort suggests that patient impairment and lesion location should be incorporated into the model in a larger study. Accounting for these differences may help determine potential sources of variability in this heterogeneous population.
The residuals are statistically different from a normal distribution, violating one of the ANOVA test’s assumptions. As a result, P values could be biased to lower values. Considering that P values for statistically significant hand opening are less than .001 and that removing outliers produced the same conclusions, it is unlikely that the change in P values would be large enough to change the interpretation.
There is additional value in evaluating the effect of both sequential and simultaneous effort during static conditions so that force can be used as an estimate for voluntary effort. We tested EMG feedback for training participants to exert specific levels of voluntary effort. Participants successfully produced 50% of maximum EMG in a single muscle without visual feedback, but we studied a multijoint reaching task that would require combining EMG from multiple muscles to effectively evaluate partial effort. While EMG could provide an estimate of effort, the highly nonlinear force–movement relationship suggests that isometric force measurements would allow for a more quantitative relationship between effort and the stimulation response.
Surface stimulation of shoulder muscles for abduction has significant limitations. The goal was to stimulate the axillary and radial nerves to activate the deltoids and triceps without producing discomfort or activating distal muscles. Stimulation lifted the arm above the lap without mechanical support in 3 participants. In the future, it is important to stimulate additional muscles to confirm that functional reach can be generated without mechanical assistance in a large population of participants. Percutaneous or nerve cuff stimulation could stimulate deeper shoulder muscles and increase selective muscle activation while reducing discomfort. Since activating and measuring hand opening was more critical to the goals of this study than recording EMGs, the placement of stimulation electrodes took precedence over EMG electrode placement. Therefore, the EMG recordings should not be viewed as highly selective but as containing information from multiple wrist and finger extensors.
The amount of mechanical arm support varied between the participants (Table 2) and was set on the basis of functional reach distance rather than as a percentage of arm weight, as employed by Miller and Dewald. 4 This variation in support level would affect the voluntary shoulder abduction activation needed and contribute to between-participant arm/forearm co-activation variability. It may be possible to reduce this variability by standardizing support to achieve a set reaching distance, since the support required to achieve a specified range of movement varies across subjects. 5 However, it is unlikely that the difference in stimulated hand opening is totally accounted for by differences in arm support considering that S1-S4 had similar moderately high levels of support with variable reductions in hand opening, while S5 had minimal support during reach but only a moderate reduction in stimulated hand opening.
The hand sensor used in these experiments provides information about average hand opening and finger grasp force but there could be variations in individual fingers that are not measured. These experiments should be repeated while independently measuring the digits to confirm that functional tasks can be completed using combined voluntary effort and FES. A functionally useful average amount of hand opening may not be useful when the hand posture is unconstrained.
Conclusions
These data support our hypotheses that reducing voluntary effort during reach and hand opening and augmenting the effort with stimulation for reach and hand opening can elicit greater hand opening. It is important to note that the effect of voluntary effort during reach and hand opening on the stimulation response varies between participants, even with similar levels of impairment. To produce effective stimulated hand opening, one must be aware of the effect that voluntary effort has on the stimulation response. While partial voluntary reaching effort can have a limiting effect on the stimulation response, partial effort does not completely overpower it. Some reach and hand opening effort could be used in conjunction with hand opening stimulation, and still produce functional hand opening.
Footnotes
Acknowledgements
The authors thank Peggy Maloney for arranging participants’ visits; Steve Sidik, PhD, for statistical consultation; and Mary Harley, Terri Hisel, Amy Friedl, and Kristine Hansen for performing the assessments.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health National Institute of Child Health and Human Development (Grant Numbers R21HD055256, K24HD054600), the American Heart Association (Grant Number 11PRE6600000), and the United States Department of Education (Grant Number P200A100112).