
Abstract
Purpose. Impaired economy of gait, prevalent in chronic stroke secondary to residual gait deficits, is associated with intolerance for performing activities of daily living. Gait economy/efficiency is traditionally assessed by determining the rate of oxygen consumption during submaximal treadmill walking. However, the mechanics and energetics of treadmill versus overground walking are very different in stroke survivors with ambulatory deficits. Clearly, overground cardiopulmonary measures are needed to accurately profile movement economy after stroke. An obstacle to obtaining such measures after stroke has been the absence of reliable portable metabolic monitoring equipment. The purpose of this study was to establish the test–retest reliability of a portable metabolic monitoring device during overground walking in hemiparetic stroke survivors. Methods. Twenty-three chronic hemiparetic stroke survivors underwent two 6-minute walk tests while wearing a COSMED K4b2 portable metabolic measurement system. Intraclass correlations coefficients (ICC) were calculated for both cardiopulmonary parameters and distance covered to determine test–retest reliability. An ICC of ≥0.85 was considered reliable. Results. ICCs for relative Vo2 (0.90), absolute Vo2 (0.93), Vco2 (0.93), and minute ventilation (0.95) demonstrated high reliability, but not for heart rate (0.76) or respiratory exchange ratio (0.64). There was no significant difference in the distance each participant walked between the first and second tests, eliminating distance as a potential confounder of our analyses (ICC = 0.99). Conclusions. Our results strongly support the reliability of the K4b2 for quantifying overground gait efficiency after stroke. Use of this device may enable researchers to study how varying poststroke rehabilitation interventions affect this central measure of health and function.
Introduction
Stroke is the most common neurological disability in older Americans and a leading cause of death in the United States. 1 The majority of stroke survivors exhibit residual neurological deficits that impair function and mobility, predisposing them to a sedentary lifestyle. 2 These deficits also result in a marked increase in energy expenditure during regular walking, contributing to a general intolerance for performing basic activities of daily living (ADLs). 3
Measurement of cardiopulmonary parameters during maximal and submaximal exercise is critical to the assessment of energy expenditure, cardiovascular fitness, and economy of gait. Research using stationary metabolic equipment demonstrates that submaximal and peak treadmill testing in chronic hemiparetic stroke survivors is highly reproducible 4 and that hemiparetic stroke survivors expend 1.5 to 2 times more energy during submaximal treadmill walking as compared to age-matched, sedentary, nonstroke controls. 5 Higher oxygen consumption in stroke survivors during treadmill walking reflects impaired economy of gait or gait inefficiency. However, the full extent of gait inefficiency after stroke may be partially masked by the artificial impact that a moving treadmill belt has on hemiparetic gait parameters and subsequently oxygen consumption. For this reason, it may be far more relevant to capture cardiopulmonary parameters reflective of gait economy during overground locomotion, based on the more natural gait dynamics that accompany floor walking. To date, the energy cost of overground walking in chronic, hemiparetic stroke survivors has not been studied either cross-sectionally or across interventions due to the absence of reliability studies for portable metabolic monitoring equipment in this population.
The K4b2 (COSMED USA; Chicago, IL) is a portable, metabolic monitoring system that has shown initial reliability for measuring energy expenditure and economy of gait during steady-state, submaximal exercise in healthy adults without neurologic disability.6,7 However, no studies have thus far been conducted to assess overground movement efficiency in either healthy individuals or stroke survivors using this device. Establishing the reliability of such portable monitoring technology in chronic stroke would affect our ability to gain insight into the metabolic costs associated with overground walking and performance of ADLs in this population. The purpose of the current study was, therefore, to determine the test–retest reliability of the COSMED K4b2 during a 6-minute walk test in older, chronic hemiparetic stroke participants. Based on previous results in nonstroke populations during treadmill walking,6,7 we hypothesized that cardiopulmonary measures would demonstrate high reproducibility in overground walking after stroke, defined by an intraclass correlation coefficient (ICC) greater than or equal to 0.85.
Methods
Subjects
Chronic stroke participants (>6 months) with residual mild-to-moderate hemiparetic gait were recruited for participation in this University of Maryland, Baltimore, Institutional Review Board–approved study. The study results reported in this are are all cross-sectional, baseline observations, but the larger study involved an exercise intervention period that is currently ongoing. After written informed consent was obtained, participants underwent screening procedures (comprehensive history and physical/neurological examination by a neurologist or nurse practitioner) and a graded exercise treadmill test to determine eligibility for participation. To ensure safety and integrity of results, participants were excluded from participation if they had congestive heart failure, peripheral arterial disease, recent myocardial infarct (last 3 months), pulmonary or kidney failure, cancer, poorly controlled hypertension and/or diabetes, untreated depression (Center for Epidemiologic Studies Depression SCale score > 16), or cognitive impairment (Mini-Mental State Examination score < 23). There were also minimal entry criteria associated with capacity to ambulate and exercise at peak levels without signs of cardiac abnormalities to assure safety of participants during subsequent testing and training procedures.
Six-Minute Walk
The 6-minute walk (6MW) test involves a distance representative of community-based ambulation that is required for sustained ADLs. This test is used widely to assess longer-distance ambulatory function in patients with chronic disease. Standard procedures as previously reported by Enright 8 were followed for administration of this test. To increase safety, all participants wore a gait belt and used assistive devices and/or orthoses whenever applicable. Participants first performed a 6MW test without metabolic monitoring equipment to develop general familiarity with the testing format. Each participant then performed the 6MW test on 2 separate occasions with the portable metabolic system as described below. Testing with the portable system was repeated on separate days within a period of 1 week, providing more than adequate rest between Test 1 and Test 2.
Portable Metabolic Testing
Open circuit spirometry (K4b2; COSMED USA) provided breath-by-breath cardiopulmonary data during the repeated 6MW tests. The K4b2 consists of a small battery pack and portable gas analyzer (with a cumulative weight of less than 1 kg) that participants wore on their chest. A flexible rubber facemask with flowmeter used for breath-by-breath analysis was attached to the portable system. Prior to performing the repeated 6MW tests, participants underwent a period of standing acclimatization with the portable gear in place to enhance comfort and familiarity. Additionally, the participants sat quietly for 5 minutes while wearing the apparatus before commencing with the 6MW and associated gas exchange measurements. Based on K4b2 portable monitoring data obtained during the final 3 minutes of each of the repeat 6MW tests (steady-state conditions), we calculated the means for oxygen consumption (Vo2—absolute and corrected for body weight), carbon dioxide production (Vco2), minute ventilation (VE), and respiratory exchange ratio (RER). In addition, polar heart rate monitoring provided a mean steady-state heart rate (HR) for each 6MW test.
Data Analysis
Data were analyzed using SPSS Predictive Analytics Software 18.0 (SPSS, Inc, Chicago, IL). Repeated-measures t tests were performed to assess significant within-participant changes between Test 1 and Test 2 on 6MW distance and all cardiopulmonary/gas exchange measures. Bland–Altman plots were also generated to depict the variability of 6MWD and Vo2 during the 6MW. Furthermore, ICCs and Pearson correlation coefficients (r) were computed from data obtained from the first and second 6MW for distance walked, Vo2 (L.min−1 and mL.kg−1.min−1), Vco2, VE, HR, and RER to determine test–retest reliability. All data are expressed as mean ± standard deviation with a 2-tailed P value of <.05 required for significance. High reliability was defined as an ICC greater than or equal to 0.85.
Results
Subjects
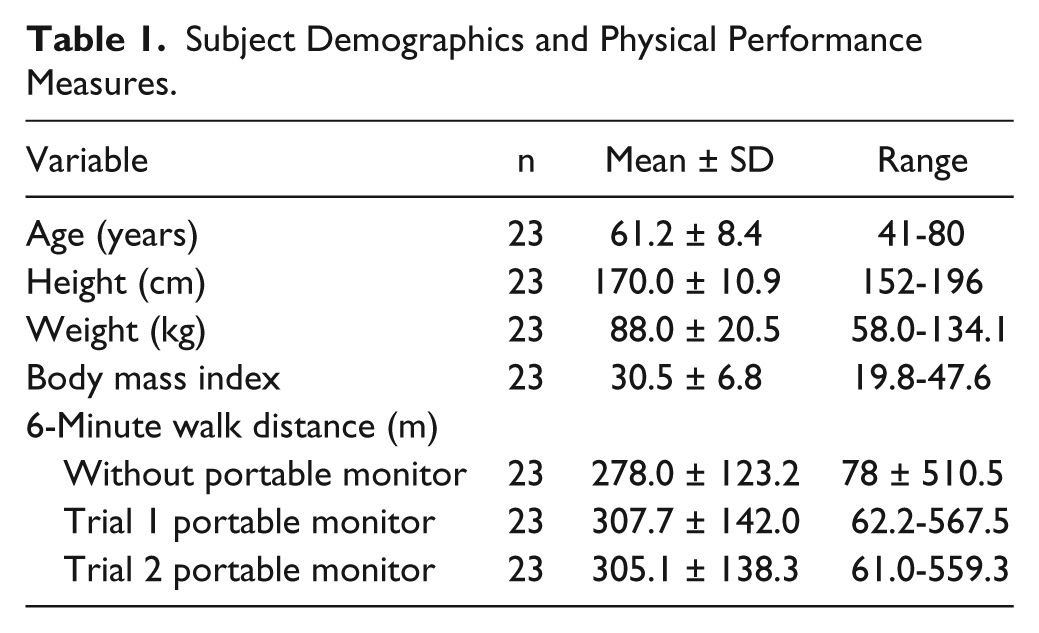
A total of 23 hemiparetic stroke patients (12 women, 11 men; mean age 61.2 ± 8.4 years, range 41-80 years) completed this study. Of those, 65% were African American and 30% were White (remainder Hispanic). Fourteen of the participants had left-sided hemiparesis and 9 were diabetic. Fifty-seven percent required the use of an assistive device for ambulation (cane n = 12; walker n = 1), and 35% used an ankle–foot orthosis. Additional details related to the physical characteristics of these participants are summarized in Table 1. There were no adverse events during portable testing, and the equipment was generally well tolerated.
Subject Demographics and Physical Performance Measures.
Six-Minute Walk
The difference in mean distance covered between the first and second 6MW (as shown in Table 1) was less than 1%. This nearly identical distance enabled confidence in the gas exchange comparisons shown below (Table 2), eliminating total work as a potential confounder. There was no significant difference between Test 1 and Test 2 (−2.6 m; P = .43) for mean 6MW distance, and the R2 value of .98 indicates that performance on Test 1 explained 98% of the variability in Test 2. Moreover, Bland–Altman plots of within-subject difference for distance walked versus the mean of Tests 1 and 2 (Figure 1) demonstrates excellent repeatability for this test. An ICC of 0.99 for distance covered further reflects an extremely high reliability for the 6MW test in this population.
Reliability of 6-Minute Walk Measurements in Stroke Patients.
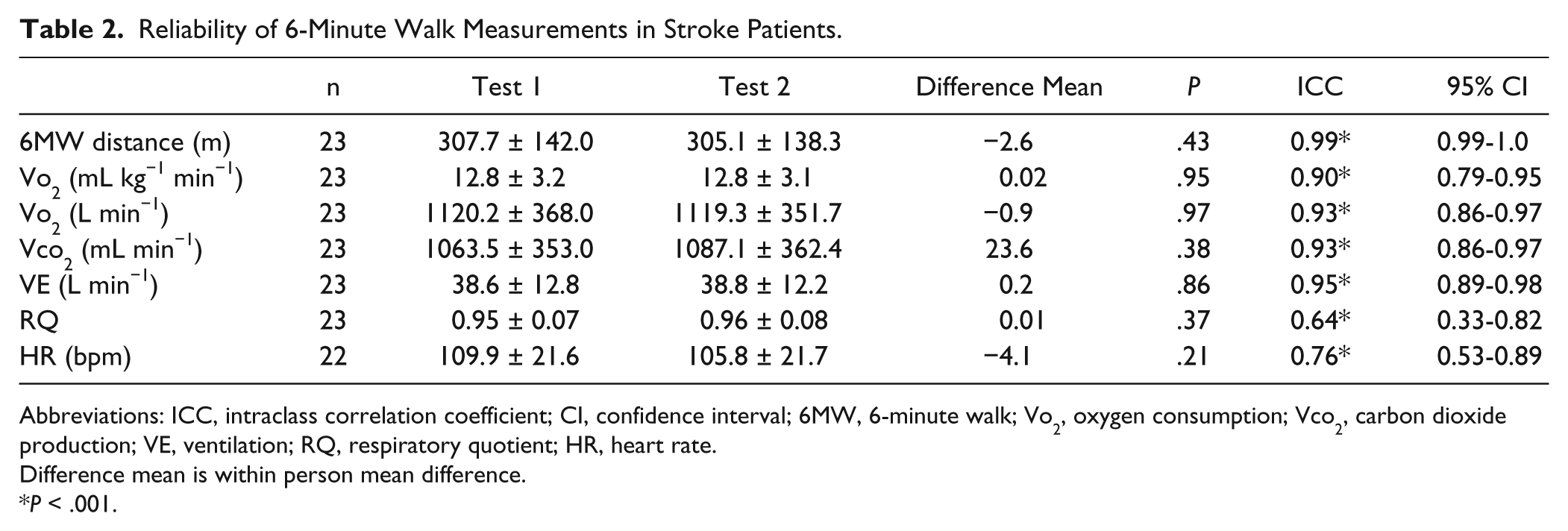
Abbreviations: ICC, intraclass correlation coefficient; CI, confidence interval; 6MW, 6-minute walk; Vo2, oxygen consumption; Vco2, carbon dioxide production; VE, ventilation; RQ, respiratory quotient; HR, heart rate.
Difference mean is within person mean difference.
P < .001.
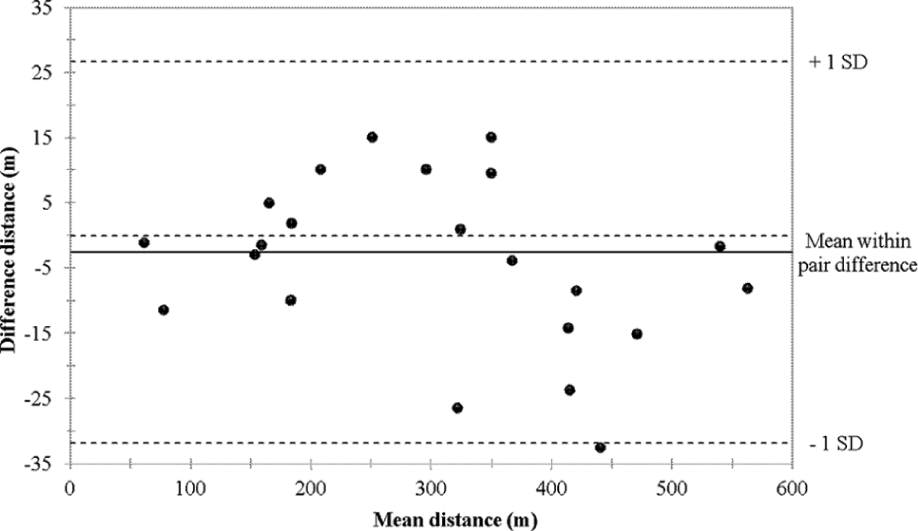
Bland–Altman plot of distance walked.
Portable Metabolic Testing
Test–retest results for all cardiopulmonary measures across the 2 separate 6MW tests with portable monitoring are also summarized in Table 2. As shown, there was no significant difference between tests for any of the cardiopulmonary measures taken. Bland–Altman plots of within-subject change in steady-state Vo2 (mL.kg−1.min−1) as a function of mean steady-state Vo2 (mL.kg−1.min−1) during Tests 1 and 2 (Figure 2) shows the high reliability of this measure. The gas exchange measures for Vo2, Vco2, and VE from test to test were also shown to be highly reliable as indicated by ICCs ≥ 0.90 (Table 2). Although there was no significant difference for HR or RER between Test 1 and Test 2, ICCs for these variables (0.78 and 0.66, respectively) fell below the previously defined reliability cutoff of >0.85.
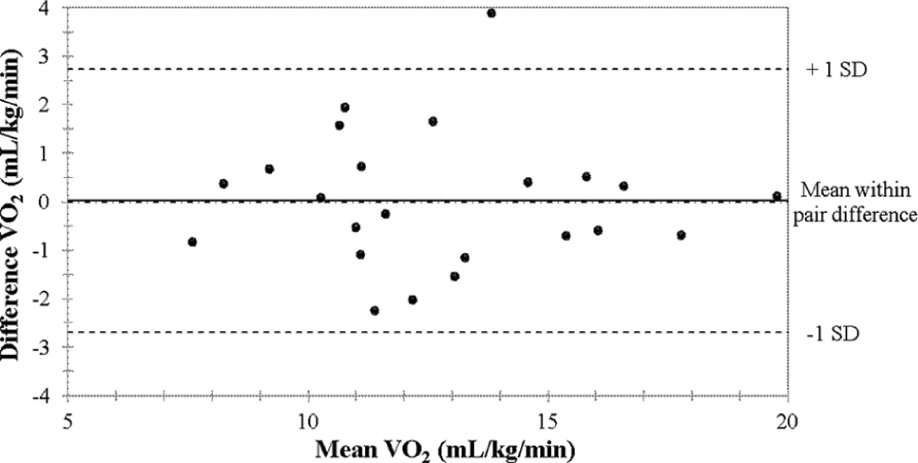
Bland–Altman plot of steady-state relative Vo2 (mL kg−1 min−1).
Discussion
This study is the first to establish test–retest reliability/repeatability of portable metabolic monitoring during overground walking in older chronic hemiparetic stroke survivors. The clinical significance is that disabled stroke participants may eventually be better evaluated for movement efficiency in the context of more natural settings compared to the artificial constraints imposed by laboratory treadmill testing. The reliability coefficients observed for Vo2, Vco2, and VE more than exceeded our preestablished reliability threshold, providing strong evidence for the validity of the Kb42 to measure overground gait economy and track intervention–induced gains in movement efficiency after disabling stroke. Importantly, this study also provides supportive evidence that the 6MW test is a highly reliable metric in the chronic phase of stroke recovery.
The 6MW was first established as a means of assessing the effectiveness of treatment in patients with cardiovascular and pulmonary disease. 8 It has since developed into a functional measure to characterize long-distance ambulation and disability in chronic stroke and other elderly populations.9-19 Research demonstrates that 6MW distances for healthy individuals range from 400 to 700 meters,20 -22 whereas, on average, stroke survivors cover 49.8% the distance of their healthy counterparts, 9 with reported ranges between 116 and 400 meters.4-19 Our cohort of 23 stroke survivors show a mean 6MW distance of 307.7 ± 142 m, placing them in the middle of the range reported by other stroke studies and establishing them as moderately impaired. Furthermore, our cohort of stroke survivors had a mean walking speed of 0.86 ± 0.39 m/s, which was 35% slower than that observed in age-matched healthy community dwelling adults (1.33 ± 0.21 m/s). 23
There is limited research analyzing the test–retest reliability of the distance covered during the 6MW in chronic stroke, but the few studies that have been conducted to date do support our current reproducibility findings. Reliability coefficients (ICCs) previously ranged from 0.98 to 0.99,11-13 which matches our finding (ICC = 0.99). Flansbjer et al 12 reported a 3.5% difference in mean distance covered between Test 1 and Test 2 of the 6MW, whereas Lui et al 13 reported a 0.5% difference in stroke. Our investigation demonstrated a less than 1% difference during testing with the portable monitoring equipment, adding to the literature by showing that the addition of the Kb42 device does not interfere with the reliability of this important measure of walking endurance. This may have important future ramifications in the context of using this functional test with portable metabolic monitoring to assess training induced improvements in poststroke functional limitations.
Reliable portable metabolic monitoring technology enables quantification of cardiopulmonary parameters outside of the laboratory, in settings more representative of typical free-living conditions. In healthy adults, research has shown that normal overground gait mechanics are altered during treadmill walking.24,25 This issue undoubtedly becomes even more prominent in the chonically disabled stroke population based on hemiparetic gait dynamics. This suggests that overground gait measures are more indicative of a patient’s functional status and should be favored over treadmill measures if possible. In fact, our current results demonstrate that walking economy numbers are 38% worse overground compared to a previously conducted treadmill gait economy study in stroke. 26 Therefore, to fully understand overground economy of gait after stroke, it is imperative to first establish reliable technology able to capture the cardiopulmonary effects of free-living movement.
The COSMED K4b2 has been shown to be valid and reliable for measuring energy expenditure and economy of gait during steady-state submaximal treadmill walking in healthy adults without neurological disability.6,7 Schrack et al 7 compared Vo2 and Vco2 obtained from the K4b2 to those obtained from a standard, stationary metabolic cart (Medgraphics D-Series Gas Exchange System) during submaximal treadmill walking (N = 19). ICCs between the 2 systems for Vo2 (0.95 and 0.97 for mL.kg−1.min−1and L.min−1, respectively) and Vco2 (0.93) showed high accuracy. Additionally, there was no significant difference between tests using the portable and stationary systems for Vo2 (P = .16), Vo2 adjusted for body weight (P = .25), or Vco2 (P = .09). Duffield et al 6 analyzed test–retest reliability of the K4b2 during treadmill running in physically fit men. High reliability was reported for VE, Vo2, and Vco2, with ICC ranging from 0.7 to 0.9, P < .05. Mendelsohn et al. 27 demonstrated moderate to high test–retest reliability of the K4b2 in older adults (82.4 ± 5.4 years) during various intensities of submaximal, all-extremity semirecumbent exercise for heart rate and METs (ICCs ranging from 0.85 to 0.91). Thus, although previous research has established the validity and test–retest reliability of the K4b2 during exercise modalities that do not incorporate overground walking,6,7,26 there are no overground studies available to gauge the reliability of this portable technology in more natural, free-living settings, representing a large gap in the literature. Furthermore, no research has determined the reliability of the K4b2 portable device in older hemiparetic stroke survivors, either on the treadmill or over ground. The current study is the first to have established this reliability in any population during overground walking, reporting ICCs quite similar to the portable unit reliability studies conducted in nonstroke adults on a treadmill, and comparing favorably with test–retest results obtained using stationary metabolic equipment during a treadmill reliability study after stroke. 4 Despite HR and RER falling below the previously defined reliability cutoff of >0.85, the most important cardiopulmonary measures in the context of overground walking economy assessment (Vo2 in particular) showed very high reliability, demonstrating the utility of the K4b2 for this purpose in older, hemiparetic stroke survivors. Further investigation is recommended prior to rendering final judgment on the utility of this device for capturing HR and RQ responses to physical activity after stroke.
Importantly, gait economy can improve with an exercise intervention after stroke according to a study using oxygen consumption during steady-state submaximal treadmill walking as the metric for economy. Specifically, Macko et al 26 observed that the same absolute level of treadmill walking required 15% less oxygen consumption following a period of regular treadmill aerobic training. Future studies, supported by our current reliability results, are now well positioned to evaluate how varying rehabilitation interventions affect the economy of movement over ground. Improvement in such measures would be far more relevant to community function and would not be confounded by either treadmill belt movement or the handrail support typically associated with treadmill testing after stroke.
Conclusion
The high reliability of portable metabolic monitoring for assessing cardiopulmonary parameters (Vo2, Vco2, and VE) during overground locomotion in older, chronic hemiparetic stroke survivors could justify a line of productive research that uniquely captures functional progression and regression in this population. Additionally, our results suggest that the 6MW test, independent of portable monitoring, is an extremely reliable and reproducible functional test in chronic stroke. Having established the K4b2 as reliable technology in the context of stroke walking economy could prove vital in gaining more insight into the energy cost of ADLs in this population. This study may have been limited by the fact that this was a heterogeneous cohort of medically stable outpatient stroke survivors. Therefore, the translation of these findings to an inpatient stroke cohort may be limited. Future research should focus on determining the extent to which economy of gait can be improved overground and understanding what types of exercise training produce the most impact on overground gait efficiency.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a VA Rehabilitation Research and Development (RR&D) CDA-1 Award, Department of Veterans Affairs and Veterans Affairs Medical Center, Maryland Exercise & Robotics Center of Excellence (MERCE), Geriatric Research, Education and Clinical Center (GRECC), The National Institute on Aging (NIA) Claude D. Pepper Older Americans Independence Center (P30-AG028747). This study was also supported by VA Merit Award funding and the National Institute on Aging Short-Term Training Program on Aging (No. 1T35AG036679).