
Abstract
Background. Neurologic music therapy has demonstrated improved walking performance in persons with neurologic disease; however, little evidence supports the use of music with functional resistance exercise to improve motor capacity and daily functions for children with cerebral palsy. Objective. To investigate the effect of additional patterned sensory enhancement (PSE) music combined with exercise for children with spastic diplegia. Methods. An assessor-blind, randomized controlled trial with 6- and 12-week follow-ups was carried out. Thirty-six children with spastic diplegia, aged 5 to 13 years, were assigned to a PSE group (n = 18) or a no-music group (n = 18). Both groups received 6-week, home-based, loaded sit-to-stand exercise, but only the PSE group exercised with prerecorded PSE music. The primary outcome was Gross Motor Function Measure (GMFM). Secondary outcomes included Pediatric Evaluation of Disability Inventory (PEDI) mobility and self-care domains, 1-repetition maximum of sit-to-stand, and walking speeds. Results. Three children did not complete the program. Intention-to-treat analysis showed both groups improved in GMFM D, E, and Goal dimensions; Functional Skills Scales of PEDI mobility domain; and 1-repetition maximum of sit-to-stand at posttest and follow-ups (P ≤ .005). The PSE group improved significantly greater than the no-music group in the GMFM D and Goal dimensions (P < .005) after training, and the improvement persisted for at least 6 or 12 weeks (P ≤ .013). No significant improvements in the rest PEDI scales and walking speeds were found. Conclusions. Adding neurologic music therapy to functional resistance exercise could induce greater improvements in gross motor capacity for children with cerebral palsy.
Keywords
Introduction
Cerebral palsy (CP) describes a group of permanent disorders of the development of movement and posture. 1 Children with CP usually have muscle weakness, 2 poor motor control, 3 and restricted daily function. 4 Studies have shown that children with spastic CP might benefit from task-specific and functional resistance exercise,5,6 such as carrying loads during sit-to-stand (STS). However, one systematic review found little evidence to support the effects of resistance exercise. 7 The poor motor control of this population may limit the training effects of resistance exercise. 8
Music has potential to elicit motor responses and make exercise more enjoyable. 9 Previous studies found that music could increase motivation and adherence to exercise.10-12 In addition, as timing plays a fundamental role in the execution of a movement, external timing constraint, such as musical rhythm, could induce coupling that decreases the spatial and temporal variability of a movement. 13 Other studies showed that brain areas processing melody, rhythm, and meter had a rich connectivity with motor areas,14-16 and the auditory rhythmic entrainment of muscle activation resulted from priming of the auditory-motor pathways.17-19 This auditory-motor facilitation is the neurophysiological basis for neurologic music therapy that uses music as an auditory cue to enhance functional movements.13,20 Patterned sensory enhancement (PSE) is one of the neurological music therapy techniques that uses all musical elements, including rhythm, pitch, and dynamics, that structure and regulate movement patterns in time, space, and force dimensions to facilitate movement execution. 21 A preliminary study examined the immediate effects of PSE music to guide the loaded STS exercise for children with spastic CP and found shorter movement time, better movement control, and greater extension power compared with the no-music control condition. 22 With evidence that PSE facilitates immediate outcomes, a study to determine the training effect of PSE music on physical outcomes with children CP is warranted.
The purpose of this study was to investigate the effects of a 6-week, home-based PSE music-trained loaded STS exercise program on gross motor capacity, functional strength, daily mobility and self-care functions, and walking speed for children with spastic diplegia.
Methods
Design
This was a prospective, assessor-blind, stratified, and randomized study. Children were assigned to either experimental (exercise with PSE music) or control (exercise with no music) group. Apart from their usual care, both groups received the same 6-week loaded STS exercise, except PSE-group children exercised with music. Parents were informed of the 2 possible allocations. The study was approved by the institutional human ethics review committee and was registered at ClinicalTrials.gov (NCT01367327).
Participants
Participants were recruited by referral from hospitals or advertising through a local CP association from November 2008 to July 2011. Written consents were obtained from their parents. The inclusion criteria were the following: (a) children with spastic diplegia, aged 5-13 years; (b) Gross Motor Function Classification System (GMFCS) 23 I-III; (c) able to stand up independently without falling; (d) able to follow verbal instructions and cooperate during the study; and (e) parental commitment to supervise the training program without altering current therapy or activities. The exclusion criteria were children who had (a) orthopedic surgery within 6 months; (b) uncontrolled seizure, severe joint contracture, cardiopulmonary disease, or other conditions preventing them from doing resistance exercise; and (c) hearing loss.
Randomization and Allocation Concealment
Participants were stratified by their age (5.0-8.5 years and 8.6-13.0 years) and gross motor function (GMFCS I-II and III) with a block size of 4. Randomization was executed after baseline assessment by drawing a sealed, opaque envelope containing assignment by a person who was not clinically involved in, and therefore blinded to, this study.
Intervention
Participants of both groups performed the loaded STS exercise at home for 6 weeks, 3 times per week under the supervision of their caregivers. The caregivers helped children schedule the exercise, put on the weighted body vest, and accompany them during the exercise. The exercise was introduced by the primary investigator during the first home visit. A chair, a rope at child body height, a body vest, and weights were prepared. The height of the chair was same as that used in the loaded STS test. The exercise regime was similar to that described by Liao et al. 6 In brief, each training session began with a 10-minute gentle muscle stretching and dynamic warm-up. The loaded STS exercise contained 3 sets: the first and third sets used load at 20% 1-repetition maximum (1-RM) of STS for 10 repetitions, while the second set used 50% of 1-RM and repeated until the child became fatigued. The session ended with a cool-down stretching. An exercise log was provided to the caregiver to record the date, number of repetitions for the exercise, duration of the exercise period, and any adverse events that occurred during or after the exercise, for example, soreness. Every 2 weeks, the 1-RM of STS was reassessed by the primary investigator during home visits. The training load was progressed accordingly, and 1 exercise session was performed under the supervision of the primary investigator. Telephone calls were made every week to parents to ensure exercise adherence.
To prescribe the PSE music, PSE-group children performed 6 repetitions of the loaded STS exercise at 50% 1-RM during the baseline assessment and the biweekly reassessments after their 1-RM of STS were determined. Sagittal plane movements were recorded by a digital video camera (DCR-TRV6; Sony, Tokyo, Japan) from the right side and analyzed by therapists to prescribe individualized PSE music for the PSE group. The fastest 3 STS movements were selected as references for prescribing the PSE music. All PSE music samples were composed by a music therapist using an electronic keyboard and GarageBand software on a Mac (Apple Inc, Cupertino, CA) following principles described previously. 22
The concept of PSE is to translate movement patterns into sound patterns in order to give the spatial, temporal, and force cueing. Pitch variation such as ascending and descending melodic lines can indicate the directions and cue the range of motion. Tempo, meter, and rhythmic patterns can reflect the speed and timing of a movement. Changes in loudness and harmony can prime appropriate strength of muscle activation. The musical elements are integrated to create an anticipatory sound pattern to cue the execution of movement. 21 The process in which the PSE music was composed to address the parameters of the STS exercise is described in the appendix.
The PSE music in this study was prerecorded for the participants to practice exercise at home. The music therapist prerecorded several PSE music templates of different meters and various tempi that were adjusted using the Cool Edit 2000 software (Syntrillium Software Corp, Scottsdale, AZ). After assessment, specific PSE recording, duration of about 20 to 25 minutes, was individually selected from the music templates according to individual movement patterns and speed and provided to each participant. A sample of PSE music composition is presented in Figure 1.

A piece of patterned sensory enhancement music sample.
Every 2 weeks, the music therapist adjusted tempo, meter, and other music elements for each participant according to the reassessment results and the individual needs. For example, for children who had difficulties in maintaining balance after standing (more likely to step forward and lose balance), an additional musical measure of sustained chords was inserted between phase 2 and the sit-down phase to support standing still. For children who could not sit down with control, a descending scale composed of longer notes in a broader register with decreased loudness was used to facilitate them to sit down slowly. During the home exercise, children were reminded to wait for the next musical cues to stand up if they mismatched the rhythm. Since PSE music provides cueing of the movement period, that is, music cueing causes the frequency entrainment of the entire duration of the movement to the rhythmic interval, 13 the caregivers were asked not to provide any cue to inform the children when to stand up, or ask the children to match the rhythmic beats. The caregivers were also not necessary to play the PSE music on occasions other than exercise because children’s movement performances might not benefit from additional music exposure.
Outcome Measures
Outcome measures were taken at baseline (T0), after 6 weeks of training (T1), at 6 weeks (T2), and at 12 weeks following the end of the training (T3). All assessments were performed by 4 trained physical therapists who were blinded to the treatment allocation. Each child was assessed by the same tester throughout the study.
The primary outcome was gross motor capacity measured by the Gross Motor Function Measure (GMFM) Dimensions D (13 items) and E (24 items). 24 The dimensions were chosen because they measured motor function in standing, walking, running, and jumping, which are common goal activities for children with spastic diplegia. Percentage scores of dimensions D and E were averaged to yield a Goal dimension score.
The secondary outcome measures included daily mobility and self-care functions, functional strength, and walking speed. The daily mobility and self-care functions were measured using the Chinese version of Pediatric Evaluation of Disability Inventory (PEDI) 25 through a structured interview with the main caregiver. The PEDI is appropriate to assess children with disabilities whose functional abilities are below 7.5-year-old level 26 and demonstrated good reliability, validity, and little ceiling effect. 27 The Functional Skills Scale of PEDI assesses capability by scoring whether the target activities can be performed or not in most situations on a binary scale. The Caregiver Assistance Scale measures performance in daily life by rating the degree or amount of physical assistance required on a scale of 0 (total assistance required) to 5 (independent). The raw scores were converted into scaled scores ranging from 0 to 100. 26
The 1-repetition maximum (1-RM) load of the loaded STS test was used to represent functional strength of lower extremities. 6 The test asked children to stand up from a chair with loads carried in a body-fitted vest and arms crossed. The chair height was set the same as the lower leg length (from floor to the popliteal fossa) for children with GMFCS I and II and was adjusted to 120% of lower leg length to make the task easier for children with GMFCS III. The 1-RM of STS is the maximal load that a child is able to carry in 1 STS movement. 28 Walking speed was measured by the 10-meter walking test. 6 Time taken to walk a 10-meter distance at the usual speed with walking aids or orthoses was assessed 3 times and an average speed was calculated. 6
Sample Size Calculation
The sample size calculation was based on an effect size of 1.0 drawn from a study that investigated the effect of exercises with music program on 1-leg balance in the elderly. 29 With a power of 80%, a 2-sided 5% significance level, and a 10% attrition rate, 18 participants were needed in each group.
Statistical Analysis
Data analysis was carried out using SPSS 13.0. Shapiro–Wilks tests were used for all continuous variables. Baseline characteristics were compared between groups using independent t tests, χ2 tests, or Mann–Whitney U tests. For all outcome measures, intention-to-treat analysis was performed using the last observation carried forward method to account for missing data. The analysis of covariance (ANCOVA) was used to assess the treatment effects between groups. Baseline measurement, number of sessions completed, and number of loaded STS repetitions completed were tested as covariates by regression. Alpha was set at .05, and the 95% confidence interval (CI) for the mean adjusted difference between the groups was calculated. If a significant difference was detected, post hoc tests with Bonferroni adjustment were conducted, so only P values less than .017 were considered statistically significant. The effect size was calculated as f value using the following formula:

where SSb is the interaction sum of squares from the ANCOVA summary table and SSe is the within-subjects error sum of squares. Criteria for judging the estimated effect size were as follows: a large effect size was .40 or more, a medium effect size was .25 to .39, and a small effect size was .10 to .24. 30
Results
The participant flow chart is presented in Figure 2. In total, 44 children were screened for eligibility, and 8 children were excluded for various reasons. As a result, 36 children were included and evenly assigned to the PSE group and the no-music group. Three children withdrew during the training period, leaving 17 children in the PSE group and 16 children in the no-music group who had completed the 12-week follow-up. No significant differences of baseline characteristics between the 2 groups were detected (Table 1).
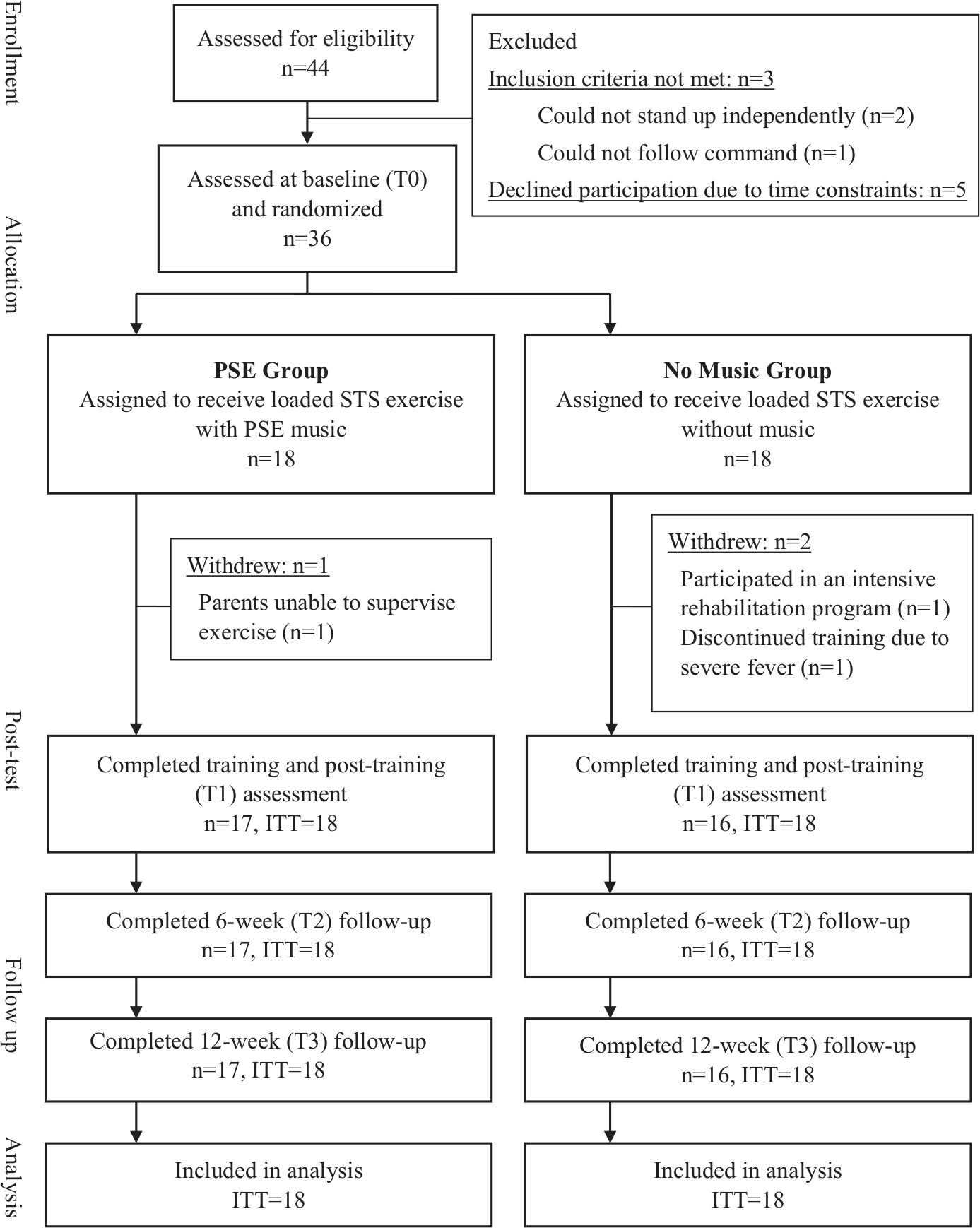
Flow diagram of participants through study.
Baseline Characteristics a .
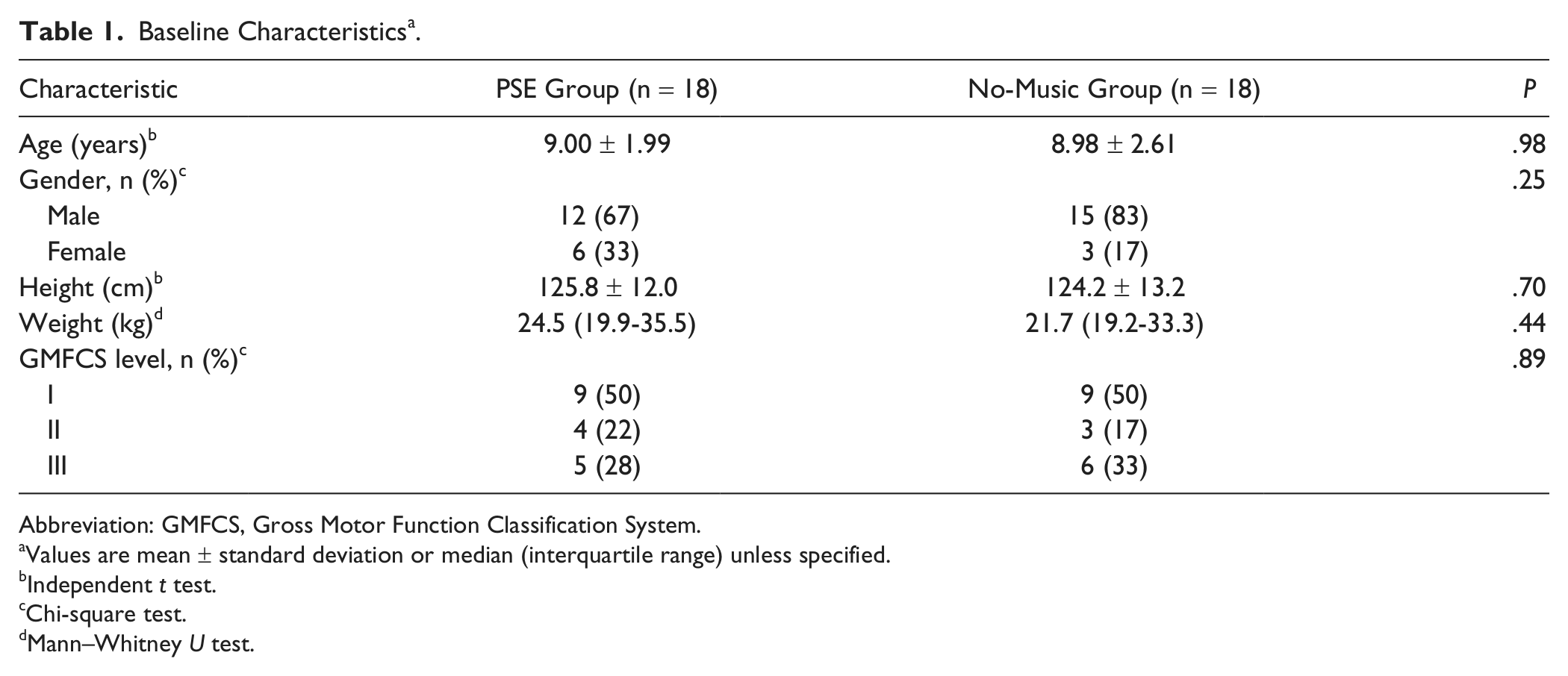
Abbreviation: GMFCS, Gross Motor Function Classification System.
Values are mean ± standard deviation or median (interquartile range) unless specified.
Independent t test.
Chi-square test.
Mann–Whitney U test.
Primary Outcomes
Table 2 shows the observed and adjusted GMFM score means at 4 time points. For both groups, significant main time effects of GMFM scores were found from T0 to T1, T0 to T2, and T0 to T3 in Dimension D (F = 8.9-32.2, P ≤ .005), E (F = 6.4-16.4, P ≤ .016), and Goal dimension (F = 12.7-28.3, P ≤ .001). Additionally, significant group by time interactions were found in Dimension D at T1 (P = .004, mean adjusted difference = 3.6) and T2 (P = .004, mean adjusted difference = 3.8) with greater improvements in the PSE group than in the no-music group. However, the music effects did not maintain at T3 (P = .06). For the Goal score, significant interactions were found at T1 (P < .001), T2 (P = .004), and T3 (P = .013). There was no significant interaction in the Dimension E (P ≥ .04).
Observed and Adjusted Means for Gross Motor Outcome Measures.
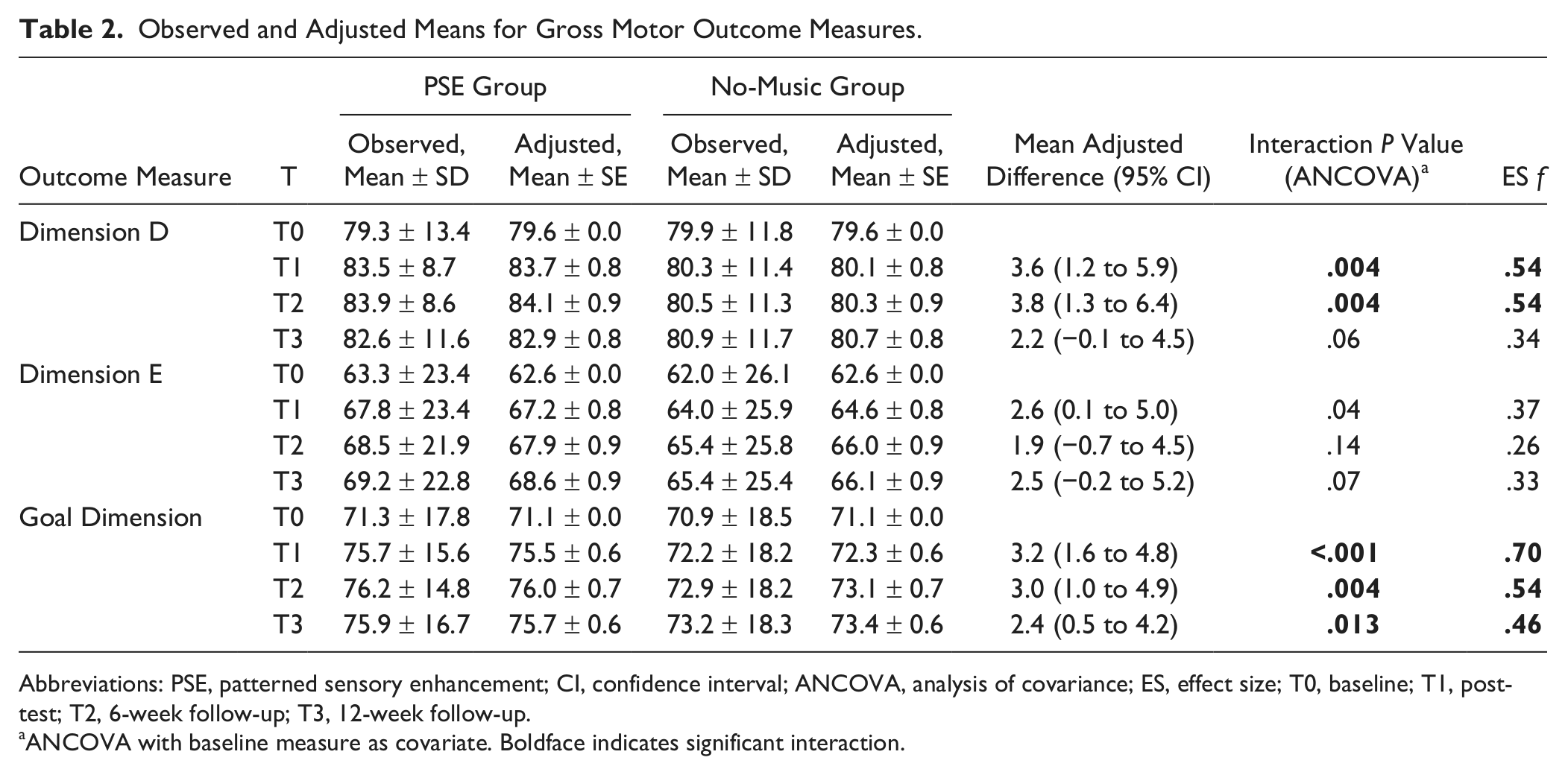
Abbreviations: PSE, patterned sensory enhancement; CI, confidence interval; ANCOVA, analysis of covariance; ES, effect size; T0, baseline; T1, posttest; T2, 6-week follow-up; T3, 12-week follow-up.
ANCOVA with baseline measure as covariate. Boldface indicates significant interaction.
Secondary Outcomes
Table 3 shows that the scores of Functional Skills Scale of PEDI mobility domain increased in both groups from T0 to T1, T0 to T2, and T0 to T3, resulting in significant main effects of time (F = 9.4-12.6, P = .001-.004). However, there was no significant interaction (P = .04-.12). The Caregiver Assistance Scale of PEDI mobility domain did not improve significantly in both groups. For the self-care domain, the Functional Skills Scale improved in both groups from T0 to T2 and T0 to T3 (F = 9.5-13.0, P = .001-.004), but not from T0 to T1 (P = .04). The Caregiver Assistance Scale showed no significant main effects of time. However, significant interaction effect from T0 to T3 (P = .005, mean adjusted difference = −6.6) with greater improvements in the no-music group was found.
Observed and Adjusted Means for PEDI Daily Mobility and Self-care Functions Measures.
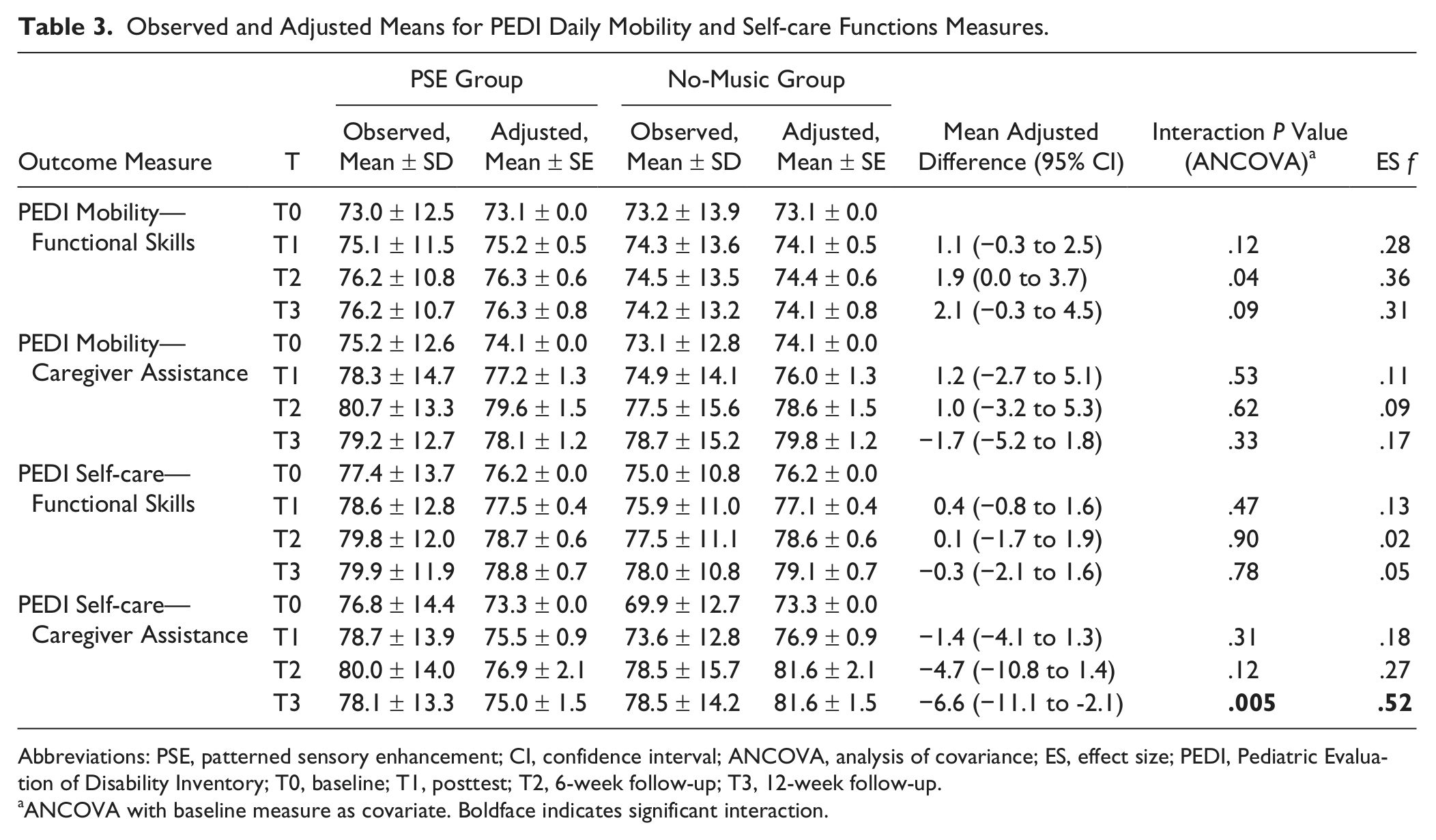
Abbreviations: PSE, patterned sensory enhancement; CI, confidence interval; ANCOVA, analysis of covariance; ES, effect size; PEDI, Pediatric Evaluation of Disability Inventory; T0, baseline; T1, posttest; T2, 6-week follow-up; T3, 12-week follow-up.
ANCOVA with baseline measure as covariate. Boldface indicates significant interaction.
As shown in Table 4, values of 1-RM of STS increased in both groups, resulting in significant main effect of time at all time points (F = 11.3-15.6, P ≤ .002), but no interaction was found (P = .06-.15). Two PSE-group children did not have 10-meter-walk data. Results of 2 × 4 ANCOVA from the rest of the participants showed a significant main effect of time (P = .02). However, post hoc analysis did not find any significant main effects of time in both groups (P = .02-.05).
Observed and Adjusted Means for Functional Strength Measures and Walking Speed.
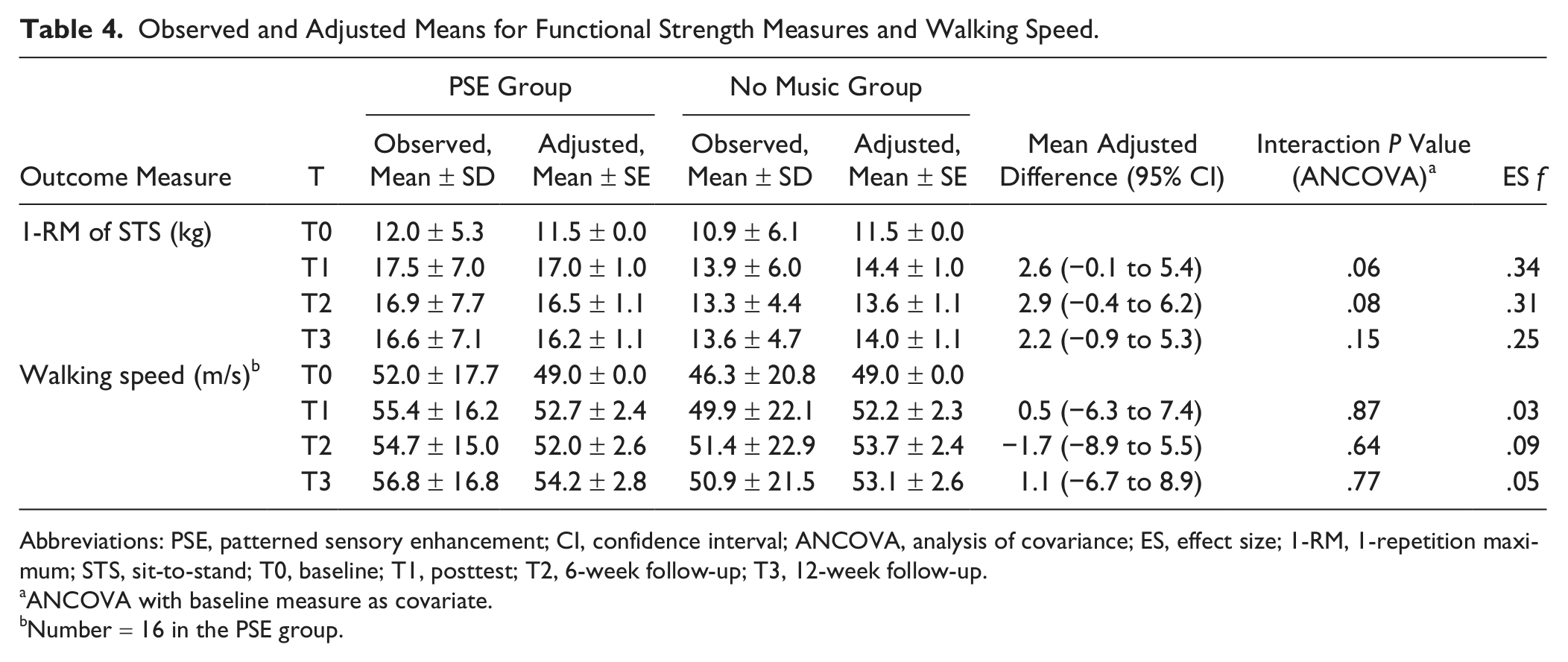
Abbreviations: PSE, patterned sensory enhancement; CI, confidence interval; ANCOVA, analysis of covariance; ES, effect size; 1-RM, 1-repetition maximum; STS, sit-to-stand; T0, baseline; T1, posttest; T2, 6-week follow-up; T3, 12-week follow-up.
ANCOVA with baseline measure as covariate.
Number = 16 in the PSE group.
Compliance and Adverse Events
Although the majority of participants followed the training protocol, 3 PSE-group children and 2 no-music-group children had discontinued the exercise for 1 week and allowed an 1-week extension before T1 assessment because of vacation (n = 2), influenza illness (n = 1), ankle sprain unrelated to the exercise regimen (n = 1), and school final examination (n = 1). According to the exercise log during the training period, PSE-group children completed an average of 17.8 sessions (range = 14-21) and 25.2 min/session (SD = 10.1 minutes) with median repetitions performed under 50% of 1-RM STS load of 73 (interquartile range = 45-84). The mean exercise load increased from 6.1 to 7.6 to 8.8 kg (range = 1-14 kg) every 2 weeks. Children in the no-music group completed an average of 17.7 sessions (range = 10-22) and 26.9 min/session (SD = 7.2 minutes) with median repetitions of 60 (interquartile range = 45-78) and mean load from 5.7 to 6.4 to 7.0 kg (range = 1-12.75 kg).
During the training period, 2 PSE-group children reported mild bruises on anterior thigh resulting from load weight hitting the thigh while sitting down. Modification by adding extra cushions under the weight and encouraging the children to sit down with control prevented further discomfort. One no-music-group child reported right knee pain at week 5 and was instructed to lessen training weight to the previous level. Seven PSE-group children (41%) and 8 no-music-group children (50%) had reported mild soreness occasionally over thigh, shoulder, and back. Most soreness disappeared within a few hours after ceasing exercise. Soreness in a few subjects dissipated after 3 to 5 days.
Discussion
This is the first randomized controlled trial investigating the combination effects of PSE music and resistance exercise for children with spastic diplegia. The results suggest that after training, children who exercised with PSE music had statistically significant improvements in gross motor capacity than those without music, and such effects could last at least 3 months; however, the PSE music did not achieve statistically significant improvements in participants’ daily functioning, strength, and walking speed.
Disturbed motor ability is a common challenge for children CP. 1 Most motor activities, such as standing up from a chair, squatting and standing to retrieve something from the floor, and going up or down stairs, require good muscle strength, balance, and motor control. The loaded STS exercise provides a great opportunity to develop lower extremities muscle strength to arise from a chair, dynamic balance ability to transit from a large base of support to a smaller one, and the motor control ability to regulate horizontal to vertical movements. 31 Since children with spastic diplegia usually stand up with a slower pace than children developing typically and have difficulties in converting flexion momentum into vertical momentum,3,32 the PSE music was designed to facilitate faster movement with earlier seat-off. A previous study demonstrated that adding PSE music to the repetitive loaded STS could immediately shorten the movement time, increase the extensor power of lower extremities, and improve smoothness of center-of-mass trajectory in children with spastic diplegia compared to the no-music condition. 22 It is believed that PSE music had similar effects on motor control and resulted in the improvement of GMFM scores in the PSE group.
It is well known that music can facilitate synchronized motor responses. Most studies in the field of neurologic music therapy investigate the effects of rhythmic auditory stimulation to improve gait pattern in people with stroke, Parkinson’s disease, and CP.20,33,34 The auditory rhythm was applied as an external timekeeper to entrain the movement frequency of a continuous task and guide movement through anticipatory cueing, where the movement is rhythmic in nature such as gait.33,35 However, the STS movement is a discrete task 31 and could be cued by rhythm as well as by pitch, melody, and loudness. The PSE music showed an effect to improve the motor capacity in the current study. Similar results were found for older adults that the self-composed PSE music with functional exercises could improve 1-leg standing balance and walking speed. 29
Although improvised music was generally recommended while applying music therapy since it could reflect subtle variations and produce most fitting music, 21 prerecorded therapeutic music based on an individual’s above-average performance has been proven to be effective and practical. 36 The recorded PSE music could help children replicate their best loaded STS movement and increase the stability of each movement in a repetitious exercise. 22 Results of this current study showed that recorded music specifically tailored to an individual and adjusted on a regular basis to reflect the change of movement is both cost-effective and clinically feasible.
Music has the potential to help children feel less fatigued and more motivated during resistance exercise. Numerous studies have supported the use of music to distract discomforting feelings and increase motivation during exercise.10-12 Observations revealed that PSE-group children performed more STS repetitions in a shorter duration, were more concentrated during training, and were more willing to carry on the exercise than no-music-group children. The psychological effects of music might also explain the improvements in GMFM found in the PSE group.
The PSE group did not significantly increase PEDI scores more than the no-music group. Smaller effect size found in the daily function outcomes showed that not all improvements in motor capacity brought by PSE music were translated into capability (PEDI Functional Skills Scale) and performance (PEDI Caregiver Assistance Scale). The relationships between capacity, capability, and performance are complex37,38 and influenced by environmental and personal factors.37,39 In addition to improved motor capacity through exercise with PSE music, changes in caregivers’ attitude, environment, and routines are also important to foster children’s independence in daily life. The small sample size might also limit the possibility to detect differences in daily functional outcomes. Since the sample size was estimated based on motor capacity measures in Hamburg and Clair’s study, 29 it is suggested that more subjects are needed in future studies to clarify the effects on daily function.
To our surprise, the no-music group had much improvement on Caregiver Assistance Scale of the PEDI self-care domain than the PSE group at the 3-month follow-up, although no time effects were found. Since the improvement was only found at 12-week follow-up, the improvement might not be totally related to the intervention. The changes of the degree of caregiver assistance might not only result from children’s capabilities but also from the academic demands, weather, and caregivers’ attitudes toward self-care. It was observed that parents rated self-care performance higher during summer vacation and lower during winter and school final examination period.
Although there were no differences in other PEDI scores between the 2 groups, there were still significant main effects of time in the Functional Skills Scales of PEDI mobility and self-care domains in this study. A literature search revealed that this is the first study to investigate the effects of functional resistance exercise on daily activities and participation for children CP that yielded relatively positive results.
For all children as a whole, the muscle strength of lower extremities improved significantly after the loaded STS exercise. Although the PSE group did not have significantly more muscle strength gain than the no-music group, medium effect sizes (.25-.34) were found at posttest and follow-ups. The medium effect sizes implied that the PSE music had some contributions to exercise training because PSE-group children tended to be more cooperative and performed more repetitions during the exercise.
Significant main time effect was found in the walking speeds, but the differences were no longer significant with a more conservative criterion in the post hoc tests. The result showing that the loaded STS exercise might improve gait speed is different from our previous study. 6 One possible explanation is that children in the current study included children with lower motor function (GMFCS level III) and slower walking speeds than those in the earlier study. These children might benefit more from resistance exercise than those with milder disabilities.
The current study did not compare the effect between PSE music and general background music because the primary assumption was that music would guide better movement form and sequence than exercise without music. However, previous studies have reported that synchronous music showed the same or better effects than asynchronous music during exercise for healthy people.10,40,41 In the future, differences between PSE and background music should be investigated while controlling the perceived motivational qualities of music. 42
There were several limitations in this study. First, there was large variability within the target population in terms of age and level of severity. Furthermore, a small sample size may decrease the power to detect statistical differences. Second, the results of the current study could only apply to children with spastic diplegia who could stand up independently. Since various patterns of assisted STS movements were found, future study may investigate effects of PSE music with different characteristics to guide these movements. 43 Third, the resistance program of this study did not follow the guidelines suggested by the National Strength and Conditioning Association. 44 Instead, the protocol of this study was based on previous evidence 6 and one unpublished pilot study, which found that loaded STS exercise with high loads resulted in poor compliance and low motivation at home. Fourth, this was a single-blind study where only the assessors did not know children’s treatment allocations but children and their parents did. It is possible the PSE-group-children might be psychologically encouraged to perform better in the posttraining assessments. Exercise compliance and motivation could also be influenced by parents’ expectancy. Telerehabilitation, which used webcams to deliver home exercise by therapists, could ensure that the exercise will be carried out more consistently in the future.
The current study showed that it is feasible to provide PSE music for children with spastic diplegia while doing the loaded STS exercise. The positive result encourages application of neurologic music therapy in children with CP to improve their functional movements.
Footnotes
Appendix
Authors’ Note
Presented in part to the 7th World Congress for NeuroRehabilitation, May 16-19, 2012, Melbourne, Australia; and the 16th World Confederation for Physical Therapy Congress, June 20-23, 2011, Amsterdam, Netherlands.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Science Council in Taiwan (Grant No. NSC98-2314-B-002-011-MY3).