
Abstract
Background. To explore whether a polymorphism in dopamine metabolism influences the effectiveness of neurological rehabilitation and the outcome after ischemic stroke. Methods. The Barthel Index (BI) and the Rivermead Motor Assessment (RMA) were assessed in 78 moderately affected stroke patients (1) after they had entered a neurological inpatient rehabilitation, (2) after 4 weeks of rehabilitation therapy, and (3) 6 months later. Polymorphisms of the gene encoding catechol-O-methyltransferase (COMT) were determined. BI and RMA results were analyzed with respect to the genetic profiles of COMT. Results. Carriers of COMT Val/Val alleles showed better results in BI and RMA than COMT Met/Met carriers at all 3 time points. Val/Met carriers exhibited results in between the homozygotes, suggesting a gene–dose relationship. Altogether, BI and RMA results were highly correlated. Conclusion. Stroke patients with COMT Val/Val alleles had higher motor functions and abilities of activities of daily living even at the beginning of the rehabilitation period. All patient groups improved during the rehabilitation period to a similar degree, suggesting that physical therapy is comparably effective in all polymorphism subtypes.
Introduction
Stroke is the most frequent disorder of the central nervous system and affects about 200 000 persons per year in Germany. The outcome depends on a number of variables among which age, the size of the brain lesion, the severity of symptoms at disease onset, the severity of damage to the corticospinal tract, glucose levels, early start of rehabilitation treatment, and the presence of cognitive and neuropsychological impairments are the most common.1,2 In patients with a subarachnoid hemorrhage a genetic factor, the polymorphism in the gene that encodes for the brain-derived neurotrophic factor (BDNF), was found to influence the outcome. 3 In our study, we were interested whether polymorphisms in the catechol-O-methyltransferase (COMT) gene modulate the outcome of patients with an ischemic stroke.
Catechol-O-methyltransferase is an enzyme that influences the availability of dopamine in the synaptic cleft by stimulating its degradation. 4 Dopamine is an important neurotransmitter in the reward and executive system and has a major influence in motor learning. Application of dopamine improved cognitive functions5,6 and motor functions in healthy subjects7,8 and also in stroke patients.9,10
In the COMT gene, position 158 either carries valine or methionine. In Europe and the United States of America, the Val/Val and the Met/Met polymorphisms in this gene are each found in about 25% of the population. The Val/Met combination is the most frequent polymorphism and can be found in about 50% of the population. 11 The Val allele is associated with higher enzyme activity, thus inducing a faster degradation of dopamine and a lower dopamine concentration in the synaptic cleft (for review, see Witte and Flöel 12 ). In carriers of the Met/Met polymorphism, COMT showed a lower thermostability and a lower enzyme activity, leading to higher dopamine levels in the synaptic cleft. It was shown repeatedly that Met 158 allele carriers displayed better executive functions, and had larger working memory capacities, better episodic memory retrieval, and a higher level of attention in reaction time tasks than Val 158 allele carriers.13,14 But this population also showed more disorganized personality features. 15 On the other hand, carrying a Val 158 allele was associated with improved ability to verbalize emotions, with an improved sustained attention 16 and with a higher cognitive flexibility.17,18
Our aim was to find out whether the outcome after an ischemic stroke and, in particular, the effectiveness of neurological rehabilitation, would differ according to the COMT gene polymorphism.
Methods
Patients
We included 83 patients (mean age, 68.7 years; 30 women; 45 left-sided hemiparesis) with a recent ischemic stroke (mean duration since stroke onset, 19 days). All patients gave informed consent and the study was approved by the ethics committee of the University of Constance. Inclusion criteria were a first ischemic stroke less than 3 months prior to study inclusion and a Barthel Index (BI) of less than 80 points at admission into the rehabilitation hospital. Exclusion criteria included aphasia, apraxia, dementia, recurrent stroke, intracranial hemorrhage, diseases of the spinal cord, peripheral nerves or muscles, severe diseases of heart, lung, liver, or kidneys, and conditions that might interfere with the understanding of instructions or the ability to give consent. All patients participated in an inpatient rehabilitation program. In all patients, computed tomography or magnetic resonance imaging of the brain had been performed to ensure the diagnosis of an ischemic stroke. Further details are provided in Table 1. Patients were included in the study within the first 7 days after admission to the hospital. A total of 3 clinical examinations were performed as follows: immediately after inclusion in the study, 4 weeks later, and 6 months later. Clinical testing comprised a neurological examination, the BI, and the Rivermead Motor Assessment (RMA). During the rehabilitation period, a blood sample was taken and sent to the laboratory to determine the COMT genotype. The study was double blind. Clinicians did not know the COMT polymorphism pattern, and the laboratory did not know the results of the clinical testing or the patient’s name.
Clinical Characteristics of the Patient Group.
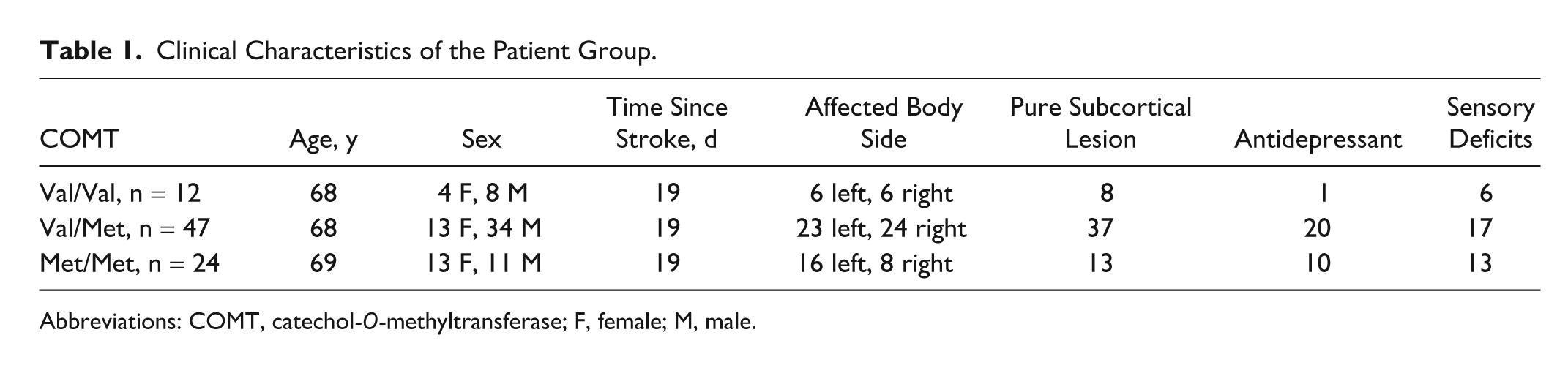
Abbreviations: COMT, catechol-O-methyltransferase; F, female; M, male.
The rehabilitation program was adapted to the individual needs and goals of each patient. In the majority of patients, mobility and the ability to regain independent walking were the most relevant aims. The treatments consisted of physiotherapy, occupational therapy, endurance training, and strength training. The amount of therapies per week was almost identical for all patients.
Statistical Analysis
Patients were analyzed in relation to their COMT polymorphism. We used analysis of variance (ANOVA) calculations with the between-subject factor “GROUP” (3 levels—Val homozygote, Met homozygote, heterozygote) and the within-subject factor “TIME” (3 levels) for each functional measurement (BI, RMA gross function, RMA leg and trunk function, RMA upper extremity function) separately. We also performed ANOVAs to test whether the polymorphism groups differed according to the clinical presentation (age, sex, time after stroke, affected body side, type of lesion, presence of sensory deficits, intake of antidepressants). If an ANOVA revealed significant differences, post hoc paired t tests with a Bonferroni correction were performed. The level of significance was assumed at 5%.
Rivermead Motor Assessment
The RMA allows testing of a variety of motor functions and is subdivided into 3 main aspects: gross, leg and trunk, and upper extremity functions. Each of the 3 subtests is a reliable and responsive measurement of motor function. 19 The RMA has been applied in numerous studies.20-24 As a general rule, the assessment contains tasks with increasing difficulty and complexity. As soon as the subject is unable to complete 3 consecutive tasks, the assessment is finished. For gross function, the scale consists of 13 items. These items mainly test transfer and walking abilities of increasing difficulty and complexity. For leg and trunk function there are 10 items. They test leg functions in lying and standing position. Upper extremity assessment consists of 15 items. These start with simple proximal movements and finish with tasks requiring good dexterity.
Barthel Index
The BI is a 10-item instrument that measures functional independence in personal activities of daily living. The items include the assessment of feeding, moving from wheelchair to bed, personal toilet, getting on/off toilet, bathing, walking on level surface, ascending/descending stairs, dressing, and controlling bladder and bowels. The BI is quick and easy to complete. It is one of the most frequently used assessments and has been shown to have good reliability and validity. Responsiveness is limited, in particular for very small and very severe deficits (for review, see Quinn et al 25 ). Several studies have compared BI and Functional Independence Measure and have found a good responsiveness for both26,27 and a high correlation between them. 28
Genotyping Technique
Genomic DNA was extracted from venous blood samples, using the GenElute DNA extraction kit (Sigma, St. Louis, Missouri). Genotyping of DNA fragments containing the COMT Val108/158Met polymorphism (human chromosome 22q11; GenBank accession number Z26491) was performed using standard polymerase chain reaction methods (for detailed protocols, see Schott et al 29 ).
The COMT genotype was determined by digesting polymerase chain reaction products with NlaIII at 37°C for 3 hours. This yielded 3 fragments (114, 70, and 54 bp) for the Val allele and 4 fragments (96, 70, 54, and 18 bp) for the Met allele. The restriction fragments were separated on an ethidium bromide–stained agarose gel (4.5%), and visualized under ultraviolet light. The Val and Met alleles were determined by the presence of a 114-bp fragment and a 96-bp fragment, respectively.
Results
Patient Characteristics
Twelve patients had Val/Val alleles, 47 patients showed a Val/Met polymorphism, and 24 patients carried the Met/Met polymorphism. There were no significant differences between these 3 groups regarding age, sex distribution, time since stroke occurrence, paretic body side, infarct localization (subcortical infarcts vs infarcts with cortical involvement), presence of sensory deficits, and intake of an antidepressant drug during the study period. Further details are presented in Table 1. The number of dropouts at the follow-up examination was low. Five patients could not be tested after 6 months. Two had died, the other 3 were still too severely affected to be transported to our hospital. One belonged to the group with Val/Val polymorphism, 3 carried a Val/Met polymorphism, and 1 belonged to the Met/Met polymorphism group. For statistical analysis, only those patients who had participated in all examinations (n = 78) were analyzed.
BI Results
The ANOVA result indicated that the 3 groups differed significantly in their BI values, F(1, 233) = 6.64; P = .002. BI values measured at the 3 time points also differed significantly, F(1, 233) = 74.4; P < .001. However, there was no interaction between the factor “TIME” and the factor “GROUP.” A post hoc Bonferroni-corrected analysis indicated that patients with Val/Val polymorphism differed significantly from patients with Met/Met polymorphism (P = .014) and Val/Met carriers were significantly different from Met/Met carriers (P = .005). No difference was observed between the BI values of Val/Val and Val/Met polymorphism carriers (P = .91). See Figure 1.
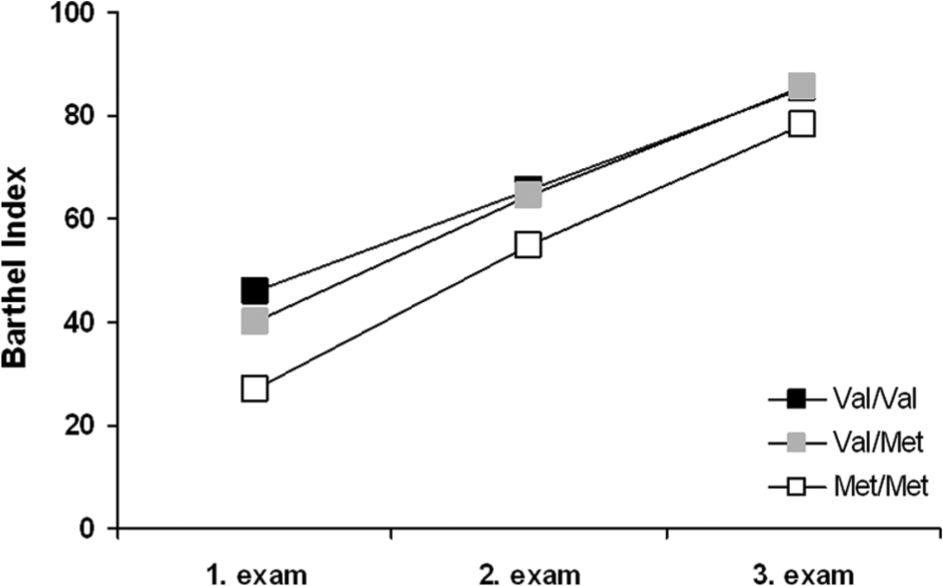
Changes of the Barthel Index in relation to the catechol-O-methyltransferase (COMT) polymorphism. 1. Examination immediately after study inclusion; 2. examination 4 weeks later; 3. examination 6 months later; for statistical significances, see Results section.
Rivermead Motor Assessment
Gross Function RMA
The ANOVA showed a significant difference for the factor “GROUP,” F(1, 233) = 5.77; P = .004, and for the factor “TIME,” F(1, 233) = 51.7; P < .001, but no significant interaction. A post hoc Bonferroni- corrected analysis showed a significant difference between Val/Val and Met/Met carriers (P = .003) and trends for the difference between Val/Val and Val/Met carriers (P = .108) and between Val/Met and Met/Met carriers (P = .147). See Figure 2.
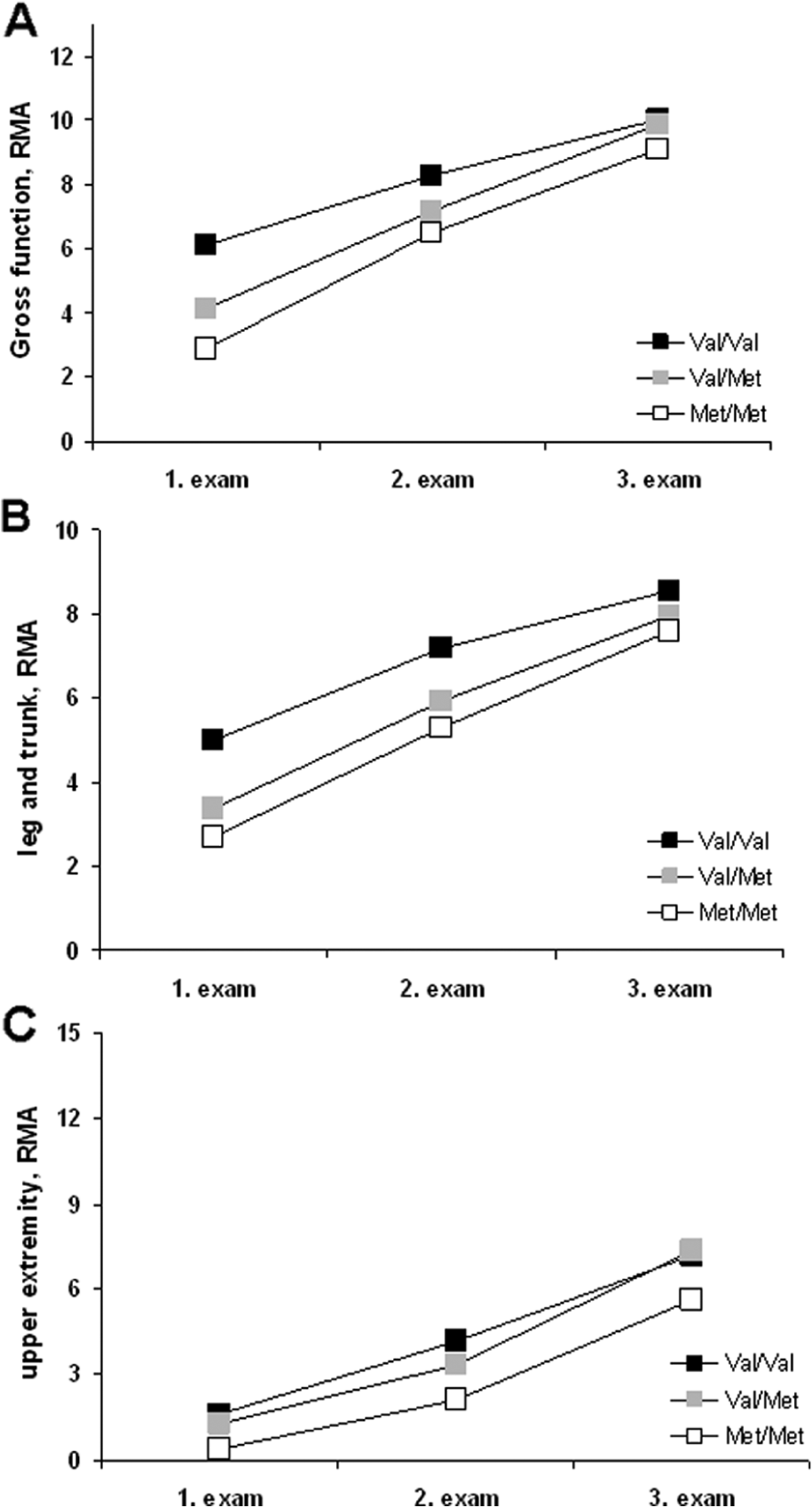
Changes of 3 scales of the Rivermead Motor Assessment (RMA) in relation to the catechol-O-methyltransferase (COMT) polymorphism. (A) Gross functions of the RMA. (B) Leg and trunk function of the RMA. (C) Upper extremity function of the RMA. 1. Examination immediately after study inclusion; 2. examination 4 weeks later; 3. examination 6 months later; for statistical significances, see Results section.
Leg and Trunk RMA
The ANOVA showed a significant difference for the factor “GROUP,” F(1, 233) = 3.68; P = .027, and a significant difference for the factor “TIME,” F(1, 233) = 31.5; P < .001, but no significant interaction. A post hoc Bonferroni-corrected analysis showed a significant difference between Val/Val and Met/Met carriers (P = .022) and a trend for the difference between Val/Val and Val/Met carriers (P = .087) but no difference between Val/Met and Met/Met carriers (P = .984).
Upper Extremity RMA
The ANOVA showed a significant difference for the factor “GROUP,” F(1, 233) = 4.42; P = .013, and for the factor “TIME,” F(1, 233) = 46.8; P < .001, but no significant interaction. A post hoc analysis indicated significant differences between Val/Val and Met/Met carriers (P = .047) and between Val/Met and Met/Met carriers (P = .038) but no difference between Val/Val and Val/Met carriers (P = .98).
There was a significant correlation between BI and RMA across all time points: Pearson’s correlation coefficient = 0.881 (P < .001).
Discussion
The main result of this study, which was conducted in a rehabilitation center, is that the outcome after ischemic stroke was related to the polymorphism of the COMT gene. Patients with Val/Val alleles had higher scores in assessments that focus on motor functions and activities of daily living than carriers of a Met/Met genotype. Results of Val/Met carriers were in between the other 2 groups, suggesting a dose–response relationship. The difference between Val carriers and Met carriers was already present at the first time point of data collection, persisted during the 4 weeks of inpatient rehabilitation and was still noticeable 6 months later. Thus, improvements of motor functions occurred in all groups to a similar degree, indicating that a clinical benefit through intense rehabilitation is independent of the COMT polymorphism.
The difference between Val and Met carriers was already present in the first assessment of functions. Therefore, it must have developed even before the patient entered the study. We carefully examined whether other factors known to influence the outcome after stroke could have been the reason for this but did not find differences regarding age, sex, time since stroke, affected body side, type of stroke (subcortical or cortical), impairment of sensory functions, and ingestion of an antidepressant. Therefore, the reason for the difference is unclear and deserves further investigation. In particular, future studies should include patients immediately after stroke to explore whether this difference is already present within the first hours after stroke or whether early recovery within the first days poststroke might be more pronounced in patients with Val/Val alleles. In our nonselected patient group, the proportion of Val/Val carriers was lower than expected based on the distribution of the polymorphism in the general population. We had expected to find a 25% fraction of Val/Val carriers but in fact only 15% of the patient group belonged to this polymorphism. Since our patient group is too small to be representative of a population, it cannot be determined whether this low proportion of Val carriers is incidental or does reflect a real asymmetrical distribution in a stroke patient population. In the latter case, however, it might suggest that the Val/Val polymorphism either protects against a stroke or is associated with a more rapid motor recovery leading to a smaller proportion of patients that needs inpatient rehabilitation. These questions can only be answered when a sufficiently large number of stroke patients in the acute phase are studied. It may also be speculated that the higher cognitive flexibility found in Val allele carriers could contribute to the higher test scores.17,18,30 Another possibility might be that relatively elevated levels of dopamine and catecholamines in Met allele carriers might not be beneficial early after stroke. At least in patients post bypass surgery, the Met allele was associated with a higher frequency and longer duration of vasodilatatory shock. 31
We do not think that our results can be attributed to a selection bias since all patients that had been consecutively transferred to our hospital from various other hospitals and had met the inclusion criteria had been included in our study. Thus, there was no selection of patients except for the degree to which they had been affected at the time of admission. We had excluded patients with small deficits because, in these patients, we did not expect to observe relevant changes of BI and RMA during the course of rehabilitation. Our blinding (clinicians only learned about the genetic profile after patients had completed the clinical examinations and BI and RMA tests) also argues clearly against a selection bias.
In our study, BI and RMA showed a very similar course and were highly correlated. The result suggests that 1 of the 2 scales is sufficient to detect changes of (motor) functions during recovery from stroke.
It has been shown recently that the antidepressant fluoxetine, a serotonin reuptake inhibitor, has a positive effect on motor recovery after stroke. 32 Mikami et al 33 concluded that patients treated with antidepressants had better recovery from disability by 1-year poststroke than patients who did not receive antidepressant therapy. This effect was independent of depression. Our patients did not receive an antidepressant to improve motor functions but only if a clinically relevant depression had been diagnosed. In this study, Val/Val carriers were less frequently treated with an antidepressant than Val/Met and Met/Met carriers. The difference was a nonsignificant trend but nevertheless allows us to draw 2 conclusions: On one hand, the higher motor functions of Val/Val carriers cannot be attributed to the effect of an antidepressant and on the other hand, it might indicate that Val/Val carriers were less frequently depressed after stroke than Met carriers. A recent publication has shown that healthy Val carriers had much lower sadness scores than Met carriers. It was therefore postulated that this constitutes a resilience factor against depression. 34 In future studies, the relationship between COMT polymorphism and poststroke depression should be explored more systematically by appropriate questionnaires and in a larger group of patients.
Two other studies have investigated a relationship between genetics and recovery after stroke. Manso et al 35 explored the association of variants in the BDNF, fibroblast growth factor 2, and vascular endothelial growth factor A genes with functional outcome after stroke. The authors did not find an effect of a single gene, but described 2 gene–gene interaction models as being associated with stroke outcome. Another recent study described an influence of the ApoE ϵ4 polymorphism on recovery after stroke but did not find a relevant effect of BDNF polymorphism. 36
In summary, our results indicate a possible influence of the COMT polymorphism on outcome after stroke but not on the effectiveness of the neurological inpatient rehabilitation. These results should be replicated in a larger group of stroke patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.