
Abstract
Background. Low physical activity levels in persons with multiple sclerosis (MS) may reduce skeletal muscle oxidative capacity. Rehabilitation strategies might be altered by a measure of capacity that did not require invasive techniques or maximal exercise testing. For this purpose, we measured exercise onset and offset oxygen uptake (Vo2) kinetics during endurance exercise. Objective. This study compared exercise-onset and -offset Vo2 kinetics in mildly affected persons with MS with healthy matched participants. Methods. From 38 MS patients who had a mean Expanded Disability Status Scale of 3.1 and 16 healthy participants, exercise-onset and -offset Vo2 kinetics (mean response time [MRT]) were determined during two 6-minute submaximal bouts of exercise separated by a 6-minute recovery interval. Blood lactate, heart rate, expiratory volume, and Borg ratings of perceived exertion were assessed during exercise and compared between groups. Relationships between clinical characteristics and MRT were assessed. Results. During exercise, blood lactate, heart rate, and expiratory volume did not differ between groups (P > .05), but exercise-onset MRT was significantly slower in MS versus healthy participants (P = .007). Exercise-onset MRT was independently related to having MS (P = .02). Exercise-offset MRT was not different between groups or was independently related to having MS (P > .05). No independent relationships between clinical characteristics of MS and exercise-onset or -offset MRT were found. Conclusions. Exercise-onset Vo2 kinetics during submaximal endurance exercise are significantly slowed in mildly disabled persons with MS, suggesting low skeletal muscle oxidative capacity. Using mean response time testing, rehabilitation interventions for this reduction in exercise capacity can be assessed and targeted.
Keywords
Introduction
Many persons with multiple sclerosis (MS) have a reduced exercise capacity. 1 Although the mechanisms for this low capacity remain moot (central vs peripheral factors),2,3 this might in part be a consequence of chronically low physical activity. 4 Indeed, long-term exercise interventions significantly improve walking capacity in persons with MS. 5
A sedentary lifestyle ultimately leads to skeletal muscle adaptations. Studies indicate smaller type 1 skeletal muscle fiber diameter, lower succinate dehydrogenase activity, and complex 1 deficiency in skeletal muscle mitochondria with MS.6-8 Moreover, the phosphocreatine resynthesis rate after exercise is significantly slower compared with matched healthy controls. 9 These data point to a lowered oxidative capacity of skeletal muscle. These characteristics have been described by skeletal muscle biopsies analyses and by 31P magnetic resonance spectroscopy. For therapeutic interventions, it could be of value to assess skeletal muscle oxidative capacity during exercise in those with MS with noninvasive techniques and without the need of maximal exercise tests. Such assessment provides an indication of exercise tolerance and physical deconditioning, which is linked to disability level. 1 To examine skeletal muscle oxidative capacity during exercise in healthy subjects indirectly, exercise-onset and -offset oxygen uptake (Vo2) kinetics are often measured. 10 In this assessment, subjects exercise at a constant low to moderate exercise intensity (below anaerobic threshold) for at least 6 minutes with continuous monitoring of Vo2, after which the time needed to achieve a steady-state Vo2, or return to resting Vo2 after exercise, and its slope, is analyzed. During this test, at least 2 exercise bouts are executed with a few minutes of recovery between them. Then, the mean response time and time constant can be calculated. 11
Experimental evidence clearly indicates that exercise-onset Vo2 kinetics are significantly correlated with maximal Vo2 (r = −0.80, P < .05), 12 and that exercise-onset Vo2 kinetics are faster in skeletal muscle with predominantly slow-twitch fibers and with increased activation of oxidative muscle enzymes.13,14 Interestingly, exercise-onset Vo2 kinetics are significantly slowed in subjects with chronic diseases that are typically characterized by a lower exercise capacity, such as lung, 15 heart, 16 and metabolic diseases 17 , and are improved by exercise training. 18 In this context, it is generally accepted that assessing exercise-onset Vo2 kinetics is a sensitive tool for the specific evaluation of oxidative capacity of skeletal muscle. 19 As such, this noninvasive technique might be an appealing measure to assess skeletal muscle oxidative capacity in MS patients.
Exercise-offset Vo2 kinetics are, at least in part, determined by restoration of O2 stores in blood and muscle, resynthesis of adenosine triphosphate and creatine phosphate, lactate removal, and increased body temperature, circulation, and ventilation. 20 In persons with chronic diseases characterized by low exercise capacity, such as lung and heart disease, exercise-offset Vo2 kinetics are significantly slowed.21,22 However, it is uncertain whether training status and exercise training affects exercise-offset Vo2 kinetics.23,24 Therefore, it remains to be determined whether exercise-offset Vo2 kinetics truly reflect skeletal muscle oxidative capacity.
This study examined exercise-onset and -offset Vo2 kinetics in persons with mild MS when executing 2 subsequent endurance exercise bouts with similar intensity and duration, and compares these data with healthy subjects. We hypothesized that persons with MS would have significantly slower kinetics, pointing to impaired skeletal muscle oxidative capacity.
Methods
Subjects
Thirty-eight persons with MS and 16 healthy subjects were selected to participate in this study after responding to local advertisements. They were matched for age, gender, and body mass index. Those with MS had been diagnosed for at least 12 months (mean disease duration of 12 ± 10 years, range 2-48 years) and all subjects were sedentary (<2 hours of sports activities or exercise training per week). Participants were informed about the nature and risks of the experimental procedures before their written informed consent was obtained. This study was approved by the medical ethical committee of Hasselt University.
Study Design
This was a cross-sectional study. Results were revealed to the subjects after completion of the study. Following Expanded Disability Status Scale (EDSS) determination 25 and medication intake screening by a neurologist (in MS patients only), subjects underwent 2 experimental sessions. During the first experimental session, body composition and physical activity were determined. In the second experimental session, exercise-onset and -offset Vo2 kinetics were determined during 2 subsequent low- to moderate-intensity endurance exercise bouts. The primary outcome parameters in this study were the exercise-onset and -offset Vo2 kinetics. The secondary outcome parameters were body composition and physical activity.
Following body weight (mechanical column scale with beam, Seca, Birmingham, UK) and length assessment, segmental and total-body adipose tissue mass and lean tissue mass were determined using whole body dual X-ray absorptiometry (DXA; D-PXL, Lunar-GE, Madison, Wisconsin). 26 Daily physical activity, related to sports and recreational activities, household activities, transportation, labor activities, and sitting time, was evaluated by the 13-item Physical Activity Scale for Individuals with Physical Disabilities.27,28 From this questionnaire, the metabolic equivalent (MET) × hours/week was calculated.
Exercise Test
Subjects performed a cardiopulmonary exercise test on an electronically braked cycle ergometer (eBike Basic, General Electric GmbH, Bitz, Germany). Subjects were advised not to perform any exercise the day before or on the day of testing, and only to eat a light meal at least 2 hours prior to testing. Pulmonary gas exchange was continuously measured breath-by-breath with a mass spectrometer and volume turbine system (Jaeger Oxycon, Erich Jaeger GmbH, Germany). During the exercise test, oxygen uptake (Vo2, mL/min) and expiratory volume (VE, L/min) were assessed breath-by-breath, after which these data were averaged every 10 seconds. Heart rate was continuously monitored by 12-lead electrocardiograph device. Predicted maximal heart rate was calculated by 220 − age.
Following each exercise bout, capillary blood samples were obtained from the fingertip to analyze blood lactate concentrations (mmol/L), using a portable lactate analyzer (Accutrend Plus, Roche Diagnostics Limited, Sussex, UK). This portable analyzer has been shown to have excellent correlations with reference lactate analyzers. 29 At the end of each exercise bout, ratings of perceived exertion (RPE) was scored by the subject on a 6 to 20 Borg scale.
Subjects were seated on the bike for 3 minutes to obtain resting data. Next, subjects were instructed to cycle at a rate of 70 rpm, against a resistance corresponding to 25% (for MS patients) or 35% (for healthy subjects) of predicted cycling power output (Wmax), for 6 minutes. 30 After 6 minutes of cycling, subjects remained seated on the bike for an additional 6 minutes, after which a second 6-minute exercise bout was initiated. Predicted Wmax was based on gender, age, body weight, and height, and calculated by previously published formulae. 31 A higher cycling resistance was selected in the healthy subjects, as opposed to MS patients, because a higher exercise capacity was anticipated in the healthy controls, while the relative exercise intensity during exercise testing should be equal. After the first 5 healthy subjects had finalized their exercise test, the elicited exercise was checked to evaluate whether it was equal when compared with MS patients. Because this was the case, the selection of an exercise intensity at 35% of predicted maximal cycling power output was maintained.
Exercise-Onset Vo2 Kinetics
Exercise-onset Vo2 kinetics were calculated algebraically and expressed as mean response time (MRT). 11 The outcome parameter that is derived from this method correlates well with, and is not significantly different from, the time constant. 11 Resting Vo2 was calculated as the Vo2 during the final minute before exercise. Steady-state Vo2 was defined as the averaged value between the fifth and sixth minute of cycling. The difference between the rest Vo2 and steady-state Vo2 multiplied by exercise time (6 minutes) was defined as the expected amount of Vo2 during the entire exercise bout. However, to examine skeletal muscle oxidative capacity by calculating exercise-onset Vo2 kinetics, it is important to ignore the cardiodynamic phase of the kinetics. As a result, the first 20 seconds of data after onset of exercise were eliminated. 32 The sum of Vo2 above resting level was defined as the actually achieved Vo2 during the entire exercise bout. The oxygen deficit could then be calculated as follows: expected amount of Vo2 − actually achieved Vo2. Division of this oxygen deficit by the difference between rest Vo2 and steady-state Vo2 equals MRT. The resultant MRT multiplied by 60 finally produced a value expressed in seconds, and this outcome is used throughout this article to quantify exercise-onset Vo2 kinetics. Finally, the 2 MRTs that were obtained from the 2 exercise bouts were averaged.
Exercise-Offset Vo2 Kinetics
Exercise-offset Vo2 kinetics were calculated algebraically and expressed as MRT. End-recovery Vo2 was calculated as the Vo2 during the final minute of recovery. Resting Vo2 is defined as the Vo2 measured during the final minute before exercise. Steady-state Vo2 was defined as the averaged value between the fifth and sixth minute of cycling. The resting Vo2 multiplied by exercise time (6 minutes) was defined as the expected amount of Vo2 during recovery. As a result, the impact of resting metabolic rate for the proper calculation of exercise-offset Vo2 kinetics was eliminated. The sum of Vo2 above resting level during recovery was defined as the actually achieved Vo2 during recovery. The oxygen deficit could then be calculated as follows: expected amount of Vo2 − actually achieved Vo2. Division of this oxygen deficit by the difference between rest Vo2 and steady-state Vo2 equals MRT. The resultant MRT multiplied by 60 finally produced a value expressed in seconds, and this outcome is used throughout this article to quantify exercise-offset Vo2 kinetics. Only one MRT was obtained because recovery was monitored only once.
Statistical Analysis
All calculations were performed using the Statistical Package for the Social Sciences 15.0 (SPSS). Data are expressed as mean ± standard deviation. For non-time-dependent variable comparisons (between healthy subjects and MS patients), one-way analysis of variance or χ2 analysis was applied. To compare parameters in the first versus the second exercise bout in MS patients and healthy subjects, a paired-sample t test was used. Multivariate regression analysis was applied to examine relations between MRT (average of 2 exercise bouts for exercise-onset Vo2 kinetics, and one MRT for exercise-offset Vo2 kinetics; dependent variable) and subject group, age, gender, total-body adipose tissue percentage, and leg lean tissue mass in total group. Multivariate regression analysis was applied to examine relations between MRT (averaged of 2 exercise bouts for exercise-onset Vo2 kinetics, and one MRT for exercise-offset Vo2 kinetics) and age, gender, total-body adipose tissue percentage, leg lean tissue mass, EDSS score, MS type, and physical activity in MS patients. Univariate relationships between parameters were examined by Pearson correlation coefficients. Statistical significance was set at P < .05 (2-tailed).
Results
Subject Characteristics
Table 1 shows the characteristics of the participants. No significant differences in baseline were present. Trends for a lower total-body lean tissue mass (P = .06) and greater total-body (P = .06) and leg adipose tissue mass percentage (P = .08) were found in the sample with MS. Medications included beta-blocker (1 in MS, 1 in control), glatiramer acetate (5 in MS), natiluzimab (5 in MS), interferons (17 in MS), muscle relaxants (2 in MS), analgesics (8 in MS), and nonsteroid anti-inflammatories (2 in MS, 1 in control).
Subject Characteristics
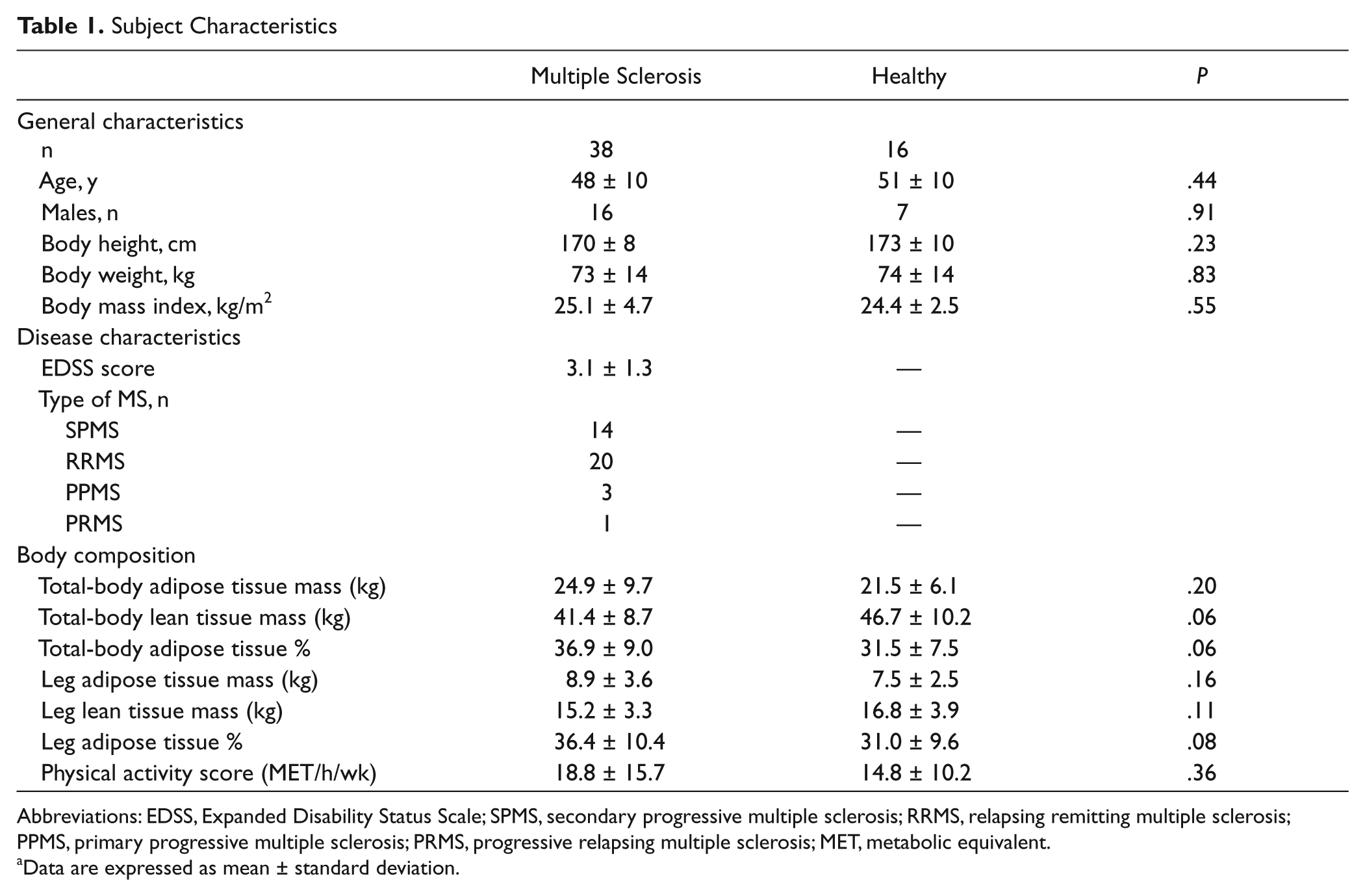
Abbreviations: EDSS, Expanded Disability Status Scale; SPMS, secondary progressive multiple sclerosis; RRMS, relapsing remitting multiple sclerosis; PPMS, primary progressive multiple sclerosis; PRMS, progressive relapsing multiple sclerosis; MET, metabolic equivalent.
Data are expressed as mean ± standard deviation.
Exercise Test Data
Exercise testing is shown in Table 2. As expected, the cycling power output was significantly higher in the healthy subjects versus MS patients (P= .001). During the first and second exercise bouts, heart rate (P = .29 and P = .48), percentage of predicted maximal heart rate (P = .25 and P = .46), expiratory volume (P = .51 and P = .33), and blood lactate content (P = .75 and P = .24) were similar between groups. Borg RPEs were significantly elevated during both exercise bouts in MS patients versus healthy subjects (P = .001 and P < .001). During the first exercise bout, trends for differences between groups were found for steady-state Vo2 (P = .07), and a significant difference between groups was found for magnitude of Vo2 (P = .04). During the second exercise bout, trends for differences between groups were found for steady-state Vo2 (P = .08). In MS patients, O2 deficit (P < .001), heart rate (P < .001), and RPEs (P = .02) were significantly different between exercise bouts (P < .05). In healthy subjects, O2 deficit (P = .03) and heart rate (P = .009) were significantly different between exercise bouts.
Exercise Test Data a
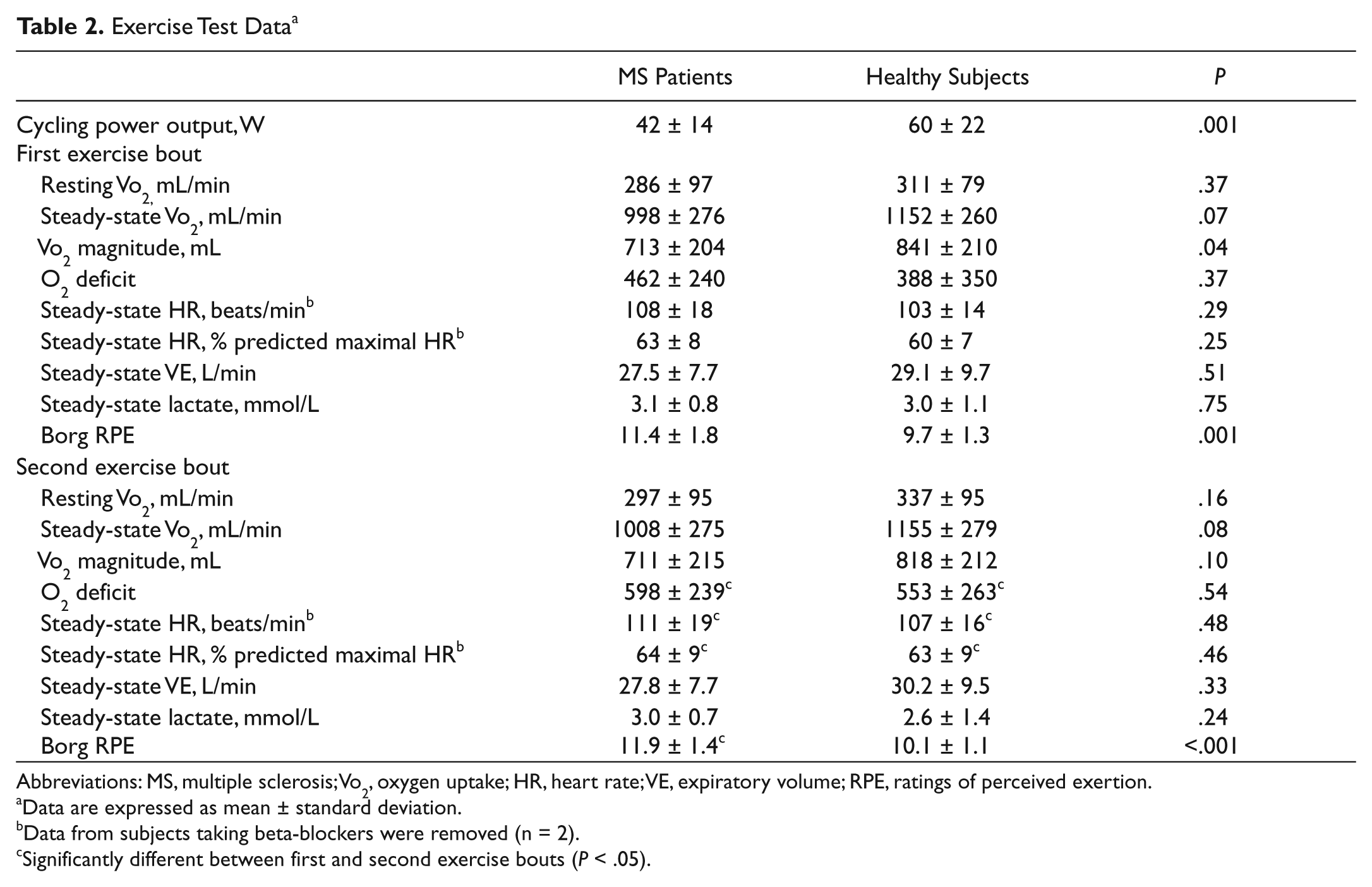
Abbreviations: MS, multiple sclerosis; Vo2, oxygen uptake; HR, heart rate; VE, expiratory volume; RPE, ratings of perceived exertion.
Data are expressed as mean ± standard deviation.
Data from subjects taking beta-blockers were removed (n = 2).
Significantly different between first and second exercise bouts (P < .05).
Exercise-Onset Vo2 Kinetics
Vo2 changes during exercise in MS patients and healthy subjects are displayed in Figure 1. The MRT during the first and second exercise bouts, and the averaged exercise-onset MRT of the 2 exercise bouts, are displayed in Figure 2. In both populations exercise-onset MRT during the second exercise bout (52 ± 20 and 40 ± 13 seconds in MS patients and healthy subjects, respectively) was significantly slower compared with the first exercise bout (39 ± 16 and 25 ± 19 seconds in MS patients [P < .001] and healthy subjects [P = .01], respectively). During both exercise bouts, exercise-onset MRT was significantly slower in MS patients (P = .01 and P = .04), when compared with healthy subjects. The averaged exercise-onset MRT of the 2 exercise bouts was significantly slower in MS patients (46 ± 17 seconds), as opposed to healthy subjects (32 ± 14 seconds); P = .007.
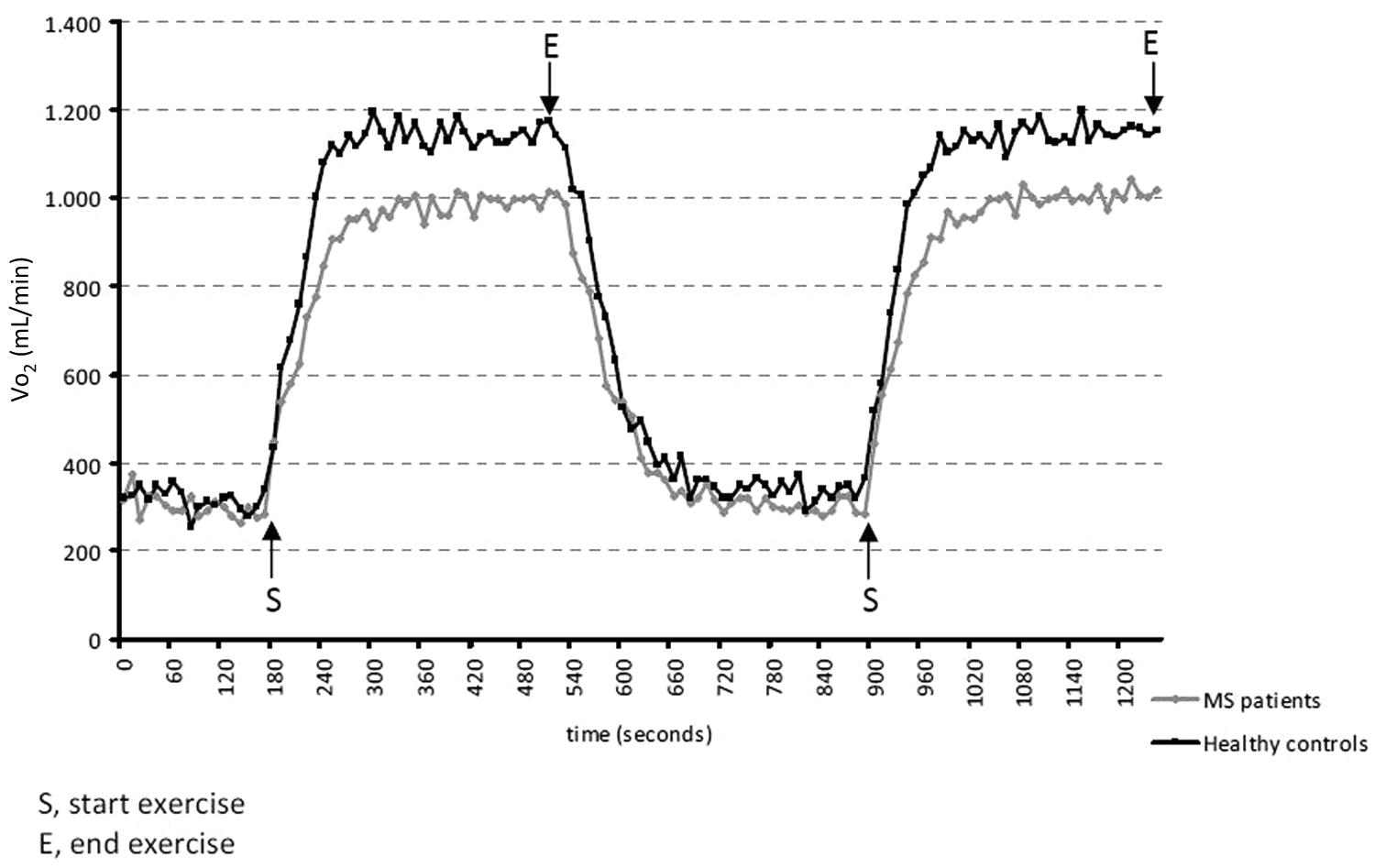
Vo2 during exercise testing. Averaged Vo2 curves when multiple sclerosis (MS) subjects and healthy participants execute 2 consecutive bouts of endurance exercise. Vo2 increases rapidly after onset of exercise and then decreases nearly to the resting (pre-exercise) level after cessation of the first bout.

Mean response time (MRT) for exercise-onset Vo2 kinetics. In A, exercise-onset Vo2 kinetics are significantly slower during the second compared with the first exercise bout in both groups (P < .05). For the first and second exercise bout, exercise-onset Vo2 kinetics are significantly slower in multiple sclerosis (MS) than in healthy participants (P < .05). In B, the averaged exercise-onset Vo2 kinetics (of the 2 exercise bouts) are significantly slower in MS than in healthy subjects (P < .05).
Exercise-Offset Vo2 Kinetics
Between groups, exercise-offset MRT (61 ± 32 and 59 ± 26 seconds in MS patients and healthy subjects, respectively) was not significantly different (P = .77).
Regression Analysis
In the total study group, only the presence of MS was independently related to averaged exercise-onset MRT of the 2 exercise bouts (P = .02). Age, gender, total-body adipose tissue percentage, and leg lean tissue mass were not correlated (P > .05). No independent relationships were found between subjects’ characteristics and exercise-offset MRT (P > .05).
In MS patients, no significant relationships were found between independent factors (age, gender, total-body adipose tissue percentage, leg lean tissue mass, EDSS score, MS type, physical activity) and averaged exercise-onset MRT of the 2 exercise bouts (P > .05). In addition, no significant relationships were found between subject characteristics and exercise-offset MRT (P > .05).
Correlations
A weak correlation (r = 0.35, P < .01) was found between exercise-offset MRT and exercise-onset MRT of the first exercise bout.
Discussion
This study shows that the exercise-onset oxygen uptake (Vo2) kinetics, expressed as mean response time (MRT) during submaximal endurance exercise, were significantly slower in persons with MS compared with healthy subjects. Exercise-offset Vo2 kinetics did not differ between groups.
Vo2 exercise-onset kinetics are significantly correlated with maximal Vo2 (r = −0.80, P < .05), 12 physical activity, and skeletal muscle oxidative capacity.13-18 It follows that an increase in physical activity and exercise training accelerates exercise-onset Vo2 kinetics. 18 Faster or slower exercise-onset Vo2 kinetics during low- to moderate-intensity endurance exercise may be related to intracellular partial oxygen pressure, phosphocreatine, and creatine kinase reactions (which are closely related to oxidative enzyme activity and mitochondrial respiration capacity), muscle perfusion, and muscle fiber type composition have been proposed as contributing factors. 33 Because this study did not observe significant and independent relationships between exercise-onset MRT and clinical subject characteristics in MS patients, it is difficult to determine the etiology of slowed exercise-onset Vo2 kinetics during endurance exercise in MS patients. Previous studies did describe characteristics of a lowered skeletal muscle oxidative capacity in subjects with MS,6-9 partly explaining the slowed exercise-onset Vo2 kinetics in MS patients. Further study is warranted to determine the etiology of slowed exercise-onset Vo2 kinetics during endurance exercise in MS patients. In such studies, skeletal muscle biopsies should be obtained, with assessment of fiber type composition, oxidative enzyme activity, and/or phosphocreatine resynthesis capacity.
Despite significantly different exercise-onset Vo2 kinetics between healthy and MS participants, exercise-offset Vo2 kinetics were not different between groups. Moreover, we failed to observe an independent relationship between MS presence and exercise-offset Vo2 kinetics in the total study group. Because previous studies already indicated that training status and/or exercise training do not always affect exercise-offset Vo2 kinetics,23,24 it remains uncertain whether this parameter truly reflects skeletal muscle oxidative capacity. Thus, the evaluation of exercise-offset Vo2 kinetics in MS patients seems less valid to estimate skeletal muscle oxidative capacity, as opposed to exercise-onset Vo2 kinetics. The weak correlation between exercise-onset and -offset Vo2 kinetics seems a contradiction. Recent studies, however, demonstrate an asymmetry between exercise-onset and -offset Vo2 kinetics, indicating that these 2 parameters are not necessarily related to each other or are different. 34
To compare exercise-onset and -offset Vo2 kinetics between different groups, it is important to match exercise intensities. In this study, the cardiac (heart rate), ventilatory (expiratory volume), and metabolic (blood lactate content) response to exercise was not different between MS patients and healthy controls. This indicates that the relative exercise intensities used were properly matched between groups, allowing exercise-onset and -offset Vo2 kinetics comparisons between the groups. Borg RPEs during exercise were significantly (P < .01) higher in participants with MS. This is probably related to greater difficulties with muscle coordination patterns necessary to cycle in the MS patients, leading to a greater subjective sensation of physical effort.
The finding of significantly slower exercise-onset Vo2 kinetics during the second exercise bout versus the first exercise bout, both in MS and healthy participants, was unexpected. Previous studies showed that high-intensity (above anaerobic threshold) endurance exercise speeds exercise-onset Vo2 kinetics during a subsequent moderate-intensity endurance exercise bout in healthy individuals. 14 A recent study evaluated the impact of a series of moderate-intensity (below the anaerobic threshold) endurance exercise bouts on exercise-onset Vo2 kinetics in healthy subjects and found no significantly different exercise-onset Vo2 kinetics between these bouts. 30 It remains difficult to explain our findings, because there is a great variance in selected endurance exercise intensities, exercise bout and recovery durations, Vo2 kinetics determination methods, and subject characteristics between studies.
Our findings suggest that some persons with MS have molecular skeletal muscle dysfunction (such as lowered oxidative capacity) at least during endurance exercise. By applying such exercise tests, investigators can clinically assess oxidative capacity of skeletal muscle without the need of maximal exercise testing or invasive procedures. This might be important since, based on our clinical experiences, poor coordination, ataxia, and weakness may be aggravated during a maximal bicycle exercise testing in MS patients. In addition, test discomfort might be too high when using invasive procedures to assess skeletal muscle oxidative capacity. This test may, however, be too difficult in more severely impaired persons with MS.5,35,36 Although exercise can improve impairments and disabilities in persons with MS, further trials are needed to determine whether exercise-onset Vo2 kinetics can be improved.
Conclusions
Exercise-onset Vo2 kinetics during submaximal endurance exercise are significantly slowed in MS patients, indicating a lowered skeletal muscle oxidative capacity. We can clinically assess oxidative capacity of skeletal muscle in MS patients, without the need of maximal exercise testing or invasive procedures.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.