
Abstract
Background. For individuals with lateral postural imbalance after stroke, the decision to adopt a cane for walking often is not based on objective findings. Objective. The authors investigated the explanatory value of 2 posturographic criteria for lateral postural imbalance on the walking abilities of poststroke subjects. Methods. Indices of postural asymmetry (percentage of body weight on the less loaded lower limb) and instability (mediolateral variance of center-of-pressure displacements) were measured in 40 healthy individuals and 52 patients (mean 94.2 days after first hemispheric stroke), who stood still on a double force platform. Cut-off values (mean ± 2 standard deviations) were calculated and compared. The predictive value of both postural indices on walking abilities with or without a cane was analyzed. Results. Of the patients, 34.6% were unstable along the mediolateral axis (variance >7 mm2), and 44.2% were asymmetrical (body weight <40%); 30% needed a technical aid and 35% walked without a cane. The probability of being able to walk without a cane was less than 5% if the paretic lower limb was not loaded more than 40%. The postural instability index was less informative. Conclusions. This study suggests that patients who do not load more than 40% of their body weight on their paretic lower limb may benefit from the prescription of a cane.
Introduction
A stable standing posture is a prerequisite for recovering an autonomous gait after a stroke and therefore is a major goal of rehabilitation. Changes in balance capacities, assessed by ordinal scales, are one of the best factors explaining walking recovery after a stroke. 1 Body weight loading–unloading mechanisms are indeed involved in the control of both gait and upright standing along the mediolateral axis. 2 This explains why postural asymmetry and lateral instability, 2 major determinants of impaired postural capacities in poststroke subjects, very often induce gait limitation. 3 Postural asymmetry, with more weight on the nonparetic lower limb, and the patient’s inability to compensate for it by loading the paretic lower limb, is because of many factors4-6 such as lower limb muscular strength. 7 This asymmetry can be compensated, at least temporarily, by the use of a cane. 8 The use of a standard cane has recently been shown to improve gait symmetry, 9 velocity, and walking distance. 10 The decision of when to adopt or discontinue the cane is often difficult to make. Discontinuing the use of the cane too soon might expose the patient to a risk of falls. 11 Keeping the cane too long might affect the recovery of an efficient gait. The value of the cane is 2-fold: (a) stabilizing, that is, reducing postural movements and (b) unloading the paretic limb during the single-limb support of gait to facilitate the step.
We evaluated the relevance of posturography, which quantifies both postural asymmetry and instability4,12 in explaining the walking ability of poststroke subjects, to analyze posturographic indices to guide recommendations for use of a cane.
Methods
Subjects
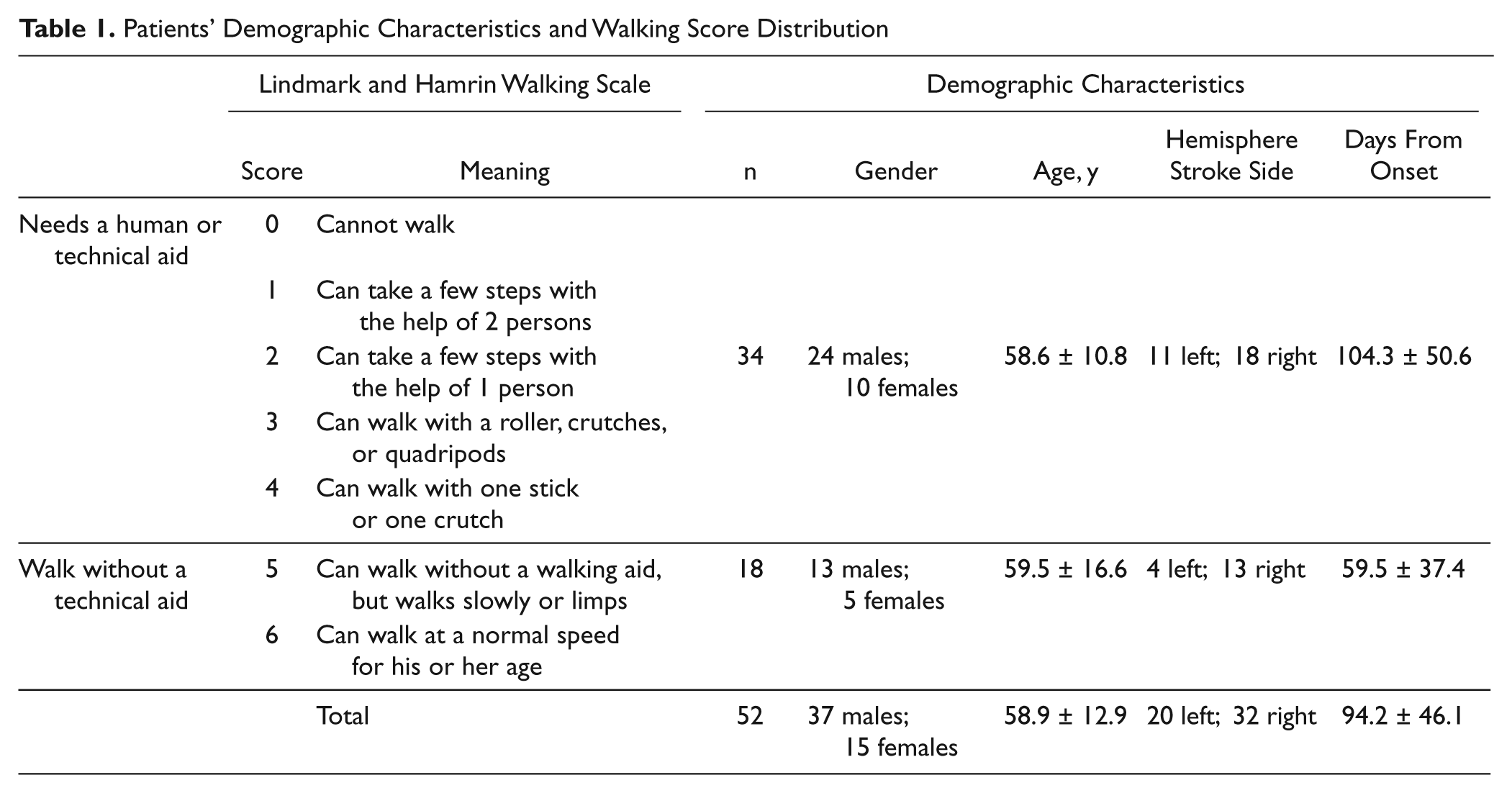
After giving informed consent, 52 subjects with stroke and 40 healthy individuals participated in the study approved by our institutional ethics committee. Subjects with stroke were consecutively admitted to a stroke rehabilitation unit after a recent first hemispheric stroke (Table 1) and controls were age-matched and not significantly different in sex ratio (age, 60.1 ± 13.2 years; gender, 21 males and 19 females). Written informed consent was obtained.
Patients’ Demographic Characteristics and Walking Score Distribution
Posture and Gait Assessment
The stability of standing posture was assessed by posturography using a double-force platform (PF02, Equi+, France). Subjects were asked to stand still, barefoot, in a standardized position with their feet placed on marks (heels 9 cm apart, toes pointing out at 30°), arms hanging freely, eyes open, for four trials lasting 32 seconds separated by 1- to 3-minute periods where the subject was seated. 4 Postural instability and asymmetry were quantified respectively by the variance of the center-of-pressure (CP) movements along the mediolateral axis (Var-CP-ML, mm2), and the percentage of body weight (BW) over the paretic (or less loaded in controls) foot (BWuf, %). Among various parameters aimed at evaluating postural instability, the variance of the CP movements is known to be one of the least sensitive to data recording conditions, with a high test–retest reliability. 13
In poststroke subjects, gait ability was assessed through direct observation by a clinician who did not know their posturographic data, using a 7-point walking score 14 (Table 1) that differentiated the subjects unable to walk without cane (score <5), from those who could walk without cane (score ≥5).
Prediction Analysis
As the distribution of both posturographic indices is Gaussian in the control group, a range of mean + 2 standard deviations was used to diagnose a postural abnormality (instability, asymmetry) for determining the inability to walk from an abnormal posturographic score. The clinimetric properties of posturographic criteria to explain the ability to walk without or with a cane was analyzed according to its sensitivity and specificity values. The sensitivity of a posturographic criterion was the probability of it being abnormal (ie, below BWuf cut-off and/or above Var-CP-ML cut-off) in patients unable to walk without a cane. The specificity of a posturographic criterion was the probability of it being normal in patients able to walk without cane. In addition, the Youden index (sensitivity + specificity − 1), as a validity coefficient informing about test efficiency, was calculated, with 1 being the strongest possible value. Finally, the positive predictive values (PPVs) were the probabilities of the gait score being <5 when posturographic indices were abnormal (ie, below the BWuf cut-off and/or above the Var-CP-ML cut-off). The negative predictive values (NPVs) were the probabilities of gait being ≥5 when posturographic indices were normal.
Statistical Analysis
Since the distribution of the posturographic data of poststroke subjects was not Gaussian (assessment using Kolmogorov–Smirnov tests), the groups were compared using Mann–Whitney tests. The data are expressed as the mean ± standard deviation when distributions were normal and as the mean (95th percentile) when they were not.
Results
Posturographic Data
Instability was diagnosed when variance was >7 mm2 along the ML axis and BWuf was <40%. Compared with controls, poststroke subjects were more unstable along the ML axis (mean 26.7, 95th percentile 51.8 mm2 vs mean 3.1, 95th percentile 6.8 mm2; P < .0001) and more asymmetric (mean 38.9, 95th percentile 51.7% vs mean 46.6, 95th percentile 49.8%; P = .0014). Among patients, 34.6% and 44.2% were classified as unstable and asymmetrical, respectively.
Explaining the Ability to Walk Without a Cane
The predictive values for patients’ ability to walk with or without a cane according to postural instability and asymmetry are presented in Tables 2 and 3, respectively.
Distribution of Poststroke Subjects According to Gait Capacities and Center-of-Pressure Movement Variance Along the ML Axis a
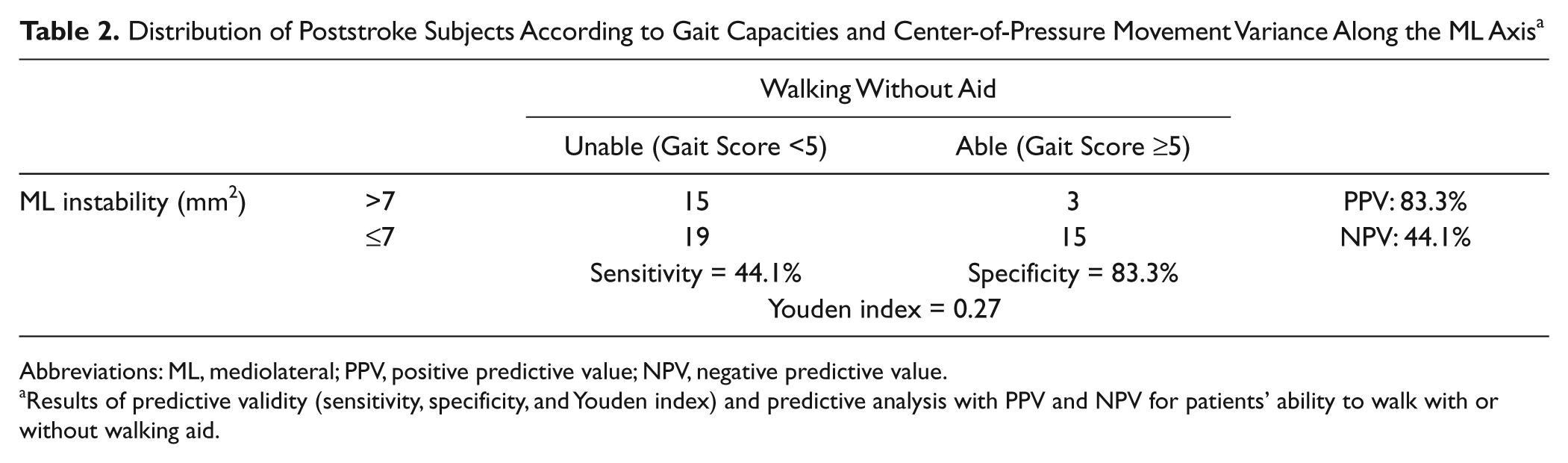
Abbreviations: ML, mediolateral; PPV, positive predictive value; NPV, negative predictive value.
Results of predictive validity (sensitivity, specificity, and Youden index) and predictive analysis with PPV and NPV for patients’ ability to walk with or without walking aid.
Distribution of Poststroke Subjects According to Gait Capacities and BWuf (%) a
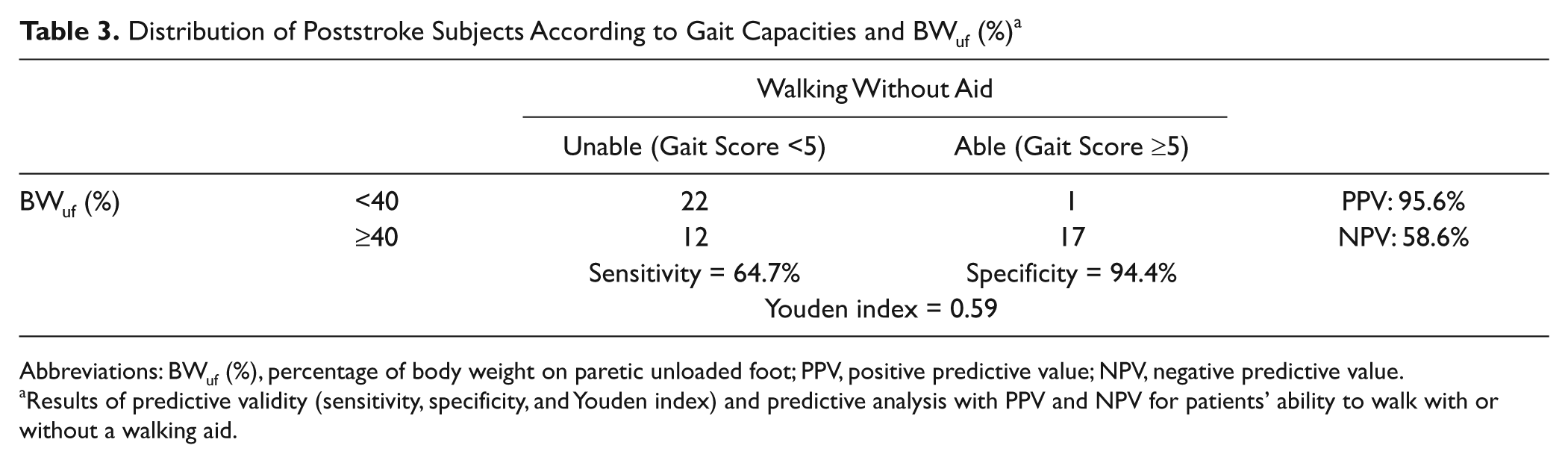
Abbreviations: BWuf (%), percentage of body weight on paretic unloaded foot; PPV, positive predictive value; NPV, negative predictive value.
Results of predictive validity (sensitivity, specificity, and Youden index) and predictive analysis with PPV and NPV for patients’ ability to walk with or without a walking aid.
Table 2 shows poor predictive validity of instability, especially in terms of Youden index (0.27). The Youden index was twice as high for the asymmetry criteria (0.59; Table 3) as for the instability criteria, meaning that postural asymmetry explained much better the need to use a cane than postural instability, with satisfactory sensitivity (64.7%) and great specificity (94.4%). Almost all patients who walked without cane behaved symmetrically on the force platform (specificity = 94.4%; see Table 3). The PPV of postural asymmetry reached 95.6% for the inability to walk without any aid, meaning that <5% of patients who spontaneously loaded their paretic lower limb with <40% of BW could walk without any aid. However, among patients in whom normal weight-bearing symmetry was observed, only 58.6% (NPV) could walk without aid. In other words, for a given patient, the probability of walking without any aid was 58.6% if they spontaneously loaded their paretic lower limb over 40% of their total BW.
Discussion
To our knowledge, this study is the first predictive analysis of the need for an assistive device for gait from posturographic data. Our approach was cross-sectional, with posture and gait assessments carried out within a short time span. Our study confirms that posturography can help assess gait ability 3 and yields novel findings for determining when patients need a cane. In an undisturbed stance, lateral body movements, resulting from loading–unloading mechanisms, 15 are similar to what occurs during gait where BW is alternatively supported by each lower limb. Postural parameters along the ML axis (percentage of BW on paretic limb and ML instability) therefore appear relevant for explaining gait capacities in patients with lateral imbalance. Our study reveals that the usefulness of a cane for walking is much better determined using postural asymmetry data than instability data. The probability for a given patient being able to walk without a cane is <5% if the subjects do not spontaneously load the paretic lower limb with at least 40% of their BW, as gait requires loading each lower limb sufficiently to master the single support phase of the stride. 3 Insufficient loading may be compensated by additional support. Our study suggests that any asymmetry corresponding to <40% of BW on the paretic lower limb would be a fair target for rehabilitation. However, loading 40% of the BW on the paretic limb must not be considered a sufficient condition to begin walking without a cane: Other factors include postural instability4,12 and verticality perception. 16
Could the variability of the delay of the stroke onset be a limitation of this study? The fact that patients who needed help to walk were investigated later than those who walked without help may be explained by the fact that all were required to maintain balance without aid for the posturography tests. Posturography was therefore performed later for the most impaired patients. Overall, this variability did not affect the explanation of the ability to walk by the capacity to stand for any given patient. Several technical points could be improved prior to a longitudinal prediction study involving more patients. One limitation is that our study required a dynamic task in which single limb stance duration does not exceed 1 second, and a postural static task lasting several tens of seconds. A second is that the posturographic parameters used in this study are measured during a nonimposed, comfortable, standing posture, which possibly obscures the ability of subjects to increase the load on their paretic lower limbs. 17 Last, the cross-sectional design of this study does not provide any information regarding the assistance needed by poststroke patients during gait recovery.
Conclusion
Lower extremity weight-bearing asymmetry is better than postural instability to anticipate the need to use a cane in poststroke subjects. This asymmetry can be tested on a single force platform 18 or 2 bathroom scales.
Footnotes
Acknowledgements
The authors are grateful to Noélie Buisson-Descombes for the proofreading in English language.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.