
Abstract
Background. Robot-assisted gait training has the potential to improve cardiopulmonary fitness after stroke, even for patients who are in the early stages of recovery and not independent ambulators. The authors compared the effects of robot-assisted gait training and conventional physical therapy on cardiopulmonary fitness. Methods. A prospective single-blinded, randomized controlled study of 37 patients receiving inpatient rehabilitation was performed within 1 month after stroke onset. The robot-assisted gait training group (n = 20) received 40 minutes of gait training with Lokomat and 60 minutes of conventional physical therapy each day, whereas the control group (n = 17) received 100 minutes of conventional physical therapy daily. Using a semirecumbent cycle ergometer, changes in cardiopulmonary fitness were investigated using incremental exercise testing. Motor and gait functional recovery was measured according to changes in the lower-extremity score of the Fugl-Meyer Assessment Scale (FMA-L), leg score of the Motricity Index (MI-L), and the Functional Ambulation Category (FAC). Results. Compared with the control group, the robot group showed 12.8% improvement in peak VO2 after training (P < .05). Compared with the control group, the robot group also improved in FMA-L score (P < .05). Conclusion. Patients can be trained to increase their VO2 and lower-extremity strength using a robotic device for stepping during inpatient rehabilitation. This training has the potential to improve cardiopulmonary fitness in patients who are not yet independent ambulators, but that may require more than 2 weeks of continued, progressive training.
Introduction
Body-weight-supported treadmill training may facilitate locomotor ability after stroke 1 by supporting a percentage of the body weight and promoting symmetrical weight bearing and stepping practice. Robot-driven gait orthoses have also been developed for use with a treadmill for body-weight-supported locomotor training. 2 Some,3,4 but not all 5 trials suggest that patients with subacute stroke show greater improvement in aspects of walking ability and strength compared with the group that did not receive robot-assisted gait training.
Studies of robot-assisted gait training have focused on the demonstration of its effect on walking ability. No studies have focused on the possible effect of robot-assisted gait training on cardiopulmonary function. Aerobic capacity has been reported to correlate with functional recovery in poststroke patients6-8; therefore, improvement of cardiopulmonary fitness is important in cases of reduced activities for prevention of cardiovascular and respiratory complications as well as other comorbidities, which can adversely affect functional recovery. 7 In these patients, neuromuscular dysfunction, such as motor weakness, sensory deficit, or loss of coordination, frequently results in decreased cardiopulmonary fitness. Because robot-assisted gait training can provide aerobic exercise, even for patients not capable of independent ambulation, it may affect cardiopulmonary fitness in the early stage of stroke, when patients usually cannot participate in an aerobic exercise program. This study aimed to investigate the effects of robot-assisted gait training on cardiopulmonary fitness and lower-extremity function.
Methods
Participants
Patients had to have motor weakness after unilateral ischemic or hemorrhagic stroke and receive inpatient care in the stroke rehabilitation unit. Inclusion criteria were (1) first-ever stroke, (2) stroke onset within 1 month, (3) supratentorial lesion, (4) age >20 years and <65 years, (5) not an independent ambulator (the functional ambulation category [FAC] < 2), 9 and (6) ability to cooperate during exercise testing. Patients who met criteria for absolute and relative contraindications to exercise testing established by the American College of Sports Medicine (ACSM) 10 were excluded. Also, patients who met contraindications for Lokomat therapy 11 or musculoskeletal disease involving the lower limbs, such as severe painful arthritis, osteoporosis, or joint contracture and other neurological diseases, were also excluded.
This study was designed as a prospective, single-blind, randomized, controlled study. The required sample size was determined using the pooled estimate of within-group standard deviations obtained from data reported in a recent article. 6 Power calculations indicated that a sample of more than 36 participants would provide an 80% (β = .20) chance of detection of a 20% (α = .05) difference in improvement between groups. We used a random permuted block design, where envelopes were sealed by persons not associated with the study. Experimental procedures were approved by the local ethics committee, and all participants provided written informed consent.
Training Protocol
Members of both groups underwent 2 physical therapy sessions for 5 days per week over a period of 2 consecutive weeks (total 20 sessions). Members of the robot group underwent a 40-minute session of gait training using Lokomat and a 60-minute session of conventional physical therapy each day, whereas members of the control group underwent a 60-minute session of conventional physical therapy and an additional 40-minute session of conventional physical therapy each day. During the study period, both groups were allowed to participate in other rehabilitation treatments, such as occupational therapy, with the same intensity and frequency.
Conventional physical therapy
Conventional physical therapy was based on neurodevelopmental techniques developed by Bobath. 12 Patients with poor function began with sitting and standing balance training, active transfer, sit-to-stand training, and strengthening exercises. As function improved, they progressed to functional gait training with the device and dynamic standing balance training while continuing to perform exercises for strengthening.
Robot-assisted gait training
Lokomat (Hocoma AG, Volketswil, Switzerland) is a robotic-driven gait orthosis for control of posture, a body-weight support system, and a treadmill. A harness, which was attached to the body-weight support system, was placed on the patient. The robot-driven gait orthosis was then positioned on the patient’s hip and knee joints for adjustment of joint movements at individualized gait speeds. Straps were used for patients with insufficient foot clearance resulting from weakness of ankle dorsiflexion. Tension on the strap was steadily decreased as motor recovery improved. The body-weight support system first lifted the patient above the treadmill. At the start of the preprogrammed, physiologically patterned, and task-specific gait program, the patient was lowered slowly onto the treadmill. A computer screen allowed patient and therapist to monitor treadmill speed, joint speed, joint angle, and other gait training information in real time. This feedback system aided patients in their efforts at more efficient movement of the lower extremities while the therapist controlled the intensity of the training.
As function improved, levels of body-weight support, treadmill speed, and guidance force were adjusted for maintenance of the knee extensor on the weak side during the stance phase. Level of body-weight support steadily decreased from 40% to 0%, and guidance force decreased from 100% to 10%. 3 By decreasing guidance force, which is used in both the stance and the swing phases, the patient is forced to participate more actively in the gait process through utilization of hip and knee muscles. Treadmill speed (starting at 1.2 km/h) was increased by 0.2 to 0.4 km/h per session to a maximum of 2.6 km/h. Although the greatest emphasis was placed on lowering of body-weight support, motor power, muscle tone, gait coordination, and gait quality were also considered during adjustment of parameters. All parameters were individually adjusted for each session. Excluding time required for putting on equipment and operation of the computer, actual training time was 40 minutes per session.
Incremental Exercise Testing Protocol
The exercise loading test was conducted by a physician who had no knowledge of which group the patient belonged to. Using the semirecumbent cycle ergometer as a modality, the cardiopulmonary function test was conducted and terminated according to standard ACSM criteria. 10 Cardiopulmonary function was assessed using the K4b2 (Cosmed, Rome, Italy), a wireless cardiopulmonary diagnostic device. Prior to the start of a test, cycle seat height was adjusted for each patient, so that the patient’s legs were almost completely extended when the pedals were at their lowest point. Patients were also familiarized with the closed facial mask and pedaling method of the ergometer until they felt comfortable. Using a strap, the foot of the hemiplegic side was fastened securely to the pedal.
According to the testing protocol, 10 W was maintained at 50 rpm. Following a 2-minute warm-up period, the work rate was increased by 5 W every minute. This protocol is identical to one designed for the study of maximal exercise testing by Tang et al. 13 To determine whether or not maximum exercise had been reached, at least 1 of the following criteria had to be met: (1) respiratory exchange ratio greater than 1.0, (2) age-adjusted peak heart rate of 85%, and (3) no increase of oxygen consumption (VO2) for more than 1 minute despite increased work load. Although maximum exercise may not have been reached, the test was stopped if discontinuation criteria from ACSM guidelines 10 were met or if the patient refused to continue.
Outcome Measures
The following parameters were evaluated within 3 days before and after 20 sessions of training. A physician who was responsible for evaluation of the participants remained unaware of each participant’s group and treatment throughout the entire study.
Outcome measure of cardiopulmonary fitness
Outcome measures of cardiopulmonary fitness were divided into 3 categories: aerobic capacity, cardiovascular response, and ventilatory response. (1) Aerobic capacity was evaluated with peak VO2 and respiratory exchange ratio at peak exercise. During the exercise test, peak VO2 was the highest VO2 achieved at maximal effort. (2) During peak exercise, cardiovascular response was evaluated with oxygen pulse, peak heart rate, systolic and diastolic blood pressure, and rate of perceived exertion at peak exercise. (3) Ventilatory response was evaluated with minute ventilation (V E) at peak exercise and ventilatory efficiency. Ventilatory efficiency was measured as the slope of V E at peak exercise versus VCO2 below the ventilator compensation point for exercise metabolic acidosis. 14
Outcome measure of motor and gait function
Outcome measures of motor and gait functional status included the lower extremity score of the Fugl-Meyer assessment scale (FMA-L), 15 the Motricity Index (MI-L), 16 and the FAC. 9
Statistical Analysis
Descriptive statistics were used for characterization of participants and exercise test results. All continuous variables used the Shapiro-Wilk test for determination of whether or not distribution was normal. For demographic data from both groups, independent t tests were used for continuous variables and χ2 tests were used for categorical variables. For comparison of change in outcome measures, the repeated-measure analysis of variance (ANOVA) with Time as the within-patient factor and Group (robot vs control) as the between-patient factor for parametric data with normal distribution were used. P < .05 was considered statistically significant. PASW version 17.0 was used in the performance of all statistical analyses.
Results
A total of 50 patients were initially screened for the study from September 2007 to May 2009. Because 2 patients refused to participate, 48 patients were divided into the robot and control groups. Of these, 3 patients in the robot group and 4 patients in the control group dropped out prior to receiving training because they were not able to perform the tasks required for incremental exercise testing; 1 patient in the robot group and 3 patients in the control group dropped out during training. Reasons for withdrawal included 3 patients who developed medical and neurological events that were not associated with training and 1 patient who did not want to commit to the time required for participation in the study. Consequently, 20 patients in the robot group and 17 patients in the control group completed training (Figure 1). We analyzed data obtained from patients who completed the designated training. Univariate analysis revealed no differences between the groups with regard to age, sex, history of cardiovascular risk factor, stroke type, hemiplegic side, weight, height, and body mass index (Table 1).
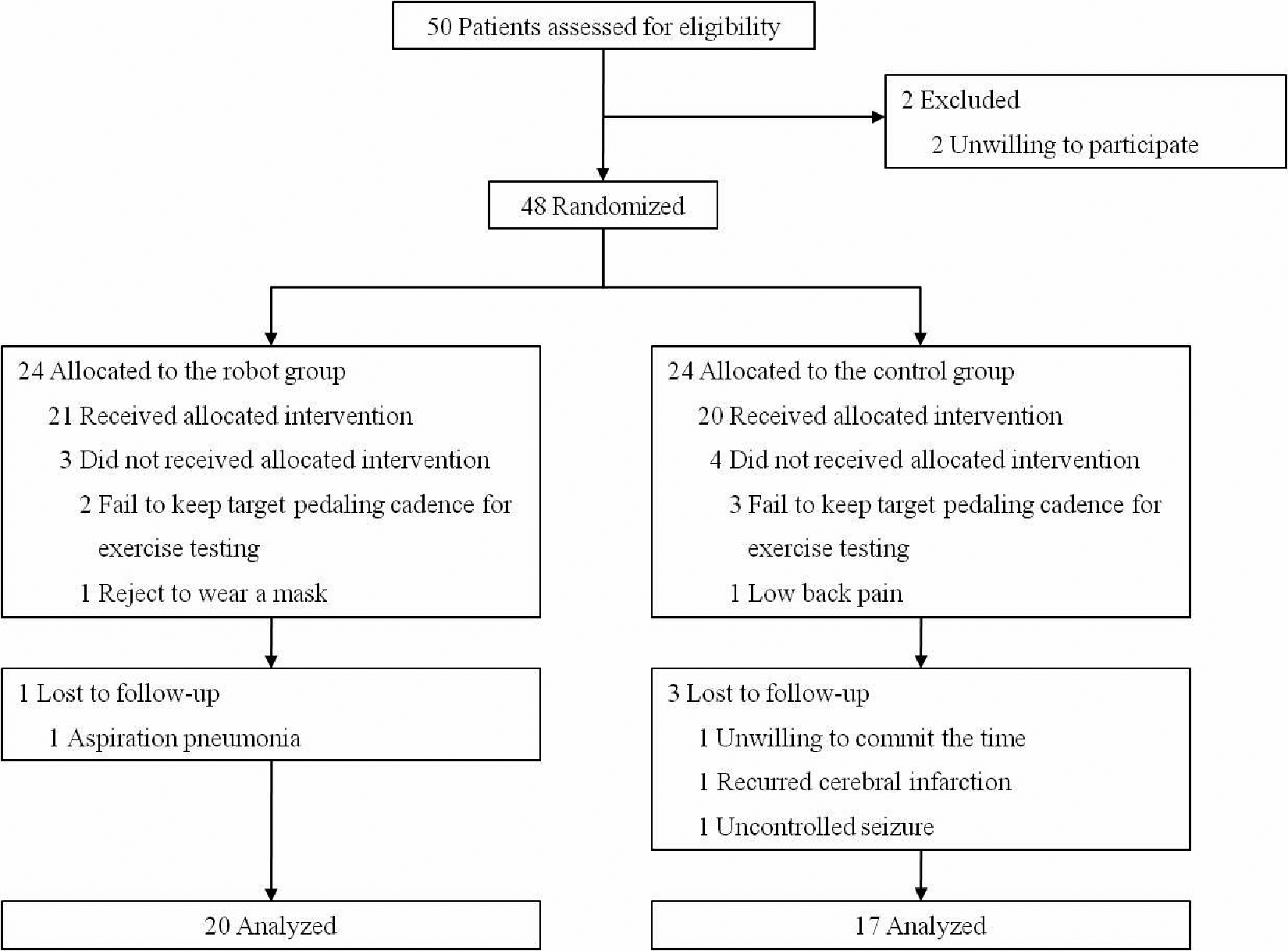
Randomization process for participants by CONSORT diagram.
General Characteristics of Patients
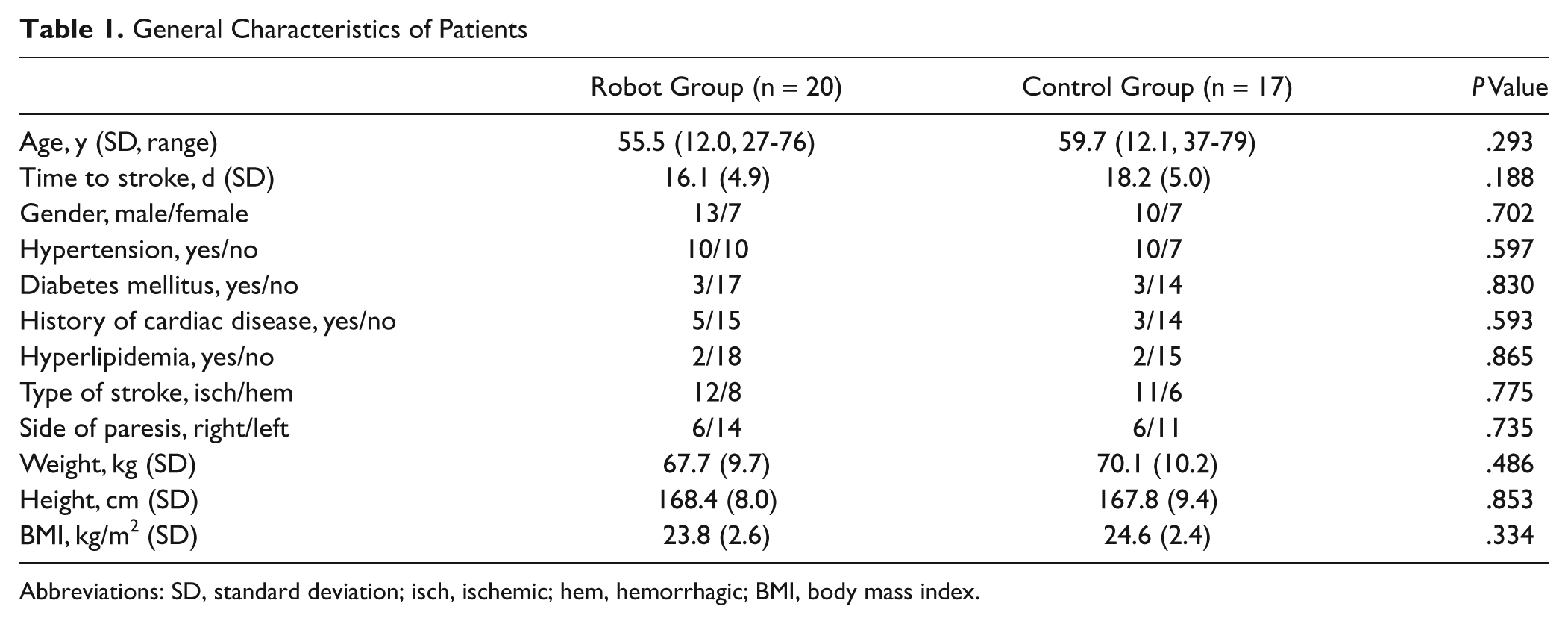
Abbreviations: SD, standard deviation; isch, ischemic; hem, hemorrhagic; BMI, body mass index.
Changes in Cardiopulmonary Fitness
Changes in measurements reflecting cardiopulmonary fitness in the robot group and in the control group are summarized in Table 2. Baseline values reflecting cardiopulmonary function were not statistically different between the 2 groups. However, peak VO2, which reflected aerobic capacity, repeated-measure ANOVA showed a significant interaction effect between time (pretraining vs posttraining) and type of intervention (robot vs control), as measured by peak VO2 (P < .05). Robot-assisted gait training produced greater improvement. No significant interaction in the parameters reflecting cardiovascular response and ventilator response were observed between the 2 groups (Table 2).
Assessment of Cardiopulmonary Function a
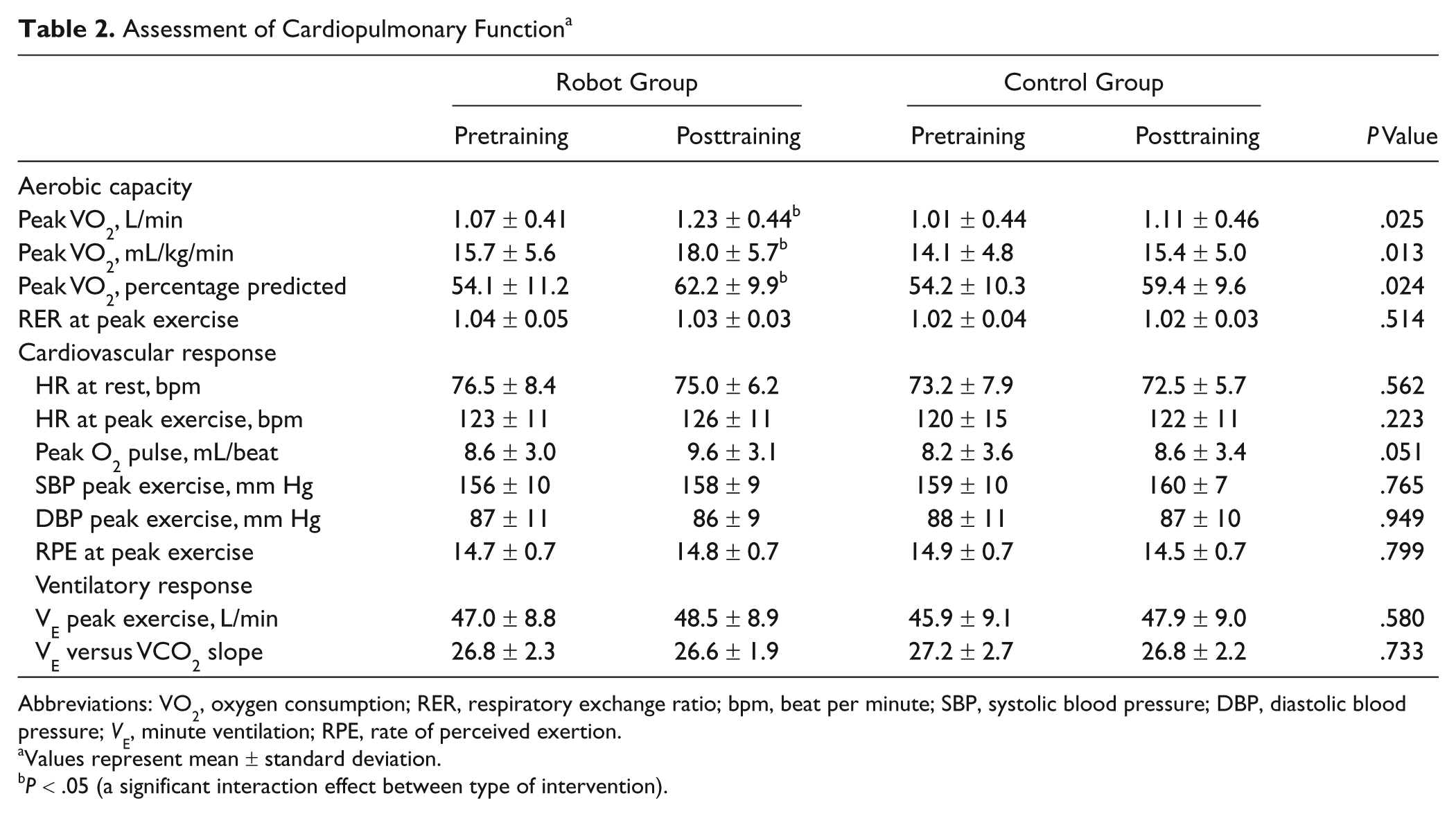
Abbreviations: VO2, oxygen consumption; RER, respiratory exchange ratio; bpm, beat per minute; SBP, systolic blood pressure; DBP, diastolic blood pressure; VE, minute ventilation; RPE, rate of perceived exertion.
Values represent mean ± standard deviation.
P < .05 (a significant interaction effect between type of intervention).
Changes in Motor and Gait Function After Training
Changes in measurements reflecting motor and gait function in the robot group and in the control group are summarized in Table 3. Baseline values were not statistically different between the 2 groups. However, repeated-measure ANOVA showed a significant interaction effect between time (pretraining vs posttraining) and type of intervention (robot vs control), as measured by FMA-L (P < .05). No significant interaction in parameters of MI-L and FAC was observed between the 2 groups.
Improvement in Motor Function and Gait Function a
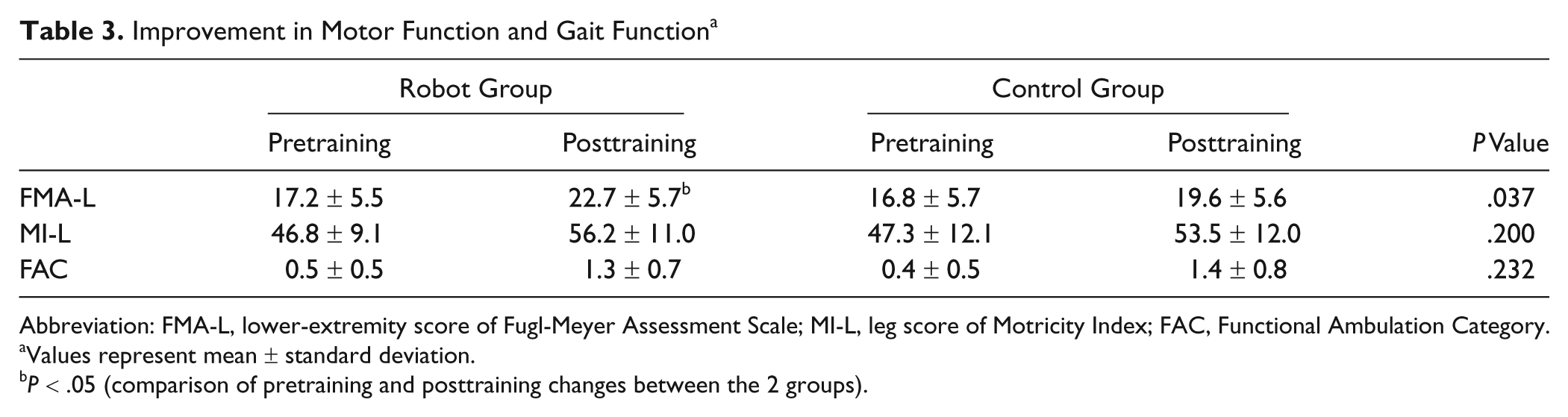
Abbreviation: FMA-L, lower-extremity score of Fugl-Meyer Assessment Scale; MI-L, leg score of Motricity Index; FAC, Functional Ambulation Category.
Values represent mean ± standard deviation.
P < .05 (comparison of pretraining and posttraining changes between the 2 groups).
Discussion
Results of this study demonstrated that, in comparison to conventional physical therapy, robot-assisted gait training has a positive effect on aerobic capacity associated with cardiopulmonary fitness as well as on lower-extremity motor recovery. The average aerobic capacity of participants prior to training was 54% to 72% of that of age-matched healthy adults, indicating severe deterioration of cardiopulmonary fitness evident in subacute stroke patients. Despite improvements of peak VO2 in patients between 1 and 6 months poststroke, substantial limitations in exercise capacity persisted even across the subacute stroke rehabilitation period. 17 Limitations in oxidative capacity and endurance of the hemiplegic side 6 as well as lowering of cardiac output and ventilation are thought to be the reasons for this decline in aerobic capacity. 18 In addition, the fact that 58% of stroke patients have a form of cardiac comorbidity could also be a reason for decline in aerobic capacity. 5 Exercise capacity appears to be an independent predictor of mortality 19 ; therefore, improvement of cardiopulmonary fitness in stroke patients may be regarded as having a positive effect on overall prognosis.
Many studies have reported on the effect of aerobic exercise in chronic stroke patients.20,21 A few studies have reported on the effect of exercise in stroke patients using diverse training methods within 3 months of stroke onset.7,8,22 These previous studies showed that aerobic exercise in patients with stroke could improve maximum walking speed and walking endurance and reduce dependence during walking. These studies used various training modes, such as a kinetron, body-weight supported treadmill, treadmill, and cycle ergometer. Also, most of the previous studies used more than 6 weeks of training duration. In this study featuring 2 weeks of training, peak VO2 in the robot group showed significant improvement compared with the control group. These findings may suggest that robot-assisted gait training can be used as a method of aerobic exercise in stroke patients. Therefore, we may be able to proclaim that therapeutic intervention for improvement of aerobic capacity has importance for functional gain and recovery after stroke.
Aerobic exercise first changes the central hemodynamics and then increases skeletal muscle capillary density.23,24 In this study, the training duration was relatively short (2 weeks) and might not have been sufficient to increase the skeletal muscle capillary density. This may be the reason that peak VO2, but not other measures of cardiopulmonary fitness, showed significantly greater improvement in the robot group than in the control group. Further study with longer training duration will be needed to confirm the effect of robot-assisted gait training on other measures of cardiovascular fitness in stroke patients. The possible mechanism of the change of central hemodynamics was an increase in central neural drive. Cardiovascular responses during exercise are governed by both central and peripheral mechanisms and their interactions with the arterial baroreflexes. 25 Exercise-related peripheral information, conveyed in part by the baroreceptors to the nucleus tractus solitarii (NTS), is transmitted directly and/or indirectly via catechoaminergic projections to the paraventricular nucleus (PVN). This results in turn in the simultaneous activation of oxytocinergic and vasopressinergic preautonomic neurons projecting back to the NTS.26,27 The sustained activation and increased efficacy of this NTS–PVN–NTS pathway during exercise appears to be mediated and sustained by neuroplastic adaptive mechanisms occurring at different loci within this interconnected network. 26
In our study, none of the patients in the robot training group showed any serious side effects during or after training. Taken together with previous reports using the same equipment,2-4,28 our study reports on the safety of Lokomat gait training for use in rehabilitation of stroke patients in the subacute and chronic stage. However, because prevalence of comorbid cardiac disease and risk of secondary stroke are relatively high in stroke patients, screening of candidates with strict adherence to ACSM guidelines will be helpful. 10 The ACSM has recommended that exercise programming for stroke survivors be set at a conservative intensity of 40% to 70% of peak VO2 or 40% to 70% of a heart rate reserve. 29
Our results clearly showed a better improvement in motor score of the affected lower limb after robot-assisted gait training in comparison with conventional physical therapy, which suggests that robot-assisted gait training has a facilitative effect on motor functional recovery after stroke. These results are in line with those of some previous studies3,30 but not those of other well-designed parallel group trials using conventional physical therapy.6,28 Westlake and Patten 30 reported that robot-assisted gait training had an advantage for the motor function of affected lower limbs over manual body-weight-supported treadmill training in patients with chronic stroke. Our study showed no significant difference in gait function between robot-assisted gait training and control groups. A possible explanation is that our protocol provided robot-assisted gait training for a short period during the subacute stage of stroke.
There are 3 different ways to increase the intensity of robot-assisted gait training. First, the ratio of body weight support is lowered. Second, guidance torque is lowered. Finally, the velocity of the treadmill is increased. Krewer et al 11 reported that stroke patients were found to have a statistically significant increase in oxygen consumption rate when body-weight support was changed from 100% to 30% during robot-assisted gait training. The guidance torque or treadmill velocity does not affect oxygen consumption. However, because of the lack of data pertaining to frequency, intensity, duration, and modality components of an exercise prescription for stroke patients, confirmation of the dose–response effects of aerobic exercise training is very difficult. 21
Exercise intensity is probably one of the most important fitness training variables. 21 We did not record the training intensity in either the robot or the control group, although we did set the same frequency and duration of training sessions. This is an important limitation in this study. Differences between the 2 groups could be attributed to training intensity.
Early robot-assisted gait training for a period of 2 weeks after stroke resulted in a cardiopulmonary effect on aerobic capacity. However, some parameters of cardiopulmonary fitness did not change after robot-assisted gait training. Compared with the control group, measurements that reflected cardiovascular and ventilatory response did not show a significant increase. We assumed that a possible reason for this would be the relatively short duration of training in this study. Although early beneficial effects despite short training duration have been reported in subacute poststroke patients, 8 to be more optimally effective, aerobic training for at least 8 weeks is likely necessary. 5 Long-term effects of robot-assisted gait training on gait function will require further investigation.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
This work was supported by a grant from the Korea Science and Engineering Foundation (#M10644000022-06N4400-02210) and Samsung Biomedical Research Institute (#SBRI C-A7-407-1), and Insung Research Foundation, Republic of Korea.