
Abstract
Background and Objectives. Robot-assisted therapy (RT) is a current promising intervention in stroke rehabilitation, but more research is warranted for examining its efficacy and the dose–benefit relation. The authors investigated the effects of higher intensity versus lower intensity RT on movements of forearm pronation–supination and wrist flexion–extension relative to conventional rehabilitation (CR) in patients poststroke for a mean of 21 months. Methods. In this pilot study, 18 patients with initial mean Fugl-Meyer Assessment (FMA) of 37 to 44 for the upper extremity were randomized to higher intensity RT, lower intensity RT, or CR intervention for 4 weeks. The dose of the higher intensity RT was twice the number of repetitions in the lower intensity RT. Outcome measures at pretreatment and posttreatment were administered to patients to evaluate beneficial and adverse effects of interventions. Primary outcomes were the FMA and Medical Research Council scale. Results. There were significant differences in motor function (P = .04) and daily performance (P = .03) among the 3 groups. The higher intensity RT group showed better improvement in motor function, muscle strength, performance of daily activities, and bimanual ability than the other 2 groups. The intensive RT intervention did not induce higher levels of an oxidative DNA biomarker. Conclusions. Higher intensity of RT that assists forearm and wrist movements may lead to greater improvement in motor ability and functional performance in stroke patients. A sample size of only 20 to 25 in each arm of a larger randomized controlled trial is needed to confirm the findings for similar subjects.
Keywords
Introduction
Stroke remains a leading cause of permanent disability and is a large source of disease burden worldwide. 1,2 Robot-assisted therapy (RT) for upper extremity (UE) motor function has emerged as a possible adjunct for stroke rehabilitation, although not yet convincingly shown to be better than the same intensity of conventional focused UE therapy. 3-9
RT incorporates some therapeutic elements for success in stroke motor rehabilitation into its design: intensive, repetitiveness, feedback, and bilateral training. 5-9 Along with these advantages, patients can be trained much more often, which has been shown to lead to better outcomes and have potential to enhance motor learning (eg, the Assisted Rehabilitation and Measurement Guide). 10,11 Previous RT studies showed significant, if modest, improvement in UE motor function, strength, and motor control parameters in stroke patients after interventions. 5,6,8 Systematic reviews found that RT significantly improved arm motor function for stroke patients but did not significantly improve daily functions. 12,13 Robotics can also provide quantitative control and measurement of therapy (eg, velocity, kinematics, resistance, and range of motion), allowing for research into the treatment dosage of rehabilitation. 14 Despite growing empirical evidence for the use of RT in stroke rehabilitation, rigorous research is needed to answer more specific questions that will maximize the benefits from the treatment. 15 For example, what is the optimal intensity of RT? What are the relative beneficial and adverse effects of RT compared with other treatments?
Dosage in stroke rehabilitation trials usually uses the duration-based measure of therapy and provides the information regarding the amount of minutes or days per week of therapy provided. 16 Most RT trials have offered the treatment in sessions lasting 30 minutes to 1.5 hours, with 3 to 5 sessions per week for 3 to 8 weeks. 5,6,8,9 In the EXCITE trial for constraint-induced therapy, the training involved forcing the patient to use the affected arm for up to 6 hours daily for 10 weekdays, and the less-affected hand was placed in a mitt for a goal of 90% of the patient’s waking hours for 14 days during a 2-week period. 17 In addition, one study found that in a standard rehabilitation session, the average of repetitions of the functional UE practice was 32. 16 According to recent research, performing about 300 repetitions of task-specific UE training per session was feasible in stroke rehabilitation. 18 Although greater duration or intensity of rehabilitation resulted in more functional improvement, 19-21 current data do not allow for a prescription of how much treatment is enough to induce improvements and not harm the patient. Thus, the definition of treatment intensity as the number of movement repetitions per unit of time 22 was adopted in this study and was investigated to inform the optimal dosage for further stroke rehabilitation.
Moreover, it is important to select the appropriate intensity of exercise or treatment, because exercise that is too intensive can be hazardous. 23 The study found that high-intensity exercise (ie, 75% maximum oxygen consumption reached) increased oxidative stress in healthy men. 23 During prolonged heavy exercise, antioxidant systems may be overwhelmed by excessive reactive oxygen species, leading to cell and tissue damage. 24 Stroke patients commonly showed activity intolerance and significantly lower maximal workloads than controls during exercise. 25 For healthy people, the RT protocols proposed in this study seem not to have been so stressful or reach the effort level of the previous study where increased oxidative stress was found. 23 For stroke patients, however, the same intensity or amount of training may have different impacts from healthy people. In addition, the oxidative stress level has been reported to be higher in acute stroke patients than in control subjects, but the effects of training on oxidative damage have not been addressed in these studies. 26,27 To date, the threshold level of training intensity that may cause oxidative stress in stroke patients remains unclear and warrants scrutiny. To address this gap in dose–response relations in stroke motor rehabilitation, this study investigated the effects of intensive RT on the 8-hydroxy-2′-deoxyguanosine (8-OHdG) level, an oxidative DNA biomarker, in stroke patients. Our goals in this study were to (a) investigate the treatment effects of RT on different outcomes relative to conventional rehabilitation (CR) in patients with stroke, (b) test the dose–response relations by using 2 groups receiving higher intensity and lower intensity RT, and (c) examine the effects of RT training on 8-OHdG, a biomarker of oxidative stress.
Methods
Participants
This pilot study recruited 18 patients between August 2009 and May 2010 from the Departments of Physical Medicine and Rehabilitation of 3 medical centers in Taiwan. The study enrolled 14.4% of screened patients (Figure 1). The inclusion criteria were (a) more than 6 months since a unilateral stroke; (b) an initial UE subsection of the Fugl-Meyer Assessment score of 30 to 56, indicating moderate to mild motor impairment; 28,29 (c) no excessive spasticity in elbow and wrist joints of the affected UE (Modified Ashworth Scale <3); (d) ability to follow study instructions and perform study tasks (Mini-Mental Status Examination ≥24); (e) no upper limb fracture within 3 months; (f) no participation in any experimental rehabilitation or drug studies during the study period; and (g) willing to provide written informed consent. The exclusion criteria were (a) painful arthritis of the elbow, wrist, or finger joints; (b) severe neuropsychologic impairments (eg, global aphasia and severe attention deficits); (c) physician-determined major medical problems or poor physical condition that would interfere with participation; and (d) cerebellar or brain stem lesions to limit potential interference of other symptoms or signs with task accomplishment (eg, ataxia). The institutional review boards of the 3 participating hospitals approved the study, and all patients signed an informed consent document.
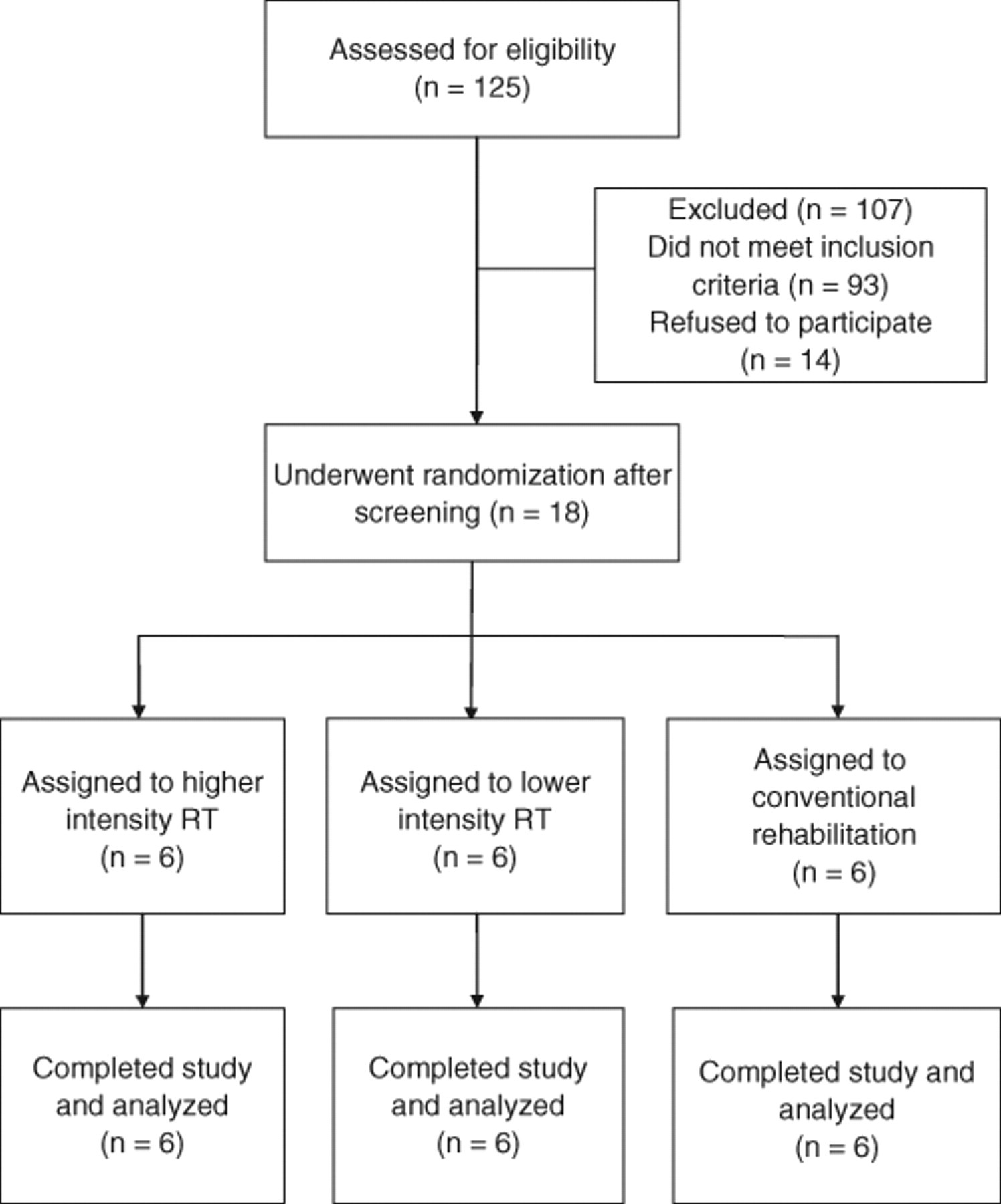
Flow diagram of study participants
Study Design and Procedures
A single-blind randomized controlled trial with pretest and posttest assessments was applied in this study. An intention-to-treat analysis was used. The eligible participants were randomly assigned to receive the higher intensity RT, lower intensity RT, or CR according to a 1:1:1 ratio using a random number table. When a new eligible patient was registered, the sealed opaque envelope identifying the group of each participant was given to the therapists, and they were informed of the group allocation to deliver therapy accordingly.
At pretreatment and immediately after the intervention, all clinical measures were administered to the patients by the same blinded rater. Before the administration of the clinical measures, the blinded rater was trained to properly administer these measures. This training included careful examination of written instructions and repeated practice. Rater competence was assessed by a senior certified occupational therapist.
Interventions
Patients received higher intensity RT, lower intensity RT, or CR intervention for 20 training sessions (90-105 min/d, 5 d/wk for 4 weeks). Licensed occupational therapists trained in study procedures provided the treatments. All patients otherwise received routine interdisciplinary stroke rehabilitation.
Higher intensity RT protocol
The robot-assisted arm trainer, Bi-Manu-Track (Reha-Stim Co, Berlin, Germany; Figure 2), was used in this study. The Bi-Manu-Track enables the symmetrical practice of 2 movement patterns: forearm pronation–supination and wrist flexion–extension. 5 Each movement pattern has 3 computer-controlled modes: passive–passive (mode 1), active–passive (mode 2, the unaffected arm actively driving the affected arm), and active–active (mode 3). The speed of movement, the amount of resistance, and range of movement can be adjusted individually. The patients sat at a height-adjustable table with their elbows bent at 90° and put their forearms in the midposition into an arm trough. A simple computer game (eg, picking up apples) that tracks patient movements was placed in front of the patients to provide instant visual movement feedback and to increase participation. The therapist also provided verbal feedback.
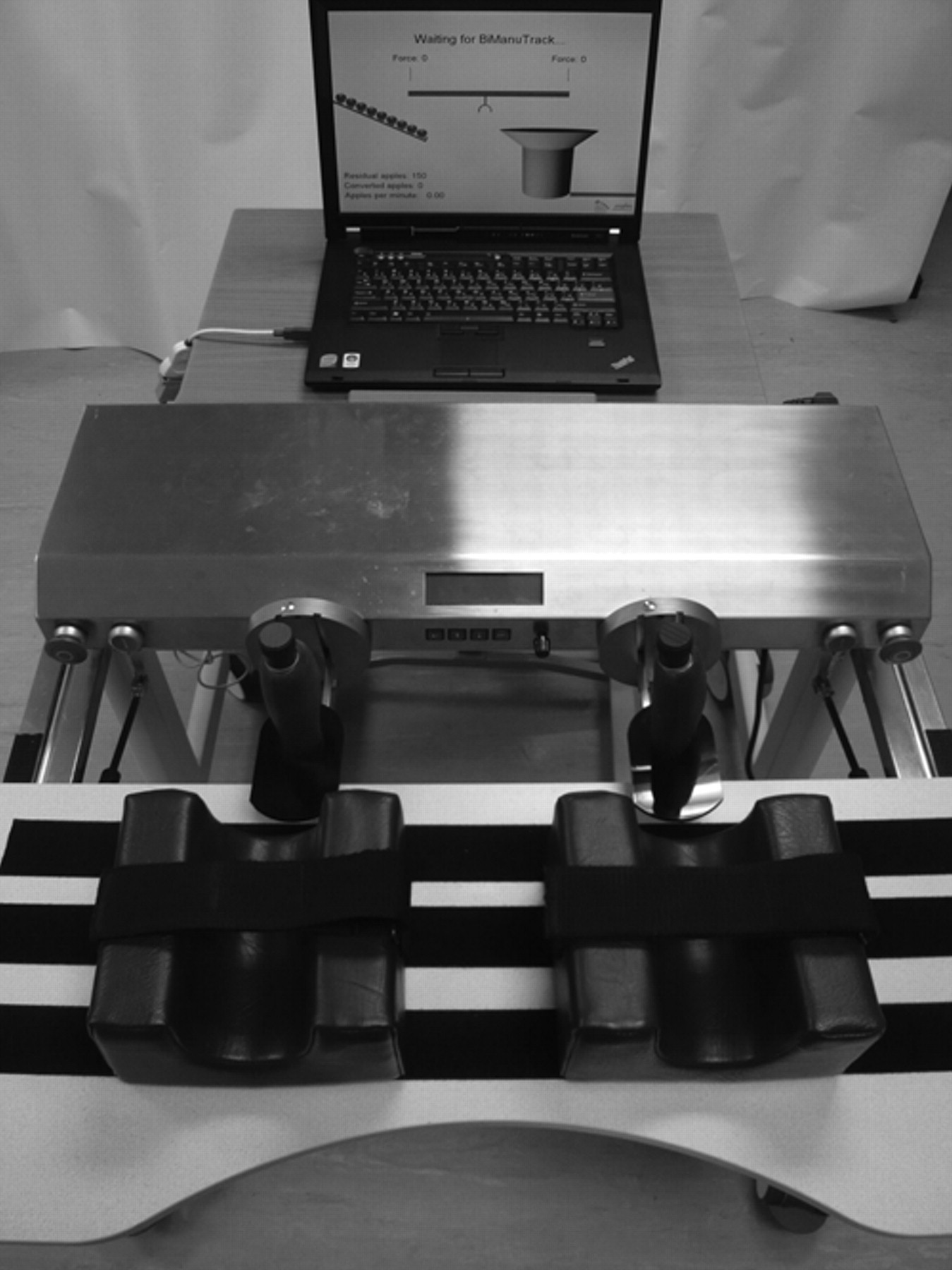
The Bi-Manu-Track.
Within 1 training session, each patient in the higher intensity RT group practiced 600 to 800 repetitions of mode 1 for 15 minutes, 600 to 800 repetitions of mode 2 for 15 to 20 minutes, and 150 to 200 repetitions of mode 3 for 5 minutes, respectively, for the forearm and the wrist movements. One repetition indicates 1 movement direction; for example, 1 pronation or 1 supination of the forearm counts as 1 repetition. If the affected arm can actively perform forearm pronation–supination or wrist flexion–extension, mode 2 can be adjusted to the affected arm actively driving the unaffected arm (300-400 maximal repetitions) to encourage more active movements of the affected arm. We reduced the number of repetitions of mode 1 into this mode (affected arm actively driving), and thus the total number of repetitions was still the same.
Before the RT commenced, 5 to 10 minutes of passive range of motion was provided as a warm-up. After the RT, patients received 15 to 20 minutes of functional activities training to help them transfer the acquired motor ability into daily activities performance. The functional activities were selected by patients and therapists and included opening a can or jar, turning a door knob, carrying heavy objects, writing, picking up a phone for listening, using chopsticks, twisting a towel, turning pages of a book, and so on.
Lower intensity RT protocol
Except for the treatment intensity, other training principles and practice parameters were the same as with the higher intensity RT group. Within 1 training session, patients in this lower intensity RT group practiced 300 to 400 repetitions of mode 1 for 15 minutes, 300 to 400 repetitions of mode 2 for 15 to 20 minutes, and 70 to 100 repetitions of mode 3 for 5 minutes, respectively, for the forearm and the wrist movements. In addition, if the affected arm could actively perform forearm pronation–supination or wrist flexion–extension, mode 2 could be adjusted to the affected arm actively driving the unaffected arm (150-200 maximal repetitions) to encourage more active movements of the affected arm.
The dosage of the higher intensity and lower intensity RT groups was determined from findings of animal studies, previous research on the Bi-Manu-Track, and practical concerns. Data from 2 animal studies showed that performing about 400 to 600 repetitions of upper limb tasks per session during motor skill learning induced neural plastic changes. 30,31 Furthermore, 200 to 500 repetitions per session for mode 1 and mode 2 were used in prior studies of the Bi-Manu-Track 5,32 in which positive benefits of therapy were found. This range might be viewed as the lowest limit of dosage for the Bi-Manu-Track training to have positive outcomes based on current evidence. In addition, the speed of movements and patients’ tolerance were taken into consideration. Therefore, 300 to 400 repetitions of mode 1 and mode 2 for 15 minutes were selected for the low-intensity RT group. A higher dose, 2-fold of the repetitions in the low-intensity RT group, was set as the intensity of the higher intensity RT group.
CR protocol
The CR group received a structured protocol using conventional occupational therapy techniques such as neurodevelopmental techniques 33 with emphasis on functional tasks and muscle strengthening. The protocol included (a) passive range of motion exercises, stretching of the affected limb, or facilitatory and inhibitory techniques for 15 to 20 minutes; (b) fine motor or dexterity training for 20 minutes; (c) arm exercises or gross motor training for 20 minutes; (d) muscle strengthening of the affected upper limb for 15 to 20 minutes; and (e) activities of daily living or functional tasks training for 15 to 20 minutes. The activities were adapted based on the level of motor impairment and functional needs of individual patients.
Outcome Measures
Outcome measures to evaluate preliminary benefits and potential adverse effects were administered to patients before and after treatment. The UE subscale of the Fugl-Meyer Assessment (FMA) and the Medical Research Council (MRC) scale were used as the primary outcomes. The 33 UE items of the FMA assess the movements and reflexes of the shoulder/elbow/forearm, wrist, hand, and coordination and speed. 34-36 Muscle strength of the affected arm was examined by the MRC scale. 37,38 The muscle strength of shoulder flexors/abductors, elbow flexors/extensors, wrist flexors/extensors, and flexors/extensors of the metacarpophalangeal joints was graded by the MRC in this study, and the average MRC score was calculated.
The secondary outcomes were the Motor Activity Log (MAL) and the ABILHAND scale. The MAL contains 30 structured interview questions related to information about the patients’ perceptions regarding the amount of use (AOU) and quality of movement (QOM) of the affected arm to accomplish common daily activities. 39 The rating score of each item for AOU and QOM ranges from 0 to 5, and higher scores indicate better performance. The reliability and validity of the MAL have been established. 29,40 The 23-item ABILHAND scale was used to measure bimanual ability. 41,42 Patients were asked to estimate the difficulty they had in performing these bimanual tasks on a 3-level scale (0 = impossible, 1 = any difficulty, 2 = easy). The Rasch reliability, construct validity, and responsiveness of the ABILHAND have been established in stroke patients. 41,42
Urinary 8-OHdG is a stable and integral biomarker of oxidative DNA damage and was used as a safety outcome. 43 Urine samples were collected from the patients before and after intervention and stored at −80°C. The urinary 8-OHdG levels were analyzed with a highly sensitive and selective method, using isotope-dilution liquid chromatography with tandem mass spectrometry (LC/MS/MS), as previously published by Hu et al. 44 On the basis of previous studies that used the LC/MS/MS analytic method, the mean urinary 8-OHdG levels in the control patients have been reported in the range of 4 to 6 ng/mg creatinine. 44,45
The general subscale of the Multidimensional Fatigue Symptom Inventory (MFSI) 46 was used to measure general fatigue of the patients. It includes 6 items with a total score ranging from 0 (not at all) to 24 (extremely). The interrater reliability, test–retest reliability, and convergent validity of the general subscale of the MFSI have been validated in stroke patients. 47
Data Analysis
The χ2 test for categoric variables and 1-way analysis of variance for continuous variables were used to compare the baseline characteristics of the 3 groups. Analyses of covariance was used to evaluate treatment efficacy, with pretreatment scores of each outcome measures as the respective covariates, group as the between-subjects factor, and posttreatment scores of each outcome variable as the dependent variables. The Tukey method was used for post hoc pairwise comparisons. The effect size of partial η2 was calculated for each outcome variable to index the magnitude of the performance difference between the 3 groups. A large effect is represented by a partial η2 of at least .138, a moderate effect by .059, and a small effect by .010. 48 Statistical analyses were performed with SPSS version 15.0 and SAS version 9.1.3 software (IBM, Somers, New York; SAS Institute, Cary, North Carolina). Values of P < .05 were considered statistically significant.
Results
Eighteen patients (13 men and 5 women) completed the study. Their age range was 31 to 69 years, stroke onset was 6 to 63 months prior, and there were 8 right and 10 left hemisphere lesions (Table 1). The baseline demographic and clinical characteristics of the participants among the 3 groups were not significantly different (Table 1). Most patients showed improvements on primary outcomes after the interventions (Figure 3).
Baseline Characteristics of the Study Participants (N = 18)
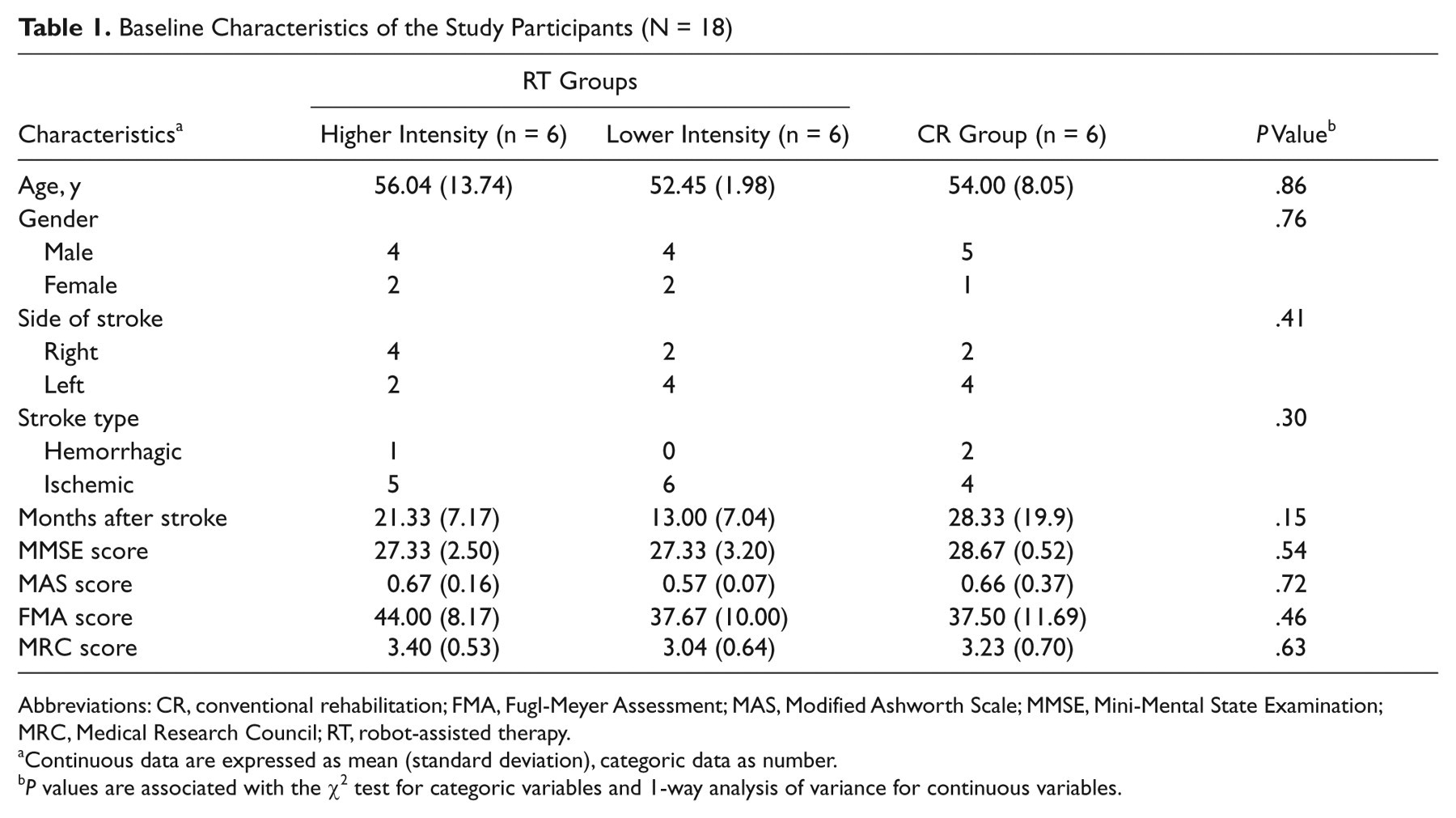
Abbreviations: CR, conventional rehabilitation; FMA, Fugl-Meyer Assessment; MAS, Modified Ashworth Scale; MMSE, Mini-Mental State Examination; MRC, Medical Research Council; RT, robot-assisted therapy.
Continuous data are expressed as mean (standard deviation), categoric data as number.
P values are associated with the χ2 test for categoric variables and 1-way analysis of variance for continuous variables.
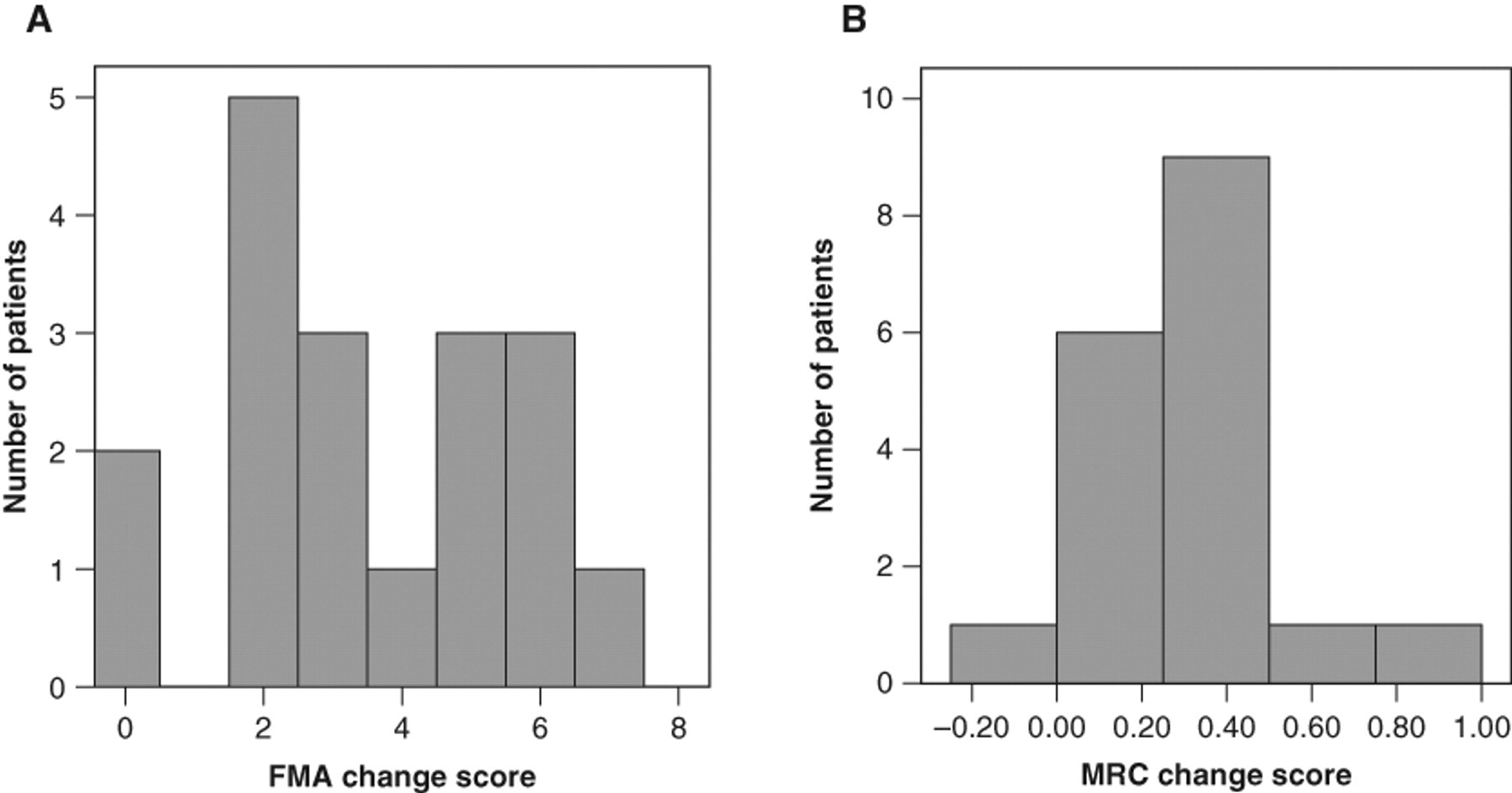
The change scores of all patients on the primary outcomes after treatment are shown for the (A) Fugl-Meyer Assessment (FMA) and (B) the Medical Research Council (MRC) scale.
Table 2 reports the descriptive and inferential statistics for each outcome of the 3 groups. For the primary outcomes, there was a significant difference in UE motor ability measured by the FMA among the 3 groups (P = .04, partial η2 = .38). Post hoc analyses revealed that the higher intensity RT group showed significantly better improvements in motor ability than the lower intensity RT group (P = .04). The difference in FMA improvements in the lower intensity RT and the CR groups was not significant (P = .88). Moreover, differences in muscle strength measured by the MRC among the 3 groups approached significance (P = .06, partial η2 = .33). The higher intensity RT group showed the most improvement in muscle strength, whereas the CR group showed the least improvement.
Descriptive and Inferential Statistics for Each Outcome Measure From Baseline to Posttreatment
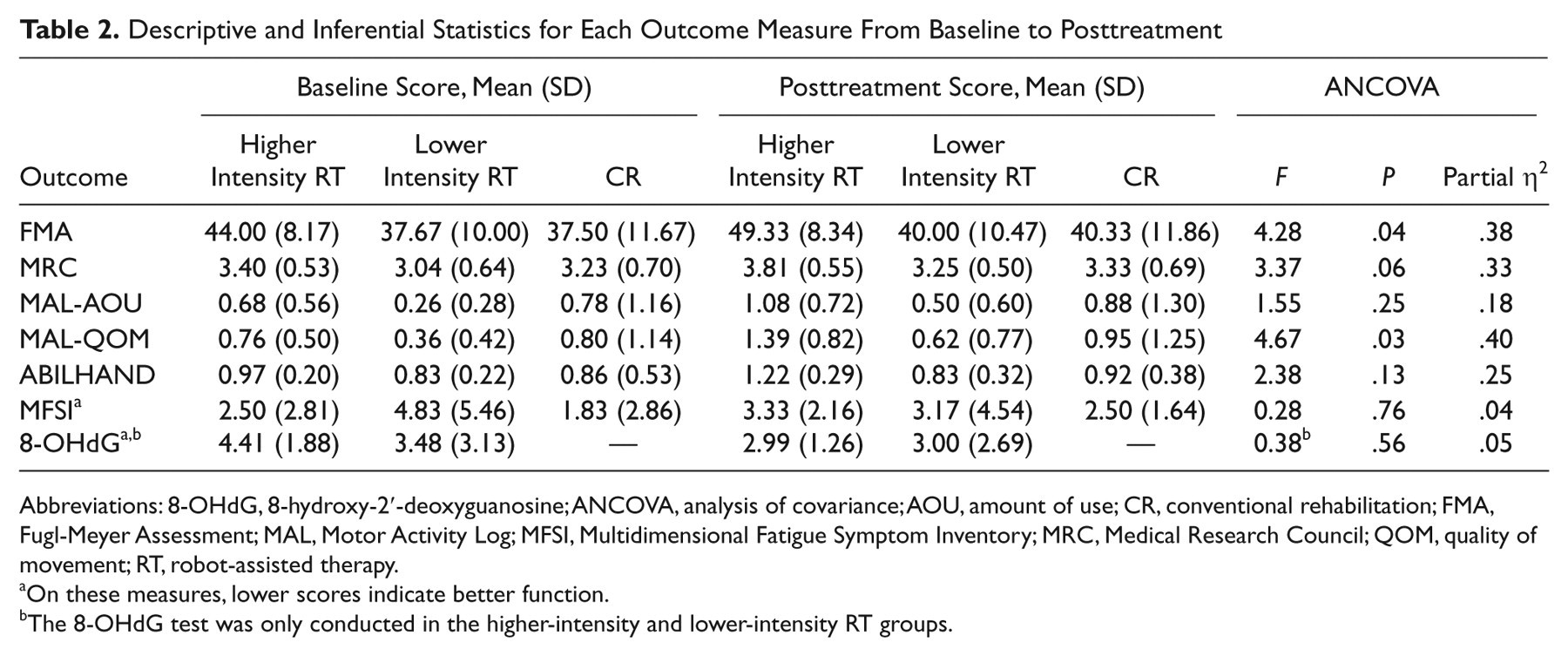
Abbreviations: 8-OHdG, 8-hydroxy-2′-deoxyguanosine; ANCOVA, analysis of covariance; AOU, amount of use; CR, conventional rehabilitation; FMA, Fugl-Meyer Assessment; MAL, Motor Activity Log; MFSI, Multidimensional Fatigue Symptom Inventory; MRC, Medical Research Council; QOM, quality of movement; RT, robot-assisted therapy.
On these measures, lower scores indicate better function.
The 8-OHdG test was only conducted in the higher-intensity and lower-intensity RT groups.
For the secondary outcomes, a significant difference in the MAL-QOM (ie, quality of movement during daily activities) among the 3 groups was observed (P = .03, partial η2 = .40). Post hoc analyses showed that the higher intensity RT group had significantly larger improvements in the MAL-QOM than the CR group (P = .02). In addition, although the between-group differences were not significant in the MAL-AOU and ABILHAND, large effects were found (partial η2 = .18 and .25). To sum up, there is a trend that the mean improvement scores from baseline to posttreatment in the higher intensity RT group on the primary and secondary outcomes are higher than those in the lower intensity RT group and the CR group.
For the safety outcomes of 8-OHdG and MFSI, there were no significant differences among the 3 groups, and the before-to-after effects were small (Table 2). No treatment-related serious adverse events were reported. Most participant ratings of fatigue were low. According to the average score, the lower intensity RT group reported decreased fatigue (pre = 4.83; post = 3.17), and the higher intensity RT (pre = 2.50; post = 3.33) and CR groups (pre = 1.83; post = 2.50) showed slightly increased fatigue after intervention. Urine samples were collected in 10 patients in the RT groups. The 8-OHdG level in most patients decreased or showed nearly no change after treatment. The mean changes of the 2 groups showed decreased 8-OHdG levels after treatment (−1.42 and −0.48 ng/mg creatinine), indicating that the intensive RT training did not cause oxidative damage to the patients.
Discussion
Most patients demonstrated improvement in motor ability and functional performance after treatment. Patients in the higher intensity RT group had better outcomes than those in the lower intensity RT group and the CR group on UE motor function, muscle strength, performance of daily function, and bimanual ability. Compared with the CR group, the lower intensity RT group performed better on the MRC and the MAL. The lower intensity RT and the CR groups had a similar degree of changes in the FMA and the ABILHAND. Furthermore, the higher intensity RT intervention seemed not to induce deleterious effects of oxidative stress. These interventions, then, can be tolerated by chronic stroke patients with moderate to mild motor deficits.
In agreement with one previous trial that used the Bi-Manu-Track, 5 the RT protocols used in our study led to greater improvement in UE motor function and muscle strength than the control intervention. In addition, there were 5.3-point gains on the FMA after the higher intensity RT intervention (within-group, although the FMA at baseline was higher than the other groups) and a mean difference of 3 points on the FMA between the higher intensity RT group and the other 2 groups (between-group). The amount of the difference on the FMA reached what some consider to be the level of minimal clinically meaningful. 49 More improvement in muscle strength after the RT than the CR intervention was also observed. The Bi-Manu-Track provided adjustable resistance and principles of progressive resistance exercise was incorporated into treatment, which may contribute to the improved muscle power after RT. However, our beneficial effects of RT on motor function did not corroborate the findings of 2 studies using the MIT-MANUS. 7,9 The differential results may be attributable to differences in motor severity of patients, sample size of studies, and the use of unilateral versus bilateral robotic devices. Unilateral and bilateral interventions for the UE may have different mechanisms of neuroplastic changes even though the degree of motor improvement was similar. 50
No significant differences in functional or disability outcomes between the RT and control groups have been reported in some previous studies in which they did not provide additional functional training in the experimental RT groups. 8,9 In contrast to previous studies, this study combined functional training (15-20 minutes for each session) with the RT, which may have helped patients to transfer the acquired motor ability and strength into the use of the affected UE in daily activities and thus gain improvements in the MAL-QOM. Compared with the EXCITE trial’s criteria for clinically meaningful changes on the MAL-QOM (a score of ≥3 after treatment), 17,29 the data in our study did not reach clinically important changes. However, when using another criterion in which 10% of the score (ie, 0.5 points) was set as minimal clinically important, 51 0.63-point gains on the MAL-QOM in the higher intensity RT group can be viewed as clinically relevant. In addition, MAL scores were low in our patients with mild to moderate motor deficits. The primary reason might be that many stroke patients developed learned nonuse of their affected UE, resulting in a discrepancy between what stroke patients can do and how much they actually do. 52-54 Further studies should emphasize the actual use of the affected UE in daily activities as home programs and incorporate the use of accelerometers to evaluate the real-world performance of patients.
We investigated not only the positive benefits but also potential adverse effects of the intensive RT intervention. Our pilot results showed that the urinary 8-OHdG levels of the patients were not significantly changed and tended to be decreased after RT, indicating the regular RT protocols of this study may be appropriate to patients with chronic UE paresis without inducing oxidative stress. Some previous studies showed an increased 8-OHdG level after heavy or extreme exercise (ie, exercise capacity had 75% maximal oxygen consumption or long-distance running), 23,55 whereas some demonstrated no change in 8-OHdG level after exercise (ie, a short-distance triathlon or progressive resistance training). 56,57 The discrepant effects of exercise on oxidative stress may be partly due to the type and intensity of exercise studied and the patients studied. Because the 2 RT protocols for UE training used in this study were likely to be modest in intensity, the 8-OHdG levels had no significant change after RT. The 8-OHdG appears to be a promising biomarker of oxidative stress, but more studies are needed to clarify its responsiveness to intensive rehabilitation interventions in stroke patients. 58 Furthermore, translating the dosages of high-intensity training from animal models to patients with stroke to balance the efficacy and safety issues of novel treatments in does–response studies is critical in furthering neurorehabilitation research.
Some limitations of this study should be mentioned. First, this study is a pilot trial with a sample representing a small percentage of all stroke patients, which limits the generalization of the findings. The positive preliminary results do provide a justification for conducting a larger trial. According to the findings of this study and a previous study 5 on motor function, the effect size f ranged from 0.40 to 0.78. An estimate of sample size requirements for each group in a 3-group study design given a power of 0.80, and a 2-sided type I error of 0.05 was in a range of 7 to 21 patients. A future efficacy trial should consider recruiting 20 to 25 patients for each group for interventions of at least 4 weeks. Second, the outcome assessments were administered immediately after the intervention. Further studies should include later follow-up for retention. Third, this study did not precisely measure the intensity of the CR group. Further studies have to define the number of repetitions in the activity-based treatment programs per session 16,18 and provide the intensity of the CR for comparison with the RT. In addition, although this small study randomized subjects, the higher intensity RT group had higher baseline FMA and MRC scores, which may have biased the outcomes. Further larger studies may use stratified randomization based on motor impairment levels of patients to avoid potential selection bias. The preliminary results showed promise for continued study of the specific effects of RT and investigation of dose–response relations.
Footnotes
Yu-wei Hsieh and Ching-yi Wu have contributed equally to this work.
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This project was supported in part by the National Health Research Institutes (NHRI-EX99-9920PI and NHRI-EX99-9742PI) and the National Sciences Council (NSC 96-2628-B-002-033-MY2, NSC 97-2314-B-002-008-MY3, and NSC 97-2314-B-182-004-MY3) in Taiwan.