
Abstract
Background:
Effectiveness of antiretroviral therapy (ART) in a routine clinical care may result different from the clinical trials. We assessed the virologic outcomes in treatment-naive persons who received either efavirenz (EFV) or atazanavir/ritonavir (ATV/r) with a backbone of tenofovir/emtricitabine (TDF/FTC) as their combination ART (cART).
Methods:
This was a retrospective cohort study conducted at the Washington University HIV Outpatient Clinic from January 2004 to June 2009. Predictors of virologic suppression (HIV RNA level <400 copies/mL) by week 48 were assessed by multivariate Cox proportional hazards regression models.
Results:
Of 324 persons, 221(68%) received EFV and 103 (32%) received ATV/r. Persons on EFV had 1.4-fold increased likelihood of virologic suppression (95% confidence interval, 1.0-1.8) when compared to ATV/r after adjustment with primary drug resistance, pre-cART opportunistic infection, HIV RNA levels, and timing to start cART.
Conclusions:
In routine clinical care settings, EFV had higher likelihood of achieving virologic suppression than ATV/r with backbone of TDF/FTC.
Introduction
After the introduction of combination antiretroviral therapy (cART), adherence, and hence long-term success, was challenging due to tolerability, toxicity, and pill burden. 1 Subsequently less toxic, better tolerated antiretroviral (ARV) agents have been developed, and many regimens are dosed once daily (QD) or twice daily (BID) with a modest pill burden. 2 The recently published US guidelines recommend the combination of tenofovir/emtricitabine (TDF/FTC) as a choice for nucleoside reverse transcriptase inhibitor (NRTI) paired with a third agent from 1 of the 3 classes of ARVs. 3 A recent AIDS Clinical Trial Group (ACTG) study compared the efficacy of efavirenz (EFV) to atazanavir/ritonavir (ATV/r) when they were given with either TDF/FTC or abacavir/lamivudine (ABC/3TC) in which no difference was seen in terms of virologic suppression (90% vs 89% at week 96 on TDF/FTC and 85% vs 83% at week 96 on ABC/3TC). 4 Another study also demonstrated equivalent virologic suppression and safety of EFV and ATV/r with a backbone of TDF/FTC (95% vs 96% at week 48). 5
One of the difficulties of interpreting clinical trials is that those enrolled in the trials may not reflect patients seen in the routine clinical care. Selection biases do exist and the patients in clinical trials are monitored frequently to ensure their adherence to the study protocol. 6 Both of the studies mentioned above excluded patients with primary drug resistance, but 15% of the persons newly infected with HIV in the United States have primary drug resistance. 7 Therefore, we also do not know the true efficacy of these ARV regimens in routine clinical care settings. The present study was conducted to compare the effectiveness of the 2 standard QD cART regimens in naive patients seen in an outpatient clinic; EFV or ATV/r with a backbone of TDF/FTC.
Methods
This was a retrospective cohort study utilizing the medical records of treatment-naive HIV-1-infected persons followed at the Washington University HIV Outpatient Clinic from January 2004 to June 2009. Data were collected for those who met the following criteria: documented HIV-1 infection, age ≥18, treatment naive. Persons included in the analyses were initiated on (1) ATV 300 mg, ritonavir (RTV) 100 mg plus TDF 300 mg/FTC 200 mg QD or (2) EFV 600 mg/TDF 300 mg/FTC 200mg QD. This study was approved by the Washington University School of Medicine Human Research Protection Office.
The following data were abstracted from the electronic medical record: demographic information, baseline genotype, psychiatric comorbidities, active illicit drug use (marijuana, cocaine, heroin, and methamphetamine use), hepatitis C virus (HCV) infection (positive anti-HCV antibody), chronic hepatitis B virus infection (positive hepatitis B surface antigen), pre-cART opportunistic infections, longitudinal CD4 counts, and HIV RNA levels. Genotypic resistance testing prior to cART were also abstracted and interpreted with transmitted drug resistance mutation list provided by the World Health Organization (WHO). 8 Virologic suppression was defined as HIV RNA level <400 copies/mL by 48 weeks.
Statistical Analysis
Differences between the groups were compared using chi-square (χ 2 ) test and Fishers exact test for categorical data and Mann-Whitney tests for nonparametric continuous data. The HIV RNA level was log10 transformed. Statistical significance was defined as P <.05. To assess the virologic outcomes, univariate analyses with a Cox model with 1 predictor was conducted. Thereafter, predictors associated with virologic failure at P <.10 in the univariate analyses were considered in the multivariate Cox proportional hazards regressions models. Persons who did not achieve virologic suppression by 48 weeks were censored at that time. All statistical calculations were made using PASW Statistics 18.0.2 (IBM Corporation, Somers, New York).
Results
A total of 221 persons were initiated on EFV and 103 persons on ATV/r with a backbone of TDF/FTC. Persons initiating EFV were older (36 years vs 30 years, P <.01), more likely to be male (77% vs 64%, P = .02), and more likely to smoke (64% s 52%, P <.05) than those initiating ATV/r. The ATV/r group had more NRTI -resistance in the baseline genotypic resistance testing (P < The incidence rate of VAP went from 9.88 occurrences/1000 vent days in 2009 .05). Nonnucleoside reverse transcriptase inhibitor (NNRTI) resistance was also significantly more seen in the ATV/r group, which was expected. Psychiatric comorbidities, active drug use, and alcohol use were not different between the 2 groups (Table 1). Multivariate analyses revealed that receipt of EFV was independently associated with greater likelihood of achieving virologic suppression by week 48 when compared to ATV/r (hazard ratio [HR], 1.4; 95% confidence interval [CI], 1.0-1.8). Initiation of cART <120 days from the first clinic visit (engagement to care) was independently associated with virologic suppression (HR, 1.6; 95% CI, 1.2-2.1). Other factors associated with lower likelihood of virologic suppression included having a pre-cART opportunistic infection (HR, 0.7; 95% CI, 0.5-0.9) and HIV RNA level of >100 000 copies/mL (HR, 0.7; 95% CI, 0.5-0.9; Table 2). In this model, NNRTI resistance was not included in the multivariate analysis due to high correlation with the receipt of ATV/r.
Baseline Characteristics of the Study Population.
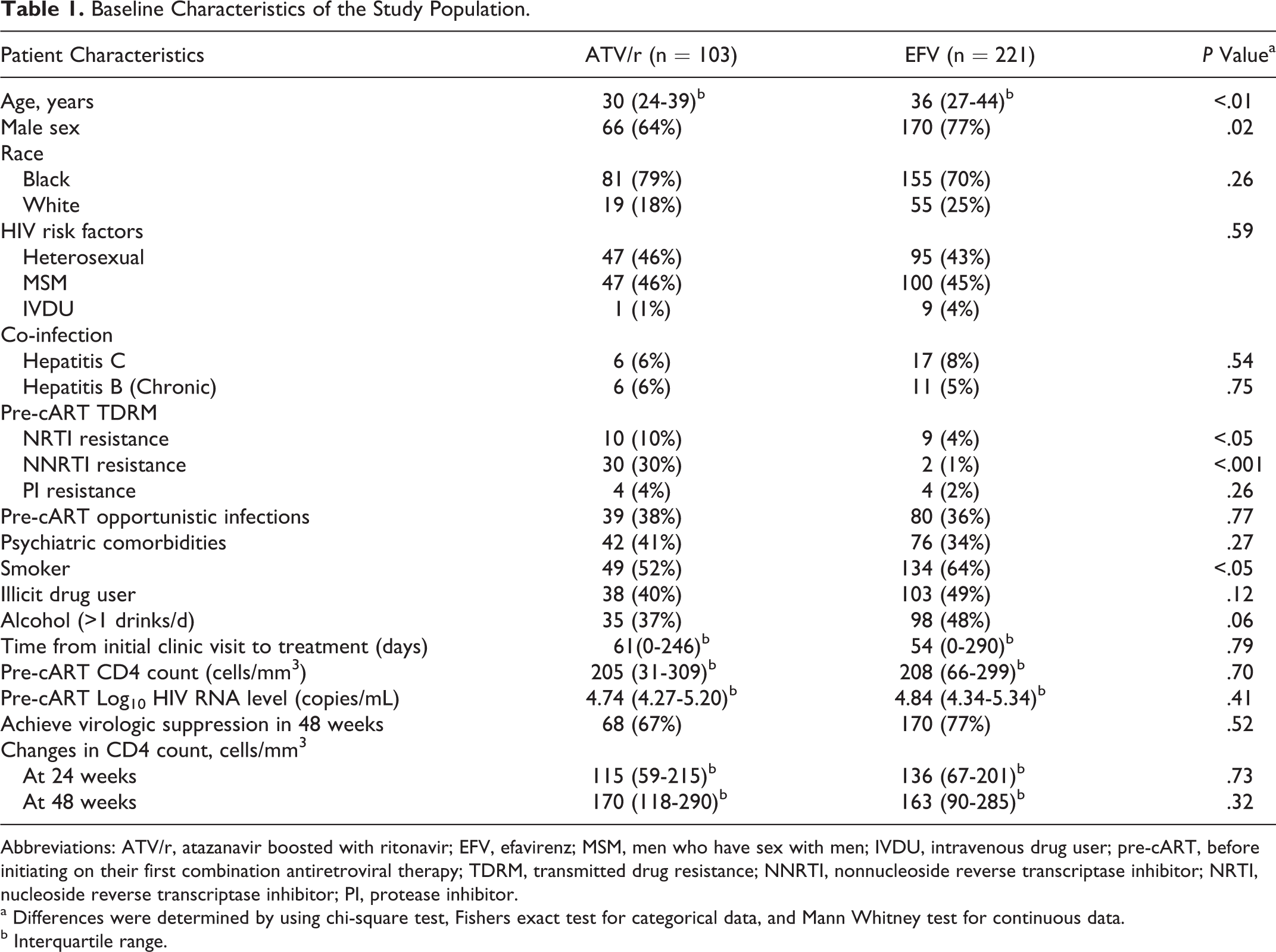
Abbreviations: ATV/r, atazanavir boosted with ritonavir; EFV, efavirenz; MSM, men who have sex with men; IVDU, intravenous drug user; pre-cART, before initiating on their first combination antiretroviral therapy; TDRM, transmitted drug resistance; NNRTI, nonnucleoside reverse transcriptase inhibitor; NRTI, nucleoside reverse transcriptase inhibitor; PI, protease inhibitor.
a Differences were determined by using chi-square test, Fishers exact test for categorical data, and Mann Whitney test for continuous data.
b Interquartile range.
Univariate and Multivariate Analyses of Predictors for Virologic Suppression.

Abbreviations: HR, hazard ratio; CI, confidence interval; ref, reference; ATV/r, atazanavir with ritonavir; EFV, efavirenz; pre-cART, before initiating on their first combination antiretroviral therapy; cART, combination antiretroviral therapy; NRTI, nucleoside reverse transcriptase inhibitor.
Discussion
Among the HIV-1-infected treatment-naive persons in a routine clinical care, our data showed that persons who were initiated on EFV had 1.4-fold increased likelihood of achieving virologic suppression compared to ATV/r when TDF/FTC was used as a backbone.
This finding is in contrast to the recently published data from randomized control trials which reported equivalent efficacy of EFV and boosted ATV.9,5 However, given the potential selection bias of clinical trials related to underlying primary resistance as well as often challenging enrollment inclusion and exclusion criteria, the results may fail to reflect what happens in routine clinical practice.
Decisions regarding the prescription of ARV drugs are influenced by numerous factors, including the simplicity of the regimen and the perception of the likelihood of patient adherence. The fixed-dose combination of EFV and TDF/FTC provides the simplest cART regimen for effective HIV treatment. An ATV-based regimen, while given QD, nevertheless has a pill burden of 3 pills, which may compromise adherence success. However, other factors may contribute to the greater success we report with EFV. Given the teratogenic concerns with EFV, young women are often preferentially initiated with a protease inhibitor (PI)-based regimen. Additionally, the age difference may explain, to some degree, our findings; younger persons have been found to have poorer adherence 10 and in our study, ATV/r group was significantly younger than the EFV group. Although there were no differences in our study, we often opt to give patients with psychiatric comorbidities a regimen that does not contain EFV. We may be choosing ATV-based regimen for our more challenging patients. These selection biases may impact the results seen in clinical practice.
The length of time from engagement of care to initiation of cART does matter; initiating earlier than 120 days had 1.6-fold increased likelihood of achieving virologic suppression. The time to initiate HIV treatment is multifactorial including social stability, CD4 count at the time of engagement to care, and other comorbidities that may delay the treatment. Complexity of the patient with delayed HIV treatment may explain the worse outcome. Although CD4 count did not predict virologic suppression in our study, the presence of opportunistic infection before initiating cART conferred 1.4-fold increased risk of virologic failure. This may be an additional complexity of HIV care resulting in worse outcome. High plasma HIV RNA level is well documented as a risk for virologic failure. 11
Another interesting finding was that baseline NRTI resistance was more prevalent in the ATV-based regimen group. Since persons receiving ATV had more NNRTI resistance, the presence of these mutations may be a proxy for other NRTI-resistant mutations that were not detected in commercially available genotypic assays. This could potentially explain the difference in the virologic suppression between boosted ATV and EFV. Therefore, we think HIV-infected persons with primary drug resistance should be monitored closely.
There are several limitations for this study. This is a single site, retrospective study; therefore, the number of patients in our data is small. We were unable to measure adherence to the cART regimen. This could be an important factor that may explain the inferiority of ATV-based regimen because of its additional pill burden.
In conclusion, in treatment-naive HIV-infected persons initiating on cART in a routine clinical care, EFV had 1.4-fold higher likelihood of achieving virologic suppression when compared to ATV/r with a backbone of TDF/FTC.
Footnotes
Acknowledgments
We thank the staff at the Washington University Institute of Clinical and Translational Sciences and the patients and staff at the Washington University HIV Outpatient Clinic.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ETO reports that he has served as a consultant, in speakers bureau, or in an advisory board for the following companies: Gilead, Bristol Myers Squibb, GlaxoSmithKline, Tibotec, Merck, Monogram Sciences, and Boehringer Ingelheim. He also reports that he has received research support from the following companies: Abbott, Gilead, Bavarian Nordic, GlaxoSmithKline, Boehringer Ingelheim, and Tibotec. All other authors: No competing financial interests exist.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Washington University School of Medicine, Department of Medicine, Division of Infectious Diseases.