
Abstract
Dramatic increases in the evidence-base for intervention approaches to support antiretroviral therapy (ART) adherence have resulted in numerous reviews, syntheses, and guidelines/recommendations. This review characterizes the current state of the literature and identifies areas in need of additional targeted focus to better align research and practice. Leading recommendations for the process of intervention development (relevant to both rigorous research and real-world intervention planning) and strategies to consider in working with individuals, communities, and systems are provided. In order to move systematically toward the identification of what kinds of interventions work best for whom and when, attending to both intervention outcomes and “drivers” of observed effects or lack of effects in controlled research is critically important. Further, evidence emerging from practice should be aggressively added to research agendas to promote better synergies between the practice and research communities.
Introduction
Expanding HIV testing and heightened investment in treatment has dramatically increased the numbers of people living with HIV (PLWH) who have access to lifesaving antiretroviral (ARV) medication. Data from 2010 estimated that 34 million people were HIV positive and in low- and middle-income countries 6.65 million PLWH were on ARV medications. 1 While the personal health benefits of ARV medications are well recognized, 2 the effects of early treatment in averting HIV transmission is now an additional goal of treatment based on HPTN052’s reported 97% reduction in HIV-infection among partners of PLWH who initiated ARV treatment at CD counts of 550 cells/mm versus 250 cells/mm (the standard used at the time of the study). 3 However, adherence insufficient to achieve viral suppression creates a gap between potential and the realized personal or public health benefits of ARV therapy.
Antiretroviral therapy (ART) adherence has been the focus of targeted attention since the wide-scale availability of ARVs and the “Achilles Heel” of treatment success. 4 Early work in ART adherence clearly identified medication-related barriers to adherence where near perfect adherence was needed for regimens that were dosed 3 times daily and often had challenging side effects, including appearance of altering fat redistributions and persistent gastrointestinal discomfort. 5 , 6 Advances in ARV therapy development have dramatically changed the tolerability of ART, and numerous first-line therapies are presently available that involve single co-formulated tablets and daily dosing. While regimen simplification is associated with higher adherence, 7 , 8 adherence continues to challenge a sizable proportion of those on ART. In one evaluation, some 40% of those on ART do not achieve the recommended rates of ART use. 9 A recent review of viral suppression outcomes among over 32 000 patients in the United States suggested that sustained viral suppression in those treated with ART improved from 45% in 2001 to 72% in 2010, 10 likely attributable in part to increasing availability and use of simplified and tolerable regimens. Conversely, even with the improved regimens presently available, over a quarter of individuals treated failed to achieve sustained viral suppression.
Numerous factors extending beyond the characteristics of the patients and regimens influence adherence, giving rise to a diverse literature of health behavior models and behavioral and structural interventions to promote adherence and treatment success. Numerous health behavior models have been developed for or applied to ART adherence in efforts to understand the driving determinants of optimal and sustained use of ART. 11 These highlight the complexities of adherence as a self-directed time-indefinite personal and social behavior. Numerous intervention approaches have been developed and evaluated drawing from these and other models. Generally, interventions appear to be effective 12 , 13 but the diversity in approaches and outcomes in the published literature limits clear delineation of what discrete strategies work and, more importantly, what works best for who and when. Because recommendations for the use of interventions to support adherence are included in a number of treatment guidelines 14–16 with relatively sparse guidance on what to target or consider in approaches for intervention, we provide a brief overview of potential determinants of ART adherence and a summary of effective and promising approaches to promoting adherence and provide recommendations for both research and practice communities.
What to Address in Adherence Interventions?
In considering strategies to promote ART adherence, it is helpful to first identify the targets of a given intervention (what will be changed or supported in order to improve or sustain high rates of adherence) and then consider how to impact those targeted factors (specific intervention strategies or approaches). Obviously, the ultimate target is adherence and its persistence over time. Short of direct delivery and observation of each dose or the development of some delivery mechanism that bypasses self-directed dosing behaviors, interventions must work with the factors that lead to good adherence or the mitigation of factors that deter adherence. Thus, identifying what to target in an intervention precedes consideration of how to actually do this, and the extent to which targeted factor/factors actually relate to adherence in many ways sets the upper limit for ultimate efficacy of an intervention approach.
There are a number of discrete factors that have been associated with ART adherence. Across populations, these include accessibility of experience of side effects, availability of resources (including food, finances, and transport to HIV care), knowledge/literacy concerning the condition and its treatment, stability of daily schedule/routine, social support and stigma, positive and negative beliefs about medications, coping, depression, competing priorities and substance use, medication management skills, executive memory and cognitive functioning, simply “forgetting,” and consistent source for medications and use of them. 17–22 Arguably, these individual level correlates are contextualized by the social–cultural context of living with HIV and community-level beliefs more generally about medical establishments treating HIV. Further, with so many discrete correlates of adherence identified, higher order organization of these correlates into models of health behavior offers multiple benefits, such as allowing for more targeted intervention approaches and appropriately contextualizing individual behavior in the context of larger social, cultural, and structural systems.
Models of adherence that combine discrete correlates and situate individual behavior in larger contexts have been proposed and offer some guidance toward identifying common “drivers” of adherence. A basic taxonomy suggested in the late 1990s continues to provide a useful heuristic for considering determinants of adherence: aspects of the patient, aspects of the provider and patient–provider relationship, aspects of the regimen and illness, and the contextual (environmental, structural, community) factors that influence adherence. 23 Health behavior models typically draw from across these general areas to identify core factors that while housed within the individual are the net result of previous and ongoing interactions with others (important others, HIV care providing staff, communities) and with systems of care. While no single behavioral model has been identified as effective in predicting adherence (see for example the study by Amico et al 11 ), when considering intervention strategies the articulation of an underlying model is essential for identifying what to target (what aspects of the person, social interactions, system of care, or regimen should be addressed by the intervention) and why it would be expected to positively impact adherence. Across behavioral models, common critical determinants of adherence include knowledge, attitudes, beliefs, perceptions of benefits and costs, social support, past and current experiences with care providers, real and perceived burdens to adherence and several executive functions like developing skills, negotiation of behavior in common situations, coping, and regulation of perceived threats to health. Determinants of adherence likely have commonalities between cultures and geographies but also unique factors emerging from unique culture and community systems (see for example the work of Simoni et al 19 ).
Behavioral models typically attempt to explain the behavior, whereas “how” to influence change on any of the identified core determinants of adherence requires additional consideration. Numerous models identifying strategies to promote change on the individual, community, and structural level are available (eg, motivational interviewing, 24 , 25 cognitive behavioral therapy strategies, 26 peer delivery models, 27 community health workers (CHWs), 28 , 29 or technology 30–33). In order to identify effective and not-effective strategies for promoting adherence, both the explanatory and the intervention delivery models adopted need to be identified. Failed intervention approaches may be ineffective because they did not change the targeted factor (eg, participants or patients did not develop new skills) or the intervention was effective in promoting change in the targeted factor, but the factor itself was not sufficiently or uniquely related to adherence for a given population (eg, new skills were developed but the development of new skills was not related to improved adherence). Additionally, the needs of a given population (eg, are rates of adherence currently suboptimal, are the barriers targeted by an intervention actual barriers in the study sample?) or lack thereof effects outcomes and must be carefully considered. Tremendous resources are allocated to rigorous research on approaches to adherence support. Whereas much of the literature currently available determines effects of a given intervention approach on the basis of intent to treat and additionally as treated, the identification of what the intervention changed or failed to change within what kind of cohort and whether success, or failure, can be attributable to one or more of these factors is less often included (see for example the study by de Bruin et al 34 ). However, we would argue that this level of granularity is essential to promoting systematic progress toward identifying strategies that are effective in promoting high and consistent adherence. At minimum, research should clearly articulate the targets of their interventions and present data relevant to the success of the intervention in influencing those targets; strategies adopted in practice should similarly identify what a strategy or approach addresses, why it would be expected to influence adherence in a given population, and monitor for success in influencing the targeted factors.
The process of identifying what explanatory models appear to be more reflective of adherence in a certain patient population and which delivery model would offer greatest benefit can involve substantial adaptation. Intervention mapping 35 offers a systematic process for intervention development that can provide guidance for this process with the advantages of producing clear delineation of what will be targeted for change or support and how. Adapting models developed to explain adherence predominantly for one population (eg, PLWH in the United States) to a different population (eg, PLWH in Uganda) can be guided by Ware et al’s 36 suggested process where 4 basic questions provide an evaluation of validity for a model: (1) Are the model concepts relevant to the new setting? (2) Are the concepts relevant in the new setting well represented in the model? (3) Do the definitions of the concepts in the model have accuracy in the new setting? and (4) Is the model comprehensive enough to explain the full complexity of adherence in the new setting? Intervention mapping and vetting model validity are both exercises that can benefit research and practice through re-focusing intervention efforts on specific populations and attending to the social–cultural context in which adherence is negotiated. The need for better articulation of the phenomenon of interest has been identified for some time (see for example the article by Bain-Brickley et al 37 ), but there continues to be a general lack of targeted efforts to evaluate the general strength and accuracy of the behavioral models that underlie intervention efforts.
Strategies and Approaches for Promoting ART Adherence
The literature pertaining to evaluation of comprehensive intervention packages has grown dramatically over the past decade. In 2003, Simoni and colleagues 38 summarized adherence interventions evaluated through January 2003, identifying only 4 studies with sufficient rigor in randomized controlled trials (RCTs) to provide evaluation of the intervention approach. Only 3 years later, 2 meta analyses included 16 RCTs 13 and 24 within-group studies and RCTs 12 providing sufficient data to determine effect of adherence. Updated through 2007, the pool of qualifying within-group and RCT studies increased to 48 39 with other reviews also noting the sharp increase in adherence intervention–focused literature (13 new intervention studies from September 2007 to October 2009 40 ). Reflecting this expanding evidence base, multiple reviews have provided insights specific to certain aspects of research, including distilling effects of quality adherence support and within special populations.
A meta-analysis focused on determining the relationship of implementation of strategies that quantified standard care quality and success (undetectable viral load) provided a novel way of evaluating effects of different kinds of adherence support in 13 different studies meeting criteria for inclusion in these analyses. 41 Across these, activities targeting adherence were classified into 7 basic targets (or determinants); activities targeting knowledge, awareness of general and individual-specific rates of adherence and nonadherence, attitudes, self-efficacy, intentions, action control (eg, reminder strategies, adherence plans), and general facilitation (eg, side effects management, home delivery of medication, regimen simplification). Within each target area, the authors identified a number of discrete techniques or strategies used in the evidence base of available interventions, each associated with a specific score. Total scores across these strategies determined the overall quality score which was associated with undetectable viral load. These findings are particularly interesting in that care quality, across intervention and control conditions, related to virologic success, calling to attention the need to consider intervention outcomes as relative to what the standard of care control condition had available in terms of adherence support.
Focusing on intervention approaches implemented with PLWH in sub-Saharan Africa through January 2011, Barnighausen and colleagues 42 reviewed 26 studies, concluding that numerous intervention approaches, including the use of diary cards, food rations, treatment supporters, and text messaging, have received support. These authors recommended that strategies leveraged to address barriers to adherence need to be linked specifically to the resources and resource limitations of a given patient population. Reviewing studies using directly observed therapy (DOT) there have been conflicting results, with Ford and colleagues 43 suggesting nonsignificant overall effects (12 studies through July 2009) and Hart and colleagues 44 found DOT participants within group and RCT trials to have significant gains in viral load, CD4, and adherence (17 studies through August 2009) although these gains were nonsignificant when restricted to only RCTs. Reviewing only studies using CHWs in the United States, Kenya and colleagues 29 concluded the these intervention strategies using over 24 weeks of CHW contact and medication management appeared to be successful in improving adherence and reducing viral load (16 studies from May 2010 to November 2010). Rueda and colleagues’ 45 Cochran review of 19 RCTs similarly identified medication management skills as particularly promising as an approach for the general clinic population. These authors also suggested that intervention delivered over 12 weeks or more and working with individuals versus groups may be more effective.
Systematic reviews of interventions are also available for youth and pediatric adherence, 46–48 adherence during pregnancy, 49 methamphetamine using men who have sex with men, 50 and other populations. Increasingly, syntheses of studies using specific intervention delivery approaches are emerging, with several reviews currently available for DOT and use of CHWs, as noted above, as well as contingency management, 54 motivational interviewing-based interventions, 24 mobile phone text messaging, 30 , 31 and cognitive behavioral interventions. 55 Accessing these reviews and the separate studies they draw from are important first steps in identifying unmet needs and the relative success of various intervention approaches within a special population or cohort.
National and international guidelines also provide general and specific suggestions for practice communities. International guidelines recently released 53 provide a number of recommendations for strategies found to be effective in the evidence-graded literature concerning adherence monitoring and support approaches, as well as for linkage and retention in HIV care. Specific to ART adherence support and promotion, these recommendations include provision of basic adherence tools (reminder and organization devices) and individual education and counseling, and offering group counseling, multidisciplinary support, and peer support. Each recommendation is graded for its quality of evidence (methodological rigor and strength of outcomes in the evidence base) and strength of recommendation in terms of scope of recommended strategy (does the recommendation apply to all, most, or some patients). Special populations, including pregnant women, substance abusers, those with comorbid mental health conditions, incarcerated individuals, homeless, and children and adolescents, have recommendations specific to work, targeting these groups. While monitoring and support ART adherence has long been included as a part of guidelines for providing ART, these guidelines are the first to offer concrete recommendations for how to do so.
Recommended processes to generate targeted adherence support and specific approaches culled from the literature are offered in Tables 1 and 2, respectively. We note that the sources provided in Table 1 are not intended to be exhaustive, nor are all recommendations, syntheses, or guidelines included. The recommendations are frequently encountered in the literature as well as in research and practice discussion groups. Many of these recommendations are straight forward and relatively inexpensive in terms of resources to implement. In addition to discrete strategies for support, the Centers for Disease Control's (CDC's) evidence-based interventions (EBIs) have recently been expanded to include a chapter on ART adherence interventions (http://www.cdc.gov/hiv/topics/research/prs/ma-chapter.htm). This compendium draws from peer-reviewed literature to identify interventions that meet criteria for best or good evidence specifically for work conducted in the United States or a US territory. Identified interventions are then “packaged” so that agencies can use the intervention approach in full. Manuals and technical assistance facilitate this process. Presently, there are 8 interventions identified as having “good” evidence, with no intervention meeting “best” evidence criteria. Good interventions include the use of nurse-delivered home visits, 57 couples-based counseling, 58 individual and group counseling, 59 , 60 peer support, 61 and 2-way texting. 61 Additionally 2 DOT interventions specifically evaluated with drug-using populations are identified as “good.” 62 , 63 Intervention package information for any of these interventions was listed as not yet available as of early 2012.
Bridging Research and Practice: Adding Practice-based Evidence to the Equation
As can be seen from Tables 1 and 2, recommendations that have substantial “face validity” and intuitive appeal are not necessarily well supported by an established research base, predominantly due to a lack of evaluation versus evaluations that demonstrate null findings. Similarly, using a parachute when jumping from a plane lacks an evidence base and nonetheless is a well-adopted, arguably effective, practice. 64 While effects of behavioral intervention certainly lack such dramatic or definitive outcomes as use and nonuse of a parachute, the recognition that not all successful strategies are those identified and demonstrated in rigorous research trials is important. It is well recognized that in practice patient needs for adherence support do not go unmet while we wait for sufficient research guidance. Rather, clinics and care providers innovate based on available resources and knowledge to develop strategies, individual and systems level, to support patient populations. de Bruin’s 41 work suggests that practices adopted in “standard of care” comparison arms in RCTs can have equally, even more, effective adherence approaches than the intervention condition. Recent work evaluating standard of care practices for ART and retention in care support suggests that a number of approaches are in place to meet patient needs in most clinical care centers. 71 Whereas evidence-based practice largely has been defined as a process in which research identifies effective support approaches and practice then adopts them, an alternative way of conceptualizing the collaboration of research and practice is to use research methods to evaluate the interventions already in place in practice (practice-based evidence).
Designing Intervention Processes.

Strategies to Promote ART Adherence from Published Reviews, Syntheses, and Guidelines.a
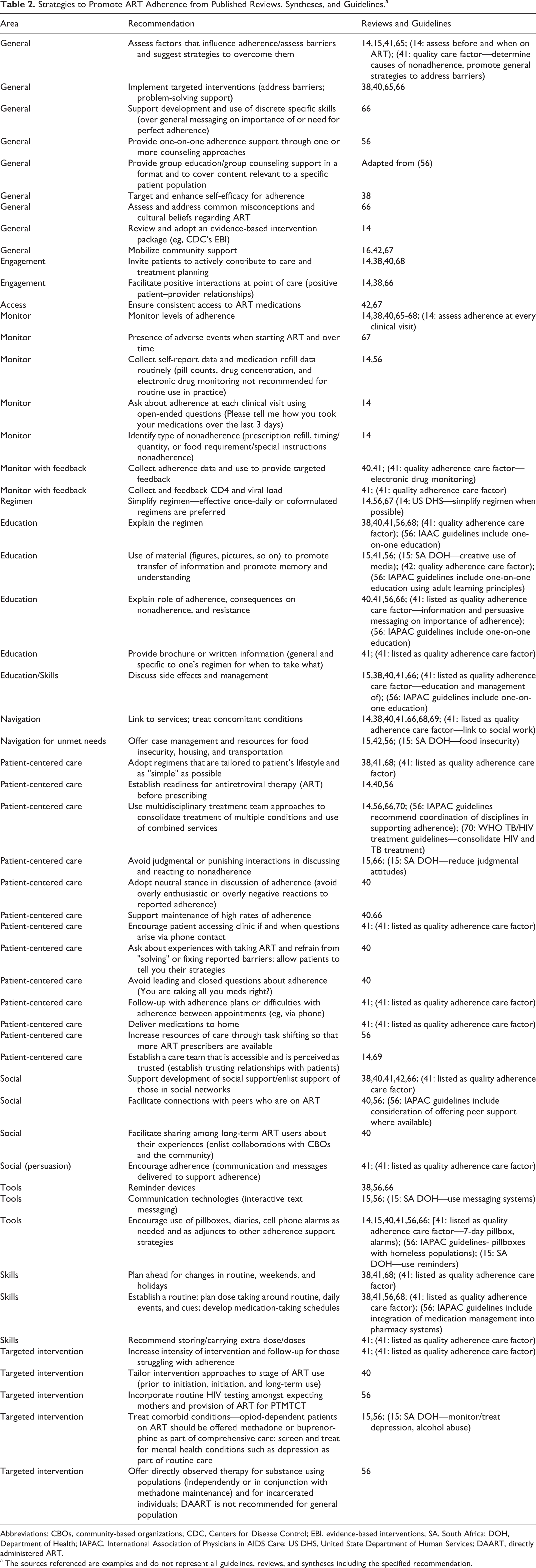
Abbreviations: CBOs, community-based organizations; CDC, Centers for Disease Control; EBI, evidence-based interventions; SA, South Africa; DOH, Department of Health; IAPAC, International Association of Physicians in AIDS Care; US DHS, United State Department of Human Services; DAART, directly administered ART.
a The sources referenced are examples and do not represent all guidelines, reviews, and syntheses including the specified recommendation.
The call to expand the focus of behavioral intervention research to include the vital process of adopting and implementing evidence-based strategies and to develop methodologies for evaluating practice-based strategies is not new. 72–75 However, guidelines and strategies for equipping practice and research communities with the resources and technical expertise to develop a practice-driven evidence base are generally lacking. Processes such as intervention mapping 35 , 53 or systems thinking 51 offer steps to constructing, applying, and evaluating intervention approaches leveraged in practice that may be very useful in these endeavors. Over the next decade, a better characterization of standard of care for adherence, and retention in HIV care, in diverse regions and with diverse patient groups would be beneficial in directing research agendas. Redefining collaborations between research and practice to aggressively establish a practice-driven evidence base could have dramatic effects on consolidating resources and synergizing areas of expertise.
Conclusions
The evidence base for effective adherence support interventions generally supports behavioral approaches but effects are modest and the need for greater specificity to identify “what works best for whom and when” is becoming increasingly possible as the availability of research and practice-based evidence expands. Adherence support strategies that emphasize patient-centered and responsive care systems are included across multiple reviews and guidelines, as are approaches that promote positive experiences with care providers and building medication management skills. There is a paucity of research focused on implementation science and practice-based evidence, which are both needed to bridge science and practice most efficiently. As recommendations for specific strategies and packaged approaches have clearly emerged in the recent literature, monitoring the implementation of these in real-world practice is critical to setting a coordinated agenda for both the research and practice. In order to move systematically toward the identification of what kinds of interventions work best for who and when, attending to both intervention outcomes and drivers of observed effects or lack of effects in controlled research is critically important. Further, evidence emerging from practice should be aggressively added to research agendas to promote better synergies between the practice and research communities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.