
Abstract
Background:
We compared HIV-positive patients receiving care in the border cities of San Diego, United States, with Tijuana, Mexico.
Methods:
Participants were HIV-positive Latinos (n = 233) receiving antiretroviral therapy (ART) from San Diego–Tijuana clinics (2009-2010). Logistic regression identified correlates of receiving HIV care in San Diego versus Tijuana.
Results:
Those with their most recent HIV visit in San Diego (59%) were more likely to be older, have at least a high school education, and were less likely to have been deported than those with last visits in Tijuana. Despite reporting better patient–provider relationships and less HIV-related stigma than those with visits in Tijuana, San Diego patients were twice as likely to make unsupervised changes in their ART regimen.
Conclusions:
We observed poorer relative adherence among HIV-positive Latinos receiving care in San Diego, despite reports of good clinical relationships. Further study is needed to ascertain underlying reasons to avoid ART-related resistance.
Introduction
San Diego, California, is the largest US city situated near the US-Mexico border and is adjacent to Tijuana, Baja California, Mexico, the second-largest Mexican city on the border. 1 San Diego and Tijuana have a combined population of 4 654 996, 2,3 making it one of the largest conurbations in the world. 4 With over 40 million northbound border crossings each year, the region has the busiest international land-border crossing. 5 California is home to the highest concentration of Mexican-origin immigrants in the United States. 6 Immigrants of Mexican origin tend to maintain close family, social, and economic ties to Mexico, especially in the border region, where geographic proximity to Mexico facilitates back and forth travel, including health care utilization on both sides of the border. For individuals living with HIV, binational mobility may contribute to disease transmission due to undiagnosed HIV, lack of access to care, poor adherence, or fragmented care. 7
In the United States, the burden of HIV in Latino communities is disproportionately higher when compared with non-Latino whites. Latinos now represent 16% of the US population, but account for almost 19% of persons who received an AIDS diagnosis in 2010. 8 California ranks among the top 5 states with highest number of reported AIDS cases, 9 and when compared to the United States, San Diego County has a larger proportion (43%) of Latino HIV cases. 10
Numerous factors contribute to disparities in HIV transmission risk and health outcomes among US Latinos. In the United States, Mexican immigrants are more likely than US-born Latinos or other US-born racial and ethnic groups to live in poverty, lack health insurance, and lack a usual health care provider. 11 Prior studies have documented that US Latinos are more likely to delay HIV testing and care, present at later HIV disease stages, and have higher HIV viral loads at entry into care than non-Latino whites. 12 Prior studies have also documented lower antiretroviral therapy adherence among Latinos living with HIV in comparison with non-Latino whites. 13,14 Among Latinos, there is evidence that use of complementary and alternative medicine (CAM) is associated with low adherence. 15 Underlying reasons for these health disparities and care-seeking behavior are complex and may be influenced by factors such as HIV-related stigma and perceived lack of care affordability. 16
In Mexico, it is estimated that there were 225 000 people living with HIV in 2010, 17 and the epidemiologic picture of HIV is changing. Although men who have sex with men have comprised a majority of HIV/AIDS cases in the state of Baja California where Tijuana is located, HIV prevalence among subgroups such as injection drug users and female sex workers is on the rise. 18 In 2010, Baja California registered the second highest cumulative AIDS incidence among Mexico’s 32 states, with 202.8 cases per 100 000, second only to the Federal District with 262.7 cases per 100 000. 17 Information is lacking about the diverse needs, binational health care utilization patterns, and health risk profile of Latinos living with HIV in the US-Mexico border region. 19 Improved understanding of these issues will inform efforts to coordinate care and reduce disparities in health outcomes for Latinos living with HIV in the US-Mexico border region.
We conducted a binational study with HIV-positive Latinos who were recruited simultaneously in San Diego and Tijuana. The current study compared HIV health care utilization practices and patterns among HIV-positive Latinos receiving HIV care in San Diego with those receiving HIV care in Tijuana. We hypothesized that Latino patients who receive HIV health care in San Diego would be more likely to receive ART and to report taking their ART regimens as prescribed by their physician and report less use of CAM than those who receive their HIV health care in Tijuana. The results of this study may lead to improved care delivery in the context of rising HIV prevalence among Latinos in the US-Mexico border region.
Methods
Study Population
Data for the current study were drawn from a cross-sectional study that explored barriers to care and health care treatment practices in Latinos living with HIV in the US-Mexico border region. 20
Between July 2009 and January 2010, a convenience sample of Latinos living with HIV was simultaneously recruited from HIV social and clinical service agencies in San Diego, California, United States and Tijuana, Baja California, Mexico. Eligibility criteria included being HIV positive, being of Mexican origin or other Latin American origin, being at least 18 years old, residing in Tijuana or San Diego for at least 1 month in the prior year, and being able to speak Spanish or English. All potential study participants were read the study consent statement and provided voluntary and informed consent prior to their participation. Details have been published elsewhere. 20 The current analysis included participants who reported their most recent HIV-related medical visit (within the past 6 months) in San Diego or Tijuana. This study was approved by the University of California, San Diego (UCSD) Human Research Protection Program and the Bioethics Committee of the Tijuana General Hospital.
Data Collection
Trained interviewers administered a structured questionnaire based on questions drawn from the Physician–Patient Relationship Quality Measure 21 ; the 2008 HIV Cost and Services Utilization Study 22 ; the Center for Epidemiologic Studies Depression Scale (CESD-10) 23 ; and our prior work with HIV+ Latinos and high-risk populations in the US-Mexico border region. 24,25 Surveys were administered face to face by trained bilingual (Spanish/English) interviewers in private rooms and took approximately 35 to 40 minutes to complete. All participants were reimbursed US$20 for their time.
Measures
Sociodemographics
Participants were asked to self-report on age, sex at birth, sexual orientation (gay, bisexual, or straight/heterosexual), race/ethnicity, highest level of educational attainment, employment status, and annual income. HIV Health Care Practices—participants were asked whether they were taking ARTs, and if so, whether they were able to fill their prescription at their last visit. We asked about their ART adherence in the past month (ie, report of making unsupervised small or major changes to ART from how it was prescribed by their physician). 21 Participants were also asked about the use of CAM in the past 6 months (eg, use of traditional healers, spiritual guides, herbs or plants, etc). 26
We included the following variables of interest: binational access to care and mobility, current medical insurance status (eg, Mexican insurance, US insurance, both US and Mexican insurance, or no insurance coverage), and number of round trip border crossings made in the past 6 months. Because deportation from the United States may be a risk factor for interruptions in health care, 27,28 we asked participants whether they had ever been deported from the United States.
We used the CESD-10 23 to screen for depressive symptoms. HIV-related stigma was measured using selected statements that probed for dimensions of stigma such as disclosure concerns (eg, “I am careful who I tell that I have HIV”) and negative self-image (eg, “since learning I have HIV, I feel set apart and isolated from the rest of the world”). 29,30 Response options were on a scale of always, sometimes, most of the time, or never. We measured patient–clinician communication using a list of statements of overall communication (eg, “how is the doctor who takes care of your HIV at explaining the results of tests in a way that you understand?”). 21 Response options were excellent, very good, good, fair, or poor. We assessed sexual risk by the number of different sexual partners reported in the past 3 months and if they had unprotected anal or vaginal sex in the past 3 months. Participants were also asked about lifetime use of drugs (eg, cocaine, crack, methamphetamines, ecstasy, heroin, ketamine, or other).
Statistical Analysis
Our primary outcome of interest was the location where participants received their most recent HIV health care-related visit in the past 6 months (San Diego vs Tijuana clinics). We compared participants who reported having their most recent HIV health care visit in San Diego with those who reported their most recent HIV health care visit in the Tijuana region across sociodemographic variables and HIV health care practices, as well as binational access to care and mobility, perceived mental health, HIV-related stigma, patient–provider relationship, and sexual and risk behaviors. The main independent variables of interest were HIV-related health care practices: receipt of ART, whether or not the participant made unsupervised changes to their ART regimen, and use of CAM. Earlier studies indicate that these ART-related practices are associated with treatment outcomes, 31 –35 however; the role of CAM in ART adherence is inconclusive. 36
Univariate associations between the outcome and covariates were explored using χ 2 or t tests. Univariate and multivariate logistic regression examined factors associated with having their most recent visit in San Diego versus Tijuana. Factors associated at the univariate level (P < .10) were manually entered into a forward multivariate logistic regression model, beginning with those with the lowest P value and removing factors that did not remain significant. The final model contained only variables significant at P < .05.
Results
Characteristics of the Overall Sample
Data were included for 233 participants who reported having their most recent HIV health care visit in San Diego (N = 137; 59%) or Tijuana (N = 96; 41%) in the past 6 months. Participants were of median age of 40 years; mostly men (79%), and almost (91%) all born in Mexico (Table 1). About one third (32%) were married or reported living in a common-law relationship and half were employed (51%). Binational access to care and mobility were as follows: 21% reported having both US and Mexican health insurance coverage, 72% reported making at least one round-trip border crossing in the past 6 months, and 26% reported having been deported from the United States.
Demographic Characteristics and HIV Health Care Practices of Latinos Living with HIV in the Tijuana-San Diego US-Mexico Border Region by Location of HIV Health Care Receipt

Abbreviations: ART, antiretroviral therapy; ARV, antiretroviral; SD, standard deviation. Values in boldface indicate a statistically significant P value.
a t Statistic.
b Single/separated vs married/with partner.
c Participants who reported always/often when asked how often they experienced specific instances of HIV-related stigma.
d Participants who reported excellent/very good/good vs fair/ poor/very poor when asked about patient–provider relationship.
A majority of participants (88%) reported being prescribed and currently taking ART, and 97% reported having been able to fill their ART prescription at their last clinic visit. Approximately one third (36%) mentioned making unsupervised changes to their ART in the past 4 weeks. The use of CAM was a relatively common practice among both groups; 70% reported using vitamins or supplements, 28% reported using herbs or plants, and 27% reported practicing meditation in the past 6 months. More than half of the participants (64%) perceived their overall health as excellent or very good. HIV-related stigma was pervasive: 29% responded affirmatively to the statement “others seem afraid of me because I have HIV” and 25% reported “feeling set apart, isolated from the rest of the world” since receiving their HIV diagnosis. Most patients (>70%) reported a good physician–patient relationship. About one fifth (21%) reported more than 2 sexual partners in the past 3 months and having anal or vaginal sex without a condom in the past 3 months (22%). The most common illicit drug reported by participants as “ever used” was cocaine (35%) and methamphetamine (33%), and only 10% reported ever injecting drugs.
Comparison between Patients Who Had Their Last HIV Care Visit in San Diego versus Tijuana
Participants who reported their most recent HIV health care visit in San Diego were more likely to be slightly older (42 vs 38 years, P < .01) and have higher level of educational attainment (
Participants who reported their most recent HIV health care visit in San Diego were more likely to report a better patient–provider relationship (eg, “provider explains test results in a way I understand”; 95% vs 68%, P < .01) than those who reported their HIV health care visit in Tijuana. Similar patterns were observed for other indicators of patient–provider relationship. Interestingly, those with most recent visit in San Diego reported making more unsupervised changes to their ART regimen (42% vs 29%, P = .05) and were less likely to report meditation as a CAM practice (21% vs 34%, P = .04). Participants who reported their last HIV health care visit in San Diego were also less likely to report experiencing HIV-related stigma in the past 6 months (eg, “since learning I have HIV, I feel set apart and isolated from the world”; 18% vs 35%, P = .02). Similar patterns were noted for other indicators of HIV-related stigma (Table 1). Participants who received their last HIV health care visit in San Diego were less likely to report lifetime use of drugs, such as cocaine (30% vs 43%, P = .04) or methamphetamine (27% vs 41%, P = .03) than those who reported their last HIV health care visit in Tijuana.
In univariate regression, those who received their last HIV care visit in San Diego were more likely to have an equal or more than high school education (adjusted odds ratio [Adj OR] = 4.20; 95% confidence interval [CI]: 2.31-7.63; P = .00), less likely to report being deported from the United States (Adj OR = 0.32; 95% CI: 0.17-0.60; P = .00), and more likely to report a better patient–provider relationship (ie, provider demonstrate caring, compassion; Adj OR = 4.47; 95% CI: 2.03-9.84; P = .00) and report 2 or more sexual partners in the past 3 months (Adj OR = 3.67; 95% CI: 1.22-10.98; P = .02; Table 2).
Factors Associated at Univariate Level with Receiving HIV Health Care in San Diego
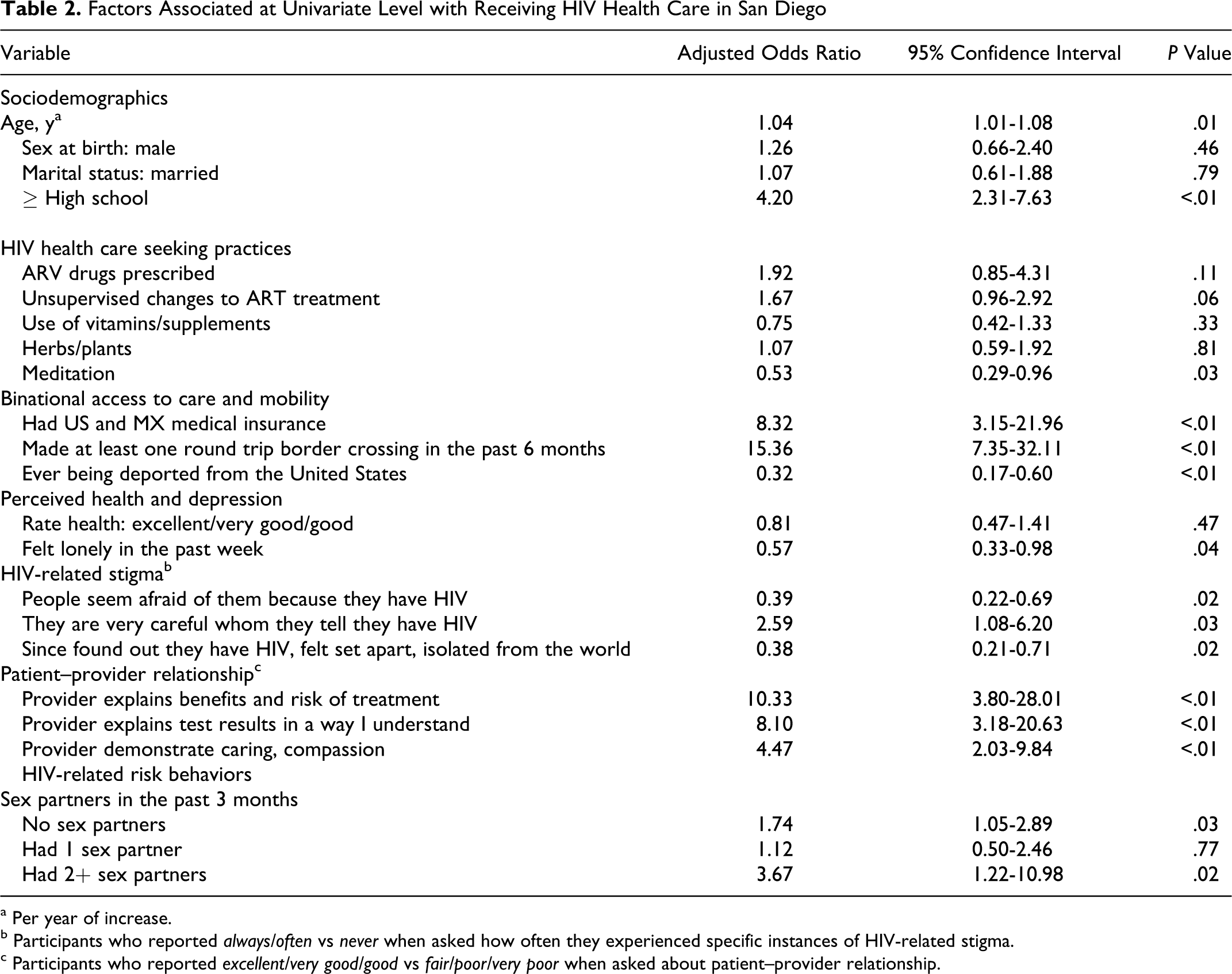
a Per year of increase.
b Participants who reported always/often vs never when asked how often they experienced specific instances of HIV-related stigma.
c Participants who reported excellent/very good/good vs fair/poor/very poor when asked about patient–provider relationship.
Factors Independently Associated with Receiving HIV Care in San Diego versus Tijuana
The following factors were independently positively associated with receiving HIV health care in San Diego (Table 3). Participants with last visit in San Diego were older (Adj OR = 1.05 per year; 95% CI: 1.01-1.08), had higher educational attainment (≥ high school; Adj OR = 4.04; 95% CI: 2.02-8.02), reported making unsupervised changes to their ART regimen (Adj OR = 2.12; 95% CI: 1.08-4.18), and reported better patient–provider relationship (eg, “provider explains results in a way that I understand”; Adj OR = 8.27; 95% CI: 2.86-23.85) compared with those who had their most recent visit in Tijuana. We also found that ever being deported from the United States (Adj OR = 0.32; 95% CI: 0.16-0.67) and reporting HIV-related stigma (ie, “since learning I have HIV, I felt set apart and isolated from the rest of the world”; Adj OR = 0.43; 95% CI: 0.20-0.92) were factors independently negatively associated with last visit in San Diego.
Factors Independently Associated with Receiving HIV Health Care in San Diego Compared with Tijuana

a Per year of increase.
b ≥ High school vs < high school.
c Yes vs no.
d Participants who reported always/often vs never when asked how often they experienced specific instances of HIV-related stigma.
e Participants who reported excellent/very good/good vs fair/ poor/very poor when asked about patient–provider relationship.
Discussion
In this binational study of HIV care, we observed that patients who reported their last HIV care visit in San Diego had a different profile than those who received their last HIV care visit in Tijuana. Participants who reported their most recent HIV care visit in San Diego had higher educational attainment, were less likely to report deportation and HIV-related stigma, and had better patient–physician relationships. On the other hand, they were more likely to report making unsupervised changes to their ART regimen. Implications of these findings are discussed below.
Although San Diego patients were more likely to report generally higher levels of satisfaction with provider care, they were twice as likely to deviate from taking their ART as prescribed by their clinicians compared with those with their last HIV health care visit in Tijuana. Reasons for this may include greater decision-making empowerment about their own health, since patients in the United States may be more likely to be considered as partners in making clinical care decisions. 37 Although we cannot rule out the possibility that some patients may have later discussed making regimen changes with their physician, it is concerning that they appear to have made these changes without consulting their physicians beforehand, since such changes could lead to increased viral load, decreasing CD4 count and possibly HIV resistance. Consistently high levels of adherence are necessary for reliable viral suppression and prevention of HIV resistance, opportunistic infections, disease transmission, progression, and premature death. 38 In an earlier systematic review of ART adherence problems, researchers found that fear of disclosure, forgetfulness, a lack of understanding of treatment benefits, complicated regimens, and being away from medications were consistent barriers to adherence across developed and developing nations. 39 Future interventions to improve and maintain high levels of adherence are clearly needed. Given the demographic boom of US Latinos in the southern border of the United States, 8 improved understanding of adherence barriers specific to Latinos and binational populations is warranted.
Participants who had their most recent HIV health care visit in San Diego were less likely to report having been deported from the United States to Mexico than those with their last visit in Tijuana. This was not unexpected as US deportation to Mexico has been on the rise over the past few years. In 2010, 404 365 individuals were deported from the United States to Mexico, 40 and HIV-positive deportees in Mexico may face substantial barriers to health care due to perceived lack of affordability 41 or the need to provide identification (which frequently they do not have) to access health services. Given that deportees in Tijuana have a 4-fold higher risk of HIV infection, 42 it is important to create effective strategies to address their health care needs.
Participants who received their most recent HIV health care visit in San Diego were less likely to report HIV-related stigma than those who reported their most recent visit in Tijuana. Although HIV-related stigma is problematic for many HIV-positive Latinos in the United States, the general public attitude toward HIV and persons living with HIV may be more tolerant and less stigmatizing in San Diego than in Tijuana. Importantly, in recent years Mexico’s Comisión Nacional de los Derechos Humanos (National Commission on Human Rights) and Mexican public health authorities have employed mass media and other methods to reduce societal stigma.
Our finding that 20% of participants reported medical insurance in the United States and Mexico is fairly unique to binational populations. We will continue to observe growth in binational health care coverage as US and Mexican insurance companies expand services to gain entry into markets on both sides of the border. 43 For some populations, binational health care insurance will improve access to care, but for others who do not qualify for insurance, limited and fragmented access to care in the United States will persist. Health outcomes resulting from populations with access to services on both sides of the border is a research area yet to be explored. Poor coordination of care could lead to drug resistance if patients are changing ART treatments without medical supervision or if persons who are deported are unable to continue with the same therapies they initiated in the United States. Lack of care continuity represents an additional burden on the health care systems of both countries. Prospective studies and binational utilization data are needed to improve coordinated care of populations in this region.
Important study limitations merit our attention. This study’s observational, cross-sectional design did not allow for assessment of changes over time. As well, the surveys were administered in sites where participants received their HIV health care, which may have led to socially desirable responses. Additionally, we cannot determine the extent to which our study population may have been concurrently accessing HIV health care services on both sides of the border. A well-designed prospective study that includes recruitment and binational tracking of HIV-positive individuals from clinical and nonclinical settings would ameliorate the study’s shortcomings.
Our study provides important insights for designing future research to improve understanding of binational care utilization among Latinos living with HIV in the border region. To our knowledge, the current study is the first to simultaneously recruit HIV-positive participants from the United States and Mexico and is one of the few in this region that compares health care experiences and utilization practices of persons living with HIV in different countries on either side of a shared border region. This study further illustrates the need for coordinated care and understanding of patients who frequently cross the border and may seek health care services in the United States and Mexico, a phenomenon that is likely to continue increasing as health care in the United States becomes less affordable to many immigrants.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: supported by the NIH/National Institutes of Mental Health [1R21MH084266-01, 5K01 MH072353].