
Abstract
Health-related quality of life (QOL) has become a high priority of long-term management of HIV-infected individuals. The newly diagnosed HIV cases were assessed to obtain sociodemographic and clinical findings. Eyesenk Personality Questionnaire (EPQ), World Health Organization Quality of Life Brief (WHOQOL-BREF) for HIV-infected patients, and Beck Depression Inventory (BDI) were used to get data regarding personality traits, QOL, and depression scores. A total of 175 patients were included in the study, 128 (73.1%) men and 47 (26.9%) women. Overall 56% of patients screened positive for depression. Presence of depression and high neuroticism score in the personality profile of HIV-infected patients are significantly associated with poorer QOL. High neuroticism score was a strong predictor of poorer QOL in psychological and spiritual domain. Management of HIV-infected patients therefore needs to address these psychological issues.
Introduction
The advent of highly active antiretroviral treatment (HAART) has changed the concept of HIV/AIDS from a deadly disease to a chronic manageable illness. The focus of management therefore has shifted from fighting the virus to ensuring a good quality of life (QOL) for patients living with HIV/AIDS (PLWHA). Quality of life is a multidimensional construct generally defined as a subjective evaluation of one's functioning and well-being. 1 Because individual lifestyle, social norms, cultural practices, and belief systems vary between different population groups, it is imperative to have a deeper understanding of the experiences of HIV-infected Indians while assessing their QOL. Unfortunately, there are only a few studies that have examined QOL among HIV-infected Indians. 2
Poorer QOL in participants with HIV has been linked with increased mortality. 3 Since the major goal of health care is to maximize function in everyday life and to achieve the highest level of QOL within the specific limits imposed by the infection, identification of factors affecting the QOL in people with HIV infection is therefore of utmost importance. Although some studies have found no relationship between health-related QOL (HRQOL) and sociodemographic and clinical variables in individuals with HIV infection, 4 some have found significant association between HRQOL and educational level, socioeconomic status, and gender. 5 –7
Although relatively little is known about what factors are important in determining how individuals assess their QOL, personality traits are thought to exert a powerful influence on people’s reporting of how well they feel. 8 One study has found certain personality traits as well as HAART adherence were associated with poorer HIV-specific QOL. 9 It has also been found that depression is an important factor regarding adherence to HAART and QOL in PLWHA. 10
There are very few studies that examined the influence of psychosocial factors on QOL in Indian PLWHA receiving HAART. In the present study, our aim is to find the predictors of QOL in a group of patients receiving HAART with particular reference to personality traits, presence of depression, and clinical and demographic variables.
Materials and Methods
All the newly diagnosed HIV cases attending ART referral center of a medical college hospital in Kolkata, India, for the first time during 2010 to 2011 and who were eligible for HAART were included in the study. Informed consent was taken, and those who refused consent were naturally excluded. The patients who were too ill or too cognitively impaired to give an interview were also excluded from the study.
The sociodemographic data, HIV-related data, and the risk behavior patterns were collected using a structured proforma. CD4 T lymphocyte count was done in the ART center using FACSCOUNT (Becton Dickson [BD] Biosciences, San Jose, CA) machine using the peripheral venous blood sample before starting HAART. The clinical staging of HIV/AIDS was done by WHO staging criteria.
Each patient was given Eysenck Personality Questionnaire (EPQ) to measure the personality traits of extroversion (E), neuroticism (N), and psychoticism (P). Extroverts are characterized primarily by sociability and impulsiveness but also by jocularity, liveliness, quick wittedness, and optimism. Introverts are opposite of extroverts. People who score high on neuroticism usually overreact to emotional stimuli and take a long time to come back to the normal state. High psychoticism score means people are often impulsive, hostile, egocentric, aggressive, cold, nonconforming, and suspicious. The EPQ was first standardized in Britain 11 to measure 4 of the major dimensions of extroversion–introversion (E), neuroticism–emotionality (N), psychoticism–strongmindedness (P), and dissimulation–social desirability (L). The EPQ used here was a validated Bengali version. 12
A validated Bengali version of World Health Organization Quality of Life Brief (WHOQOLHIV-BREF) was used for the assessment of QOL. This is a 31-item short form of WHOQOL100. 13 In the present study, the Hindi version of the WHOQOL-BREF has been translated to Bengali and retranslated to Hindi by 2 different persons who were conversant in both the languages and a third bilingual person compared the original with the translated version. The translated Bengali version and the Hindi version of the WHOQOL-BREF were then administered one after another at an interval of 1 week to 20 bilingual (ie, people conversant in both the Bengali and Hindi languages) HIV-infected patients admitted to the hospital. It was found that the translated Bengali version and the validated Hindi version had a high correlation.
The WHOQOL-BREF has 6 domain scores representing different dimensions of QOL, viz physical, psychological, level of independence, social relationships, environment, and spirituality. Five of these facets are specific to HIV/AIDs. Individual items are rated on a 5-point Likert scale where 1 indicates low negative perception and 5 indicates high positive perception. A validated Bengali version of the Beck Depression Inventory (BDI) was used to measure depression among the PLWHA. 14
The work obtained ethical clearance from the Institutional Ethical Committee of the study institution.
Statistical Methods
In order to predict the outcome of PLWHA from other measures, we used the tree classification technique. Classification trees are generally used when one attempts to predict values of a categorical dependent variable (class, group membership, etc.) from one or more continuous and/or categorical predictor variables. A classification tree is an empirical rule for predicting the class of an object from the values of predictor variables.
Results
A total of 175 patients were included in the study, 128 (73.1%) men and 47 (26.9%) women. Mean age of male participants (34.7 ± 7.7 years) was significantly higher (t = 3.7, df = 173, P = 3 × 10−4) than female participants (30.23 ± 5.4 years). Majority of the patients were educated up to class IV. Overall 56% of the patients screened positive for depression. Figures 1 to 5 show the results of our attempt to predict various domains of QOL using sociodemographic, clinical, psychological, and treatment variables.
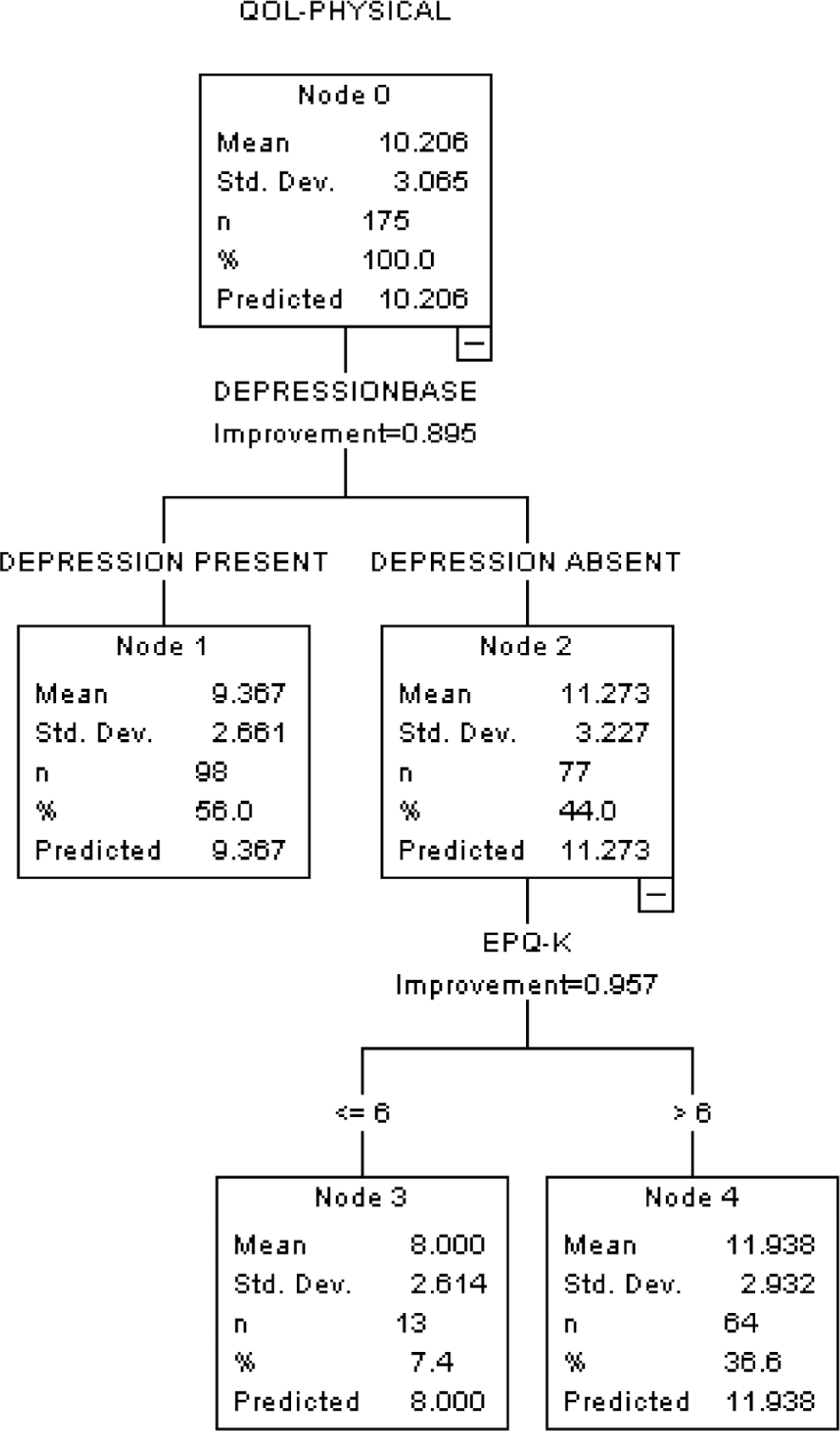
Summary of decision tree method, classification and regression tree (CRT), to predict quality of life (QOL)–physical domain from sociodemographic and clinical variables.

Summary of decision tree method, classification and regression tree (CRT), to predict quality of life (QOL)–psychological domain from sociodemographic and clinical variables.

Summary of decision tree to predict quality of life (QOL)–level of independence domain from sociodemographic and clinical variables.

Summary of decision tree method, classification and regression tree (CRT), to predict quality of life (QOL)–social relationships domain from sociodemographic and clinical variables.

Summary of decision tree to predict quality of life (QOL)–spirituality domain from sociodemographic and clinical variables.
Presence of depression was a strong predictor of poorer QOL in physical and level of independence domains; high neuroticism score was a strong predictor of poorer QOL in psychological and spiritual domain; and longer duration of specialized HIV care predicted better QOL in social relationship domain.
Discussion
Personality traits have always been important in the context of HIV/AIDS. Research has shown that the traits of high sensation seeking and a combination of extroversion and neuroticism are associated with HIV-related risk behavior. The same traits also predict a low adherence to HAART.
The interrelationship of personality traits with physical and psychological QOL is complex. Burgess et al 8 have proposed a model where neuroticism is considered to be a determinant of psychological QOL. A similar article by Penedo et al 9 reported poorer QOL in PLWHA with high neuroticism scores. Personality traits of extraversion and conscientiousness were, on the other hand, associated with better QOL. Neuroticism predisposes one to a prolonged and severe reaction to emotional stressors. The stress inherent to living with HIV/AIDS might cause a long drawn emotional vulnerability and ineffective coping in these individuals, contributing to a poorer psychological QOL. Chronic stress can also lead to elevated glucocorticoid levels, resulting in further suppression of an already compromised immune system.
Although the prevalence of depression in HIV-infected people has not been definitively determined, it is estimated that between 20% and 69% of all individuals with HIV/AIDS experience depression. 15 The study conducted by Adewuya et al 16 found that diagnosis of depression was significantly correlated with poorer QOL in all domains except the “social relationship” domain. In our study, higher depression scores as measured by the BDI is associated with poorer physical QOL as well as lower level of independence. This is not an unexpected finding, given that depression often gives rise to feelings of hopelessness and helplessness, which lead to a sense of having lost one’s independence. It should also be noted that the BDI, though a reliable and valid instrument to measure depression, gives a lot of weightage to somatic symptoms like sleep, appetite, fatigue, and so on, which may be the results of HIV infection per se. This overlap may account for the poorer physical QOL in depressed individuals, or it may be that depression actually adds up to the physical burden of HIV/AIDS. In another recent study, it has also been found that depression is associated with poor adherence to HAART because 95% adherence is needed to suppress viremia successfully and depression inversely affects QOL in HIV/AIDS. 10 Depression not only affects adherence but also results in decreased CD4 count, increased viral load, and increased mortality. 17 In general, depression in HIV-infected patients leads to a decrease in HAART adherence. However, appropriate psychiatric intervention may increase adherence to HAART, improve QOL, and decrease mortality. Therefore, detecting and treating depression in HIV-positive individuals is even more important. 18
Longer duration of specialized HIV care predicted better QOL, particularly in the social relationship domain. Numerous studies have reported better QOL in PLWHA on regular antiretroviral treatment. 19,20 The HAART alone is known to reverse HIV-associated depression, dementia, not to mention improvement in clinical parameters. Hence the longer the duration of HAART, the better the control of the disease and its related complications, leading to better QOL.
Conclusion
Quality of life measurement is important in assessing the overall status of PLWHA. Psychosocial factors are as important as clinical parameters in determining the QOL in HIV-infected patients. Data on follow-up visits is likely to give more information needed for comprehensive care of HIV-infected patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.