
Abstract
Introduction
Three decades into the HIV pandemic, an estimated 34 million people were living with HIV at the end of 2010, while 2.7 million people were newly infected, and 1.8 million AIDS-related deaths during the same period. 1 HIV prevalence varies substantially by country: approximately 10% to 20% of the southern African populations are infected; while some Middle Eastern, Western European, North American, and most Latin American countries have a prevalence below 1%. 1 Antiretroviral therapy (ART) has increased life expectancy for people living with HIV/AIDS (PLWHA) in high- as well as low-income countries,2,3 and the condition is now viewed as a chronic disease. Thus, addressing longer term quality-of-life issues and attitudes toward treatment are integral to the management of HIV-infected patients.
Importantly, a recent combination of drug price reductions, private donations, generic drugs, and the establishment of programs like the Global Fund to Fight AIDS, Tuberculosis and Malaria and the US President’s Emergency Plan for AIDS Relief (PEPFAR) have decreased financial and logistical barriers to ART in resource-limited settings.1,4 Although still inadequate, 47% (6.6 million) of the estimated 14.2 million people eligible for treatment in low- and middle-income countries were accessing ART in 2010, a substantial improvement from the 0.5 million people who were accessing ART in 2004. 1
Effective delivery of HIV care and treatment requires that people know their HIV status and that infected individuals seek care. Because of the clear individual and public heath benefits of HIV testing and treatment, the scientific community has recently pushed universal voluntary HIV testing as a strategy to decrease HIV transmission. 5 However, a major barrier to accessing HIV testing, care, and treatment services is HIV-related stigma. 6 Stigma has been characterized as self, or internalized, stigma, which can limit self-efficacy and empowerment; perceived stigma, the sense of what others think or how they might treat persons thought or known to have HIV; and experienced stigma, actual experience of discrimination, exclusion, or other social sanctions based on perceived HIV status. 7 Experienced stigma, our primary focus here, includes the blaming of HIV-infected individuals for their illness and negative attitudes from the community which result in discrimination.
The established negative consequences of stigma for PLWHA are many: negative self-image, feelings of shame or guilt, and depression 7 ; reluctance to disclose HIV status to others, including sexual partners,8,9 resulting in social isolation and increased likelihood of unsafe sexual activity 10 ; decreased access to and retention in care11–13; and poorer adherence to ART.14–16 Evidence is growing that interventions to reduce HIV-related stigma are associated with improvements in access to and/or outcomes in HIV prevention and care services.17,18
Only limited global survey data are available on PLWHA perspectives on perceived HIV-related stigma and its impacts. Among the numerous objectives of an AIDS Treatment for Life Survey (ATLIS) conducted in 2010 was a global assessment of perceptions of HIV-related stigma among PLWHA.
Methods
Study Design, Sampling, Enrollment, and Settings
ATLIS 2010 was a multicountry cross-sectional survey of PLWHA from 5 regions (Table 1). The project was initiated by the International Association of Physicians in AIDS Care (IAPAC) and governed by an ATLIS Task Force composed of selected HIV/AIDS experts from 5 continents. The ATLIS 2010 survey fieldwork was conducted by Kantar Health, an independent global research organization, from January through March 2010. The ATLIS 2010 protocol, questionnaires, and patient recruitment materials were reviewed and approved by Essex Institutional Review Board, Lebanon, New Jersey, as well as research ethics review boards in each of the countries involved.
Geographic Settings, Interview Method, and Participant Recruitment

Patients were recruited using a proprietary database and through assistance from community-based organizations, HIV/AIDS support groups, and health care facilities. Study eligibility included being aged 18 years or older, diagnosed with HIV or AIDS by a health care provider, and on antiretroviral medication within the past 5 years. Those who were eligible and provided written informed consent were interviewed based on a standardized interview script through 1 of 3 approaches: (1) an online self-administered questionnaire; (2) an interviewer-administered questionnaire carried out by telephone; or (3) a face-to-face interviewer-administered questionnaire. Face-to-face and telephone interviews lasted 20 to 40 minutes and were conducted by an in-country trained interviewer in the participant’s preferred language; face-to-face interviews occurred in a location of the participant’s choice. Monetary incentives ($10) were offered to respondents for completion of interviews where customary and varied by country depending on local ethics practice. The participant recruitment approach, sampling frame, and recruitment setting were specific to each country involved (Table 1).
Survey Questionnaire
The standardized survey questionnaire included specific questions related to mental health, isolation, disclosure, and stigma. The stigma items were adapted from measures utilized previously. 19 In the HIV status disclosure section, participants were asked how concerned they were about people knowing that they have HIV/AIDS (using a Likert scale from 1 to 5, where 5 means very concerned and 1 means not at all concerned), who is currently aware that they are living with HIV or AIDS, and to whom it was most difficult to reveal their HIV status.
Statistical Methods
Data were entered in the study database via a secure Internet site directly following the interviews. Data analyses were performed using STATA Release 10 (Stata Corporation, College Station, Texas). Statistical descriptive analyses included means, median, or proportions, and t test or analysis of variance (ANOVA) was used for continuous variables, while chi-square tests were performed for categorical variables. Multivariate logistic regression generating odds ratios with 95% confidence intervals was performed to identify independent predictors of (1) perceived stigma, (2) HIV status disclosure, and (3) reported depression across all regions. Given the study sample size by country or region, there was at least 80% power to detect a difference of 20% for all outcomes when comparing 2 prevalence rates by country and smaller difference (<10%) when comparing by region, with a type1 2-sided error of 5%. All P values reported are nominal and 2-tailed. A P value less than or equal to .05 is considered statistically significant.
Results
Sociodemographic Characteristics, HIV Testing, and ART Use
A total of 2035 participants completed the survey. Overall, 63% of participants were men and 37% were women. However, in the African region, 67% of participants were women (P < .01, Africa compared to each other region). Overall, 40% of participants were aged 18 to 39 years, 54% were 40 to 59 years, and 6% were ≥60 years. Respondents from Africa were more likely to be younger than those from North America (<40-year-old; 63% versus 16%, P < .01). Asian/Pacific (Korea especially) and African participants had a higher proportion (49% and 71%, respectively) of recent (<5 years) HIV diagnosis versus North America (11%, P < .01). The overall proportion of respondents who had actively sought testing was low (25%). It was highest in North America (40%), followed by Asia-Pacific (29%), Europe (24%), Latin America (22%), and Africa (19%; P < .01, North America compared to each other region). Nearly all (97%) participants were currently taking ART, and 53% had been taking ART for more than 4 years.
Social Isolation, Depression, Stigma, and Discrimination
Overall, 37% of participants reported loneliness and social isolation as a result of their HIV status, with highest levels in North America (42%), Latin America (41%), Europe (35%), and Asia-Pacific (52%) and lowest levels in Africa (24%; P < .01 comparing Africa to each other region). In addition, 27% of participants reported symptoms of depression, with levels highest in North America (47%) and lowest in Africa (13%; P < .01 comparing Africa to each other region). Factors associated with reported depression were living in North America versus other regions (odds ratio [OR]: 2.0; 95% confidence interval [CI] 1.54-2.70), not belonging to a support group (OR: 0.85; 95% CI: 0.76-0.95), being unemployed (OR: 1.28; 95% CI 1.11-1.50), and not disclosing HIV status to anyone (OR: 0.77; 95% CI: 0.58-1.04).
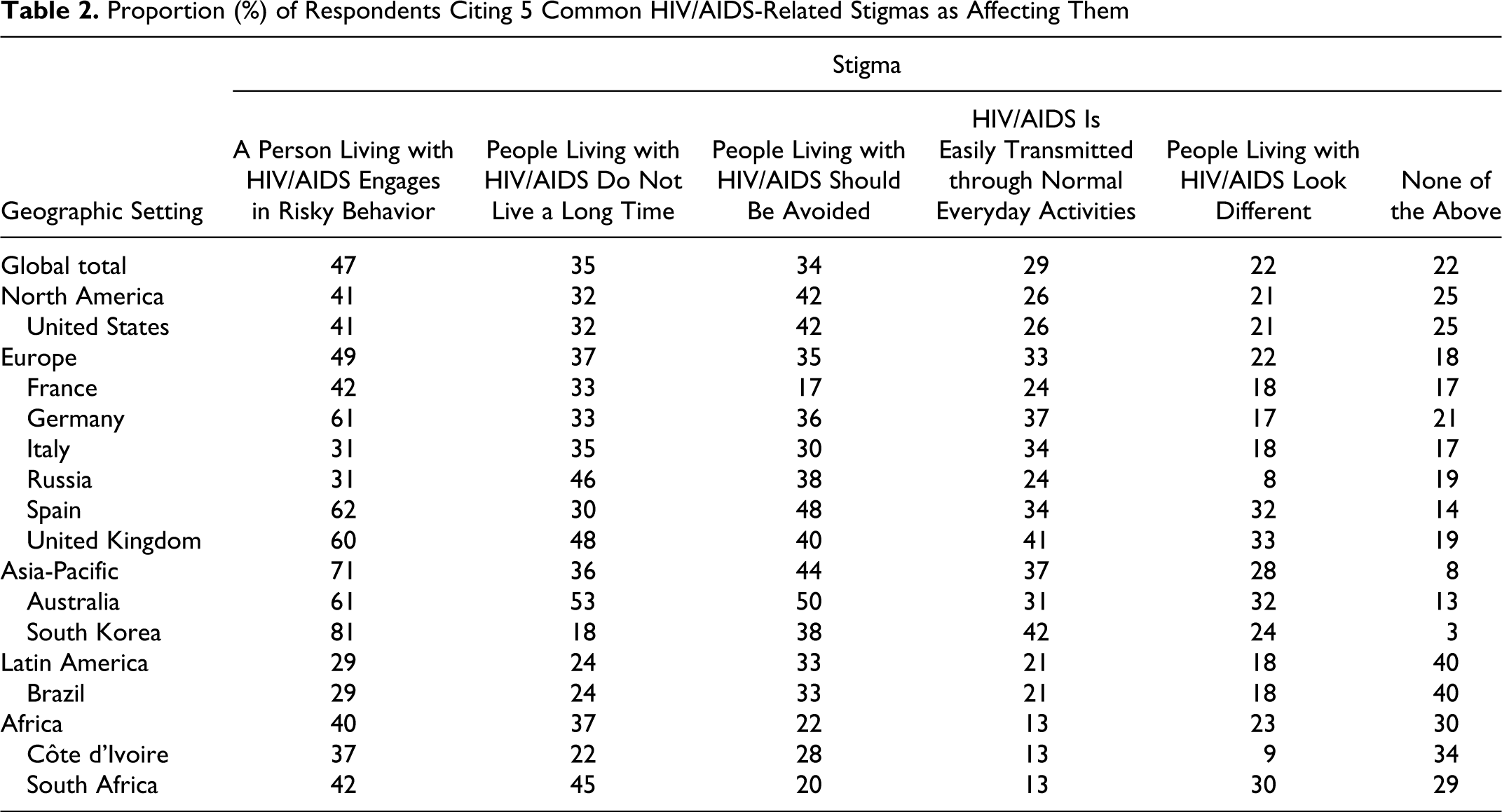
Overall, 78% of respondents reported experiencing some type of stigma associated with their HIV status. Respondents were asked about a series of well-documented HIV-related stigmas; the 5 stigmas most often reported by respondents are shown in Table 2. Levels of specific stigmas varied across countries. The most commonly reported stigma overall (47%) was the perception that other people believe PLWHA engage in risky behavior, such as sexual promiscuity, drug use, and prostitution. This response was significantly more common among respondents from Asia-Pacific (71%) compared to Europe (49%), North America (41%), Africa (41%), and Latin America (29%; P < .01 for each comparison). In addition, 34% of all participants reported that the stigma most affecting them was societal avoidance of PLWHA (44% Asia-Pacific, 42% North America, and 33% Latin America compared to 22% in Africa; P < .01 comparing Asia-Pacific and North America to Africa), while 29% reported being most affected by others' erroneous perceptions of modes of HIV transmission (eg, holding hands or sharing food and drinks with PLWHA; 37% Germany, 41% United Kingdom, 42% Korea compared to 13% in Africa; P < .05 for each comparison). Overall, a substantial proportion of the respondents (37%-68% depending on the stigma) reported that the stigmas surrounding HIV/AIDS have not improved or have worsened in the past 5 years. Respondents from Africa were more likely than those in all other regions (P < .05 for all regions and all stigmas) to report improvements across all 5 of the stigmas in the past 5 years: 62% of participants in Côte d’Ivoire and 56% in South Africa reported improvements with respect to social avoidance of PLWHA. Factors associated with greater perceived stigma were longer duration of HIV infection <5 versus >5 years (OR: 1.42, 95%CI 1.22-1.66); living in Asia-Pacific versus other regions (OR: 1.77 95%CI 1.96-3.92); having experienced body or face changes (OR: 1.11; 95%CI 1.00-1.23); reported depression (OR: 1.23; 95%CI 1.11-1.23); and nondisclosure of HIV status (OR: 1.75; 95%CI 1.28-2.41).
Proportion (%) of Respondents Citing 5 Common HIV/AIDS-Related Stigmas as Affecting Them
HIV Status Disclosure
Overall, 24% of respondents were very concerned about others knowing their HIV status (Table 3). There were substantial differences by region and country; being very concerned was reported by 43% of participants in Asia-Pacific compared to 16% in Africa (P < .01). Length of time since HIV diagnosis was associated with extent of disclosure concerns; concern was most likely in those more recently diagnosed (<5 years, 56% versus >10 years, 47%; P < .01). Reasons for concerns about disclosure are presented in Table 4.
Proportion (%) of Respondents Reporting Being (1) Not At All Concerned, (2) Somewhat Concerned, and (3) Very Concerned about People Knowing His or Her HIV-Positive Status

Proportion (%) of Respondents Reporting Various Reasons for Being Concerned about Disclosure of Their HIV Status, among Respondents Who Reported Any Level of Concern about Disclosure

Overall, 96% of respondents reported having disclosed their HIV status to at least 1 person—most commonly a family member (89%). Disclosure to at least 1 person was higher in North America (100%), Europe (97%), and Africa (98%) compared to Latin America (92%) and Asia-Pacific (85%; P < .01 for each comparison). Overall, 83% of the respondents who reported being in a long-term relationship indicated they had disclosed their HIV status to their spouse/partner. But in Korea, only 71% of responders had told anybody about their HIV status, and only 45% of respondents who were in a relationship reported having shared the information with their sexual partner. Factors associated with disclosure of HIV status to at least 1 person were living in North America versus Africa (OR: 5.71; 95%CI 1.14-28.4), >5 years since diagnosis (OR: 1.70; 95%CI 1.22-2.22), and no perceived HIV-related stigma (OR: 1.67; 95%CI 1.22-2.29). Overall, the main reasons cited for nondisclosure of HIV status were social discrimination (79%) and impact on establishing future relationships (46%; Table 4). Fears that disclosure of HIV status would cause the respondent to lose family or friends were significantly higher in Asia-Pacific (50%) and Latin America (44%) compared to the other regions (P < .05 for each comparison).
Approaches to Address HIV-Related Stigma and Discrimination
In each region, more than 80% of respondents thought that there is still much work to be done to educate society on HIV/AIDS. However, 60% of respondents reported improvements in the past 5 years in society’s perception that PLWHA have a shortened lifespan, and almost one third (31%) reported improvements in the past 5 years in society’s perception that PLWHA engage in risky behaviors. Although some variation by region exists, 66% of respondents believed that the media was the best way to educate the public about nondiscriminative attitudes toward PLWHA (eg, Latin America 78%, Asia-Pacific 77%, and Africa 47%). School education programs were also commonly suggested among ways to decrease HIV-related stigma and discrimination, particularly in North America (46%) and Europe (45%) compared to Africa (35%) and Latin America (36%; P < .01). Programs run by HIV/AIDS organizations were more commonly mentioned in Latin America (36%) and Africa (35%) than in North America (24%), Europe (27%), and Asia-Pacific (25%; P < .05 comparing Latin America and Africa to other regions).
Discussion
This global investigation of perceptions of HIV-related stigma among HIV-infected individuals shows that people in both high and low HIV prevalence settings continue to perceive HIV-related stigma that negatively impacts their quality of life and their disclosure of their HIV status to others. Our findings suggest that about one quarter to one third of PLWHA live with a sense of isolation, depression associated with self-stigma, and/or fear of discrimination due to their HIV status. These findings also contribute to the existing literature by comparing the extent, content, and consequences of HIV-related stigma in different regions of the world.
The negative individual and public health consequences of HIV-related stigma have been clearly established,8–16 and growing evidence suggests that reducing stigma leads to improved outcomes in HIV prevention and care services.10–16 One estimate suggests that a substantial reduction in HIV-related stigma in a region with 15% HIV prevalence among 100 000 women of child-bearing age could result in a 55% reduction in maternal-to-child HIV transmission—from 2991 to 1346—due to improved uptake of and access to effective preventive interventions. 17
Surprisingly, respondents from Africa compared to other regions were more likely to report improvements across all stigmas in the past 5 years, likely reflecting the positive impact of educational and public health initiatives, including ART rollout programs, in these countries that as many people are living with HIV, this disease is being “normailzed” and far less stigmatized. From anthropological theory, the recent increase in access to ART in Africa may have triggered a “virtuous social cycle” by treating these individuals and alleviating their visible signs of disease, enabling them to return to socially and financially productive lives, and sparking interest in testing and treatment 20 and, ultimately, reducing HIV-related stigma. African participants were also the least likely to report loneliness, an encouraging finding.
We found that living in North America was significantly associated with HIV status disclosure, with 100% of respondents in that region reporting having disclosed their status to at least 1 other person. This agrees with other studies that have found higher prevalence of disclosure in developed countries than in the developing world.21,22 There was substantial geographic variation in the proportion of respondents who harbored strong concerns about others knowing their HIV status (highest in Asia-Pacific and lowest in Africa). African respondents were less likely to be concerned about the impact of disclosure on establishing future relationships, on current relationships, and on reputation and the risk of losing/friends or family. It may be that in Africa, because a collective orientation with strong social ties is a way of being, and people are for the most part tied to their families (including extended families), the adverse consequences of disclosure are perceived to be less of a threat than in other regions. 23
Our finding that social discrimination and concerns about future relationships are the most common fears creating barriers to disclosure agrees with other studies.10,16 –19 A review of 17 studies on HIV status disclosure in developing countries found that the main barriers to disclosure for women were fear of infidelity accusations, abandonment, discrimination, and partner violence.21,22 Nondisclosure of HIV status applies to both men and women, but it is more common in women. Indeed, previous studies of women in the United States, sub-Saharan Africa, and Asia suggest that culturally based gender differences in personal sexual freedom and social empowerment explains high rates of nondisclosure among women worldwide.7–10 Nondisclosure of HIV status to intimate partners or household members can have serious consequences. For example, such individuals are likely to experience treatment interruptions due to the fact that tablets must be hidden and not taken in the presence of others, and they also are likely to have worse clinical outcomes due to disease progression. 24 Nondisclosure to sexual partners also could result in continued unprotected sexual activity. 24
Our results demonstrate a continuing and urgent need for interventions to reduce HIV-related stigma and facilitate safe HIV status disclosure, as well as for services to screen for and treat depression among PLWHA. Respondents generally agreed that the media is the best way to reach and teach the public. It is known that educational strategies have limited effectiveness and less lasting impact when used alone since they do not address drivers such as harmful stereotypes, even if they improve knowledge.25,26 Therefore, the multifaceted (for the range of stigmas) and multitiered (to account for individual and structural level of stigma and discriminations) interventions should be explored.25,26 Combination anti-stigma programs should include 1 or more of the following: education (mass media such as TV, radio, print, and social marketing); school education programs; self-help and support groups; civil advocacy groups; government education programs; education in local communities, religious or spiritual center education programs; workplace education programs. 6 In addition, structural approaches such as policies and legal interventions to fight HIV-related stigma should promote and protect human rights through laws and policies. Indeed, decriminalization of HIV, sex work, and same-sex relationships; provision of harm reduction strategies for intravenous drug users (IVDUs); as well as guaranteeing equal rights for all PLWHA, should be the minimal legal standards to help reduce HIV-related stigma and discrimination.27,28
Our study has several possible limitations. First, different interview strategies were used in different regions to meet cultural and other differences and could have introduced information bias when comparing regions. In addition, these data were generated by self-report, and while this is appropriate for measuring concepts such as perceived stigma, it has implications for our measurement of depression, which was not clinically assessed or validated. Finally, our study has possible selection bias given that the convenience sampling in each setting may not necessarily be representative of HIV-infected patients living in that setting. However, despite the above possible limitations, we believe that our data contribute to the existing literature on HIV-related stigma globally.
We conclude that 30 years into the HIV pandemic, despite great strides in the management of HIV disease, perceptions of HIV-related stigma, isolation, and discrimination persist. Addressing HIV-related stigma will benefit individual and public health by improving the quality of life of PLWHA and encouraging testing, disclosure, care seeking, and treatment adherence. More research is needed to quantify the impact of HIV-related stigma reduction interventions on the uptake of specific HIV services and implementation of positive behaviors. Finally, as more interventions are instituted and evaluated, cost-effectiveness data will be needed to inform and guide stakeholders and policy makers in choosing the most appropriate stigma-reduction strategies to pursue in their settings.
Footnotes
Acknowledgments
The authors thank Christiana Noestlinger, PhD, and Connie Kekwaletswe, PhD, for critical reading and advice on the manuscript, as well as Kantar Health for statistical analysis support. This paper was presented as an oral late-breaker presentation at the XVIII International AIDS Conference, July 18-23, 2010, Vienna, Austria. Late-Breaker Track D. Abstract #17566.
The authors wish to thank the following organizations in each country that made data collection possible. Australia: NAPWA; National Association of People Living with HIV/AIDS; PLWHA (Vic) Inc—People Living With HIV/AIDS—(in Victoria); Queensland Positive People; Western Australian AIDS Council; PLWHA (SA)—People Living With HIV/AIDS—(in South Australia); Positive Life (NSW) Inc; Positive Women's Network. Korea: KANOS—Korea HIV/AIDS Network of Solidarity; Love4one. Côte d’Ivoire: Lumiere Action; Club Des Amis (Association Des Personnes Vivant Avec Le Vıh); Aıbef (Association Pour Le Bien Etre Familial); Le Mıssı; Cip Cames; Fsu Com; Chu De Yopougon; Hopital General Yopougon Attie (Port Bouet 2); Fsu Com Abobo Avocatier; Fsu Abobo Baoule; Hopital General D'Anyama; Centre plus de yopougon. Russia: ‘Human Action' ('Gumanitarnoye Deystviye'); Regional Center for Prophylaxis and Treatment of AIDS and Infectious Diseases; Social and Psychological Center “Doveriye”; Center for Prophylaxis and Treatment of HIV of Sverdlovsk Region; Jasen. South Africa: Beatit; Moretele Sunrise Hospice; Bophelong MES Impilo Hospice; Sicelinceba Health Organisation; Tswaragang; Hermanus Rainbow Trust; SAMAREC. U.K.: Positively Women (local branches); Positive Action local branches; Terence Higgins Trust (local branches); AB Plus (local Branches); Body Positive (local branches).
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: ATLIS 2010 was funded by Merck & Co., Inc., Whitehouse Station, NJ, USA, which operates in many countries as Merck Sharp & Dohme. Merck & Co. had no input in the study design, data collection, data analysis or presentation of the results reported in this manuscript.