
Abstract
Introduction
More than 1.7 million people in the United States have been diagnosed with HIV and 1.1 million people are presently estimated to be living with HIV. 1–2 The estimated annual incidence of HIV in the United States in 2006 was 56 000 new cases. 1,3,4 Undiagnosed cases of HIV remains a significant problem with 21% of HIV-infected patients estimated to be unaware of their status. 1,2 In addition, diagnosis is often (32%) made at a late stage. 4 Delay in diagnosis leads to increased probability of transmission and inability to access life-sustaining therapy. Infected patients who are unaware of their HIV status are 3.5 times more likely to transmit the infection compared with those who are aware and they account for 54% of new infections. 5 Also, earlier initiation of highly active antiretroviral treatment (HAART) has shown to decrease mortality in patients with HIV. 6 HIV screening has been shown to be cost effective even in low-prevalence settings. 7 –9
Traditionally, many providers have tested only patients believed to be at high risk or those with clinical indicators. However, assessment for traditional risk factors for HIV transmission has proven to be insufficiently effective in recognizing patients with HIV, particularly in the early stages of the illness. 10 –13 Regardless of the patient selection method used, barriers to testing include insufficient time, pre- and posttest counseling, requirement for informed consent, inadequate reimbursement, competing priorities, and lack of knowledge of current recommendations.
To improve earlier diagnosis and decrease the stigma of HIV testing, the US Centers for Disease Control and Prevention (CDC) revised its recommendations in 2006 to include one-time testing for all patients 13 to 64 years of age in all health care settings unless they declined. 14 Annual testing is recommended for those with any higher risk practices. 14 Consent is recommended to be an opt-out mechanism that is integrated with the general consent for medical care. Prevention counseling is no longer a required prerequisite for testing. Many states have enacted laws to adopt these newer CDC guidelines. However, the degree to which physicians are aware of CDC guidelines or have adopted them is not known.
Internal medicine (IM) and emergency medicine (EM) residents, especially at urban centers, are expected to take care of many patients at higher risk of HIV and thus are pivotal to the effort to increase testing. To our knowledge, there are no published studies that compare the knowledge and attitudes of IM and EM physicians toward HIV testing, particularly among trainees. HIV screening has not been universally implemented like other screening for chronic diseases with similar cost-effectiveness (eg, breast cancer, colon cancer, and hypertension). 15 Therefore, we evaluated the knowledge and attitudes of residents and attendings in EM and IM about their HIV screening practices and barriers to testing.
Methods
We conducted a cross-sectional electronic survey regarding the knowledge and attitude of residents and attendings toward expanded HIV testing. The institutional review board approved the study.
Setting
This study was conducted at a large urban, tertiary, referral academic health center characterized by a college of medicine, allied health programs, hospital, emergency department (ED), and primary and specialty clinic system.
The ED has an annual census of approximately 85 000 patient visits. Approximately two thirds of this population is Medicaid or self-pay; 57% are black, 39% are white, and 0.5% are Hispanic/Latino. The ED has a long-standing HIV counseling and testing program that uses conventional opt in consent. 16 Patient selection for this testing program is predominately targeted, with the test positivity rate of approximately 0.7%. The program tests only a small minority of the overall ED patient population annually (∼4000 tests/year). Although the program takes referrals from EM physicians, most patients are approached and tested independently of physician involvement. All EM physicians are educated about this HIV testing program. In 2008, the program has started using rapid HIV testing when counselors are present. Otherwise conventional nonrapid HIV testing is used.
Sample
We identified 324 resident and attending physicians in IM, combined IM pediatrics and EM at the University of Cincinnati Academic Health Center using lists from the medical staff office and graduate medical education office. Members of the research team were excluded from participation. Potential participants were invited to participate in the anonymous survey by e-mail. Up to 3 invitations were sent to encourage participation from May 25, 2010 to August 15, 2010. Participants completed the survey by navigating to a Web-based survey instrument. Participants were not compensated for participation in the study.
Survey Instrument and Data Collection
The survey included 41 closed-ended questions and was created using REDCap (Research Electronic Data Capture). The survey included information regarding (i) physician demographics (age range, sex, level of training, and field of training), (ii) frequency of assessing HIV transmission risk factors (unprotected sex, sexual orientation, marital status, injection drug use, number of sexual partners in the past year, and previous history of sexually transmitted diseases), (iii) comfort in assessing risk factors, (iv) frequency of offering expanded HIV testing in different settings (ED, hospitalized patients, and primary care settings), (v) factors influencing their decision to offer HIV testing (age of patients, sex, marital status, history of sexually transmitted diseases, and sexual orientation), (vi) knowledge of current CDC recommendation, (vii) how often residents are encouraged by attendings to offer testing, and (viii) reasons for not offering testing and suggested ways to overcome barriers to testing.
Statistical Analysis
Internal medicine pediatric physicians were combined with physicians in IM for the purposes of this analysis (IM group). The primary outcome variable was the percentage of physicians that self-reported screening for HIV. We hypothesized that there was no difference in the percentage of residents and attendings or IM and EM physicians who offered HIV testing. Results were compared using the continuity-corrected chi-square tests at the 5% level of significance for the following categorizations: attendings versus residents and IM versus EM; and males versus females.
To determine whether knowledge and attitudes variables were associated with the frequency of physician self-reported offer of an HIV test, chi-square tests for independence were used for each of the R × C contingency tables as appropriate. As a control for multiplicity, each of these tests was done at the 1% level of significance. As a further exploratory analysis, logistic regression analysis was done to model the relationship between selected demographic, knowledge and attitude variables and whether or not a physician screens for HIV. Statistical analysis was performed using JMP software version 8.0.
Results
Of the 324 physicians surveyed, 232 (71.6%) responded. Six physicians submitted incomplete surveys. There was a trend toward a higher response rate among female physicians (77.9% vs 67.0%; P = .031) but no difference between residents versus attendings (70.1% vs 75.0%, P = .365; Table 1). Internal medicine residents were more likely to respond compared with EM residents (77.7% vs 48.3%; P < .001).
Participant Characteristics

aSix physicians submitted incomplete surveys.
HIV Test Offering
Emergency medicine residents were more likely to offer HIV testing to most or all of their HIV negative or unknown status patients compared with IM residents (60.7% vs 27.8%; P < .001; Table 2). Overall, there was no difference in offering routine HIV testing by sex of physician (male 32% vs female 35.6%), by resident versus attending (33.8% vs 33.3%; Table 3), or between EM and IM attendings (33% each; Table 2). Internal medicine residents were more likely to offer HIV testing for hospitalized patients compared with patients in the ambulatory settings (53.2% vs 29.8%; P < .001).
Comparison between IM and EM Physicians in Assessing for HIV Transmission Risk Factors, Expanded HIV Testing, and Awareness of the Current CDC Recommendations

Abbreviations: IM, internal medicine; EM, emergency medicine; CDC, Centers for Disease Control and Prevention.
Comparison between Residents and Attendings in Assessing for HIV Transmission Risk Factors, Expanded HIV Testing, and Awareness of the Current CDC Recommendations
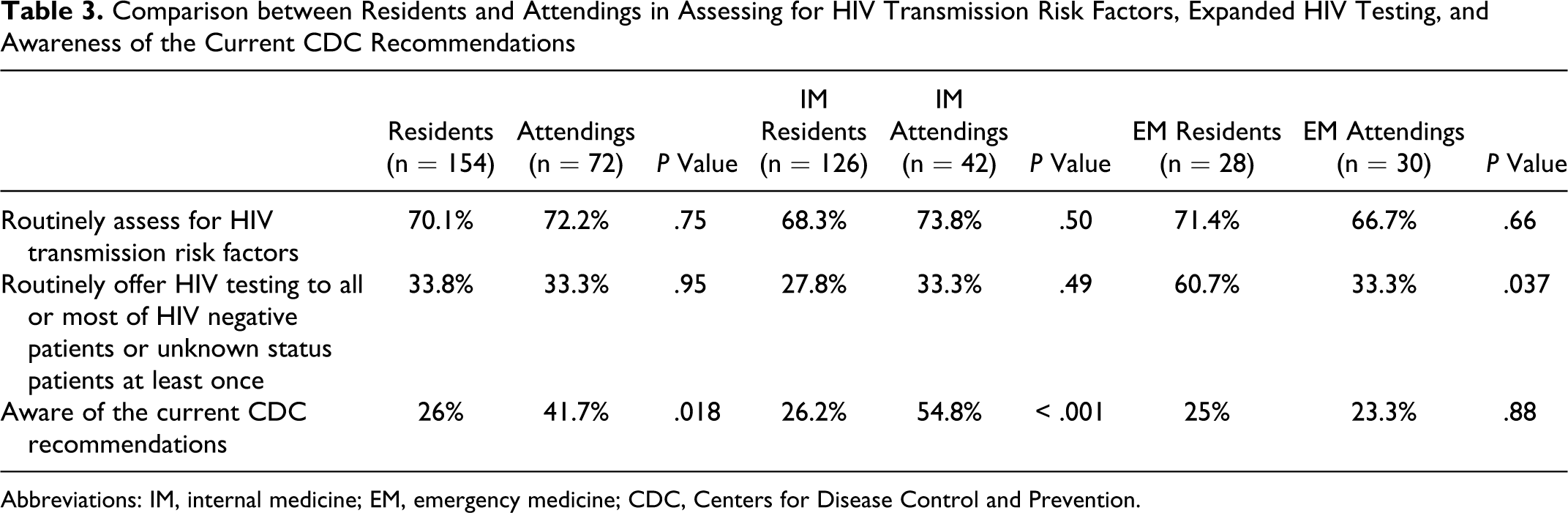
Abbreviations: IM, internal medicine; EM, emergency medicine; CDC, Centers for Disease Control and Prevention.
Most respondents stated that they were more likely to offer HIV testing if the patient was a man who reported having sex with other men (97.7%), had a history of a sexually transmitted disease (94.2%), had a new sexual partner within the last year (67.9%), or was younger than 30 years of age (53.7%). They were less likely to offer HIV testing if the patient was married (52.3%) and testing was not influenced by the patient’s race, ethnicity, or sex (Figure 1).

Factors affecting likelihood of offering HIV testing (n = 226). Abbreviations: STD, sexually transmitted disease; MSM, men who have sex with men.
The most common reasons cited for not offering routine HIV testing (Figure 2) were “not medically indicated” (53.1%), “lack of time” (37.6%), and “not high enough priority on my list” (23.5%). The most common physician identified methods that would enhance testing were (Figure 3), “making it a quality improvement core measurement required for every patient” (61.5%), “changing the process of performing the consent by allowing nurses and other health care staff to obtain it” (47.8%), and “changing the federal/state/hospital laws by making the consent for testing not required” (46.9%).

Reasons for not offering expanded HIV testing (n = 226).

Ways to increase expanded HIV testing (n = 226).
Assessment for HIV Transmission Risk Factors
Internal medicine residents were less likely to assess HIV transmission risk factors compared with EM residents in the ambulatory setting (33.3% vs 71.4%; P < .001; Table 2) but not in hospitalized patients (59.5% vs 71.4%; P = .24). There was no difference in assessing HIV risk factors between IM and EM attendings or between residents versus attendings (Tables 2-3).
When assessing HIV transmission risk factors, physicians were more likely to ask about history of injection drug use (82.9%), marital status (65.4%), being sexually active (64%), previous sexually transmitted disease (53.9%), and use of safe sex precautions (43.9%) as compared with asking men about having sex with other men (28.5%, P < .001 for all comparisons; Figure 4). Physicians were also more comfortable asking about a history of injection drug use (89.9%), unprotected sex (81.1%), and previous sexually transmitted diseases (85.1%) compared with asking about sexual orientation of their patients (69.3%, P < .01 for all comparisons; Figure 5).

Assessing HIV transmission risk factors (n = 226). *P < .0001 compared with sexual orientation. **P = .0006 compared with sexual orientation. #P = .31 compared with sexual orientation. Abbreviation: STD, sexually transmitted disease.

Frequency of feeling comfortable assessing HIV transmission risk factors (n = 226). *P < .0001 compared with sexual orientation. **P = .003 compared with sexual orientation. #P = .115 compared with sexual orientation. Abbreviation: STD, sexually transmitted disease.
Awareness of the Current CDC Recommendation
Only 70 physicians (31%) accurately identified the current CDC recommendations. There was a nonsignificant trend toward a difference in awareness between attendings versus residents (41.7% vs 26%; P = .018; Table 3) and no difference between IM and EM physicians (33.3% vs 24.1%; P = .19; Table 3). Resident awareness of the CDC recommendations was not associated with increased test frequency (residents aware and who routinely offered testing versus residents not aware and routinely offered testing 32.5% vs 34.2%; P = .998).
Resident Encouragement
Only 25 residents (16.2%) stated that they received encouragement from their attendings to offer routine HIV testing, while 21 attendings (29.6%) stated they routinely encouraged residents to offer expanded HIV testing. There was a nonsignificant trend toward a higher level of encouragement by attendings to offer routine HIV testing between EM residents and IM residents (32.1% vs 12.7%; P = .012). Residents who stated they received encouragement from attendings to offer routine HIV testing were more likely to offer it (68% vs 27.1%; P < .001).
Discussion
Our findings suggest that a minority of both IM and EM physicians at our institution offer expanded HIV testing to all patients 13 to 64 years of age as advised by the current CDC recommendations. External medicine physicians were more likely to offer expanded screening compared with IM physicians. Most physicians ordered HIV testing more frequently for high-risk patients and were generally uncomfortable about obtaining complete transmission risk factors. The most frequently cited reason for not offering expanded HIV testing was that it was “Not medically indicated.” This indicates either a lack of awareness of current testing paradigms or a disagreement with those recommendations. Other reasons for not routinely testing included the lack of time and the difficulty of obtaining a separate written consent. Of note, Ohio Statutes do not require a separate written consent to obtain HIV testing, but current hospital policy does. Ohio recently revised its HIV testing Statutes to comply with current CDC recommendations. 17
This is the first study, to our knowledge, that compares HIV testing between residents and attendings. Both groups infrequently offered expanded HIV testing. Also, they both lacked the knowledge of the current CDC recommendations. Residents who frequently offered testing were more likely to receive encouragement from their attendings to do so. Attendings play a major role in residents’ education and their practice behavior may greatly influence the behavior of their residents. 18
Increasing the awareness of the current CDC recommendations may be an important adjunct to increase HIV testing, but awareness alone may not be sufficient. Our study suggests that awareness alone was not associated with increased rates of testing. Physicians tended to support several policy and practice changes that could be used to further increase testing.
Further efforts should be made toward encouraging attending physicians to model and encourage better screening behaviors in trainees because of the importance of their role in the education process. The addition of HIV screening as a quality improvement measure may also encourage more physicians to offer expanded testing.
Few studies have been published regarding expanded HIV testing and physician awareness of current CDC recommendations. Bernstein et al 19 surveyed more than 5000 US physicians in the American Medical Association’s Master file and found that the percentage of self-reported HIV screening was 28.4%, which was lower than what we found (33.7%). Another survey of osteopathic primary care physicians showed that only 22% of participants recommended HIV testing at the initial patient visit. 20 A study of HIV testing-related knowledge among New York City’s IM residents showed similar results to our study; 33% of residents who completed the survey were aware of the 2006 guidelines and 36% utilized a routine testing approach. 21 However, in contrast to what we found, they reported that respondents aware of current guidelines were more likely to practice routine testing (odds ratio [OR] 3.7, 95% confidence interval [CI]: 2.4-5.6). Reilley et al 22 assessed physician and nurse awareness of the CDC recommendations in the Indian health service and reported a much higher rate (58%) compared with other studies. Finally, one study 23 showed that implementation of a focused training program for EM residents improved the attitudes toward ordering HIV testing.
Our results should be considered in the context of several key limitations. The survey was not validated. It is not known whether emergency physicians credited themselves as having offered an HIV test when the test was performed independently by the established ED HIV testing program. Similarly, terms such as routine were not defined by the survey. Only 48% of EM residents responded compared with 78% of IM residents potentially lessening the strengths of our conclusion. One potential bias is that those physicians who are motivated to order HIV testing may have been more likely to respond to the survey. The presence of a long-standing publicly funded HIV counseling and testing program in the ED may have also affected survey responses. Finally, our center provides care to a largely indigent population with a moderate prevalence of HIV and may not be generalizable to other testing.
Conclusion
Residents and attendings fail to offer HIV testing or assess for HIV transmission risk factors at sufficient levels. There is a gap in knowledge of the current CDC recommendations. More emphasis needs to be placed on HIV screening practices in training programs for residents. Physicians’ awareness of current recommendations is unlikely to be sufficient to overcome barriers to testing; additional strategies will be needed if physician-directed universal testing is to be more broadly translated.
Footnotes
Acknowledgment
The Center for Clinical and Translational Science and Training (CCTST) provided REDCap survey as well as statistical support.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
This project was supported by an Institutional Clinical and Translational Science Award, NIH/NCRR Grant Number 5UL1RR026314-02. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH.