
Abstract
Keywords
Introduction
In 2008, an estimated 1.3 million children were born to women living with HIV in sub-Saharan Africa. 1 The HIV prevalence among pregnant Kenyan women was 9% in 2007. 2 Although the use of single-dose nevirapine (NVP) at the onset of labor reduces the risk of mother-to-child transmission (MTCT) of HIV during delivery, 3 it does not prevent HIV transmission from breast-feeding. 4 In breast-feeding populations, maternal combination antiretroviral therapy (ART), as triple antiretroviral (ARV) prophylaxis, can reduce the risk of MTCT of HIV from 35% to <5%. 5 The World Health Organization (WHO) recommends initiating ART in all HIV-infected pregnant women who require treatment of their own health (ie, CD4 count ≤ 350 cells/mm3 or WHO clinical stage 3 or 4 disease). 6 In addition, WHO recommends initiating ART for triple ARV prophylaxis as an option for all HIV-infected pregnant women who do not require ART for their own health (ie, CD4 count >350 cells/mm3 and WHO clinical stage 1 or 2 disease) to prevent HIV transmission. 7
Nevirapine-based ART is the most widely used ART regimen in sub-Saharan Africa, 1 and single-dose NVP is highly effective in preventing MTCT of HIV. 3 Nevirapine use (as a component of ART), however, has been associated with an increased risk of rash-associated hepatotoxicity in nonpregnant women with a baseline CD4 count ≥250 cells/mm3 (11.0% compared with 0.9% among women with baseline CD4 count <250 cells/mm3). 8 In addition, there have been case reports of deaths due to fulminant hepatitis in HIV-infected pregnant women with a baseline CD4 count ≥250 cells/mm3 receiving NVP. 9 These findings led the US Food and Drug Administration (FDA) to issue a black box warning in January 2005 against treating women with CD4 counts ≥250 cells/mm3 with NVP unless the benefits clearly outweigh the risks. 10
In resource-limited settings where NVP-based ART is becoming more widely used to prevent MTCT of HIV, concern has been raised that the benefits may be offset by increased NVP-associated hepatotoxicity, especially among women with CD4 counts ≥250 cells/mm3. Few clinical studies, however, have evaluated NVP-based ART in HIV-infected pregnant women in resource-limited settings. 11 –13 To address this lack of evidence, we compared the rates of hepatotoxicity stratified by CD4 count among pregnant women enrolled in a clinical trial, who initiated either NVP- or nelfinavir (NFV)-based ART.
Materials and Methods
The Kisumu Breastfeeding Study (KiBS) was a phase IIB clinical trial (Clinical Trials registration number NCT00146380) approved by the ethical review committees of Kenya Medical Research Institute (protocol #691) and US Centers for Disease Control and Prevention (CDC; protocol #3677). 5 The primary study objective was to measure the rate of MTCT of HIV among breast-feeding HIV-infected women receiving ART as triple ARV prophylaxis.
Between July 2003 and November 2006, HIV-infected pregnant women were recruited from antenatal clinics. Eligible HIV-infected pregnant women were ≥15 years, ≤34 weeks of gestation, and antiretroviral naive. Exclusion criteria included a baseline serum alanine transferase (ALT) greater than 105 IU (ie, 2.5 × the upper limit of normal [ULN]), and 1 woman was excluded for this indication. Antiretroviral therapy was initiated in women who provided written informed consent at 34 weeks of gestation and discontinued at 6 months postpartum after the infant had been weaned from breast-feeding. Women who met WHO treatment criteria 14,15 at any time during the study were continued on ART. Between July 2003 and January 2005 (first enrollment period), all women initiated NVP, zidovudine (ZDV), and lamivudine (3TC). Nevirapine was initiated at 200 mg once daily (QD; half-dose) for 14 days and then increased to 200 mg twice daily (BID). Between July 2005 and November 2006 (second enrollment period), women with a CD4 count <250 cells/mm3 and a negative hepatitis B virus surface antigen initiated NVP, ZDV, and 3TC (as above). However, women with a CD4 count ≥250 cells/mm3 or a positive hepatitis B surface antigen initiated NFV, ZDV, and 3TC. This protocol change was made in response to the FDA’s advisory 10 on NVP use in women with CD4 count ≥250 cells/mm3.
Participants had their serum ALT and total bilirubin measured and were evaluated with a standardized clinical assessment for any illness or adverse event, including rash, at enrollment; every 2 weeks until delivery; and at 2, 6, 14 weeks, and 6 and 9 months after delivery. The ULN for ALT was 42 U/L and the ULN for total bilirubin was 17 μmol/L. Although the definition of NVP-associated hepatotoxicity has not been standardized in clinical studies, serious hepatotoxicity is usually defined in 1 of 3 ways: (i) an increase in ALT to greater than or equal to 5 times the ULN (severe hepatotoxicity), (ii) rash associated with a 2.5-fold increase in ALT above ULN (rash-associated hepatotoxicity), or (iii) fatal hepatotoxicity. We graded all adverse events, including rash and hepatotoxicity, according to NIH Division of AIDS (DAIDS) guidelines 16 : grade 1/mild (ALT elevation 1.25-2.49 × ULN), grade 2/moderate (2.5-4.99 × ULN), grade 3/severe (5.0-9.99 × ULN), or grade 4/life-threatening (≥10.0 × ULN) toxicity. Nevirapine was discontinued for grades 2, 3, and 4 hepatotoxicity that were confirmed on repeat testing within 72 hours. Nevirapine was also discontinued for grades 3 and 4 rash and for grade 2 rash with urticaria or evidence of concomitant hepatotoxicity.
The primary outcomes in this analysis were (i) severe hepatotoxicity and (ii) rash-associated hepatotoxicity. Severe hepatotoxicity was defined as grade 3 or 4 hepatotoxicity. Rash-associated hepatotoxicity was defined as the onset of a rash (any grade) with any grades 2 to 4 hepatotoxicity, provided these 2 events occurred at the same study visit or within 1 study visit of each other. These outcomes were not mutually exclusive, and a participant could have developed both severe hepatotoxicity and rash-associated hepatotoxicity. A secondary outcome in this analysis was severe rash defined as a grade 3 or 4 rash or a grade 2 rash with urticaria, systemic symptoms, or evidence of progression to grade 3.
Because the study protocol was revised in 2005 in response to the FDA’s advisory on NVP and hepatotoxicity, we conducted 2 related analyses to examine the risk factors associated with severe hepatotoxicity and rash-associated hepatotoxicity. The first analysis was limited to women who initiated NVP between July 2003 and January 2005 (first enrollment period). During this phase of the study, there were no CD4 count restrictions on the use of NVP. This first analysis examined the relationship between CD4 count and hepatotoxicity outcomes among women who initiated NVP. The second analysis was limited to women with a baseline CD4 count ≥250 cells/mm3. These women initiated NVP, if they enrolled in the study between July 2003 and January 2005 (first enrollment period), and NFV, if they enrolled between July 2005 and November 2006 (second enrollment period). This second analysis examined the relationship between ARV regimen and hepatotoxicity outcomes among women with a CD4 count ≥250 cells/mm3.
We performed all analyses using SAS software version 9.1 (SAS Institute Inc, Cary, North Carolina). We used the Wilcoxon rank sum test (continuous variables) and the Fisher exact test (categorical variables) to assess for differences in clinical and demographic variables (eg, CD4 count and gender) among participants with and without each outcome; we considered a finding statistically significant, if the P value was <.05. For the first analysis (women who initiated NVP), we calculated the adjusted relative risk (aRR) and 95% confidence intervals (CIs) with multivariate analysis (SAS proc genmod) to identify variables associated independently with each primary outcome. We included all variables with a P value <.05 in our multivariate model. 17 We also included CD4 count ≥250 cells/mm3 in the multivariate model because evaluating the associations with a CD4 count ≥250 cells/mm3 was our primary study objective.
Results
Antiretroviral therapy for triple ARV prophylaxis was initiated in 522 pregnant HIV-infected women at a median gestational age of 34 weeks. During the first enrollment period (enrollment between July 2003 and January 2005), 254 women enrolled and initiated NVP-based ART (Figure 1). During the second enrollment period (enrollment between July 2005 and November 2006), 268 women enrolled, of whom 212 (79%) initiated NFV-based ART and 56 (21%) initiated NVP-based ART (Figure 1).

Antiretroviral therapy regimens used for triple antiretroviral prophylaxis and enrollment CD4 count results of participating HIV-infected pregnant women in the Kisumu Breastfeeding Study, 2003 to 2009.
Overall, 500 (96%) women delivered during the study and 439 (84%) women completed the entire study intervention (ie, received ART for at least 6 months postpartum). Reasons for early discontinuation (n = 83) included participant withdrawal (56%), infant death/stillbirth (19%), early discontinuation of breast-feeding (7%), noncompliance (5%), maternal death (5%), and other reasons (7%). The median time from ART initiation to delivery was 40 days (interquartile range [IQR]: 28-54).
Participants had a median age of 23 years (full range: 15-42) and a median CD4 count of 398 cells/mm3 (IQR: 256-562). Overall, 403 (77%) participants had a baseline CD4 count ≥250 cells/mm3, and no participants had an abnormal baseline ALT result. In the first enrollment period (analysis #1), participants with a CD4 count <250 cells/mm3 were older, more likely to have WHO clinical stage 2 or 3 disease, and had a higher baseline HIV viral load compared with participants with a CD4 count ≥250 cells/mm3 (Table 1). Among all women with a baseline CD4 count ≥250 cells/mm3 (analysis #2), participants in the first enrollment period were more likely to have WHO clinical stage 2 or 3 disease and a higher baseline HIV viral load compared with participants in the second enrollment period (Table 1).
Baseline Characteristics, HIV Clinical Status, and Medication Use of HIV-Infected Pregnant Women Initiating Antiretroviral Therapy for Triple Antiretroviral Prophylaxis by Study Period and Baseline CD4 Count, Kisumu, Kenya a

Abbreviations: ALT, alanine transferase; BMI, body mass index; IQR, interquartile range; WHO, World Health Organization; NVP, nevirapine; 3TC, lamivudine; ZDV, zidovudine; NFV, nelfinavir.
aData are medians unless otherwise specified (N = 522).
bFirst enrollment period enrolled women from July 2003 to January 2005 and the second enrollment period enrolled women from July 2005 to November 2006.
cP < .01 in the first enrollment period for participants with a CD4 count ≥250 cells/mm3 compared with <250 cells/mm3. No significant difference was seen for weight, BMI, gestational age, or ALT result.
dOne participant was missing baseline weight and BMI measurements, 1 participant was missing a baseline estimation of gestational age, and 2 participants were missing baseline HIV viral load results.
eFour participants were missing baseline WHO clinical stage information; WHO clinical stage 1 was compared with WHO clinical stages 2 and 3 combined (no participants had WHO clinical stage 4 disease).
fP < .05 among participants with a CD4 count ≥250 cells/mm3 in the second enrollment period compared with the first enrollment period.
gP < .01 among participants with a CD4 count ≥250 cells/mm3 in the second enrollment period compared with the first enrollment period. No significant difference was seen for age, weight, BMI, gestational age, or ALT result.
hDuring the study (December 2005), Kenya’s HIV treatment guidelines were revised to recommend cotrimoxazole prophylaxis for all HIV-infected patients unless contraindicated. 14
Severe Hepatotoxicity
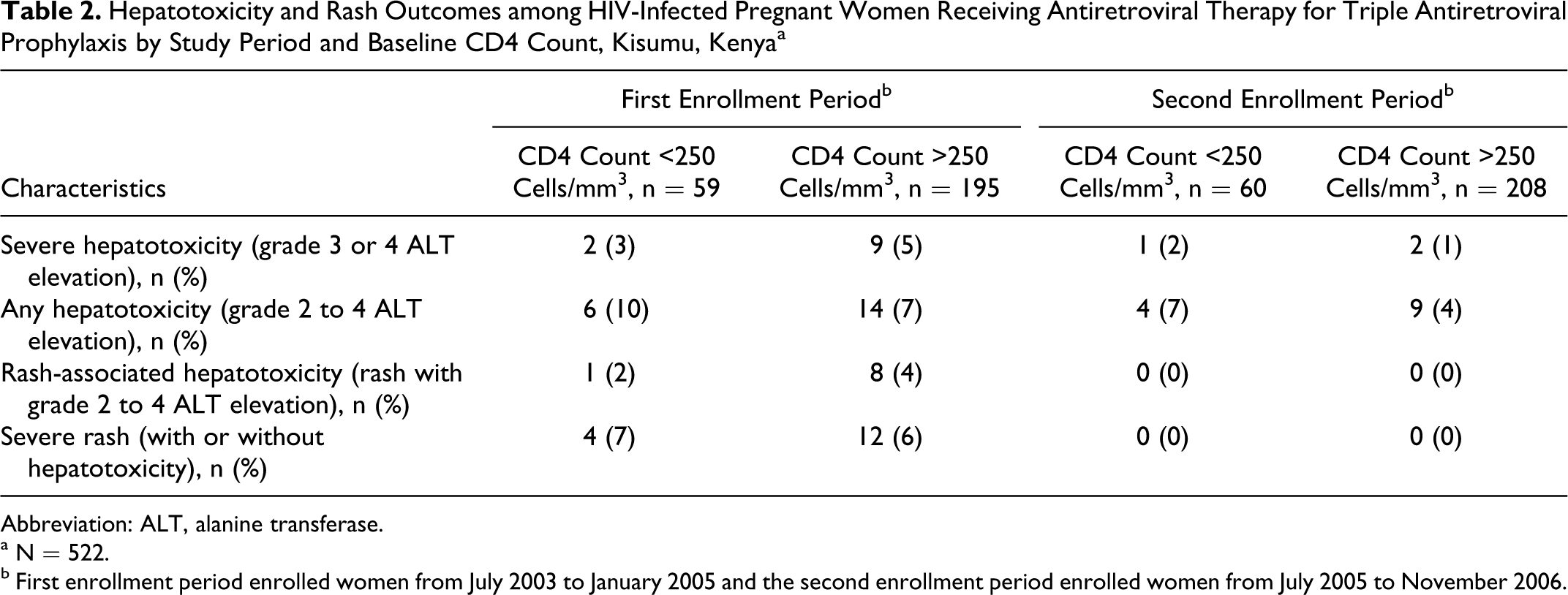
After initiating ART, 14 (3%) women developed severe hepatotoxicity (grade 3 or 4 ALT elevation), including 12 women who initiated NVP (Table 2). Severe hepatotoxicity occurred before delivery (n = 4), at delivery (n = 3), and after delivery (n = 7). The median time from ART initiation to severe hepatotoxicity was 68 days (IQR: 35-127 days). Among women who developed severe hepatotoxicity, the median total bilirubin result was 43 μmol/L (IQR: 23-93) and 4 women had a total bilirubin >210 μmol/L (>5 × ULN). Severe hepatotoxicity was symptomatic in 8 (57%) of 14 cases; the most frequent symptoms were rash (n = 7), jaundice (n = 4), fever (n = 3), abdominal pain (n = 2), and nausea (n = 2). In 6 of 7 severe hepatotoxicity cases with rash, the rash preceded the development of hepatotoxicity by a median of 8 days. Hepatitis B virus surface antigen was tested for in 13 of 14 women with severe hepatotoxicity but was negative in all 13 cases at the time of their toxicity. No deaths were attributed to severe hepatotoxicity. Nevirapine was discontinued in 11 (92%) of 12 severe hepatotoxicity cases and ART was reintroduced with a single drug substitution with NFV. Alanine transferase elevations resolved in 10 (91%) of 11 women who switched to NFV. One woman had persistent ALT elevations, despite switching to NFV. Nevirapine was continued in 1 woman with severe hepatotoxicity because her grade 3 ALT elevation had resolved on repeat testing.
Hepatotoxicity and Rash Outcomes among HIV-Infected Pregnant Women Receiving Antiretroviral Therapy for Triple Antiretroviral Prophylaxis by Study Period and Baseline CD4 Count, Kisumu, Kenya a
Abbreviation: ALT, alanine transferase.
aN = 522.
bFirst enrollment period enrolled women from July 2003 to January 2005 and the second enrollment period enrolled women from July 2005 to November 2006.
Rash-Associated Hepatotoxicity
Rash-associated hepatotoxicity (rash with grades 2-4 ALT elevation) occurred in 9 (2%) women, all of whom were receiving NVP (Table 2). Rash-associated hepatotoxicity occurred before delivery (n = 2), at delivery (n = 3), and after delivery (n = 4). The median time from NVP initiation to rash-associated hepatotoxicity was 47 days (IQR: 36-66 days). In 7 of 9 cases, the rash preceded the development of hepatotoxicity. There were no deaths attributed to rash-associated hepatotoxicity. Nevirapine was discontinued in 8 (89%) of 9 rash-associated hepatotoxicity cases, and ART was reintroduced with a single drug substitution with NFV (1 women also had ZDV switched to stavudine [d4T]). Alanine transferase elevations resolved in 7 (89%) of 8 women who switched to NFV. As mentioned above, 1 woman had resolution of her rash but persistent ALT elevations despite switching to NFV and 1 woman with rash-associated hepatotoxicity continued NVP because her rash and ALT elevation had resolved on repeat clinical evaluation and testing.
Severe Rash
Severe rash (with or without hepatotoxicity) occurred in 16 (3%) women, all of whom were receiving NVP (Table 2). The median time from NVP initiation to severe rash was 33 days (IQR: 23-51 days). The rashes were described (a rash can have multiple descriptions) as maculopapular (n = 9), urticarial (n = 7), having mucosal involvement (n = 5), macular (n = 4), bullous (n = 2), desquamative (n = 2), and papular (n = 1). No deaths were attributed to severe rash. Nevirapine was discontinued in 15 (94%) of 16 severe rash cases, and ART was reintroduced with a single drug substitution with NFV in 14 cases (1 woman had completed the ART intervention at the time of rash onset). Rash resolved in all 14 women who switched to NFV. Nevirapine was continued in 1 woman with severe rash (without hepatotoxicity) because her rash had substantially improved on repeat clinical evaluation.
Risk Factors
In the first analysis (limited to participants who initiated NVP in the first enrollment period), women with a CD4 count ≥250 cells/mm3 had similar rates of severe hepatotoxicity (4.6% vs 3.4%; aRR = 1.6; P = .52) and severe rash (6.1% vs 6.8%; aRR = 0.9; P = .77) compared with women with a CD4 count <250 cells/mm3 (Table 3; data not shown for severe rash). Rates of rash-associated hepatotoxicity were higher among women with a CD4 count ≥250 cells/mm3 (4.1% vs 1.7%; aRR = 2.4; P = .69), but the 95% CIs were wide due to a limited number of outcomes. The median CD4 count was similar among women who developed severe hepatotoxicity (408 cells/mm3) and rash-associated hepatotoxicity (416 cells/mm3) compared with women who did not have these adverse events (390 cells/mm3; P = .63 and P = .17, respectively). In multivariate analysis, severe hepatotoxicity was associated with having developed a rash on ART (aRR = 17.3; P < .0001) and having a body mass index (BMI) ≤20 kg/m2 at enrollment (aRR = 6.5; P = .02; Table 3). Other baseline variables were not associated with the development of severe hepatotoxicity, rash-associated hepatotoxicity, or severe rash; these variables included age, weight, WHO clinical stage, HIV viral load, and the use of cotrimoxazole prophylaxis, antituberculosis treatment, or fluconazole. In the second analysis (unadjusted and limited to women with CD4 count ≥250 cells/mm3 in either the first or second enrollment period), women who initiated NVP had higher rates of severe hepatotoxicity (4.6% vs 1.0%; P = .03), rash-associated hepatotoxicity (4.1% vs 0%; P = .003), and severe rash (6.1% vs 0%; P < .0001) compared with women who initiated NFV.
Associations with Severe Hepatotoxicity and Rash-Associated Hepatotoxicity among HIV-Infected Pregnant Women Initiating Nevirapine-Based Antiretroviral Therapy for Triple Antiretroviral Prophylaxis in the First Enrollment Period, Kisumu, Kenya a

Abbreviations: BMI, body mass index; CI, confidence interval; WHO, World Health Organization; ART, antiretroviral therapy; ALT, alanine transferase.
aN = 254.
bOnly women who enrolled in the first study period (July 2003 to January 2005) are included in this table.
cSevere hepatotoxicity indicates grade 3 or 4 ALT elevation and rash-associated hepatotoxicity indicates rash with grade 2 to 4 ALT elevation.
dTwo participants were missing baseline WHO clinical stage information; WHO clinical stage 1 was compared with WHO clinical stages 2 and 3 combined (no participants had WHO clinical stage 4 disease).
Discussion
Although serious NVP-associated hepatotoxicity and rash occurred among HIV-infected pregnant and postpartum women in this study, the rate of these events was comparable with the rates observed in the studies of nonpregnant HIV-infected women in Zambia and Kenya (3%-5%), 18 HIV-infected patients in high-income settings (3%-9%), 19 and HIV-infected pregnant women in Mozambique with a CD4 count ≥250 cells/mm3 (6%). 11 These toxicities resulted in an interruption of triple ARV prophylaxis but were successfully managed with a single drug substitution with NFV and no toxicity event resulted in fulminant hepatotoxicity or death. Importantly, more than 50% of the severe hepatotoxicity events and more than 25% of rash-associated hepatotoxicity occurred more than 2 months after initiating NVP, in most cases after delivery. In previous studies of HIV-infected nonpregnant 18 and pregnant 9,11 –13,20 –22 women receiving NVP, the onset of these toxicities has usually been reported within the first 6 weeks of NVP initiation.
We did not detect a significant association between severe hepatotoxicity or rash-associated hepatotoxicity and initiation of NVP-based ART at a CD4 count ≥250 cells/mm3 that has been reported among nonpregnant women in the retrospective analysis of Boehringer Ingelheim trials, 8,10,19,23,24 but these results should be interpreted cautiously, given the low frequency of these events in our study. Pregnancy may also complicate the association between CD4 count and NVP-associated hepatotoxicity since pregnancy causes a decline (50-75 cells/mm3) in the CD4 count due to hemodilution 25 and may be a risk factor for hepatotoxicity independent of NVP exposure. 26 We did observe an association between severe hepatotoxicity and development of a rash on NVP and having a low BMI at approximately 34 weeks of pregnancy. In our study, the occurrence of rash often preceded hepatotoxicity, which reinforces the importance of patient education and close clinical follow-up for the early detection of potentially severe hepatotoxicity. A low BMI at enrollment (approximately 34 weeks of pregnancy) likely reflects a low prepregnancy BMI or an inappropriately low weight gain during pregnancy. Low BMI with HIV infection has been associated with a variety of adverse events (including mortality 27 ) and may be secondary to nutritional deficiencies, HIV-associated wasting, or opportunistic infections (eg, tuberculosis). Although animal models have demonstrated a reduction in drug metabolism by the liver with protein calorie malnutrition, 28 it is not clear how a low BMI in the context of HIV infection affects NVP metabolism.
Common NFV-associated toxicities include diarrhea, hyperlipidemia, and fat accumulation; by comparison, rash and hepatotoxicity are rare. 29,30 In this study, rash-associated hepatotoxicity did not occur among pregnant and postpartum women receiving NFV. Although this association was expected, it demonstrates that the background rate of new onset rash or liver toxicity is relatively low in this setting despite high rates of comorbid infections (eg, tuberculosis, schistosomiasis, and hepatitis B virus coinfection), concomitant medications (eg, isoniazid and fluconazole), and environmental exposures (eg, aflatoxins 31 ) that could contribute to these toxicities. Among HIV-infected pregnant women initiating NVP-based ART in these settings, clinicians should suspect that new onset hepatotoxicity is caused by NVP even if the onset seems delayed (including after delivery) or the CD4 count <250 cells/mm3.
World Health Organization recommends initiating ART in all HIV-infected pregnant women who require treatment of their own health (ie, CD4 count ≤350 cells/mm3 or WHO clinical stage 3 or 4 disease) 6 and as an option (triple ARV prophylaxis) to prevent HIV transmission to the infant in women with less advanced disease (ie, CD4 count >350 cells/mm3 and WHO clinical stage 1 or 2 disease). 7 Initiating antiretroviral at these higher CD4 count thresholds is associated with a reduced risk of progression to AIDS or death, 32 an improved chance of immune restoration, 33 and a lower rate of HIV transmission from mother to child. 5 In resource-limited settings, where NVP-based ART is becoming more widely used as triple ARV prophylaxis to prevent MTCT of HIV, there has been concern that these benefits may be offset by increased NVP-associated hepatotoxicity, especially among women with CD4 counts between 250 and 350 cells/mm3. Access to alternative ARVs, such as efavirenz (EFV) or protease inhibitors, may be limited because of their potential first-trimester teratogenicity risks 34 and high cost. Although in our study serious NVP-associated hepatotoxicity occurred, in the context of monitoring for rash and ALT elevations these events were successfully managed with a single drug substitution with NFV. In resource-limited settings, where clinical monitoring for rash and ALT testing can be provided, our data indicate that NVP-based ART can be safely used in HIV-infected pregnant women regardless of their CD4 count.
There were several limitations to our study. Our sample size was small, which limited our ability to detect relatively small absolute increases in the risk of hepatotoxicity. Although we had greater than 80% power to detect previously reported differences in the risk of hepatotoxicity by CD4 count, 8 these calculations assumed a 11% rate of severe hepatotoxicity and rash-associated hepatotoxicity among women with a baseline CD4 count ≥250 cells/mm3. The actual rate of these events among women with a baseline CD4 count ≥250 cells/mm3 was much lower (5% and 4%, respectively), which limits our ability to assess the risk factors. We also do not have complete data on hepatitis B and hepatitis C virus coinfection and on exposure to other hepatotoxins (eg, alcohol and aflatoxin 35,36 ). Among women with severe hepatotoxicity who were tested for hepatitis B virus surface antigen, however, all were negative.
These events, however, were successfully managed with a single drug substitution with NFV and no toxicity event resulted in fulminant hepatotoxicity or death. Our data support the continued use of NVP-based ART in women with a CD4 count ≥250 cells/mm3, especially in settings where clinical monitoring for rash and laboratory monitoring for ALT elevations are available.
In summary, severe hepatotoxicity, rash-associated hepatotoxicity, and severe rash occurred in 4% to 6% of HIV-infected pregnant Kenyan women after initiating therapy with NVP-based ART for triple ARV prophylaxis. Risk of these outcomes was not predicted by a CD4 count ≥250 cells/mm3. Our data support the continued use of NVP-based ART in pregnant women with a CD4 count ≥250 cells/mm3, when safer options are unavailable. Routine, scheduled monitoring for rash and ALT elevations, however, may have improved the clinical outcomes and should be considered for pregnant women (regardless of their CD4 count) receiving NVP-based ART during pregnancy and after delivery.
Footnotes
A preliminary version of these data was presented at the 12th Conference on Retroviruses and Opportunistic Infections (CROI), February 25, 2005, Boston, MA, USA. Abstract Number: 809.The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the US Centers for Disease Control and Prevention (CDC). Study drugs were provided by GlaxoSmithKline and Boehringer Ingelheim.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the study was provided by the Kenya Medical Research Institute (KEMRI) through a cooperative agreement with the US Centers for Disease Control and Prevention (CDC). The study design, data collection instruments, data collection, data analysis, decision to publish, and preparation of the manuscript were led by CDC and KEMRI staff based in Atlanta and at the KEMRI/CDC Field Station in Kisumu, Kenya.