
Abstract
Aims and Objectives:
To correlate asymptomatic oral candidal carriage in HIV-positive patients and normal individuals and determine its association with CD4 count.
Material and Methods:
Forty HIV-positive patients and forty healthy individuals were included in this study. Saliva from both groups was collected by the spitting method. The saliva from each individual was incubated aerobically on Sabouraud Dextrose agar with antibiotics at 37°C. The germ tube method was used for differentiation of candidal species, whether the Candida albicans or non-Candida albicans. Surface count method was used to count the number of colonies of candida species. Data were analyzed by chi square and Mann-Whitney test.
Results:
Oral candidal carriage was found in 22 out of 40 (55%) HIV-positive patients. In healthy volunteers, oral candidal carriage was found in 6 out of 40 (15%) individuals (p value = 0.0002), which is significantly higher. Similarly, density carriage in the HIV-positive patients was found to be significantly higher than that in the HIV-negative group (p value = 0.002). However, oral yeast carriage was not associated with CD4 count (correlation coefficient r = −0.087).
Conclusion:
Within the limits of the study, we concluded oral candidal carriage rate and density carriage higher in HIV-positive patients than in healthy individuals.
Introduction
HIV causes devastation to the body by attacking the host’s immune system. In a healthy individual, there exists a delicate balance between the complex microbial ecology of the mouth and the body’s immune system. On entry into the host’s body, HIV attacks and destroys this delicate balance, thereby rendering the host susceptible to life-threatening opportunistic infections, neurological disorders, and unusual malignancies. Oral lesions are known to be common in HIV/AIDS, 1,2 like in many chronic, debilitating conditions. 3 The most common lesions of the oral mucosa, associated with HIV are candidiasis, hairy leukoplakia, herpetic infections gingivostomatitis, aphthous ulceration, necrotizing gingivitis, pigmented macules, Kaposi sarcoma, and periodontal diseases. 4 Candida species particularly Candida albicans are considered harmless colonizers of the human oral cavity. In HIV-infected (HIV-positive) patients, however, these organisms can become opportunistic pathogens and lead to mucosal infections. The reported prevalence widely ranges from 7% to 93%, depending on the study design and group. 5 Another study 6 conducted at the University of Melbourne, Australia, in 1982 found the prevalence of candidiasis to be greater in females. Sedgley et al 7 reported a carriage rate of 12.5% among healthy children in Hong Kong. Brawne and Cutler 8 showed the carriage rate in healthy, nonhospitalized individuals to vary from 22% to 24%.This fungal infection may occur as the first sign or symptom of HIV disease and at times can be the patient’s chief complaint. Candida may spread by direct extension from the oral cavity to other sites in the host and put the immunocompromised partners at risk of transmission. 9 It is generally thought that in HIV-infected patients immunodeficiency is the main cause of their susceptibility to various opportunistic infections like candidiasis. CD4 count in peripheral blood is important when evaluating the immune status of the host. In this study, we have correlated asymptomatic oral candidal carriage in HIV-positive patients with healthy individuals. The relationship between CD4 count and asymptomatic oral candidal carriage was also evaluated.
Objectives
To correlate asymptomatic oral candidal carriage in HIV-positive patients and healthy individuals.
To correlate the relative density of asymptomatic oral candidal carriage in HIV-positive patients and healthy individuals.
To determine whether candidal colonization was associated with CD4 count.
To determine which Candida species are predominant in HIV-positive patients.
Materials and Methods
Participants
The study group consists of 40 HIV-positive patients and 40 healthy individuals. Inclusion criteria for these individuals were as follows.
No clinical signs of oral candidiasis (OC) or any HIV-related oral lesions.
No ongoing or prior treatment with antifungal or antimicrobial mouth rinses during the previous 6 months.
Individuals with a history of prolonged antibiotic or steroid therapy, iron-deficiency anemia, diabetes, xerostomia, HIV–salivary gland diseases, and any other condition or treatment promoting oral candidal colonization were excluded from the study. Women in the study were neither pregnant nor taking oral contraceptives. The individuals were confirmed for HIV by rapid test. A comparison group consisting of 40 otherwise healthy individuals without risk factors for HIV infection was included in this study. None had oral symptoms and all presented with normal oral mucosa on clinical examination. Inclusion/exclusion criteria for enrollment were same as those followed for the HIV-positive patients. Written informed consent was obtained from all participants, and the research protocol was approved by the local Ethics Committee. Each of the healthy individuals was blood tested for HIV. CD4 count was done by flow cytometry.
Microbiologic Procedures
The participants fasted and had no liquids or any oral cleaning procedure for 1 hour before sampling. Unstimulated whole saliva of 1 mL was collected from each individual.
Method of Saliva Collection
In all patients saliva was collected by the spitting method. 10
Laboratory Diagnosis of Candidiasis
The saliva from each patient was incubated aerobically on Sabouraud dextrose agar with chloramphenicol and incubated at 37°C. Colonies appear as cream colored, pasty, and smooth.
Diagnosis of candidiasis was confirmed by the identification of pseudohyphae using Gram stain in microbiology department of a hospital (Figure 1). Total viable counts were performed on Sabouraud dextrose agar plates and expressed as colony forming units per milliliter (CFU/mL).
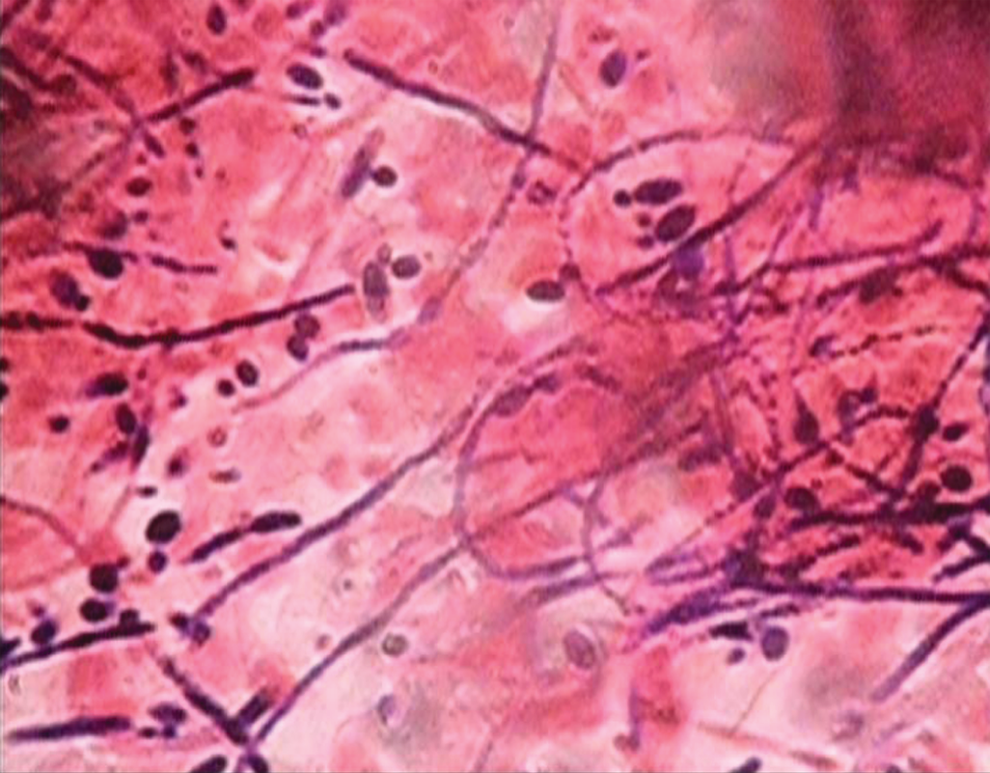
The Candida hyphae along with budding yeast cells under the electron microscope
Germ tube test
The culture of the Candida species was treated with sheep or normal human serum and incubated at 37°C for 2 to 4 hours. A drop of the suspension is examined on a slide under the microscope. The germ tubes are seen as long tube-like projections extending from the yeast cells (Figure 2). The germ tubes are formed within 2 hours of incubation in C albicans. Demonstration of the germ tube is also known as Reynolds–Braude phenomenon. The germ tube method was used for differentiation of Candida species, whether C albicans or non-C albicans. 10
Method Used to Count the CFU
Surface count method was used to count the colonies. In this method, 0.1 mL of the sample measured with standard loop was placed in the center of a well-dried plate of suitable medium and spread with a loop or spreader all over the surface. The plate was then incubated and the colonies were counted.

Positive germ tube test
Results
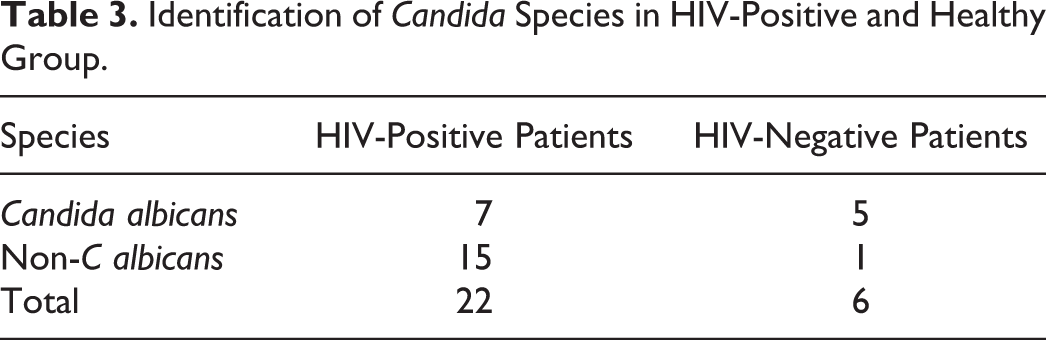
Oral candidal carriage was detected in 22 (55%) of 40 HIV-positive group and in 6 (15%) of 40 HIV-negative group (chi-square test P = .0002), which was significantly higher (Table 1). Similarly, density carriage in the HIV-positive patients (18 990.18 ± 39 100.173 CFU/mL, range: 0-100 000 CFU/mL) was found to be significantly higher than that in the HIV-negative group (54.33 ± 51.052 CFU/mL, range: 0-150 CFU/mL; Mann-Whitney test P = .002; Table 2).However, oral yeast carriage was not associated with CD4 count (correlation coefficient r = −.087). Non-C albicans was the most commonly isolated species in HIV-positive patients (15 [68.1%] of 22 patients), whereas C albicans was the most commonly isolated species in the control group (5 [83.33%] of 6 patients; Table 3). Non-Candida species were not further studied. HIV-positive individuals were stratified by CD4 counts (<200 vs >200 per L) and their carrier rates and density carriage were compared. Oral carrier rates and density carriages did not significantly differ among individuals with CD4 count <200 (10 [58.8%] of 17 individuals) compared with those with CD4 counts >200 (12 [52.17%] of 23 individuals; chi-square test, P = .6799; Mann-Whitney test, P = .94).
Identification of Candida Species in HIV-Positive and Healthy Group.
The Relative Density of Candidal Carriage in HIV-Positive and -Negative Patients.

Comparison of Asymptomatic Oral Candidal Carriage Rates in HIV-Positive and HIV-Negative Patients.

Discussion
Significant difference in oral candidal carriage rate was found in healthy individuals and asymptomatic oral candidal carriages in healthy cohorts published in previous studies are different. For instance, the carriage rates reported by different studies are 53% among adults seen at dental outpatient clinics, 10 whereas it was 29.3% and 18% among healthy adults. 11,12 The median carriage rate within healthy individuals 13 was 34.4%. The carriage rate in healthy individuals in our study was 15% by means of salivary culture. Various methods are often used for sample collection such as epithelial smears, mucosal swabs, salivary cultures, oral rinses, and imprint cultures. Oral rinse sampling was demonstrated to be the most sensitive method for the detection and quantification of yeast carriage. 14 The salivary culture method used in our study could account for the lower carrier rate (Figure 3). A wide range of candidal carriage rates has been reported for HIV-positive patients (11.0%-68%) as well as for healthy individuals (10.0%-68.0%). Among the HIV-positive patients, we discovered a higher overall carriage rate (55%) than that found in healthy individuals (15%, P = .0002). Schoofs et al 15 and Campisi et al 11 reported similar results. In uncontrolled studies including HIV-positive individuals, Hamilton et al, 16 through the use of smears, and Fetter et al, 17 through the use of swabs, reported lower prevalence values (16.0% and 24.0%, respectively).

Culture with candidal colonization
In the present study, the mean density carriage of Candida species was significantly higher in the HIV-positive group (18 990.18 CFU/mL) than in the volunteer comparison group (54.33 CFU/mL; P = .002). The higher density Candidal carriage in the HIV-positive group suggests that HIV seropositivity may lead to changes in the oral environment and in local immunological reactivity thus allowing greater numbers of Candida to colonize the oral cavity. This may explain high incidence of OC in HIV-seropositive patients while still in the early stages of the disease. Campisi et al 11 also reported similar results that the mean density carriage of Candida species is significantly higher in the HIV-positive group (6702.38 CFU/mL) than in the healthy comparison group (155.12 CFU/mL; P = .0002).
Moreover, we did not find any association between oral carriage and CD4 count. These observations are consistent with those of Gottfredsson et al 9 and Campisi et al. 11 In contrast, Fetter et al 17 and Schoofs et al 15 reported a significant relationship between carriage rate and CD4 counts less than 400 × 106 per mm3 and 200 × 106 per mm3, respectively.
Despite OC being significantly associated with immunodeficiency and representing the most common lesion strongly associated with HIV infection, 18 the symptom-free oral candidal carriage and relative density have not been shown to be related to CD4 count, in this study population. This may be due to the lower sample size. Factors such as mucosal immune system and humoral immunity could have an impact on the development of clinical infection by Candida. 19 Other factors such as blood group secretor status, low salivary rates, antimicrobial constituents of saliva, lysozyme and lactoferrin release, presence of normal bacteria flora, and local mucosal immune system could have an impact on the development of oral infection by Candida.
In the present study, non-C albicans was most commonly isolated from HIV-positive patients. Coleman and Sullivan 20 have reported similar findings. However, Margiotta et al 18 in his study found C albicans to be the most commonly isolated species in HIV-positive patients.
Conclusion
In this study, asymptomatic oral candidal carriage and relative density were found to be significantly higher in the oral cavity of HIV-positive patients than that of the healthy individuals. The asymptomatic oral candidal carriage was not associated with CD4 counts. Further investigation, notably longitudinal, is warranted to clarify the role of density carriage as a predictor of the occurrence of OC.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.