
Abstract
This study evaluates the risk factors for the abandonment of antiretroviral therapy (ART) among patients receiving care in an AIDS clinic in Vitória, Brazil. We conducted a case–control study of patients with AIDS attending a reference center for sexually transmitted disease (STD)/AIDS. A total of 62 patients, who abandoned therapy in 2008, and 188 HIV-infected patients answered an interview including demographic, social, and clinical characteristics. Risk factors associated with abandon in univariate analysis were entered into logistic regression models. A total of 250 patients were included in the study. Groups were similar regarding age, gender, and monthly income. In the final multivariate model, illicit drug use (adjusted odds ratio [AOR], 2.3; 95% confidence interval [CI], 1.03-5.07), previous abandon of medication (AOR 38.6; 95% CI 10.49-142.25), last CD4 count <200 cells/mm3 (AOR 1.5; 95% CI 1.03-2.10), and viral load higher than 1000 copies/mL (AOR 2.0 (95% CI 1.34-3.09) were independent predictors of abandonment of ART. In addition to the clinical indicators, behavioral factors remained important throughout the multivariate analysis in our study.
Introduction
Antiretroviral therapy (ART) improves the survival and the quality of life of patients with AIDS 1,2 because it reduces viral load and decreases the destruction of CD4 lymphocytes, which improves the immune system of the patient. 3 Clinical improvement of HIV-infected patients under ART has often been measured by reduction in mortality, opportunistic infection rates, or severe AIDS-related symptoms. 4 Patients on ART also report significant improvements in physical, emotional, and mental health, daily function, and economic well-being. 5 On the other hand, complications emerging in successfully treated HIV-infected patients have changed since the advent of ART. Cardiovascular, renal and bone risks, neurocognitive disorders, lipoatrophy, and non-AIDS-related malignancies must be introduced into the routine of care. 6
The level of adherence to ART has been considered the most important predictor of viral load in patients receiving treatment. Studies suggest that the viral load decreases 7 and the prevalence of undetectable viral load increases 3,8,9 when adherence increases. High adherence rates are usually necessary for attaining therapeutic effectiveness and the phenomenon of nonadherence to treatment has been considered international. 10
Studies on factors associated with ART in developed countries have confirmed that treatment adherence is a complex multicausal phenomenon. 11 Antiretroviral therapy was introduced in the Brazilian health system in November 1996, as part of the country’s policy on free universal access to health care services and medications. A previous study performed in Brazil found that ART was the single greatest predictor of survival. The authors demonstrated that ART treatment, diagnostic criteria, and transmission category remained significant to predict survival and concluded that no factor other than ART could reasonably explain the increase in survival between the 1980s and 1996. 12 In Espírito Santo State, as in the whole country, patients receive ART without any costs after being registered in the surveillance system.
Among factors that compromise the success of the free universal medication distribution program is the patient’s adherence to ART. Knowledge about difficulties of HIV-positive patients regarding the use of therapy can help to understand factors associated with the treatment adherence in Brazilian clinics and to implement policies directed to this group. The aims of this study were to assess the associated factors to abandon ART among HIV-positive patients attended in the reference center for sexually transmitted disease (STD)/AIDS in Vitória, Brazil.
Methods
A case–control study was performed among HIV-positive patients attending a reference center for sexually transmitted infection (STI)/AIDS in Vitória, Brazil, in 2008. Participants were interviewed after providing a written informed consent. Abandonment of ART was defined as not being in use of the prescribed ART regimen for at least 4 months and present virological unsuppression. In this clinic, patients come for routine visit at 4 months for collecting viral load and CD4 counts. It is in this moment that they tell the health professional whether they are correctly taking their medication.
This clinic had 580 patients registered as in use of ART in 2008. We enrolled all patients who presented abandonment of therapy in 2008 as cases, and patients who presented adherence to the ART regimen as controls. Controls were randomly selected in a proportion of 3 controls for 1 case. In this period, we identified 62 patients in the abandon group.
The risk assessment questionnaire included questions on participant’s sociodemographic characteristics (age in years, gender, skin color, education, monthly income, employ situation) and attitudes and behaviors (alcohol and illicit drug abuse, sexual preferences, feeling related to HIV status, side effects, disturbance regarding number of daily pills, previous interruption of ART).
Sample size was calculated based on adherence to ART being 3 times more frequent than patients who abandoned therapy (odds ratio [OR] = 3.14) with a power of 80% and significance of 5%. The number of HIV patients necessary was 60 in case group and 180 in the no-adherence group (controls).
Standard descriptive statistical analysis were performed, including frequency distributions, medians and interquartile ranges (IQRs), or means and standard deviations (SDs) for continuous variables with nonnormal and normal distributions, respectively. Odds ratios and 95% confidence interval [CI] were calculated in bivariate analyses. They were estimated based on a binomial distribution. Multivariate logistic regression analyses to assess variables are associated with abandon outcome. Variables which were significant at P < .15 in the bivariate analyses and known confounders (for instance, age and gender) were considered in the multivariate analysis using a stepwise multiple logistic regression model, with P < .15 as the critical value for variable entry and P < .10 as the criterion for variable elimination. Parsimonious models were finalized based on variables found to be significantly associated with the ART’s abandon at P < .05. The Ethical Committee in Research of the Federal University of Espírito Santo approved this study.
Results
A total of 250 patients were included in the study. Median age was 39.5 (IQR 33-48) years and median of education was 8 (IQR 4-11) years. Cases and controls were similar regarding age, gender, schooling, monthly income, and unemployment (Table 1).
Demographics Characteristics of Patients Attending the Reference Center for HIV/AIDS in Vitória, Brazil by Abandoning ART
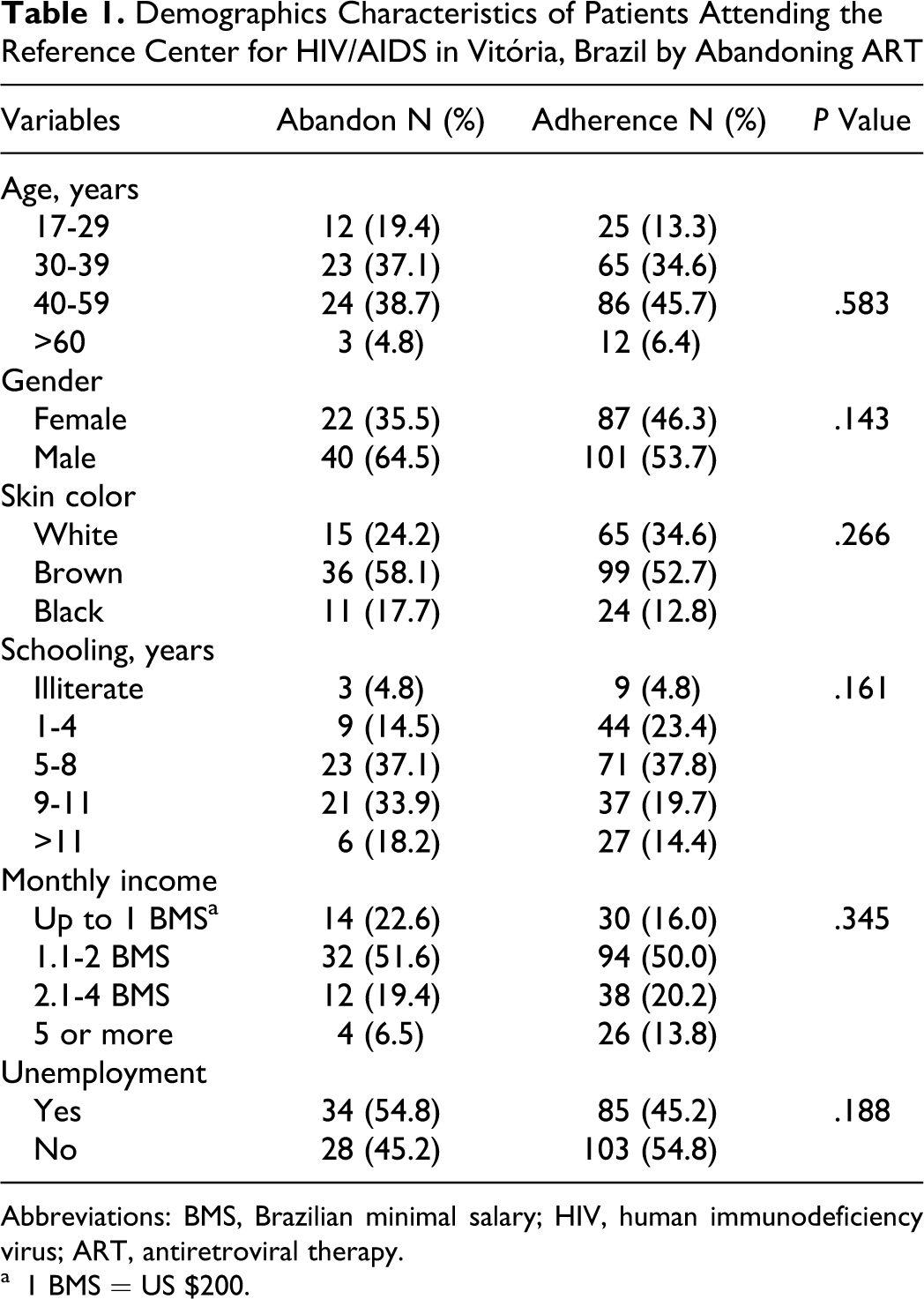
Abbreviations: BMS, Brazilian minimal salary; HIV, human immunodeficiency virus; ART, antiretroviral therapy.
a 1 BMS = US $200.
Table 2 shows behavioral characteristics of patients. Illicit drug abuse was associated with abandon to therapy (33.9% versus 17.0%, P = .007) when compared to adherent group. Social and clinical characteristics of patients by abandon to ART are also described in Table 2. Patients who abandoned therapy reported less frequently that someone at work knew about their seropositivity condition (9.7% versus 16.5%, P = .015) when compared to adherent patients. On the other hand, they reported more side effects (88.7% versus 69.7%, P = .002), taking ART disturbed their daily activities (41.9% versus 21.8%, P = .003) or previous treatment interruption (91.9% versus 30.9%, P = .000) when compared to adherent ones.
Behavioral and Social Characteristics of Patients Attending the Reference Center for HIV/AIDS in Vitória, Brazil, by Abandoning ART

Abbreviations: HIV, human immunodeficiency virus; ART, antiretroviral therapy.
Undetectable viral load (47.1% versus 78.2%, P = .500) and CD4 counts higher than 500 cells/mm3 (16.3% versus 35.6%, P = .001) in the abandon time were more frequent in adherents’ patients.
In the final multivariate model, illicit drug use (adjusted odds ratio [AOR], 2.3; 95% CI 1.03-5.07), previous no-adherence of medication (AOR 38.6; 95% CI 10.49-142.25), last CD4 < 200 cells/mm3 (AOR 1.5; 95% CI 1.03-2.10), and last viral load higher than 1000 copies/mL (AOR 2.0 (95% CI 1.34-3.09) were independent predictors of abandon to ART.
Discussion
In this study, the factors associated with abandon to ART were illicit drug use, previous abandonment of medication, last CD4 < 200 cells/mm3, and last viral load higher than 1000 copies/mL. These results are in agreement with other studies showing that the prevalence of undetectable viral load increases with the level of adherence to the treatment. 3,8,9 The viral load decreases as the adherence level increases. 7
According to Paterson et al, 3 good adherence is related to better disease prognostics, making possible higher CD4 counts and the stability of undetectable viral load. These are the important immunological parameters that can be used to implement a regular clinical evaluation.
In our study, the abandon group reported more frequently previous abandon to therapy than the adherent group. Interruption of ART on its own can be considered a behavioral characteristic determined by a punctual or a permanent context. It can happen because some patients prefer to hide from people at work that they use ART and also because they can have collateral effects of medication disturbing their daily activities. 13,14 Nemes et al15 evaluated ART adherence in 322 AIDS clinics in Brazil and reported higher chance of abandoning ART among patients reporting lost of some doses previously.
Our findings support an association between alcohol and illicit drugs abuse and abandon of ART. Another study reviewing the impact of alcohol on ART adherence, health care utilization, and biological treatment outcomes among people living with HIV/AIDS found an association with alcohol and illicit drugs. 16 These data are also in agreement with prior studies of adherence in HIV-positive individuals that demonstrated the relationship between illicit drug abuse and risk of abandon therapy. 14,17,18 Some drug users have a chaotic life style and it is the determining factor for abandoning ART and not only the use of illicit drugs per se. 19 Some authors have been discussing the importance of a planned health care intervention to implement ART adherence among drug addicters. 20
Limitations of this study include the distribution of and the nature of the sample, which could limit inferences to other data in Brazil. The possibility of response bias, owing to the tendency to provide socially acceptable answers, cannot be excluded. We suggest that such biases would result in underestimation of risky attitudes and behaviors. We also did not performed any specific analysis for different antiretroviral classes because our goal was to measure risk related to abandoning ART, in general.
In Brazil, ART is recommended for symptomatic HIV-positive patients regardless of viral loads and for asymptomatic patients with CD4 counts below 350/mm3 and decisions to start treatment are determined on a case-by-case basis. The total number of patients receiving ART has increased each year since 1997, with a reported 180 000 of the estimated 600 000 HIV-infected Brazilians receiving treatment in 2009. 1 Over this period, there was a decline in mother-to-child transmission of HIV; AIDS-related hospitalizations, mortality, and morbidity declined; and life expectancy of HIV-positive patients more than tripled from an estimated 18 to 58 months. 1 Now the challenge is to help patients have a better compliance to therapy because the dynamic of access involves limitative factors to ART and the question of the universality meets the limits of a widespread country with extremely high levels of social, cultural, and economic inequities. 21
It is important to monitor the indicators of quality of care and adherence carefully 5 and to have care planning that prioritizes patients at risk, especially those who have missed appointments or who have been taking more complex antiretroviral regimens. In relation to the health team, they need to communicate well in order to be understood by all patients.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.