
Abstract
Keywords
Introduction/Background
Occupational exposure to blood-borne infections, including HIV infection, via accidental exposure occur frequently among health care personnel. It has been reported that nearly 1 million health care workers suffer needle stick injuries each year. As a result, hundreds of health care workers are infected with diseases such as Hepatitis B, Hepatitis C, HIV and other blood-borne diseases. 1 The risks for occupational transmission of HIV vary with the type and severity of exposure. In prospective studies of Health Care Providers (HCPs), the average risk of HIV transmission after a percutaneous exposure to HIV-infected blood was estimated to be approximately 0.3% and approximately 0.09% after a mucosal membrane exposure. 2
According to the World Health Organization, every year there are approximately 3 million percutaneous exposures among Health Care Providers (HCPs) worldwide. These exposures are estimated to result in 200 to 5000 HIV infections. 3
The first occupationally acquired HIV infection was reported in 1984 4 and up until December 1997, there had been 95 definite and 191 possible cases of occupationally acquired HIV infection among health care workers. Most of these were from developed countries, where there is a good reporting system. 5
There is however paucity of data in Nigeria on the knowledge and practice of PEP among health care providers, hence this study was carried out to determine the knowledge and practice of post-exposure prophylaxis among various categories of health care providers in a tertiary health facility in Abuja, Nigeria.
Materials and Method
The study was a cross-sectional survey conducted among Health care Providers working in University of Abuja Teaching hospital (UATH), Gwagwalada, Abuja, to assess their knowledge and practice of post-exposure prophylaxis (PEP) against HIV infection. A stratified random sampling method was used to select participants for the study. Health care providers in UATH were first stratified into doctors, nurses, laboratory scientists, and others. Then, there was proportionate allocation of sample to each stratum of the health care providers. Simple random sampling was used to select health care providers from each of the strata for the survey. Data was collected with the aid of a pretested self-administered questionnaire. A total number of 230 health care providers (comprising 92 doctors, 127 nurses, 9 laboratory scientists, and 2 others) of the hospital participated in the survey.
Ethical approval was obtained from the Ethical Committee of University of Abuja Teaching Hospital. Verbal consent was obtained from each of the respondents after the purpose of the study had been explained. Respondents were allowed to decide whether or not to participate in the study. Confidentiality of participants was ensured throughout the study.
Data was analyzed using standard statistical procedures including the use of Epi-Info2008 statistical software.
Results
A total of 230 questionnaires were administered and analyzed. Of the 230 respondents who participated in the study, 131 (57.0%) were females (Table 1 ). The age range of respondents was 20 to 50 years, with 63.5% of respondents between the ages of 30 and 44 years. Majority of respondents (60.4%) were married, while 37.8% were unmarried. Majority of the respondents were nurses (55.2%), while doctors and laboratory scientists were 40% and 9% respectively. This fairly represents the numerical distribution of the 3 professionals in the hospital. Most of the respondents have worked in the hospital for at least 1 year. Those who have worked for 1 to 5 years were 64 (27.8%), 6 to 10 years 39 (17%), more than 10 years 84 (36.5%). Christians were 185 (80.4%) while Muslims were 44 (19.4%).
Sociodemographic Characteristics of Study Population

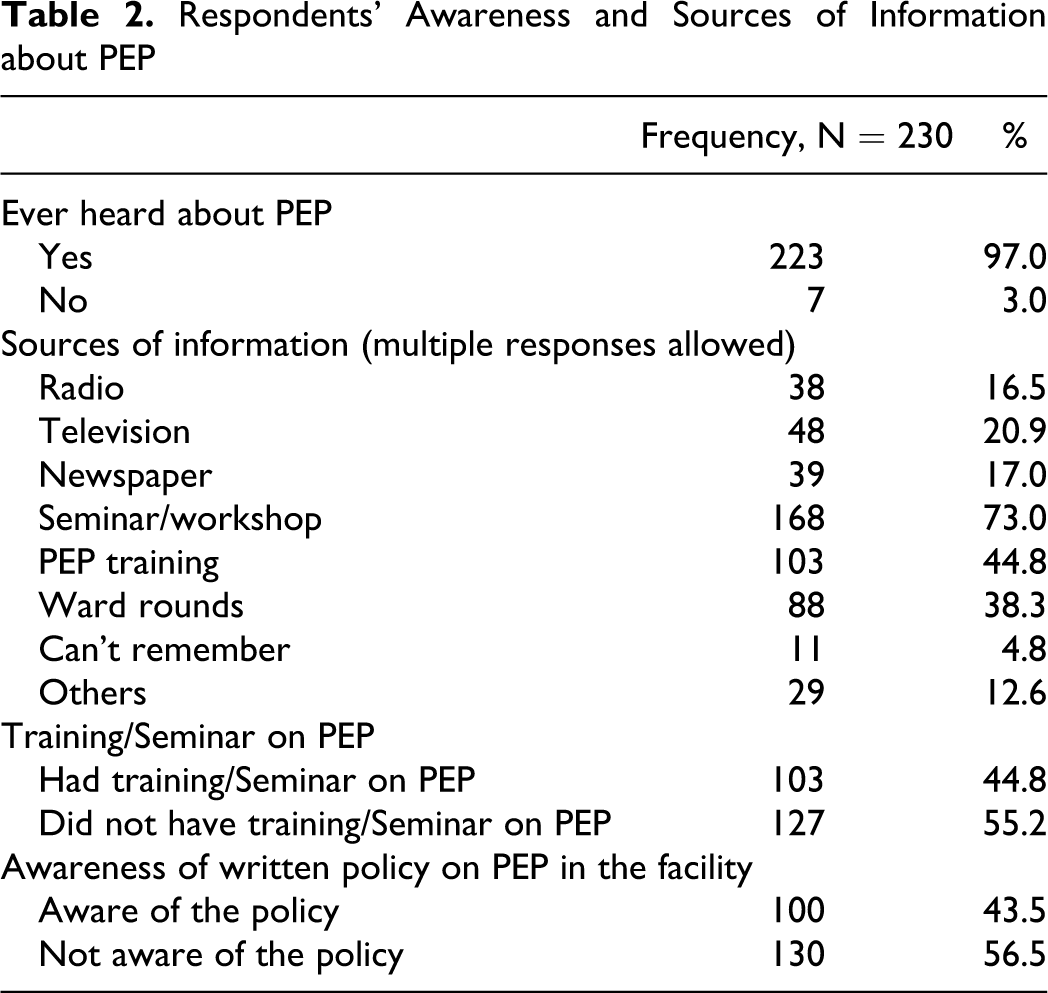
Ninety-one (99%) of doctors, 121 (95.3%) of nurses, and 9 (100%) of lab scientists have heard about PEP (Table 2 ). Majority (97.0%) of the respondents have heard about PEP. Sources of respondents’ information about PEP included; seminars or workshops 168 (73%), PEP training 103 (44.8%), and ward rounds 88 (38.3). The other source of information was the mass media; radio 38 (16.5%), television 48 (20.9), and newspaper 39 (17%). Eleven respondents (4.8%) could not remember their sources of information about PEP.
Respondents’ Awareness and Sources of Information about PEP
Of the respondents, 3 (1.3%) said that PEP is for life, 53 (23%) identified 4 weeks as the duration of PEP, 11 (4.8%) said that PEP duration is for 6 months, while 161 respondents (70%) did not know the duration of PEP (Table 3 ).
Respondents’ Awareness about PEP Drugs, Indications and Duration, and Prevalence of Exposure

In all, 102 (44.3%) respondents identified lamivudine, 132 (57.4%) identified nevirapine, 71 (31%) identified stavudine, and 98 (42.6%) identified zidovudine correctly as drugs that may be used for PEP. Thirty (13%), 11 (4.8%), and 12 (5.2%) respondents said that Levirapine (a nonexisting drug), Ranitidine (an anti-peptic ulcer drug), and Levamisole (an antiparasitic drug), respectively, were drugs used for PEP (Table 3). Only 71 (30.9%) of the respondents could correctly identify the antiretroviral drugs used for PEP.
In all, 198 (86.1%), 180 (78%), 172 (74.8%), and 155 (67.7%) respondents, respectively, knew that needle pricks, blood splashes on mucosal surfaces, rape, and HIV-exposed babies, respectively, are likely indications for PEP (Table 3).
Seventy-one (31%) respondents have had one form of exposure or the other (Table 3).
Of the 71 respondents who reported having been exposed, 46 (64.8%) had needle pricks only, 14 (19.7%) had splashes on their mucosal surfaces only, while 11 (15.5%) had a combination of both exposures (Table 5 ). Forty-five (63.4%) of the respondents have had 1 exposure, 20 (28.2%) and 6 (8.4) have had 2 to 3 exposures and more than 4 exposures, respectively (Table 4 ). The circumstances of exposure in order of frequency are as follow: setting intravenous line 35.2%, surgery 28.2%, drawing blood 25%, giving injections 22.5%, recapping needles 10%, and during delivery 8.5% (Table 4).
Respondents’ Practice of PEP

Types, Frequency, and Circumstances of Exposure

Of the respondents, 71 (30.9%) had occupational exposure to patients’ body fluids within the last 12 months. Of the 71 respondents, 31 (43.7%) who were exposed had post-exposure HIV screening, while the remaining 40 (56.3%) of the exposed respondents did not undergo HIV screening after the exposure. The reasons given by the 40 respondents for not being screened for HIV after exposure included lack of awareness about the need for post-exposure HIV screening 18 (45%), assumption that source was not positive 7 (17.5%), while the remaining 15 (37.5%) gave other reasons for not being screened for HIV after the exposure. Only 4 of the 71 exposed (5.6%) had post-exposure prophylaxis, 3 (75%) of these respondents that had PEP commenced it within 24 hours of exposure to patient’s body fluids, and 1 (25.0%) had PEP after 24 hours of exposure. The 3 respondents that commenced PEP within 24 hours of exposure completed its doses, but the one that commenced PEP after 24 hours of exposure took only the start-up dose of PEP. The respondent that did not complete PEP did not have his or her source of exposure tested for HIV to know whether he or she is HIV positive or not, but the 3 that completed PEP were exposed to HIV-positive sources.
Sixty-seven (94.4%) of the respondents that had exposure to patients’ body fluids did not receive PEP. The reasons given by these 67 respondents for not receiving PEP after exposure varied. Thirty one (46.3%) of the respondents said PEP was not necessary, 24 (35.8%) said the source of exposure was negative, 3 (4.5%) claimed that antiretroviral medications were not available, while the remaining 9 (13.4%) gave several other reasons for not receiving PEP after exposure.
Of the 71 exposed respondents, majority, 46 (64.8%), did HIV screening for the patients through whom they were exposed. Thirty-three (71.7%) of the tested patients were HIV negative, while the remaining 13 (28.3%) were HIV positive. Of the 13 respondents that were exposed to body fluids from HIV-positive patients, only 3 (23.1%) received PEP, while majority, 10 (76.9%), did not receive PEP, in spite of being exposed to body fluids from HIV-positive patients. The reasons given for not receiving PEP by these 10 respondents were not aware of the need to receive PEP after the exposure 7 (70.0%), not aware of the PEP protocol in the hospital at that time 1 (10.0%), and believed that he or she can never be infected with HIV 1 (10.0%). The remaining 1 (10.0%) of the respondents gave no reason for not receiving PEP after the exposure (Table 5).
When the data was analyzed according to professional group, 55 among the 92 doctors (59.8%) did not know the duration of PEP, 98 (77.2%) of nurses and 7 (77%) out 9 of lab scientists did not know the duration of PEP. Only 33 (35.9%) and 17 (13.4%) of doctors and nurses, respectively, knew that 4 weeks is the duration of PEP according to the current national guidelines. One (1.1%), 2 (1.6%), and none (0.0%) of doctors, nurses, and laboratory scientists, respectively, said that PEP is for life (Table 6 ).
Respondents’ Knowledge about Duration of PEP by Professional Grouping

Tests of Statistically Significant Association
When the test of significance was performed on the data in Table 6 as it is, there was no statistically significant association between professional grouping (Job description) and knowledge of PEP duration (P > .05), but when the table was redrawn into a 2 by 3 table (in which those who knew the duration of PEP were grouped under “correct” duration, while those who did not know PEP duration or gave wrong duration of PEP, were grouped under “incorrect duration), there was statistically significant association between professional grouping and knowledge of PEP duration (chi-square [χ2] = 15.32, and P = .0005). The test of significance on the redrawn Table 6 shows that among the various categories of professionals, doctors were significantly most likely to know the correct duration of PEP, followed by Laboratory Scientists, and then, Nurses.
Other significant associations noticed when test of significance was done between respondents’ sociodemographic characteristics and some variables were associations between respondents’ year of working experience and testing of their sources of exposure for HIV (χ2 = 13.22, P = .004), respondents’ year of working experience and knowledge of PEP duration (χ2 = 12.34, P = .006), respondents’ professional grouping and testing of respondents’ sources of exposure (χ2 = 8.16, P = .017), respondents’ professional grouping and exposure to patient’s body fluids (χ2 = 8.74, P = .033), and association between respondents’ professional grouping and frequency of exposure (χ2 = 7.00, P = .030).
Discussion
The study observed that majority of respondents have heard about PEP. The finding is consistent with other studies in Ugandan 6 and London. 7 In contrast, a similar study among pharmacy students in Malaysia demonstrated a low level of awareness of PEP (18.5%). 8 Though majority of respondents have heard about PEP, yet only about one third (30.9%) of them could accurately identify the antiretroviral drugs used for PEP. This finding is comparable to the findings in similar studies where majority of respondents could not name any of the drugs used for PEP.8,9
That the most common sources of respondents’ information about PEP are seminar/workshops and ward rounds imply that post-exposure prophylaxis is a topic least discussed and paid attention to even in societies where a lot of AIDS campaign goes on all the time. PEP is not often seen as a component of comprehensive health care for HIV and AIDS, and even those caring for HIV and AIDS patients are likely to understand it only in the context of preventive measures for occupational hazards.
About one third of our respondents have had at least one accidental exposure. The circumstances of exposures were during recapping of needles, setting intravenous infusion, surgeries, and during administering injectable drugs. This is consistent with studies in Nigeria 10 and India. 11 The findings in this study is lower compared with what was reported in the study among junior doctors in London. 7 In spite of the high exposure rate among the study respondents, only about 6% sought PEP. This finding is supported by findings from similar study conducted in Nigeria that revealed poor attitudes of health care providers toward PEP. 12 The reason why many of them did not seek PEP was that the source patient was HIV negative. Of the 13 respondents who had accidental exposure, and whom the source patients were HIV positive, more than three quarter of them did not receive PEP either because they did not appreciate the risk involved or they did not have an idea of what actions to take at the time of the incident. This finding is corroborated by the similar studies from Kenya and Malawi, which reported a low uptake of PEP among health care workers who had needle stick injuries.6,7,13,14 There is therefore the need for the hospital authorities to train health care workers on the protocol for health care workers with accidental exposure to infectious body fluids detailing the steps the health care workers should take and also making the drugs available. Health care workers need to understand the pathophysiology of HIV infection that when a patient is HIV negative does not totally rule out HIV infection. A careful HIV risk assessment should be done on every patient before a final decision is taken concerning the use of PEP in health care workers who have had accidental exposure to potentially infectious body fluids.
These findings show that the knowledge and practice of PEP among health care providers are very poor. The implication of this is that these health care providers who were exposed to HIV-positive sources and did not take PEP may undergo positive seroconversion, which can increase occupationally acquired HIV infection among this group. If they become HIV positive, this may become a source of demotivation of other health care providers who provide care for HIV-positive clients.
Conclusion
This study shows that the knowledge and practice of PEP by health care providers are poor. There is an urgent need for policy makers in the health sector to put in place programs that will rapidly scale up PEP services in health care settings, so that avoidable occupationally acquired HIV infection can be prevented among the health care providers.
Footnotes
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.