
Abstract
In the 1990s, an interdisciplinary group including pediatricians, anthropologists, health educators, psychologists, and statisticians developed and evaluated an HIV prevention intervention targeting early adolescents living in public housing developments in the USA. The intervention, “Focus on Kids,” (FOK) was effective in reducing risk behaviors, intentions, and perceptions and ultimately was included in the Center for Disease Control's portfolio of effective adolescent programs, “Programs that Work.” Learning about FOK and concerned about the need for a structured program to address high rates of teen pregnancy and risk for HIV, professionals from the Ministries of Health of The Bahamas approached the researchers about collaborating to develop a program for Bahamian youth. A partnership developed which has spanned over a decade and led to the development of an intervention program targeting Bahamian children in grade six, a 10-session adolescent HIV prevention program entitled “Focus on Youth in the Caribbean” (FOYC). Two programs including a video and parent discussion were developed for their parents. Caribbean Informed Parents and Children Together (CImPACT) emphasizes the importance of parent-child communication about sexuality and “Goal for It” (GFI) emphasizes the importance of planning ahead. The US-Bahamian team evaluated these interventions through a randomized, controlled 3-celled longitudinal trial (36 months follow-up) involving 15 elementary schools in The Bahamas. The programs have been shown to be effective. This article describes the context in which the epidemic occurred, events leading up to the collaboration and the issues, decisions, processes, and relationships that we have developed that have allowed it to succeed.
Brief History of The Bahamas
The Bahamas has a complex heritage, defined significantly by the indigenous Lycayan Indians and their subsequent enslavement by Spanish colonialists, the arrival of British settlers in 1648, and its role as a major link in the African slave trade until the abolition of slavery when it served as a safe-haven for escaping US slaves. The ~700 islands and cays (ie, small reefs or sandy islands of low elevation) constituting The Bahamas has been an independent nation since 1968. It remains part of the British Commonwealth. 1, 2
Approximately 85% of the estimated 323 000 Bahamians are of African descent including the estimated 10% Creole population. Although the per capita GNP is $16 140, wealth in the country is highly skewed, with the small population of affluent residents controlling most of the wealth. Unemployment exceeds 9%. 2 Overall, 99% of children attending public high school in New Providence (the most populated island and location of Nassau) are of African descent (Personal communication, MOE). English is universally spoken, although a small proportion of adults are primarily Creole-speaking. School is compulsory through age 16 and literacy rates are high. While the Bahamian economy has thrived on tourism and banking, unemployment is high; 41% of high school seniors have neither job nor further educational prospects. Accompanying the increase in unemployment, the rate of crime has increased substantially over the last 5 decades, with the vast majority of these crimes occurring in New Providence (Johnson M, unpublished data).Drug-trafficking and drug-use have emerged over the last several decades. 3, 4 Crimes have increased dramatically from 3100 in 1964 to 16 400 in 1998. It is estimated that 85% of Bahamians have security bars or security systems. Despite these recent changes, Bahamian society remained very community-based. For example, the elementary schools served as neighborhood meeting sites with many community events occurring during the evenings.
During our ongoing research in The Bahamas, parents have expressed concerns about to how to monitor and supervise their children in such a changing and challenged environment and were apprehensive about allowing outsiders into their homes. Both of these concerns had intervention implications as we discuss later in this chapter.
History of the HIV Epidemic in The Bahamas
In the 1990s, The Bahamas (population 250 000) had the highest annual incidence of AIDS in the English speaking Caribbean, and the second highest rate in the Caribbean overall. Heterosexual activity was the predominant mode of transmission. In the early 1980s, the Bahamian Infectious Diseases and STI experts documented a connection between crack cocaine use, genital ulcers diseases and HIV infection. The occurrence of these 3 epidemics happening almost simultaneously led to the rapid spread of HIV. An estimated 4.13% of adults were infected. The Bahamas still has the second highest annual incidence of AIDS in the Caribbean. An estimated 3% of adults are infected; this figure represents a significant decrease from the rate of 4.13% at the time our collaboration began. However, after several years of declining incidence of HIV and prevalence of HIV/AIDS, the past 3 years have witnessed increases in both of these rates. This increase has been especially prominent among young adults; currently 57% of non-AIDS HIV cases are among adolescents/young adults (15 years to 34 years) who represent <20% of the population. HIV is the leading cause of death among those 15 to 44 years of age for both males (76 per 100 000) and females (53 per 100 000) and is the leading cause of death among males of all ages. 5, 6
HIV/STD Risk Behaviors among Bahamian Adolescents and Young Adults
In addition to the high rates of HIV infection, high rates of teen pregnancy also provide evidence that a high proportion of youth are engaging in unprotected sex. 7 National data describing HIV/STD risk behaviors among high school students, The Bahamas Youth Health Survey 2002 8 was conducted among ninth and eleventh grade students in Bahamian schools; 41% were sexually experienced, including 32% of those aged 13 to 15 years and 57% (70% of males and 41% of females) of those 16 years and older. One tenth of females and one third of males aged 13 to 16+ reported having had >5 lifetime sexual partners. One half (54%) of sexually active adolescents reported having never used any birth control; only one third reported consistent use of birth control. Among those using birth control, condoms were the most frequent method (73%) followed by withdrawal (38%) and rhythm control (23%). Reasons cited for not using protection were “sex was unexpected; no time to prepare” (41%); “didn’t think about it” (40%); and “partner did not wish to use it (24%); 18% of sexually active youth reported that “they didn’t know how to get protection or were too embarrassed.”
Universal access to health care without regard to ability to pay is available throughout the Bahamas. Contraceptives (oral contraceptive, Norplant, and condoms) are provided free of charge or at a minimal cost by the MOH and the Bahamas Planned Parenthood Program. However, parental permission is required for provision of contraceptives to children under age 16. Condoms are not provided in the schools. 9
Response
Several critical events occurred that shaped the Bahamian response. First, as the epidemic began to claim victims, some families were scared and turned infected members away. The Roman Catholic Church, led by Archbishop Lawrence Burke, SJ, responded to the AIDS epidemic by forming the Samaritan Ministry, in 1988. Priests, Sisters, and volunteers from the interfaith community were trained in clinical pastoral education, teaching and counseling, to reach out in ministering not only to those infected with HIV but also to their families and friends. Each Samaritan minister works with one HIV-infected person at a time. Central to the continued success of the Samaritan Ministry is its very confidential and caring approach to People Living with HIV/AIDS (PLWHA) and their families.
The Ministry of Health, with the formation of the AIDS Secretariat, adapted an inclusive approach to the epidemic, encouraging the whole nation to become involved in HIV/AIDS awareness efforts. The nation quickly “went public” with the epidemic. At a time that other nations were ignoring the problem, pretending it did not exist or hiding the problem (and therefore increasing stigma against those involved), The Bahamas began active educational efforts. At this time, the involvement of the church community was limited, and many churches were vocal in their opposition to condom promotion.
As the nation increasingly understood that HIV was everyone’s problem and with the health professionals seeking active partnerships, the schools became involved. At first the involvement was sporadic. In 1988, in recognition of the Second World AIDS Day, the schools became actively involved in an annual national school competition including essays, poetry, posters, and slogans, all part of the awareness program. The competition was highly visible, applauded nation wide and formally involved the school system in New Providence and the major Family Islands in the response to the epidemic. At this time, however, curricular efforts regarding HIV were scant and not well-organized. In response to the disturbing teen pregnancy statistics, some schools had already become more tolerant of the idea of discussing the dangers of unprotected sex (including condoms) in the school system during the 1980s and 1990s. In these early efforts, physicians and the Ministry of Health officials had collaborated with teachers and school counselors and the Ministry of Education laying the groundwork for the collaborations that would prove critically important to the Focus on Youth in the Caribbean (FOYC) partnership. In fact, the individual who would eventually become the coordinator of FOYC had been Supervisor of School Psychological Services within the Ministry of Education; the individual who would become the Associate Coordinator, had worked in teen pregnancy prevention for many years. The 2 individuals had collaborated more than two decades earlier on a successful non-government drug prevention program, Drug Action Service. The Director of the National HIV/AIDS program and the Managing Director of the HIV/AIDS Outreach clinics had worked with Associate Coordinator as she was the Health Educator & Research Assistant at the AIDS Secretariat. Initially, the efforts of the AIDS Secretariat were primarily focused on care, treatment, and support (as opposed to prevention); while all agreed that treatment was essential, later on, the overriding importance of effective prevention programs began to become clear to them.
A critically important decision was made by the AIDS Directorate at that time. Not only would the national AIDS program need to embrace prevention, the prevention efforts needed also to address all age groups, including children. Given the successful overtures that the Ministry of Education had already made in the HIV effort, it became clear to the Managing Director of the HIV/AIDS Centre that a partnership with the school system and Ministry of Education would become part of their overall approach.
As substantial as this progress was, the question of what kind of program addressing what grade or age children remained to be addressed. As The Bahamas worked with international agencies, they began to learn more about the available options.
What Was Known about HIV Prevention
Although controversial for some STDs, the evidence was already strong that condoms do significantly reduce transmission of HIV. 10 A Cochrane review of 23 cohorts of discordant couples found that transmission rates among those who “never” used a condom was 5.75 per 100 person years compared to 1.14 among those who “always” used a condom, yielding a reduction of approximately 80%. 11 At the same time, there was considerable evidence that inappropriate use of condoms is widespread and is associated with slippage and breakage. 10 During the commencement of our collaboration, several reviews were published demonstrating that HIV prevention interventions, including several that focused on adolescents, could reduce adolescent risk behavior. For example, in 1 review of 40 studies assessing adolescent HIV-risk prevention programs, among the 8 articles that assessed condom-use behavior, 5 (63%) reported significant increases in condom-use. 12 A meta-analysis confirmed the overall positive impact. 13 Furthermore, several studies have found positive impact with ethnic minorities including African American adolescents. 14–16 The implication of these findings provided exciting evidence that behavioral interventions can make a difference.
Serendipity
In the mid-1990s there was, as there remains to date, considerable international interest in the development of an HIV vaccine. As several candidate vaccines were nearing readiness for a trial, international agencies approached the leadership of several countries including The Bahamas to consider participating in these trials. The meeting did not proceed as expected and ultimately The Bahamas did not participate as a site for the vaccine trial. However, at the meeting in which the trial was presented, a faculty member at the University of Maryland presented a description of an HIV risk reduction prevention intervention, “Focus on Kids,” targeting young adolescents living in public housing developments in Baltimore. She reported that she had a small grant which could be used to adapt and pilot test the program for The Bahamas if there was interest. Several members of the audience from the AIDS Secretariat were very interested and sought to learn more about the program.
Risk Prevention in the United States: Focus on Kids (Later Known as Focus on Youth)
Our interdisciplinary research team has been developing and assessing adolescent risk prevention programs across the US and globally for nearly two decades. In the early- to mid-1990s, we developed Focus on Kids, an 8-session face-to-face intervention targeting youth aged 9 to 15 years. Focus on Kids is based on Protection Motivation Theory, a social cognitive model. 17 Protection Motivation Theory posits that environmental and personal factors combine to create a potential health threat which activates 2 cognitive pathways. The perceived threat initiates 2 cognitive processes: threat appraisal and coping appraisal. The threat-appraisal process evaluates the factors associated with the threat including perceived intrinsic rewards (eg, sex feels good) and extrinsic rewards (eg, my friends will think I am the man if I am having sex with a lot of girls) accompanying the behavior minus the perceived severity of the threat (eg, HIV would not be so bad) and one’s vulnerability to the threat (eg, I have had unprotected sex before and not contracted HIV). The coping appraisal process evaluates one’s ability to avert the threatened danger including both self-efficacy (eg, I would be able to tell my partner that I did not want to have sex) and response efficacy (eg, if I told my partner that I did not want to have sex, he would listen to me) balanced against the response cost (eg, my boyfriend might leave me if I don’t have sex). These 2 appraisal pathways combine to produce protection motivation (or intention), which if high enough may result in protective action. The adoption of a health behavior—whether a risk or a protective behavior—is thus a balancing between competing pathways and considerations.
Each of the 8 sessions of Focus on Kids addresses one or more of the constructs of Protection Motivation Theory through a series of interactive stories, games, and exercises. Facts about HIV/STDs and pregnancy are discussed. Negotiation and communication skills are presented and practiced through vignettes, role-playing, and games. Following a condom demonstration, games serve to familiarize the youth with the proper techniques in condom use. The “SODA” (
Focus on Kids was evaluated by a longitudinal, randomized, controlled trial involving 383 youth. A significant intervention effect on unprotected sex was found at 6 and 18 months and cumulatively over 3 years of postintervention follow-up. 18 Focus on Kids was identified by the CDC DASH Program as a “Program that Works” and as a “Promising Program” by the National Registry of Effective Programs.
Developing FOYC
The Bahamian team recognized that research was going to be critical to driving the program’s success. They also recognized the importance of active partnerships between the Ministries of Health and of Education to secure the grant to begin the FOYC project. Initially, the group went to Baltimore to visit the Focus on Kids program “at work” in the community and to meet with the developers. Utilizing formative research and several stages of curriculum adaptation (which are consistent with state-of-the-art adaptation recommendations 19 ), the US-Bahamian team produced a 10-session program entitled “Focus on Youth in the Caribbean” (FOYC) which retained most of the content of Focus on Kids except for the activities involving touching and practicing with an actual condom. Two additional sessions were added, one emphasizing sexual abuse and healthy relationships and the other providing more basic factual material regarding substance abuse and sexual risk behaviors given the correlation between alcohol and intercourse. The intervention was pilot-tested through a quasi-experimental design among 289 females aged 9 to 17 during lunch break or immediately after school. Condom use and protective perceptions were significantly higher among intervention youth. 20 The US-Bahamian research team recommended that the curriculum be administered at the sixth grade level because this approach would reach the majority of Bahamian youth before they initiated sexual intercourse. Since the majority of youth in sixth grade are aged 10 and 11, it was anticipated that most would be sexually inexperienced, although approaching sexual initiation. (See Table 1 for a synopsis of the FOYC intervention).
Brief Summary of the “Focus on Youth in the Caribbean” (FOYC) Curriculum

Abbreviations: SODA, Stop to think-consider your options and consequences-make a decision-take action; STD, sexually transmitted disease
The Ministry of Health then requested permission to temporarily relocate the individual who had previously worked with them in the drug prevention program who was then supervising School Psychological Services within the Ministry of Education. Permission was granted and ultimately she became the coordinator of the FOYC program.
Next Steps: Plans for Large Scale Evaluation and Addition of Critical Components
Buoyed by the success of the pilot test, officers of both the Ministries of Education and of Health met with the US team of researchers to discuss adapting the program for use in the school system, with plans to target children before they became sexually active. In preparation for introducing this to students in elementary schools, the US Bahamian team conducted a series of focus group discussions among children, parents, and teachers in The Bahamas. These discussions identified the need for 2 substantial additions to FOYC.
First, teachers and professionals from the Ministry of education were concerned that follow-up would be needed to the basic FOYC program, especially given the plans to deliver it to children in grade 6, the majority of whom would have little first hand experience with many of the topics being discussed in FOYC. Therefore, 2 booster sessions were designed to review key concepts in grade 7 and grade 8 (see Table 2 ).
Brief Summary of the 2 Booster Sessions for the “Focus on Youth in the Caribbean” (FOYC) Curriculum

Abbreviation: SODA, Stop to think-Consider your Options and consequences-Make a Decision-Take Action
Second, parents, youth, and teachers reported the need for educating parents about HIV, with a specific focus on communication between parents and youth as well as involvement of parents in helping youth to make healthy personal decisions. This request was timely as a growing literature was addressing the importance of parental involvement in adolescent HIV prevention. In fact, the US team was in the process of evaluating a parent component in Baltimore that had been developed based on a similar request from the community, although among parents of older youth.
Concurrent Developments in Parenting Interventions: Informed Parents and Children Together
While researchers in the United States and elsewhere were encouraged by the short-term effectiveness of some adolescent HIV prevention programs, concerns—which continue to vex the public health world—were emerging about the waning effect of even these successful interventions after relatively short intervals. 21–23 Researchers were exploring hypotheses that parents/other guardians could serve as an intervention option that could both sustain and broaden intervention effect. The protective influence of the parenting process, including parental monitoring, parent-child closeness, role modeling of appropriate sexual behaviors, parental disapproval of adolescent sexual activity, and parent-teen sexual communication have generally been shown to be among the most influential factors in adolescent’s lives. 24–28 Parent-teen sexual communication may be especially important, with evidence that such discussions may lead to later initiation of sex, less sexual activity, more consistent condom use, and lower self-reported rates of STDs. 29–34
The US researchers had attempted to address these issues in our parental intervention, Informed Parents and Children Together (ImPACT), which consists of a 20-minute culturally appropriate video followed by 2 supervised, interactive play-acting “vignettes”, a condom demonstration, and a condom activity in which the youth and parent practice correct condom use. The video, delivered to a parent-child dyad in the privacy of their home, emphasizes the importance of talking, in an age-appropriate fashion, openly and clearly about values and expectations as they relate to sexual practices. The follow-up discussion reinforces these messages and enables both the parent and youth to practice their newly acquired communication skills. To assess ImPACT, the US team conducted a series of evaluations culminating in a randomized trial of a combined youth face-to-face intervention with a parental monitoring intervention. In this trial conducted among 821 African American parent-youth (aged 12 to 16 at baseline with a median age of 14 years) “dyads” residing in 35 urban, low-income communities in Baltimore, all youth received a basic “face-to-face” adolescent risk reduction intervention (Focus on Kids) and about two thirds of youth with their parents also received ImPACT while the others received Goal for It (GFI), a 22-minute video emphasizing the importance of planning ahead and is followed by supervised discussion and answers. At 6, 12, 18, and 24 months postintervention, rates of sexual risk and drug risk behaviors were significantly lower among youth who received Focus on Kids plus ImPACT compared to those who received Focus on Kids plus GFI. 35,36
Next Steps: Caribbean Informed Parents and Children Together
Given the above-mentioned US experience with ImPACT in combination with Focus on Kids, the Bahamian Ministries of Education and of Health wished to explore a similar format, with some culturally appropriate changes. In the United States, ImPACT was delivered in the parent’s home to the parent and youth, and included a video featuring older youth, and involved handling a condom. Feedback from the Bahamian community identified several necessary modifications of the ImPACT parent intervention for use in The Bahamas. First, they recommended refilming the ImPACT video in The Bahamas using Bahamian preadolescents and their parents (eg, the age of sixth-grade students) rather than mid-adolescents and parents. Second, they asked that both of the parent interventions be delivered in a group setting (rather than one-on-one) and in community settings such as the elementary schools (rather than homes which would not be culturally acceptable). Finally, they wanted more scenes modeling parents talking with their children. The revised intervention, Caribbean Informed Parents and Children Together (CImPACT), required ~50 minutes to administer; 25 minutes to view the new video (filmed in The Bahamas with grade 6 youth rather than with youth in their mid-teens) followed by a condom demonstration to the parents, individual condom practice, and a group discussion. (See Table 3 for a brief summary of CImPACT.)
Brief Summary of Parent Intervention, Caribbean Informed Parents and Children Together (CImPACT)

Implementation and Effectiveness Trial of FOYC + CImPACT
The Ministries of Health and Education and the US researchers decided to conduct a longitudinal 3-celled randomized trial of FOYC and CImPACT and alternative youth and parent interventions among grade 6 youth and their parents attending 15 of the 26 government elementary schools in New Providence. The 15 schools were selected based on geographic representation (the 4 quadrants of the island), rural-urban considerations, and size and expressed interest on the part of the schools. Because the curricula were implemented as part of the Health and Family Life Education curriculum, all students in grade 6 in these 15 schools would receive the intervention to which the school was randomized. Therefore, the researchers, ministry officials, and teachers all felt very strongly that each intervention arm should offer a high-quality intervention of relevance to students. Because of the importance of water conservation and the need to preserve the ecosystem, the research team approached the Bahamas Natural Trust and the ecologist who agreed to prepare a 10-session water conservation curriculum for grade 6 youth entitled “The Wondrous Wetlands.” Teachers and students were delighted with the curriculum which had great relevance following 2 major hurricanes. For the alternative parent control, the US team had developed an intervention consisting of a video followed by role play detailing steps for career planning. The teachers and parents who previewed the film and intervention felt it was entertaining, instructive, and would be a valuable tool for parents. They did not feel that the video needed to be remade in The Bahamas.
Youth and parents from 15 of the 26 elementary schools located on the island of New Providence (the site of the capital, Nassau) were randomly assigned at the level of the school to receive (a) FOYC plus CImPACT for the parents (5 schools); (b) FOYC plus GFI for the parents (5 schools); or (c) the control, The Wondrous Wetlands, for the youth plus GFI for the parents (5 schools). Teachers and some guidance counselors from the participating schools received a 5-day training workshop in the appropriate curricula involving the theory of the curricula, an overview of the curricula, and a walk-through of the activities and role-play of the entire curricula. The 10 sessions of FOYC or The Wondrous Wetlands were delivered as part of the Health and Family Life Education curriculum. Parents who enrolled in the study received the appropriate intervention in groups on the weekend or evening. Youth who enrolled in the study received the baseline and follow-up questionnaire The Bahamian Youth Health Risk Behavioral Inventory (BYHRBI), 5 a cultural adaptation of the Youth Health Risk Behavior Inventory 35 to assess risk and protective knowledge, condom-use skills, perceptions, interventions, and self-reported behaviors. Ultimately, about two third of grade 6 youth in the 15 schools (1360 youth) and 1175 of their parents enrolled in the study. Youth who did not enroll did not complete questionnaires; their parents did not receive the parent intervention and did not complete questionnaires.
Commitment of The Bahamas to School-Based HIV Prevention Efforts
The dedication of The Bahamas to the research was demonstrated in countless fashions. Beyond the unsurpassable work ethic of the Bahamian research team, there was wide involvement of many members throughout the educational and health care system in multiple aspects of the project. Several guidance counselors, principals, teachers, nurses, and health educators became “core” trainers of the FOYC curriculum; they felt that without a cadre of trainers, it would be difficult to maintain the level of skill of the teachers given changes in personnel, leave etc. Many of these individuals also filled in during short-term illnesses to make certain that the curricula were consistently taught. Likewise, because the teachers were asked to leave the classroom during the administration of the baseline and follow-up questionnaires, many officers from the Ministries of Education and Health served as monitors. The teachers were very impressed with the Stop, Options, Decision, and Action (SODA) decision-making model; it became a part of their natural classroom environment, helping the class address challenges and conflicts that arise on a daily basis within the classroom and school setting. Several have made SODA posters which remain displayed in their classrooms. All elementary school teachers are required to teach Health and Family Life Education. Although they receive targeted training in other major subjects such as math and writing, previously they had no specific training in sexual health activities and many were not comfortable with topics such as sex, sexuality, and HIV prevention, particularly the condom. Prompted by the positive reactions of teachers to FOYC, discussions are ongoing in the Department of Education about introducing all teachers in training to the approach and to the materials contained in FOYC regarding how to discuss sexually explicit and other high-risk behaviors, including condom use and safe sex negotiations.
Finally, although the majority of funding was through the US National Institute of Mental Health, local groups (eg, Cable Bahamas Cares Foundation, the Exuma Foundation) as well as the US Embassy and the Pan American Health Organization also supported selected and extended activities of FOYC.
Intervention Effects
As shown in Table 4 , the intervention effects across 3 years for knowledge, condom-use skills, perceptions and intentions regarding condoms, and condom use behavior are strong. 5,37–39 Although condom use behavior only reached statistical significance at the 36-month follow-up, the trend was present earlier even though the rates of sexual activity were low (eg, insufficient power to detect a difference).Outcomes Beyond the Study Question
Condom-Related Behavior and Perceptions from Baseline through 36 Months Follow: FOYC + CImPACT versus Control
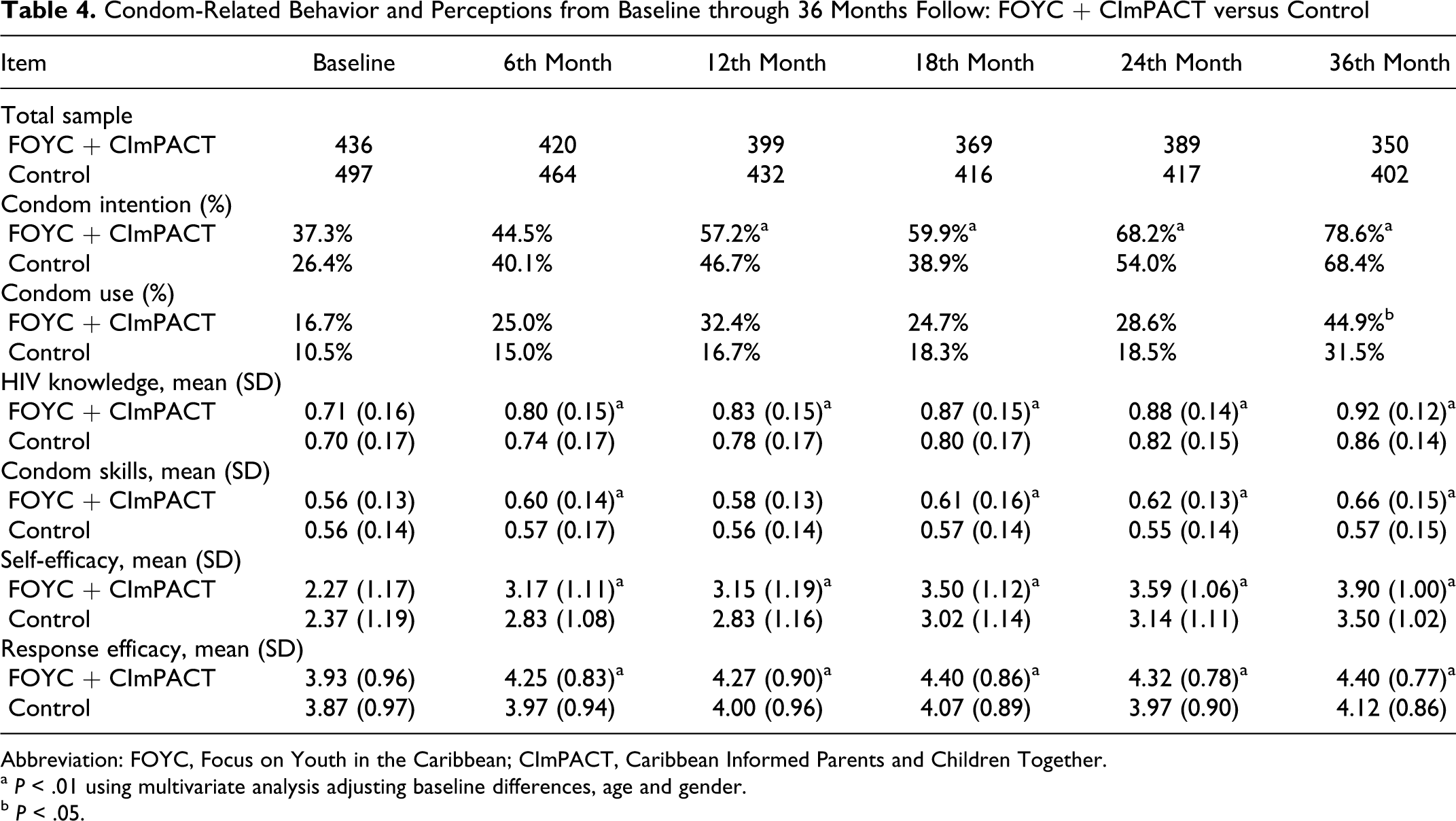
Abbreviation: FOYC, Focus on Youth in the Caribbean; CImPACT, Caribbean Informed Parents and Children Together.
a P < .01 using multivariate analysis adjusting baseline differences, age and gender.
b P < .05.
Both the research team and the Bahamian Ministries of Education and Health are very pleased with the results of the intervention trial. Beyond the study results, the relationships and anecdotal experiences have been equally as rewarding. Follow-up has been excellent (>80% in all waves) among all youth regardless of gender and intervention assignment. The high retention rate was impressive because after grade 6 (during which the baseline and 6 month follow-up were administered) the study children graduated from the 15 elementary schools and were dispersed among 7 government and about a dozen private and religious schools. Anecdotally, the US-Bahamian researchers observed that the youth enrolled in the study were excited to see the research team, often asking when we zwere going to teach them again and during the 36-month follow-up indicating that they wished to continue in the FOYC evaluation.
Parents have been very enthusiastic and became involved in many ways. Turnout for the evening parenting sessions was overwhelming; so much so that the schools began to ask if they could “piggy-back” other activities in which they wanted the parents to participate. Despite inclement weather including torrential rains and wind, parents would come. Many parents were interested in learning about the FOYC curriculum. One father was so charmed by the notion of the “family tree” discussions, that he built a wooden doll house which he gave to one of the schools for enactment of the exercise during the class discussions of the Family Tree. For many of the parents, including the control parents, just completing the questionnaire about parental monitoring and communication proved to be a valuable tool encouraging introspection and prompting questions about better ways to communicate with their children in general and especially with regard to uncomfortable topics.
The church became involved; in fact several of the scenes in the CImPACT video “Keeping the promise” were filmed in a local church while the pastor discussed the importance of informing youth about sex and sexual protection including condom use. Many church leaders were trained in the FOYC curriculum and have incorporated portions or all of it into their youth group training. Ministers who previously had responded to sexually active youth by delivering a strong abstinence-only message now refer these sexually active youth to organizations that provide safer sex counseling.
Where Are We Now? Working with Our Youth in High School
When compared to the youth receiving the control program, FOYC youth exhibit higher levels of condom use intention, supportive perceptions, and condom use behavior. However, the levels of condom use among both intervention and control youth are below 50%. Further, sexual initiation among this cohort of middle-school children is rapidly occurring, with a baseline sexual experience of 4% in both groups increasing to 33% of youth by grade 9. Finally, after several years of declining rates of HIV infection in The Bahamas, these past few years have witnessed rising rates which are largely among youth and young adults. Therefore, the Ministries of Education and Health are again collaborating with the US-Bahamian Research Team to identify an effective intervention that can be delivered to Grade 10 students and their parents in The Bahamas. Currently, we are conducting a randomized, controlled longitudinal trial among Grade 10 students in all 8 of the government high schools in New Providence.
Next Areas of Importance for Our Partnership; Concurrent Changes in the Field of Adolescent HIV Risk Prevention
The Department of Education of the Bahamas has decided to incorporate FOYC + CImPACT throughout the grade 6 curriculum. Since the beginning of our research partnership, the field as a whole has continued to advance. These advances have served to inform our partnership—and our partnership has contributed to the emerging field. Therefore, the Department of Education has decided to undertake the implementation in such a fashion as to better understand the critical elements necessary to sustaining effective programs within the classroom and to thereby continue to inform research efforts.
The need to move science to practice has inspired countless publications and lectures and serves as the foundation for the National Institutes of Health Roadmap Initiative. Efforts to move science into the community (the “Translation 2 Roadway”) have focused renewed efforts on understanding the processes of diffusion (defined as the uncontrolled or natural spread of innovations), dissemination (defined as purposeful or deliberate efforts to move an innovation), and the final step, implementation (defined as adoption or utilization of the innovation). 40 Traditionally, implementation has generally been conceptualized as the final step of the broader processes of diffusion or dissemination and, as such, has typically not been the primary focus of the theory or research. Green et al argue that implementation requires a separate paradigm or theoretical framework from that of the dissemination of science, which is typically supported by “highly centralized (mostly federal and national) funding, storage, indexing, synthesizing and communication of science, whereas application of that science is highly decentralized” 40(p 154) Our increased understanding of the process of diffusion and the dissemination of effective interventions has led to increased recognition of the need for focus on the related but unique issues of implementation. 40,41 Central among the issues to be addressed in implementation research is better understanding of the role of fidelity in achieving comparable outcomes to the original intervention.
Currently, the Ministries of Health and Education and the US-Bahamian Research Team are planning to roll out FOYC plus CImPACT in a manner that will also allow them to explore important questions in implementation and fidelity.
Footnotes
Acknowledgments
This research was supported by National Institute of Mental Health. We gratefully acknowledge the contributions of many people including other members of the US research team (Jim Chen, Xiaoming Li, Carole Harris, Lesley Cottrell, Lisa Sorensen, Sharon Marshall, Shuli Yu, Linda Kaljee, Jennifer Galbraith,, Pamela Albertsen, Rebecca Clemens, Lindsay Welles, and Kristen Albertsen), the Bahamian Ministry of Education and the Ministry of Health, The Bahamas National Trust and Cable Cares. A special tanks goes to the many students, parents, teachers, and school administrators as well as the many community religious and civic leaders who helped make FOYC + CImPACT possible. We thank Madeline Balice for her help with this manuscript.
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.