
Abstract
The vascular laboratory was asked to evaluate a 1-day-old male infant who presented with a neck mass that was first detected by prenatal ultrasound imaging. Duplex ultrasound imaging revealed an internal jugular venous aneurysm that was later confirmed by computed tomography (CT) imaging. The diagnosis was consistent with internal jugular vein phlebectasia, a rare congenital venous anomaly characterized by an abnormal dilatation of a vein. This case highlights the capability to provide early diagnosis using non-invasive imaging techniques in identifying venous anomalies in neonates. Although internal jugular vein phlebectasia is uncommon, it should be considered in the differential diagnosis of neck masses in infants and young children. Early recognition allows for appropriate management and follow-up for these patients.
Introduction
A venous aneurysm is an abnormal dilation or bulging of a vein, resulting from a weakening of the vessel wall. Although symptoms are not always present, when they do occur, they may include visible swelling or a lump under the skin, localized pain at the site of the aneurysm, or varicose veins associated with venous insufficiency. Several factors contribute to the weakening of vein walls, including congenital abnormalities, chronic inflammation (often due to vasculitis), trauma from surgery or accidents, arteriovenous fistulae, and deep vein thrombosis, all of which can compromise the structural integrity of the veins.
Internal jugular phlebectasia, a rare congenital form of venous aneurysm, typically occurs unilaterally. 1 It is most commonly observed in young children during episodes of increased intrathoracic pressure, such as coughing or sneezing. This may be the first reported case of prenatal detection of internal jugular phlebectasia with post-partum ultrasound confirmation on the first day of life. Treatment is typically conservative, as spontaneous rupture of these aneurysms has not been reported.
Case Report
A healthy 23-year-old pregnant patient presented to the high-risk obstetric (OB) ultrasound department for a detailed anatomy scan of the 37-week and 1-day old fetus. During the scan, a cystic structure was identified below the right fetal mandible, extending into the right side of the neck. The largest cystic component measured 4.4 × 1.6 cm (Figure 1). The identified structure appeared to have blood flow (Figure 2). A fetal magnetic resonance imaging (MRI) was obtained and revealed a large vessel on the right side, extending into the mediastinum, possibly representing the internal jugular vein and superior vena cava (Figure 3). The male infant, born at 37 weeks and 2 days, was referred to the non-invasive vascular lab on his first day of life for imaging of the central venous system.
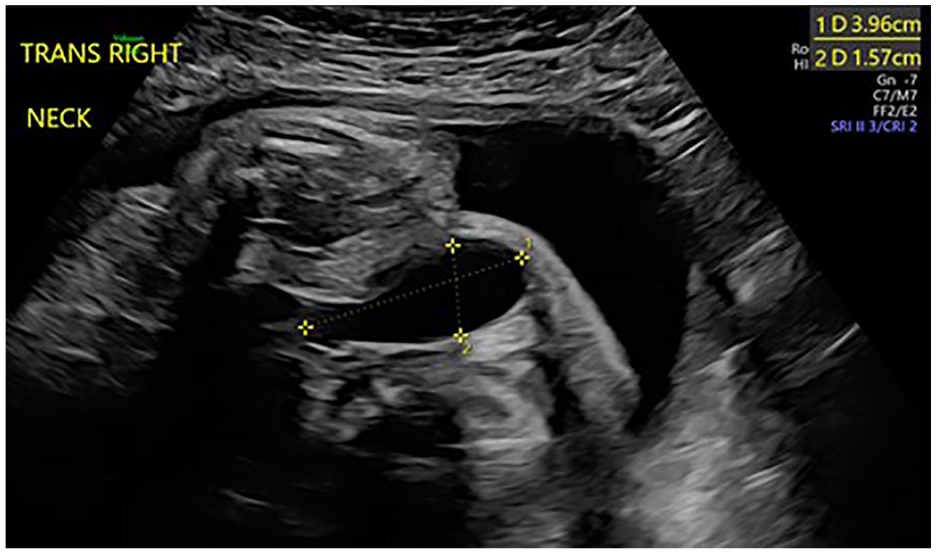
Prenatal B-mode ultrasound of a right neck tubular echolucent structure.
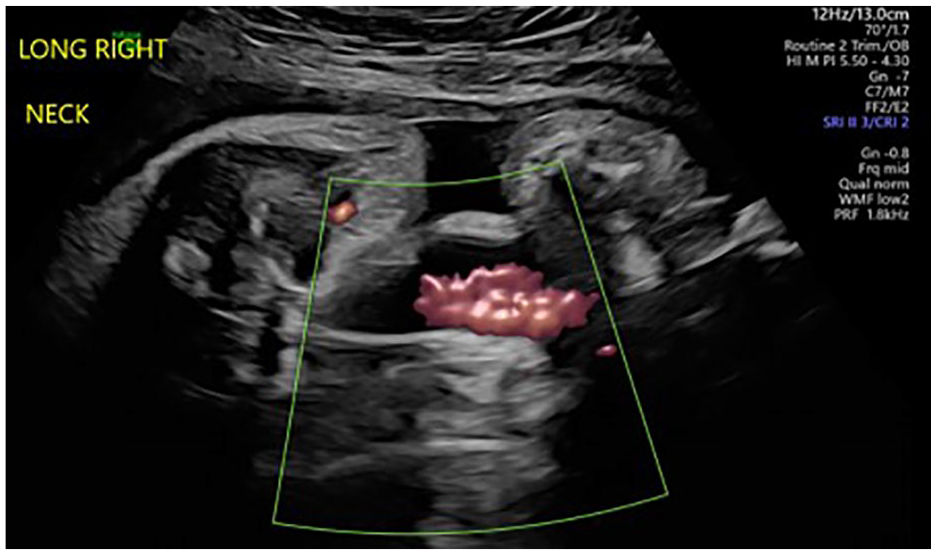
Prenatal power Doppler ultrasound of the right neck showing vascularity.
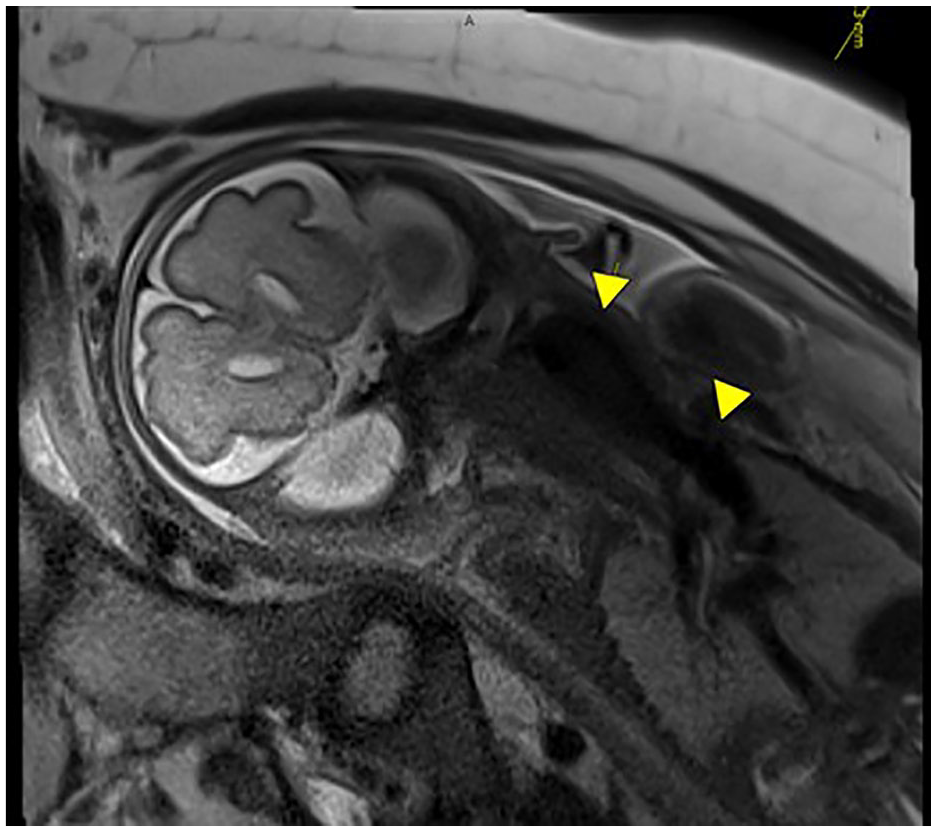
Prenatal MRI depicting a large vessel extending from the right neck into the mediastinum, possibly the internal jugular vein as it becomes the brachiocephalic vein. MRI=Magnetic Resonance Imaging.
A vascular duplex ultrasound exam showed a patent right internal jugular vein with measurements of 1.3 × 2.7 × 3.9 cm (Figures 4 and 5). The subclavian, brachiocephalic, and axillary veins were all patent, demonstrating spontaneous, phasic venous Doppler flow signals. No thrombus was identified in the evaluated vessels. The contralateral internal jugular vein measured 0.3 × 0.4 cm (Figure 6).
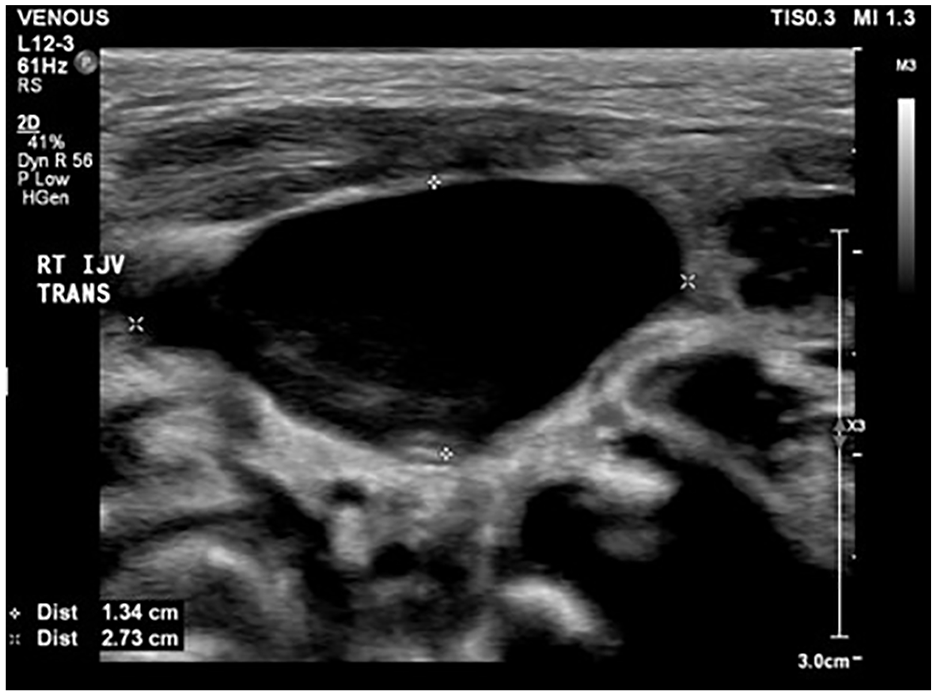
B-mode ultrasound with measurements of the right internal jugular vein in the 1-day-old infant.
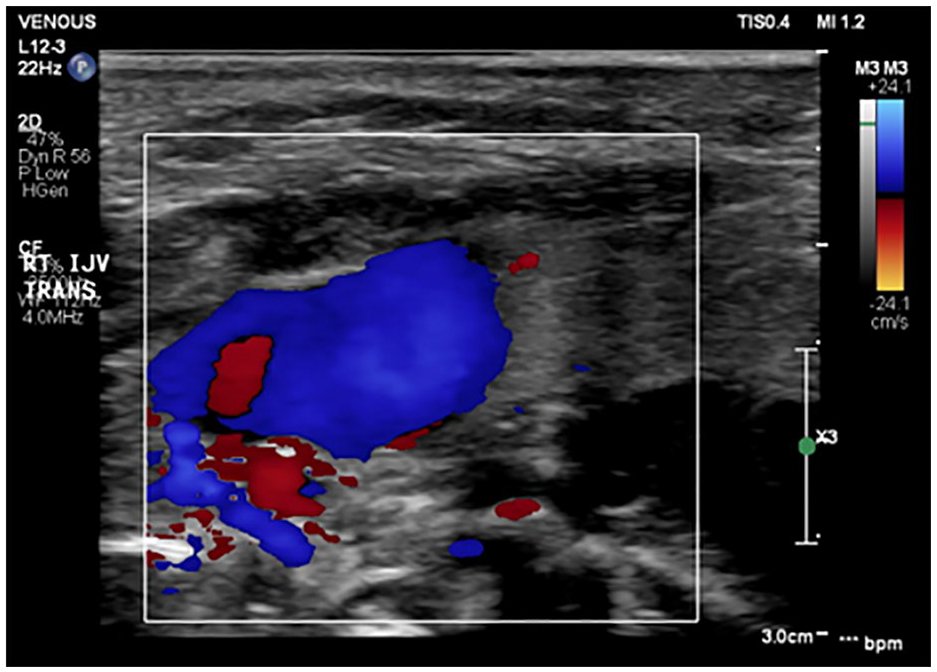
Color Doppler image of the right internal jugular vein.
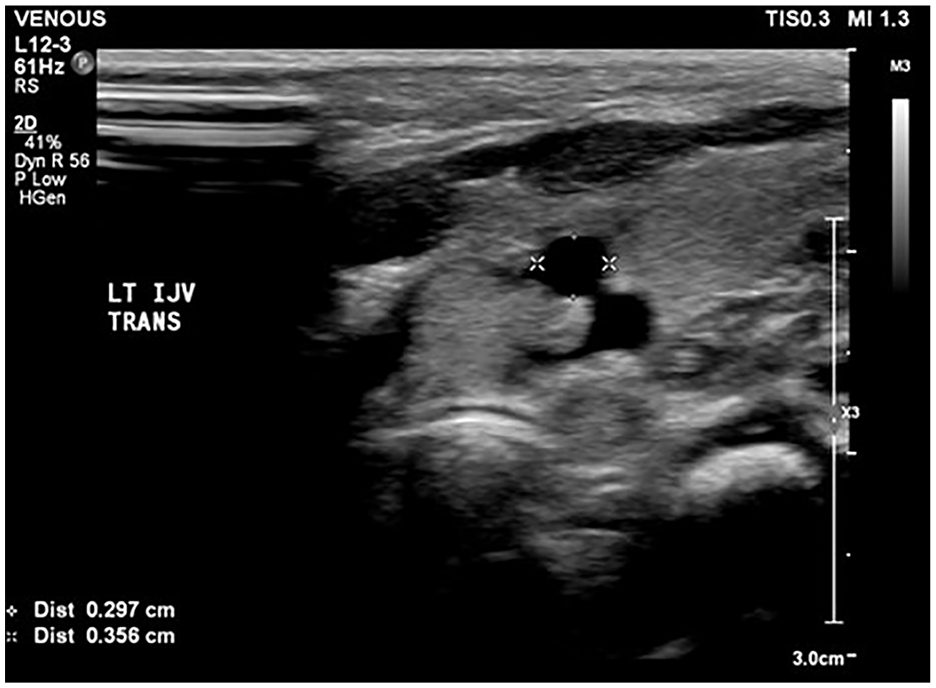
Left internal jugular vein showing normal size.
A computed tomography (CT) venogram confirmed the vascular ultrasound findings (Figure 7). The patient was diagnosed with internal jugular phlebectasia and discharged on day 2 of life. Conservative management was elected with annual follow-up; earlier evaluations as needed if symptoms arise.
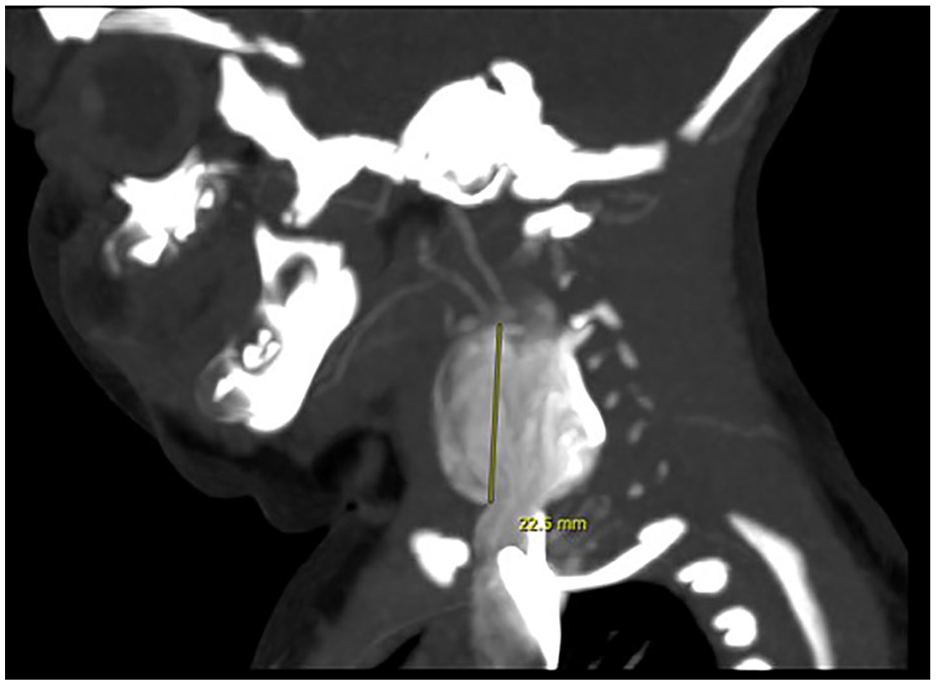
CT venogram with contrast-enhancing right neck mass in continuation with the right internal jugular vein, which changes shape and density on the venous phase, consistent with an internal jugular vein aneurysm (phlebectasia). CT=Computed Tomography.
Discussion
Phlebectasia refers to abnormal dilation of a vein without the characteristic tortuosity that often accompanies varicose veins or aneurysms. This condition can affect veins throughout the body but is most commonly observed in the neck, specifically the internal jugular vein, as well as the external jugular, anterior jugular, and other communicating superficial veins 2 (frequency of occurrence is in descending order). Males are twice as likely to be affected than females, although the reasons for this gender disparity are not understood. 3
Internal jugular phlebectasia is typically seen in childhood. Symptoms include swelling in the neck that is aggravated by straining, sneezing, coughing, bending, valsalva, and/or after exertion. Ultrasound is the primary diagnostic tool for phlebectasia, as it allows for the visualization of the vein’s patency and dilatation. The CT scans and venography are additional imaging techniques that can be used to further assess the condition, particularly in complex cases where ultrasound may not provide sufficient detail. 4
There are 2 primary approaches to management: conservative management and surgical management. Conservative management is recommended for many patients with phlebectasia, especially those presenting with benign, asymptomatic cases. Supporters of conservative management argue that the condition is typically non–life-threatening and that there have been no significant complications, such as rupture or thrombosis, in the majority of cases. This approach emphasizes the natural history of the condition, which often does not require intervention. Close observation allows for the monitoring of any potential changes in the condition, providing an opportunity for timely intervention if complications arise.
Surgical intervention is advocated by those concerned about the potential risks associated with phlebectasia, such as intraluminal thrombus formation and rupture of the dilated vein. Surgical options include:
Ligation of the affected vein
Longitudinal constriction suture venoplasty—a technique used to reduce the size of the dilated vein by suturing it lengthwise
Partial resection of the phlebectasia, which involves removing the dilated segment of the vein
Wrapping the dilated segment with a PTFA tube graft—a newer technique that involves reinforcing the vein with synthetic material to prevent rupture. Notably, this option preserves the venous drainage of the brain. 2
Surgical management is not without risks; potential complications may include damage to nearby structures or infection. However, surgery may be necessary when the risk of thrombosis or rupture outweighs the potential risks of intervention.
Currently, there is no consensus on the optimal management approach for internal jugular phlebectasia. 5
Conclusion
Although the exact cause of phlebectasia remains unclear, this case emphasizes the congenital component of the condition. Both prenatal ultrasound and postnatal ultrasound play a crucial role in the early diagnosis and conservative management of internal jugular phlebectasia. Early identification through non-invasive imaging can assist in monitoring the condition and guide appropriate management strategies, ensuring better outcomes for affected patients.
In 2024, our level 1 trauma center conducted a total of 547 vascular ultrasounds on pediatric patients across different age groups: 262 on infants (0 to 2 years old), 118 on children (3 to 12 years old), and 167 on adolescents (13 to 18 years old). Although these 547 pediatric exams represent only 4.8% of our total vascular ultrasound procedures, they are vital for the diagnosis and management of a variety of conditions in the pediatric population.
Pediatric vascular ultrasounds are most often ordered for and are particularly valuable for detecting iatrogenic complications such as deep vein thrombosis, arteriovenous fistulas, and arterial occlusions. These conditions result from medical interventions and require prompt detection and management to prevent further complications. However, vascular ultrasound exams can also be instrumental in recognizing congenital vascular disorders. Early identification of these conditions is crucial for ensuring appropriate management and achieving optimal outcomes for pediatric patients.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.