
Abstract
The utilization of deep vein arterialization (DVA) is a feasible and successful operative strategy for patients with severe chronic limb-threatening ischemia (CLTI) with no open or endovascular surgical options other than major limb amputation. The DVA technique creates a connection, either percutaneously or surgically, between a source of arterial inflow and venous outflow, allowing distal blood flow to heal chronic wounds that otherwise would have required amputation. In this case report, we describe a single patient with CLTI and nonreconstructable arterial disease and a chronic nonhealing wound who underwent a percutaneous DVA procedure with improvement in their ischemic rest pain and complete healing of their wound.
Keywords
Introduction
Chronic limb-threatening ischemia (CLTI), characterized by ischemic rest pain and nonhealing wounds with or without gangrene (Rutherford 4 to 6 categories), represents a severe form of peripheral artery disease (PAD). Up to 20% of CLTI patients have no endovascular or surgical options for revascularization. This can be due to the location of atherosclerotic lesions, lack of appropriate bypass target or conduit, or severe medical comorbidities, leaving patients with amputation as the only surgical option. 1 However, recognizing the significant damaging medical and psychological effects of amputation and a 5-year mortality rate of 52% to 80%, limb preservation remains the goal of CLTI treatment. 2 With an incidence of 50 to 100 CLTI cases per 100 000 adults in the United States, as well as up to 20% mortality, finding a successful surgical approach can be challenging. 3
Although endovascular techniques have improved, the rates of comorbid conditions such as diabetes, hypertension, and kidney disease have increased as well, making conventional revascularization challenging and often not an option. This can result in untreated pain and nonhealing wounds due to lack of arterial flow, and patients are often referred for amputation. 4 Deep vein arterialization (DVA) is a revascularization technique that involves the creation of a fistula between a proximal arterial inflow source and a distal venous outflow site in order to perfuse the distal limb that may offer a treatment option for patients who otherwise would require amputation. 5 In this report, we present a case study of a patient with Rutherford category 5 CLTI who had no endovascular or conventional open surgical options for limb revascularization and who successfully underwent a DVA procedure for limb salvage.
Case Presentation
A 76-year-old male with a past medical history of hypertension, myocardial infarction requiring drug-eluting stent placement, diabetes mellitus (hemoglobin A1c 6.8), and PAD presented to the Emergency Department with acute pain in his left foot, left fifth toe dry gangrene, and ischemic eschar on his left heel. He had undergone an endovascular intervention for CLTI 6 weeks prior (Figures 1 and 2). He had monophasic Doppler signals present in both pedal vessels bilaterally. A computed tomography angiogram was performed that revealed severe atherosclerotic disease of the bilateral tibial arteries with no runoff visualized to the ankles. A catheter angiogram showed severe distal small vessel disease with no options for endovascular revascularization and very poor bypass options. The patient also lacked an appropriate saphenous vein conduit for a bypass graft (Figure 3). Based on these findings, he was deemed an appropriate candidate for DVA for limb salvage.

Ischemic changes on the left fifth toe.

Ischemic changes on the left heel.
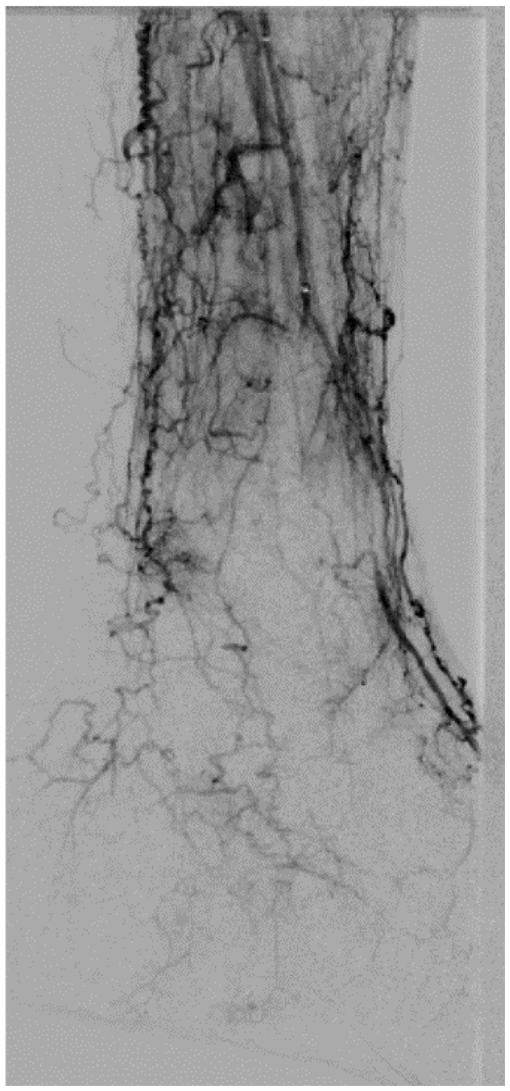
Angiogram showing severe distal small vessel disease.
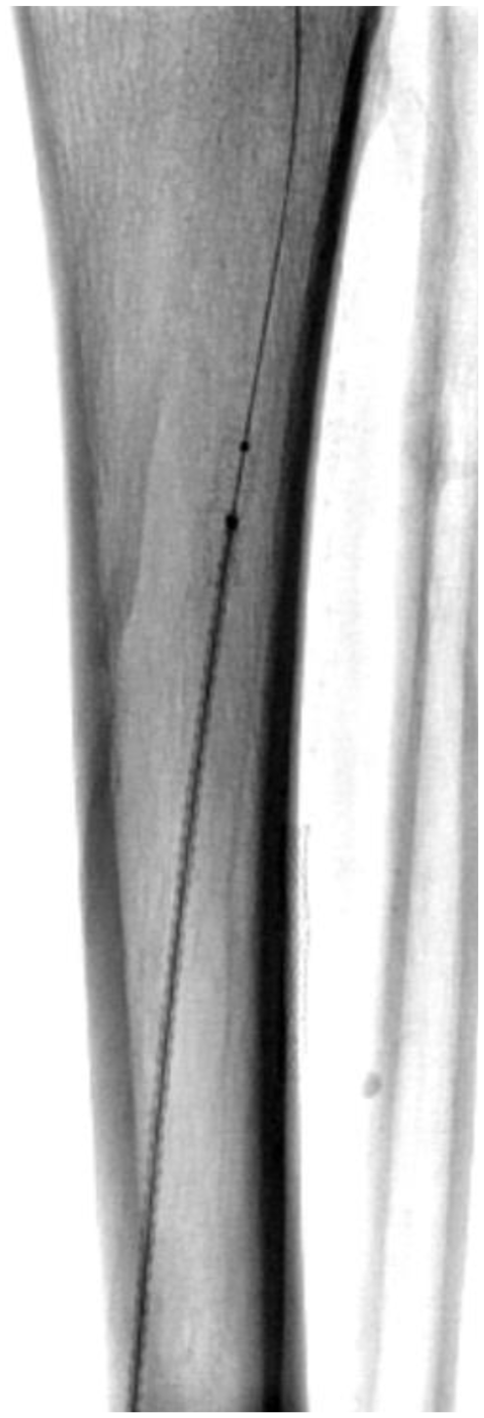
The angiogram revealed widely patent superficial femoral and popliteal artery segments and patent proximal tibial arteries with long segment occlusions and no major vessels crossing into the foot. Antegrade puncture of the ipsilateral common femoral artery, along with retrograde puncture of the common plantar vein, was performed, and 0.014″ wires were passed into the proximal posterior tibial artery and vein. From the arterial access, an intravascular ultrasound-guided re-entry device (Pioneer Plus, Philips Volcano) was used to cross between the posterior tibial artery and vein. With a micro-snare in the posterior tibial vein, this crossing wire was captured and externalized through the common plantar vein sheath. Next, the arteriovenous fistula was dilated with a 3 mm balloon and crossed with a 3.5 mm covered coronary stent. The posterior tibial vein was predilated with a 4 mm balloon and a 5 mm covered self-expanding stent was advanced through the fistula, and the vein was stented from the fistula down to the level of the lateral plantar vein (Figure 4). An antegrade wire was passed into the medial plantar veins and across the plantar venous arch, a 4.5 mm bare metal woven self-expanding stent was placed across the valves in the common plantar vein, and balloon angioplasty of the entire plantar venous arch was performed into the anterior tibial veins for outflow. Completion angiogram revealed excellent arterial flow through the fistula and into the plantar venous arch (Figure 5).
Arteriovenous fistula dilatation and covered coronary stent placement.
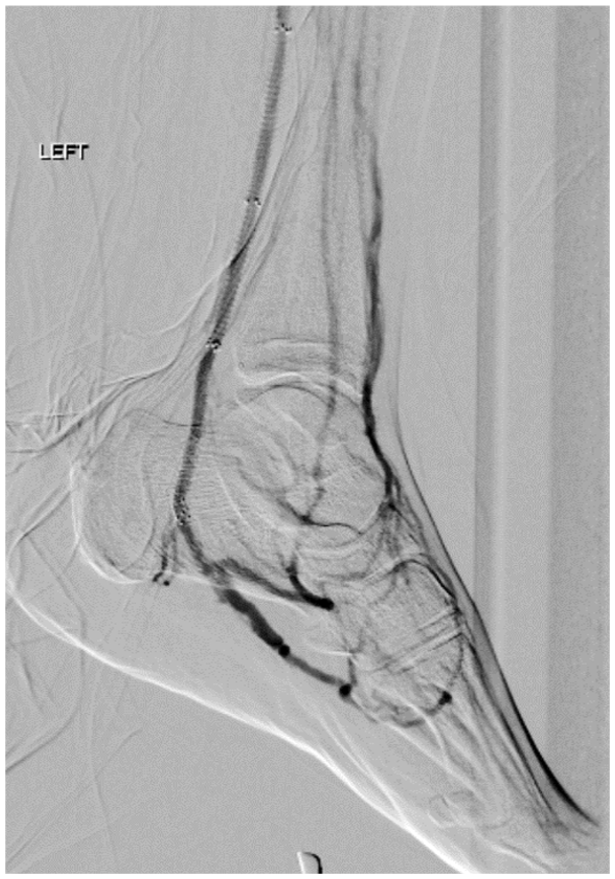
Post deep vein arterialization angiogram showing arterial flow through the fistula into the plantar venous arch.
Upon completion of the procedure, the patient had a low resistive multiphasic Doppler signal at the level of the ankle with a palpable pulse in the posterior tibial vein. Duplex imaging showed arterialization of the vein (Figures 6 and 7). He was discharged from the hospital on postprocedure day 5 with no lower extremity pain, and imaging done at follow-up showed the left posterior tibial artery with a patent stented fistulous connection to the arterialized posterior tibial vein. He underwent left fifth toe amputation due to gangrene 6 weeks after the DVA procedure, allowing the arterialized vein time to mature. His calcaneal wound and toe amputation site went on to heal due to the improved arterial perfusion to the foot, and he is currently ambulatory at home. The DVA fistula did thrombose after 5 months when the patient had to stop blood thinners due to hematuria.
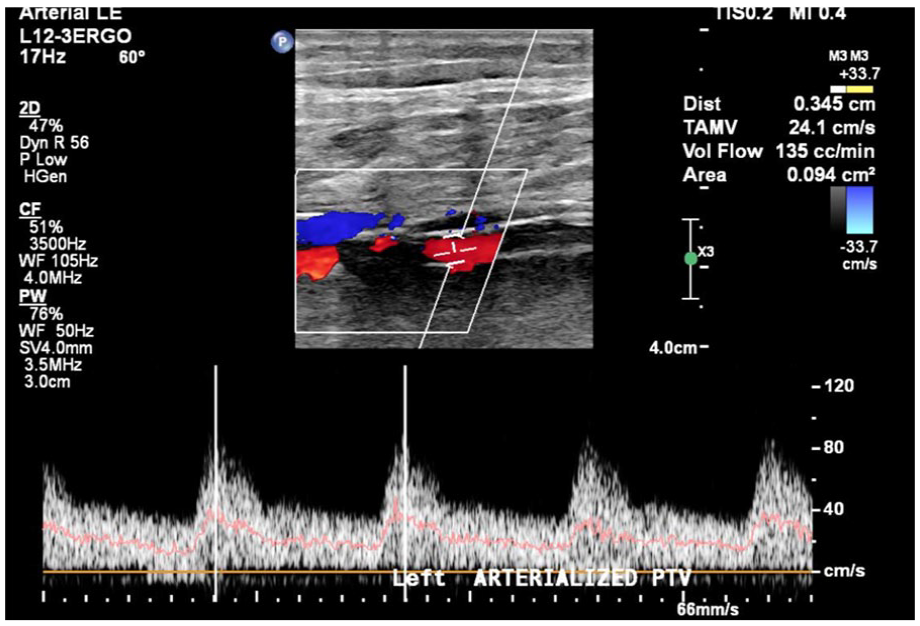
Duplex image showing arterialized low resistive flow in the left posterior tibial vein.
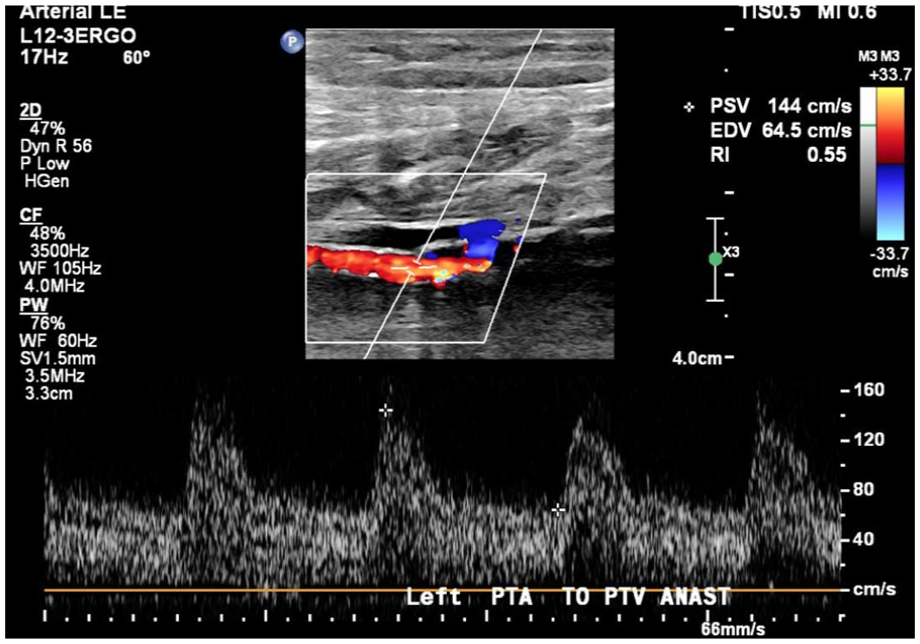
Duplex image of the left posterior tibial artery to posterior tibial vein fistula.
Discussion
More than 10 million people are affected by PAD in the United States. With 5% to 10% of those people progressing to CLTI, additional interventional techniques such as DVA are necessary for limb salvage. This approach can provide an option for treating those patients deemed as having “no-option” CLTI. The DVA concept, which proposed using a conduit to the venous system to help arterial perfusion of the extremities, was first reported in 1912. 6 Since then, open and endovascular surgical options have been utilized; however, as comorbidities of patients have worsened and increased number of CLTI patients have no surgical options, DVA has become an endovascular option at some centers.
Kum et al 7 recruited 7 patients with CLTI with no traditional endovascular or surgical revascularization options who were at high risk of amputation, and all underwent DVA. Each of the patients was successfully treated with no amputations and resolution of claudication and improvement of wounds following DVA. Because of the rarity of DVA, more studies are needed on this intervention, in addition to tracking long-term outcomes. The PROMISE II trial is currently assessing the efficacy of DVA utilizing the LimFlow system (LimFlow, Inc.) for CLTI with no other endovascular or open surgical options. 2 This trial will monitor the incidence of complications and long-term outcomes, which will be important in documenting the results of DVAs. Complications from DVA can occur, including thrombosis and loss of patency of the DVA conduit and limb loss. 2
Conclusion
In this case report, utilization of DVA provided a successful endovascular option for limb salvage. The use of duplex ultrasound to monitor the DVA procedure is essential, especially when trying to time a second procedure, as in this case. While this is a single case report, DVA should be considered in patients without other surgical or endovascular options in an attempt to salvage limbs and reduce the number of major amputations, as well as improve CLTI symptoms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.