
Abstract
Symptomatic ischemic steal syndrome (ISS) is a complex complication that develops in a small number of patients who have undergone a dialysis access procedure. This report describes the case of a 44-year-old female with aberrant upper extremity arterial anatomy who developed ISS following a radio-cephalic fistula. Ultrasound evaluation revealed abnormal blood flow in the radial artery and identified a communication between the radial and ulnar arteries distal to the anastomosis of the arteriovenous fistula. These findings assisted with the development of a surgical plan to ligate the intervening radial artery which resulted in resolution of the ISS symptoms.
Introduction
An arteriovenous fistula (AVF) is the preferred access for hemodialysis in patients with end-stage renal disease (ESRD). 1 The benefit of an AVF is improved long-term patency and lower risk of infection as compared to other types of dialysis access. The importance of dialysis access though an AVF was reinforced through Medicare’s Fistula First Breakthrough Initiative. The goal of this initiative is to have 50% of new patients begin hemodialysis through an AVF and 40% of patients to be dialyzed long-term through an AVF. 2 However, even with the many benefits of an AVF, the surgery is not without complications. These include hematoma formation, nerve damage, failure of maturation, early thrombosis, and ischemic steal syndrome (ISS).
The development of ISS following AVF creation is a hemodynamic complication that results in loss of antegrade blood flow to the hand. The clinical manifestations of ISS include pain in the hand at rest, hand pain during dialysis, and eventual tissue loss. The hemodynamic patterns that are associated with this complication are inadequate arterial inflow, high distal arterial resistance, and low resistance of the venous outflow. 3 The incidence of ISS among patients undergoing arteriovenous access procedures ranges from 0.2% to 9%. 4 Patient risk factors associated with development of this complication are female gender, diabetes mellitus, peripheral arterial disease, coronary artery disease, and a previous history of ISS. 3 Multiple surgical procedures have been developed to treat ISS by correcting the abnormal hemodynamic patterns. We present a case where a novel technique was utilized to treat a patient with aberrant upper extremity arterial anatomy and ISS. Written informed consent was obtained from this patient to publish this case and any associated images.
Patient Description
A 44-year-old female with a medical history significant for ESRD, diabetes mellitus, hypertension, and morbid obesity was found on preoperative imaging to have a high (proximal) brachial artery bifurcation in her non-dominant left arm. This aberrant brachial artery anatomy is relatively common with an incidence of 8% in the general population. 5 She subsequently underwent creation of a left radio-cephalic fistula just proximal to the antecubital fossa. The fistula matured as expected but required superficialization to allow for cannulation.
Upon initiating hemodialysis, the patient developed debilitating left upper extremity pain and numbness in the first 3 digits of the left hand. These symptoms were not present at baseline and only occurred during dialysis sessions. The patient had a clinical diagnosis of ISS, and an ultrasound examination was performed to determine the hemodynamic characteristics of the AVF. For this procedure, we utilized the GE Logiq E9 and a linear 9L probe. The AVF had an adequate mean flow volume of 902 ml/min. There was retrograde blood flow in the radial artery just distal to the fistula (Figure 1); however, the flow became anterograde in the distal forearm (Figure 2). The ulnar artery also had antegrade blood flow along its course. An aberrant connection between the ulnar and radial arteries was visualized distal to the anastomosis of the AVF (Figure 3). Photoplethysmography was performed in all digits of the left hand and waveforms demonstrated adequate amplitude in each digit, and this finding did not change with compression of the AVF. These results demonstrated that there was no evidence of ISS at rest, but the patient developed symptoms during dialysis secondary to decreased venous resistance.
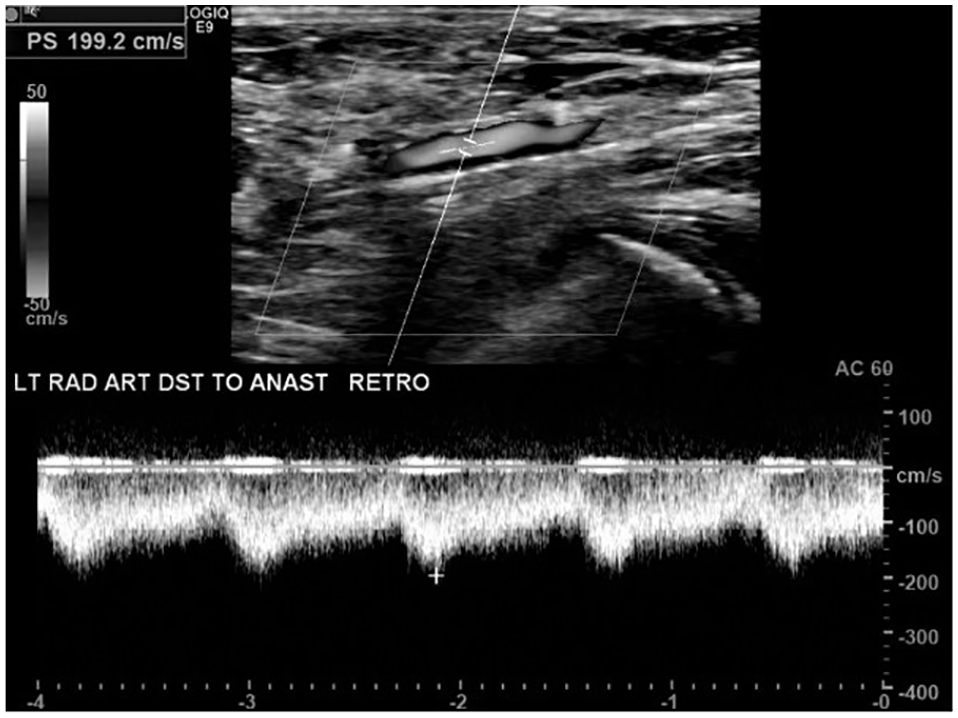
B-mode image and spectral waveform taken from the left radial artery just distal to the anastomosis of the arteriovenous fistula showing retrograde flow direction.
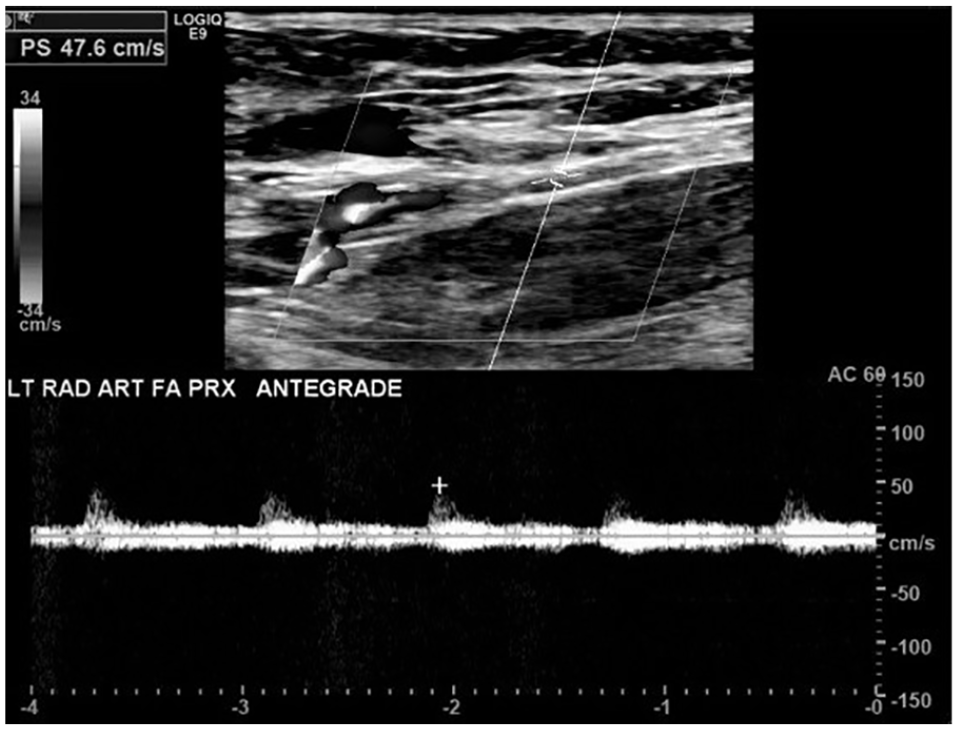
B-mode image and spectral waveform taken from the left distal radial artery showing antegrade flow direction.
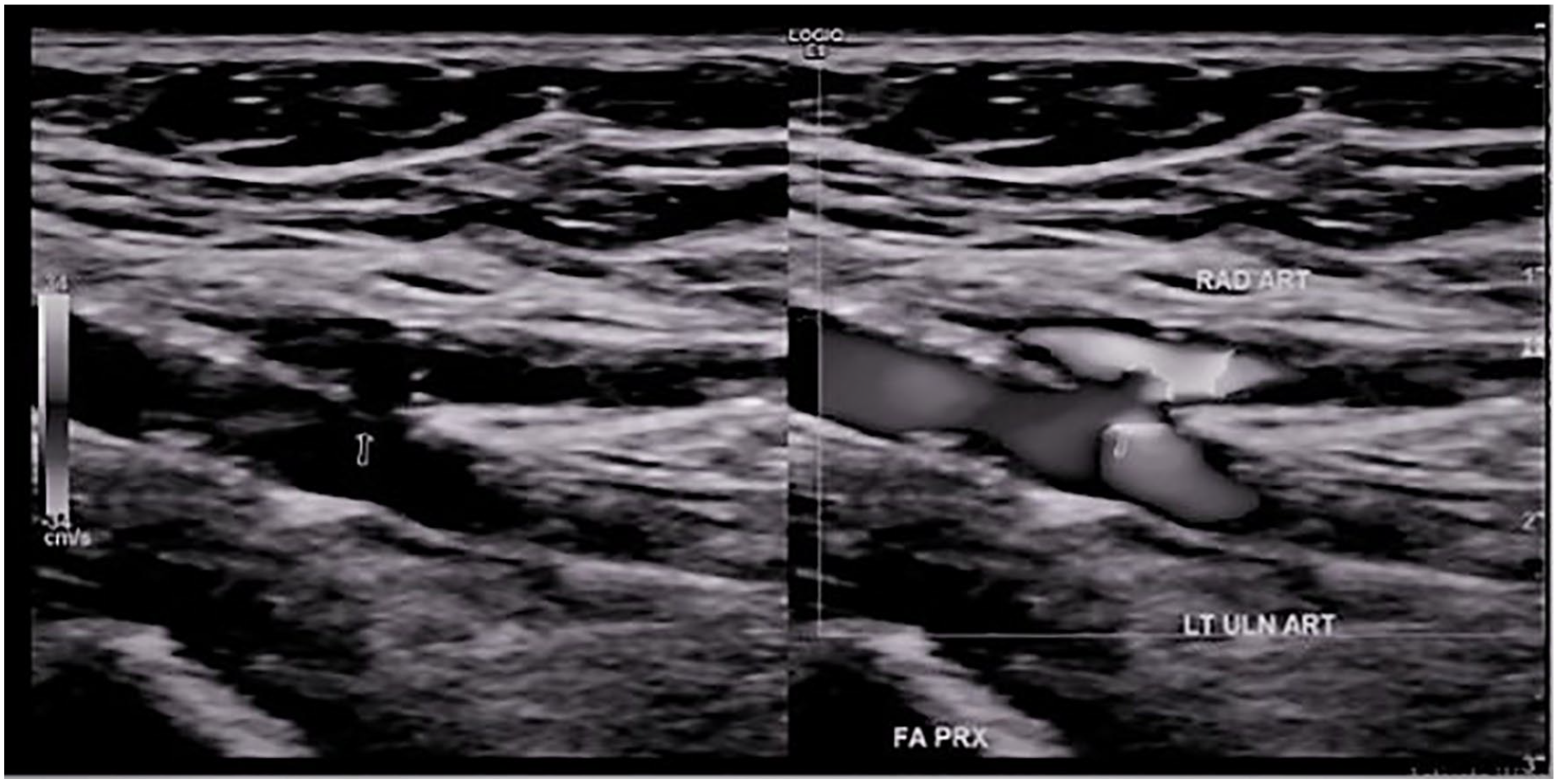
Power Doppler image of the aberrant connection between the left radial and ulnar arteries.
The information regarding the AVF and forearm hemodynamics provided by the ultrasound examination is summarized in Figure 4 and allowed for an operative strategy to be developed. The procedure consisted of ligation of the radial artery distal to the anastomosis of the AVF but proximal to the aberrant connection of the radial and ulnar arteries. Following this procedure, the patient recovered well without incident.
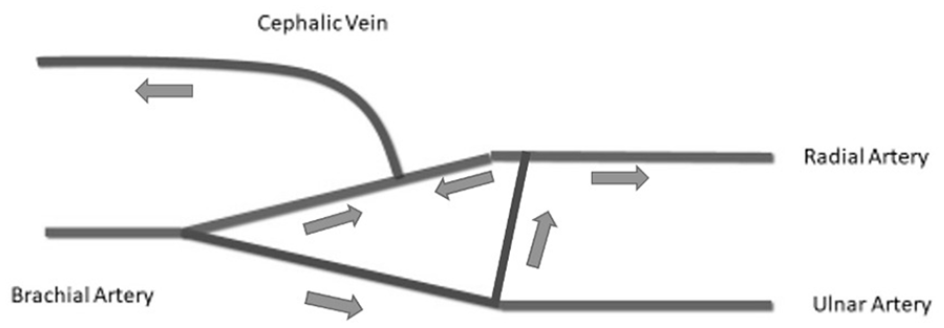
Diagram of the hemodynamics of the left upper extremity arteries as shown by the initial ultrasound examination. There is retrograde flow in the radial artery just distal to the arteriovenous fistula anastomosis.
A repeat ultrasound examination of the AVF was performed postoperatively. This demonstrated a patent radio-cephalic fistula with adequate flow. The inflow to the fistula was the proximal radial artery. The portion of the radial artery that had been ligated was occluded (Figure 5). The ulnar artery was patent with antegrade blood flow, and the patient had antegrade flow in the radial artery via the aberrant connection between the radial and ulnar arteries. The hemodynamic pattern following ligation of the radial artery is summarized in Figure 6. Photoplethysmographic waveforms in all digits of the left hand demonstrated adequate amplitude postoperatively.
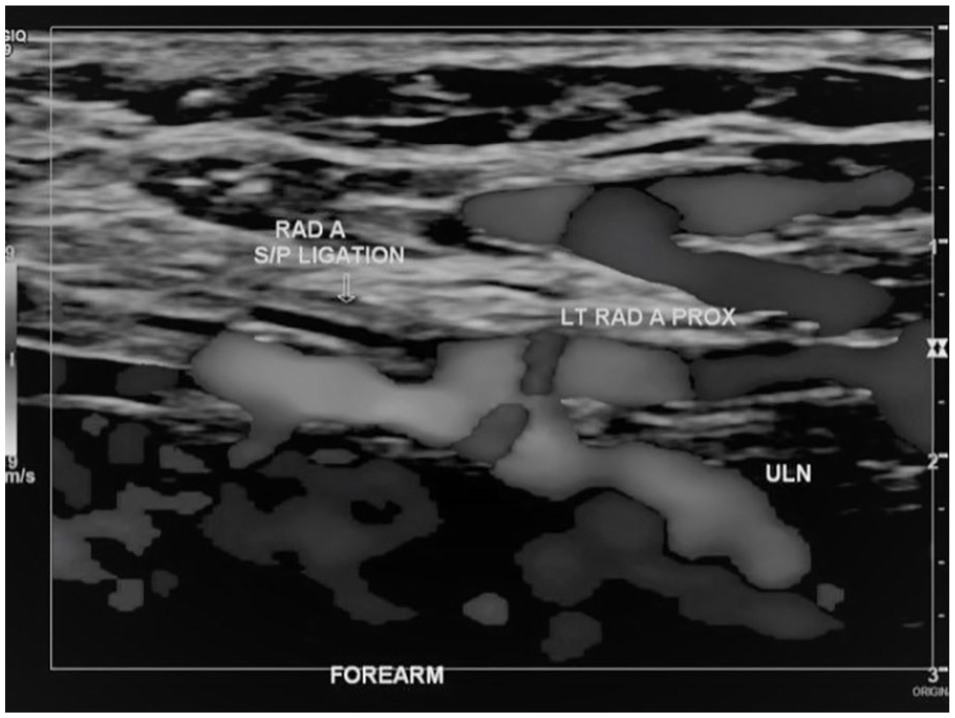
Power Doppler image of the ligated left radial artery and the aberrant connection between the radial and ulnar arteries.
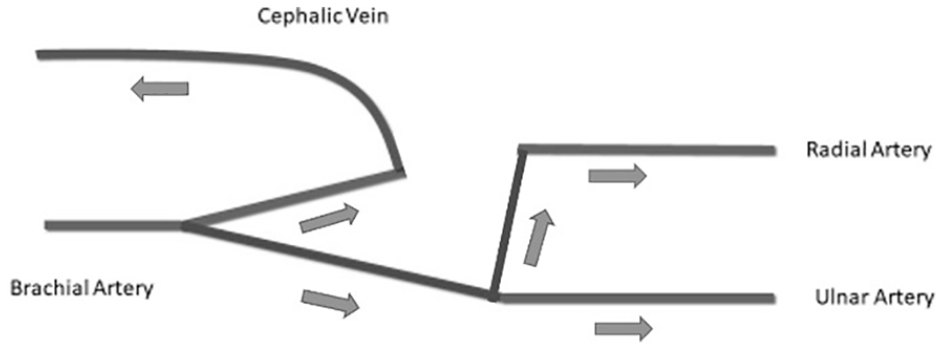
Diagram of the hemodynamics of the left upper extremity following ligation of the radial artery just distal to the arteriovenous fistula anastomosis.
Following this surgical revisional procedure, the patient reported improvement in symptoms and was able to tolerate hemodialysis sessions without further episodes of hand discomfort.
Discussion
Symptomatic ISS is a clinical diagnosis, and the hemodynamic factors that cause this condition are complex. Ultrasound examination and the use of photoplethysmography are integral studies that assist in elucidating the anatomy and hemodynamics of the AVF. The gold standard for diagnosis of arterial steal is through angiography; however, ultrasound is a valuable tool in the evaluation of ISS, and in some cases can replace angiography. 6 The results of Doppler ultrasound can be utilized to create surgical strategies to treat ISS.
Numerous surgical procedures have been developed to treat ISS by altering the hemodynamics of the dialysis circuit. These include ligation of the access, banding of the access, revision using distal inflow (RUDI), proximalization of arterial inflow (PAI), distal radial artery ligation (DRAL), and distal revascularization with interval ligation (DRIL). 7 The standard description of the DRIL procedure requires a bypass from the brachial artery proximal to the AVF anastomosis to the brachial artery distal to the anastomosis; the brachial artery between the AVF anastomosis and the distal portion of the bypass is then ligated. This configuration allows blood to reach the hand first by traveling through the bypass prior to blood entering the AVF. The patient described here ultimately had a hemodynamic configuration that is similar to a DRIL procedure after the ligation of the radial artery between the anastomosis of the AVF and aberrant connection between the radial and ulnar arteries.
Conclusion
Symptomatic ISS is an uncommon but significant complication of AVF surgery. Doppler ultrasound is important in the evaluation of the altered hemodynamic patterns associated with an AVF and aids in preoperative planning for correction of ISS in individuals with aberrant anatomy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.