
Abstract
The author of this article considers moral distress theologically, as a potential shattering of core sustaining belief systems, hope, securities, self-identities, and organizing principles of one's existence. Shattering of individual moral expectations can occur in both medical and military moral injury.
Introduction
“Moral injury” as a term began to be used among those who provide pastoral and psychological care for military veterans. It was first used by Jonathan Shay in 1994, then revisited by Bret Litz and his colleagues some 10 years later, as a way of articulating and naming the deleterious moral impact of violence and killing in war on the post-war lives of veterans. Nearly 20 years after Litz et al., the term is now being used to describe difficult experiences, often traumatic in nature, in an ever-broadening range of professions.
The global COVID-19 pandemic has brought about a flurry of research seeking to understand its effect on health care workers (HCWs) beyond that of physical fatigue and exhaustion. Post-traumatic stress disorder (PTSD), adjustment disorder (AD), and moral injury have been named as possible ways of understanding the extensive, lasting, and damaging impact experienced by HCWs (Brunet et al., 2022; Chandrabhatla et al., 2022; Jiang et al., 2020; Karatzias et al., 2020; Norrholm et al., 2021; Shevlin et al., 2020; Van Overmeire, 2020; Zerach & Levi-Belz, 2021). For this reason, research on moral injury experienced by medical professionals now represents the largest body, outside those among veterans. A significant number of researchers use moral injury as a generic term without qualification. Alexander (2020) and Sloane are more circumspect, using “medical moral injury” to distinguish this from military experience. Sloane, in particular, notes that “differentiating kinds of moral injury and the contexts in which they occur matters not just for their diagnosis, but also to effective clinical, moral, and theological responses” (Sloane, 2023, p. 1). Further, Čartolovni et al. (2021) note how the use of moral injury in medical contexts has been criticized for the lack of conceptual clarity in relationship to existing discussions such as burnout and moral distress among HCWs.
This article clarifies “medical moral injury” in relationship to existing research in both military and medical contexts. The experience of medical moral injury is approached from the perspective of military chaplaincy and moral injury research in military contexts. I do this with a proprietorial sense of both caution and discomfort. The naming of veteran experiences since the Vietnam War as “moral injury” brought so much clarity and understanding to struggles veterans faced over and beyond PTSD. This article explores whether a generic, expanded use of the same term might lead to a dilution of its power to name and describe the harm experienced, thus trivializing the deep suffering of veteran experiences and the impact of moral trauma in all its forms (Eikenaar, 2022; Wiinikka-Lydon, 2019).
Unsurprisingly, ready divergences between military and medical experiences of moral injury are sometimes be identified. Even so, from a theological perspective, an unambiguous common thread emerges between the two.
The article consists of two sections. The first discusses the divergences between military and medical moral injury and identifies areas of further research to sharpen the conceptual clarity around moral injury in the medical professions. The experience of moral injury during the COVID-19 pandemic is then examined through Brian Powers’ theological analysis of military moral injury. Moral injury experiences, in both military and medical contexts, will be shown to be born of, and situated in, “the fragile and imperilled human condition” (Powers, 2019, p. 5). This theological common thread will frame strategies for moral repair which go beyond mere cure toward human flourishing.
Divergent Experiences
Divergences Identified
The Contexts of Potentially Morally Injurious Event (PMIE)
In the COVID-19 pandemic, Amsalem et al. explain how HCWs continually faced the deaths of their patients. They argue that this—combined with the lack of resources such as ventilators, personal protection equipment (PPE), guidance, and training—formed a context for their trauma. These experiences of trauma in turn led to personal senses of helplessness, anger, shame, guilt, and mistrust, further manifested in depression, suicidal ideation, and drug and alcohol misuse (Amsalem et al., 2021). In military contexts, however, a PMIE is not in the failure to save life, but in the taking of life, often multiple lives, and perhaps including the killing of civilians, especially women and children (Kudo, 2018; Sites, 2013).
A stark contrast is thus found between the respective contexts for PMIEs among combatants in war, and for HCWs. The circumstances are radically different.
Differing Ethical Frameworks
Military members are formed and trained in an ethical framework built around Just War Theory, the Geneva Convention, and other international laws. 1 These seek to justify, direct, and limit the use of violence and lethal force in the conduct of wars. In a similar way, members of medical professions are immersed in an ethical framework formed around the traditional Hippocratic oath, now expressed in contemporary forms such as the Declaration of Geneva (Australian Medical Association, 2006). This consistent framework seeks to inspire and direct the provision of medical services and initiatives.
The contrast is again stark. The task of the military is to destroy enemy forces and military infrastructure in the most efficient, thorough, and timely manner (Lucas, 2016). For the medical profession, however, destruction is far from the center of practice. Saving lives, helping the sick and most vulnerable, is front and center of medical ethics (Jeffrey, 2020).
Divergences Ignored
Despite such divergences in the respective contexts in which moral injury is claimed, most studies in medical and COVID-19 contexts fail to acknowledge them. For example, the measuring instruments of moral injury in military contexts are used as assessment tools in medical contexts with minor amendments. The examples below illustrate the lack of awareness of the original design intentions of the instruments, and how the same words may take on different meanings out of their original contexts. There are indications, too, that the modifications fail to understand several significant aspects of veteran moral injury experiences.
Example 1—Moral Injury Symptom Scale Health Professional (MISS-HP)
Mantri et al. modified the short form of the military version of Moral Injury Symptom Scale (MISS-M-SF) “to provide a reliable and valid measure for identifying MI among HCWs for use in healthcare settings” (Mantri et al., 2020, p. 2324). They named this MISS-HP. See Table A1.
According to its original designers, MISS-M, both in its long form (45 items) and short form (10 items), specifically assesses moral injury symptoms, based on the dynamics of the injury, as understood in military contexts (Koenig et al., 2018). Thus MISS-M locates PMIEs squarely in the military, and more specifically in combat. Koenig et al. (2018) therefore list examples of PMIE as involving:
Killing Violence to others Witnessing violence Not protecting Morally compromised position Witnessing others, especially leaders, violate moral codes. De-humanizing others (enemy) Plundering others (dead or alive) Rape, torture (victim or perpetrator).
2
Item 1 (MISS-M-SF) asks a specific question about betrayal by a leader, “those who hold legitimate authority.” Item 1 (MISS-HP) turns this into a different question about betrayal by others, which corresponds to Item 8 in the long version, MISS-M-LF. Item 5 (MISS-M-SF) seeks to measure the loss of trust “as it interferes with their [combatants’] ability to maintain family relationships and friendship networks.” It is not about the trustworthiness of professional colleagues, as implied by the corresponding item in MISS-HP. Item 6 (MISS-M-SF) assesses “loss of meaning” in sufferers’ lives. It is a “meaning of life” question, not a question about “making life meaningful as a health professional.” Item 8 (MISS-HP) is the most unfortunate example in this regard. MISS-HP changes the original wording of the military version, “All in all, I am inclined to feel that I am a failure” to “All in all, I am inclined to feel that I’m a failure in my work as a health professional.” The item is not about a mere sense of failure as a professional, but as a human person. Sufferers typically see themselves to be “monsters” and no longer human (Shibaoka, 2023, p. 231).
Every “symptom” measured by MISS-M is a direct consequence of killing and violence, yet discussions on moral injury in medical context fail to recognize this. In the medical context, death and dying, may be present in the failure to save life: medical professionals do not routinely aim to perpetrate violent acts or killing. Mere modifications to wording make nonsense of measuring instruments such as MISS-M without carefully addressing and exploring the divergences in PMIEs in military and medical contexts. Most MISS-HP modifications are problematical from this point of view, but some are more concerning than others.
Example 2—Moral Injury Event Scale (MIES)
Amsalem et al. (2021) as well as Chandrabhatla et al. (2022) use a modified 9-item Moral Injury Event Scale (MIES) to assess moral injury among HCWs. Unlike MISS, MIES includes references to the location of PMIE in the wording, but modifications are again, minimal, and much of the texts are unchanged—see Table A2. These authors also appear not to realize how the same questions, asked in different contexts, may convey completely different meanings.
Item 2 remains the same: “I am troubled by having witnessed others’ immoral acts.” This, in military contexts, refers to acts of violence such as shooting unarmed civilians in the back, torturing and rape of prisoners of war, planting weapons as false evidence, and the like (Phillips, 2018; Rios, 2018; Sherman, 2010). The same question in medical environments is most unlikely to draw responses from inside the experiences of intentional violence and killing, but from being troubled through failure to save life. Item 6, “I am troubled because I violated my morals by failing to do something I felt I should have done,” in a military context might mean having left behind their dead or dying comrades, or having become complicit in covering up war crimes (Sites, 2013). Again, it is difficult to see parallel situations involving intentional acts of harm in medical contexts. He warned against the comparison of even rare moments in medical practice as being akin to battle because the connections between the two so quickly break down under scrutiny—for instance, willingness to kill or be killed is never expected of health care providers. (Alexander, 2020, p. 83)
In moving from one context to another, the same questions become transposed as questions of a fundamentally different order. As Alexander, drawing on Asken writes:
Eliding the Divergences—A “Hegemony of Symptoms”
It is surprising, from the perspective of military moral injury research, that the exploration of moral injury in the medical profession appears to lack awareness of these radical differences in the location of original trauma.
Warren Kinghorn (2020) may provide an explanation. He argues that moral injury, as with PTSD, is increasingly subjected to a “hegemony of symptoms” whereby symptoms are disengaged from their original traumatic context. 4 The “moral injury symptom set” becomes identified as the moral injury itself, and the pathologized foci of individual therapeutic interventions. In this process, the PMIE and the nature and the context of the originating trauma become minimized and neglected. This is understandable from the perspective of clinicians who are confronted day after day by human distress and suffering. Nevertheless, it is important to hold closely together both the specific traumatic context and the experience of moral injury, in order to effectively address the suffering not merely in the present, but also into the future. 5
In the COVID-19 pandemic, it seems that a set of symptoms—of helplessness, anger, shame, guilt, and mistrust are observed, together with depression, suicidal ideation, and perhaps drug and alcohol misuse—is identified as moral injury. The original trauma context recedes, disappears into the background. This is also observed by Sloane (2023) and Čartolovni et al. (2021) as failure to deal with the “moral” aspect of moral injury in most of the literature. Catchphrases such as “deeply held beliefs” and “moral compass” are used without much content, meaning, or significance, to satisfy the definition of moral injury (Čartolovni et al., 2021).
The problem is the hegemony of symptoms; worse, the hegemony of “generalized” symptoms, as well as morality. Alexander asks: [I]s it enough to say that exhausted physicians should be able to share the label with disoriented veterans because some of their least complex common features [of distress] overlap, and because these features bear some connections with a moral transgression? (Alexander, 2020, p. 85)
Reclaiming the Divergences
The impact of the hegemony of symptoms goes beyond the distortion of measuring instruments: the symptoms become the focus of investigation. Attention is taken away from the links between the specific PMIEs and their discrete symptoms, and thus away from the actual construct of moral injury in medical environments. This is fatal to proper analysis. Divergences between military and medical contexts must be acknowledged. Three existing studies, indicative of divergences that can be built on, are noted below, so as to refine and tailor therapeutic strategies for specific and individual PMIE, as well as moral repair.
Moral Injury-Self and Moral Injury-Others
At least two different experiences of moral injury have been identified in military context. Stein et al. (2012, p. 799) hypothesized that “there are multiple types of traumata in the military context, each with unique peri-event and post-event response patterns.” These findings, incorporated into adaptive exposure therapy in military contexts, support discrete modifications to address different patterns of posttraumatic sequels. For example, while “moral injury by self” requires attention to feelings of guilt and shame, those who live with betrayal-based “moral injury by others” need strategies to prevent them from revenge-taking, and to deal with their moral emotion of anger (Litz et al., 2016, pp. 2, 89, 118, 122). Further, the identification of specific types of trauma encountered in medical contexts, and their unique posttraumatic sequels involved, will assist in the reclaiming of the divergences.
Type I and Type II Trauma-Network Analysis
The use of network analysis, a relatively new tool in this field of study, appears promising. Stefanovic et al. (2022) identified significant differences in PTSD-symptom networks in survivors of type I trauma (single event; sudden and unexpected high-level threat), as against type II (repeated and/or protracted; anticipated) trauma. Given the close relationship between PTSD and moral injury, such analysis may see new patterns of correlation identified between trauma types and symptom networks of moral injury among HCWs, beyond a generalized list of guilty feelings, shame, powerlessness, and anger. Work by Levi-Belz, Greene, and Zerach (2020) using network analysis on PTSD and moral injury among Israeli veterans, has shown promising results. 6 Similar work in medical contexts may identify differences in the cluster of symptoms and experiences for HCWs to those prevalent among veterans.
Burnout—A Point of Differentiation
Multiple studies, including Zerach and Levi-Belz (2021), find associations between medical moral injury and burnout. Epstein and Delgado (2010) see burnout as a consequence of moral residue, an experience related to moral injury; Chandrabhatla et al. (2022), see burnout, having a unique role in predicting moral injury in COVID-19; and Jeffery (2020), in fact, identifies burnout with moral injury. Čartolovni et al. (2021, p. 592) describe how Dean and his colleagues differentiate between burnout and moral injury “by arguing that in burnout, the root of the problem lies in the broken individual who lacks resilience … in the case of moral injury, the root of problem is in the broken system that, using a reductionist business model, has prioritised profit over healing.”
In contrast, the discussion of military moral injury is devoid of any mention of burnout, except by physicians treating family members (Balmer et al., 2021). As a point of differentiation between the two moral injury experiences, this is a further area of possible investigation into the medical moral injury construct.
In sum, it is suggested that reclaiming the lost awareness of divergences, and exploring links between cause (PMIE) and effect (symptoms), are expected to yield vital insights that will sharpen the conceptual clarity of moral injury among HCWs. This will also assist in designing culturally appropriate instruments to assess both the nature and the extent of moral injury among HCWs (Maguen & Griffin, 2022). This outcome will further translate into more refined, agile, and nuanced therapeutic strategies for moral repair for members of both professions.
Divergent Experiences—Conclusion
This first section explored radical differences between moral injury in military contexts, responding to violence and killing, and in medical contexts of caring and healing. Typically, these divergences came to be minimized and elided: clinicians came to focus on the immediate alleviation of symptoms, the confronting of suffering and pain. They came to see moral injury, not as a PMIE intimately coupled with attendant traumatic responses, but as a mere set of symptoms. The impact of this “hegemony of symptoms” was illustrated by assessing the ways that tools of military moral injury are deployed into medical context, oblivious to their radically divergent cultures and situations. Reclamation of the elided divergences, however, is key to a sharper conceptual clarity for moral injury in medical contexts, especially in the wake of the COVID-19 pandemic.
Theological Exploration
The experience of moral injury in the COVID-19 pandemic is now examined through Brian Powers’ theological analysis of military moral injury. This is followed by reflection on how Augustine's understanding of the human condition of sin offers cogent analysis of experiences of moral injury in the COVID-19 pandemic.
Military Moral Injury
Brian Powers, a former USAF officer with personal exposure to moral injury, explored the interactions between significant aspects of moral injury and the challenges faced by many who live with it, placing Augustine's concept of sin alongside the lived experience of moral injury. Alluding to the key biblical passages, Genesis 3 and Romans 5:12–19, he writes, What precedes Adam's physical act of disobedience is the true moment in which evil enters humanity: the turning of Adam's perception of the ultimate good, and thus of his will, from God, the source of all true goodness, to himself… It is not… that the will has turned towards something that is evil, but that it turned to itself and therefore, instead of desiring the ultimate good, which is God, it desires what is inferior—its own gratification. (Powers, 2019, p. 19) Augustine argued that as personal agents, our willing follows that which we desire—the problem is that our desires are externally and internally distorted and our willing thus follows goods that are twisted and false. (Powers, 2017, p. 325) is more than simply a betrayal or transgression of our most deeply held values… Moral injury… may be best understood as the commitment of one's active willing in service of a powerful and compelling moral orientation that is understood at some point to be false; this is most evident in the fact that it does not engender psychiatric well-being. In their connection with a memory that continues to poison a person's sense of boundaries and relationality, feelings of guilt, shame, moral anguish, or ambiguity—all serve as markers of moral injury. (Powers, 2019, p. 157)
Medical Moral Injury
Could the experience of the COVID-19 pandemic be framed in a similar way for HCWs? Consider this draft position: Having been persuaded, formed and moulded by the powerful and compelling moral orientation framed around the Hippocratic oath, and having come face to face with war-like experience of COVID-19 pandemic, some members of medical profession come to realise that they have served a moral orientation which they now see as false.
It is important to note that much of what Williamson, Amsalem, and others raise as “causes” of moral injury in COVID-19 existed prior to the pandemic. The same shortage of resources, training, and leadership, were already visible as nexuses of moral frustration and moral distress (British Medical Association [BMA], 2021, fn.10). Some can be seen as institutional and policy issues; others are highly personal in nature. The theological understanding of sin as the turning away from the true good, and the pursuit of what is penultimate, has explanatory power over much of the complex experiences of moral frustration and distress in pre-pandemic medical contexts. 7
Two connected elements contribute to the experiences of moral frustrations, distress and injury among HCWs can be seen as located in sin, just as violence and killing in military moral injury are likewise located. First, the effect of turning away from God to self becomes particularly evident in the limitations of biomedical perspectives. Biomedical knowledge alone is unable to comprehend the what, who, and why of a human person—issues of anthropology and teleology. Second, the dynamic and distorting impact of sin, both internally and externally, becomes evident in human desires that seek after penultimate goods, and how these dictate human wills and actions. This drives oft-experienced, intractable, and compounding problems and conflicts among competing priorities in medical policies and institutions, which lead to experiences of moral frustration and distress.
The What, Who, and Why of a Human Person
A series of questions explicates the distinctive ways in which moral injury may possibly be understood in medical rather than military contexts.
Cure Apart From Healing—Fragmenting Human Persons?
Willis (2000, p. 357) notes that “cure focuses like a laser-beam on a body part: set a bone, excise a tumour, eradicate cancer cells.” Healing, he argues, is “broader, deeper, bigger” than mere absence of disease. Healing approximates “wellbeing, feeling whole—personally, physically, spiritually, mentally socially whole,” while “cure is concerned with a part.” When medicine is practiced merely as a biomedical process, cure becomes detached from healing. Healing a human person involves addressing more than biomedical malfunctioning. The evident impact of sin here is a human person divided into parts, with one part the sole focus at the expense of others.
Groenhout (2006, p. 143) likewise notes how “healthcare has a built-in tendency to adopt a triumphal attitude towards illness, as though medicine could cure every human ill,” the point also made by (Berger, 2002) from Judaic perspective. When human persons are reduced to biological existence, with the focus on the mere elimination of biomedical “disease,” the “good” of healing the whole person is replaced by the lesser “penultimate good” of mere cure—proclaimed, even so, as a triumph. Further, physicians may lose the sight of “illness” that can only be “understood in a particular social context” (Norris, 2009, p. 23). The disease may be treated, but not the illness. Human existence is then seen as fragmented, not just within the person, but also cleaved from their broader community.
Death: Good, Untimely, and/or Unnecessary?
With such a focus on cure, continued biological existence, just staying alive, can in medicine become the sole measure of all that is good, regarded as of ultimate value. The perception of the ultimate good is lost: having turned away from God, human life is all that is left of value. From a theological perspective, human life has immense value, the killing of Abel by Cain attests (Genesis 4:1–16). What marked that killing by Cain was not the ending of life as such, however, but the manner, and the untimeliness, of that death. Human beings, created mortal, may thus see death itself as a natural part of good creation (Groenhout, 2006).
Just as not all biomedical diseases can be cured, every biological life comes to an end, irrespective of medical interventions. When approached with the moral expectation of medical triumphalism, failure to save lives can be experienced as moral trauma. Such failures were commonly experienced during the COVID-19 pandemic, especially given the lack of key resources. Indeed, all deaths in the context of the pandemic might be seen as “untimely”: a nuanced understanding of death is what is needed.
Suffering and Pain—Redemptive and Transformative or Meaningless and Unnecessary?
If biomedicine sees death as failure, Norris argues that it also sees that all pain and suffering must be avoided. 8 If pain cannot be seen as redemptive or formative, meaningful and meaningless pain and suffering cannot be distinguished. This has direct relevance to responding to moral injury. Clinical medicine may seek to remove all pain, and the difficult symptoms of moral injury, yet in doing so, they may also take away the very tools that can be useful for moral repair for those who live with the experience. 9
In sum, the above questions highlight troubling outcomes in medicine of the human condition of sin, the turning away from true good, God, to self. The limitations involved can be seen as factors contributing toward experiences of moral frustrations and distress, even before the pandemic.
The Dynamic and Distorting Impact of Sin
The ongoing impact of sin is that these limitations become amplified, multiplied, and compounded. The sinfulness of sin is such that, having lost sight of the true good, human desires continue to be externally and internally distorted in the willful pursuit of goods that are false and twisted. In this understanding, what is pursued as good is actually false; and the ways by which it is pursued are twisted; and that both conditions have their root (origo) in “original sin.” This understanding is drawn on to explicate the moral frustrations and distress experienced by HCWs.
Long before the pandemic, medical professionals knew dissonance with priorities and policies in the system in which they worked. A theological perspective observes that the choices were not necessarily between distinct “right” and “wrong” policies, priorities, and ideals, but between penultimate goods (Shibaoka, 2023, pp. 100–101). Some found that what others claimed to be “good,” were not good enough for them, so that penultimate goods come to vie against each other, even to gain dominance. HCWs are taken up into these conflicts. How they are pursued is also under the power of sin, and thus twisted. Consequently, moral expectations (even though penultimate) are not met, resulting in moral frustration and distress. For example, many in medicine have been sharply critical of priorities given to efficiency measures. As Willis (2000, p. 356) notes, “health care has become a business or industry, treatments of a particular disease has become a product line, and hospitals become cost centers.” The British Medical Association [BMA] survey (2021, p. 5) stated: Years of underfunding, increasing layers of bureaucracy, and less autonomy for doctors contribute to a myriad of problems. As well as the impact on the wellbeing of the doctors, (such as burnout), many physicians report being forced to make suboptimal decisions for patients based on institutional constraints.
Moreover, it is not only physicians who find themselves navigating sin's dynamics. Patients too, enter the healthcare system from “a world marked by its history of socially entrenched sinfulness, a world in which bodies often do not function properly, in which people's choices lead to all sorts of misery and malfunctionings” (Groenhout, 2006, p. 143).
Patients’ powerlessness to make health choices that will enhance their own healing, individual “proclivities to do what the individual knows to be completely wrong,” are additional factors leading to moral frustrations experienced by treating HCWs.
The COVID-19 Pandemic—A War-Like Experience
As noted above, HCWs’ experiences in the pandemic were qualitatively different from those of combatants in war, in that they were not involved in acts of violence and killing. Significant moral frustration and distress existed prior to the pandemic, but became profoundly problematical in the crisis. In BMA survey (2021, pp. 9–10), 86.2% of respondents reported moral distress in their (in)ability to provide care during the pandemic; 70.8% experienced distress in relationship to a colleague's (in)ability to provide care. This compares with 59.6% of respondents who experienced moral distress in the 12 months prior to the pandemic. ICU and ED staff were simply unable to employ best-practice and were forced to allow people to suffer respiratory distress and even die from respiratory failure who had good prospect of recovery had they been provided with standard treatment. (Sloane, 2023, p. 15)
Physicians take their Hippocratic oath seriously, but experience how biomedical anthropology and teleology are inadequate in practice to live out that oath. The healthcare system seeks to hold together competing priorities, which further limits their desire to fulfill their oath. In the pandemic, the walls closed in, and choices became so contracted that physicians and other HCWs felt they were unable to care, relieve suffering, and save lives. Whether healthcare system was felt to no longer represent the morality framework of the Hippocratic oath, or they came to regard the oath itself as no longer adequate, it came to be realized that they had willingly placed themselves in a morality framework that was false, in situations of ever diminishing choices. When military members realize they have served a false morality framework, they experience feelings of guilt, shame, and anger (Powers, 2019)—moral emotions now sensed by physicians and other medical professionals.
Such crisis experiences prompted researchers such as Amsalem and Mantri in 2020–2021 to name them as moral injury. If violence and killing were the context of PMIE for military members, crisis experiences during COVID-19 were nevertheless “war-like” for HCWs—with the experience of moral injury born of the human condition, located in sin, for military and medic alike.
Medical moral injury is thus no less a moral injury than military moral injury. HCWs, too, come to understand as false the “powerful and compelling moral orientation,” to which they have “offered their active and willing service.” The impact of their shattered moral orientation is similar, and just as deeply damaging, as their sense of boundaries and rationality, feelings of guilt, shame, moral anguish, and ambiguity: the marks of medical moral injury. 11
The Significance of Theological Insights
Theological perspectives on moral injury in medical contexts offer further insights that point the way to understanding the injury and moving toward moral repair.
The Sinfulness of Sin
Two connected parts of the impact of sin were noted above. The turn toward the self, away from true good, leads to an inadequate anthropology and false telos. Second, the dynamic and distorting impact of sin is evident in the struggles for dominance between divergent penultimate goods. 12
This insight contributes to experiences such as burnout among HCWs, where opinions and problem-solving coalesce around two poles, one around the broken individual, the other around a broken system. At times individuals are blamed—advised to seek help, develop resilience, to self-care; or the system is blamed—policies and institutions are condemned, reforms are demanded. 13 The theological perspective, however, recognizes how both individuals and institutions are located in the human condition of sin: neither can be repaired on its own. As individual HCWs are drawn into penultimate goods vying for dominance over each other, they will be hurt in that very process, and experience moral frustration and distress.
Litz's Continuum
Theological analysis also shows how moral frustration and distress may have become moral injury, the pandemic being the trigger. This affirms the proposal of Litz and Kerig (2019) of a heuristic continuum of morally relevant life experiences, and corresponding responses. In this, a rising level of moral stress is met by a corresponding rise in psychological, social, and spiritual harm and impairment. Moral challenges lead to moral frustration; moral stressors to moral distress; and at the extreme, morally injurious events to moral injury. But where and what is the line that is crossed, as moral distress becomes moral injury? Responding to Zalta and Held (2020), Litz (2020) differentiates moral injury from moral distress, on the extent the event has on individual's functional impairment. Similarly, Čartolovni et al. (2021, p. 597) argue that: [M]oral distress represents a form of situational problem (due to the internal or external constraints), while moral injury represents an experience of the problem that results in a long-lasting change to an individual's sense of lasting hope, trust, integrity and so on.
The significant contribution to this hypothetical continuum from theological analysis is in identifying the elusive transition point from moral distress to moral injury. While moral frustration and distress may lie on a continuum, from this theological perspective, there is a decisive moment at which the compounding, intertwining, and interacting moral frustrations and distress reach a point of shattering individual moral expectations. 14 This in turn implodes the very morality framework within which the expectations themselves were formed. Shattering then, is of a different order of event, from a response to “moral emotions that are very high in magnitude and impact” (Litz & Kerig, 2019, p. 345).
Theological recognition of a common thread for moral injury across the two contexts makes insights into moral repair in the military experience available for medical contexts. In particular, biblical perspectives reveal that moral repair is more than mere biomedical cure, a return to how things were before. It is a journey of new meaning making, one that requires proactive participation.
15
It is not a journey undertaken by individuals alone, but undergirded by God's grace embodied in supportive colleagues, families, and communities (Shibaoka, 2023).
16
Some existing and proven strategies can be adapted for HCWs, including:
Training and education toward moral injury awareness and protective factors prior to a PMIE. Development of moral injury first aid appropriate for HCWs. Recognizing the importance of supportive networks of relationships and communities around those who seek to find new meaning out of their shattered morality framework.
Moral injury is no superficial injury. It bites deep, beyond a professional persona, into the core of self-identity. Survival and growth as a flourishing human person requires an understanding of surviving, beyond limited biomedical perspectives of human persons and purpose.
All Morality Frameworks Are Penultimate
The theological perspective employed identifies all morality frameworks as penultimate: born of, and situated in, the human condition of sin. Having lost sight of the true good, our desires are externally and internally distorted, and our willingness thus follows goods that are twisted and false. Moral repair must therefore involve living with shattered moral expectations and growing new meaning-making even in that difficult place, while also building a better morality framework, yet not a perfect one. Even the new, better framework remains penultimate. Yet the biblical narratives of God's grace point again and again toward posttraumatic growth through characters such as Saul of Tarsus who became Paul the Apostle, and Simon who once denied the Lord but became Peter, the “rock” (Shibaoka, 2023).
Conclusion
This exploration started in a place of personal reticence and discomfort. Might the use of moral injury to describe some of the experiences HCWs in COVID-19, however difficult these may have been, dilute the power of the term for veterans? This article concludes, however, by recognizing that from a theological perspective on the human condition of sin, both medical and military moral injury reflect the shattered moral expectations that tear apart the moral orientation of a person—their core sustaining belief system, hope, securities, self-identities, and organizing principles of their existence. This understanding represents a point of convergence between military and moral injury. 17
Even so, several radical divergences between the two experiences have been illustrated. Deeper investigation of these divergences is urgently needed, to clarify the differences and so sharpen the conceptualization of medical moral injury, leading to more nuanced, agile, and appropriate therapeutic strategies for both experiences. Their common thread also suggests that some parameters identified for veterans’ care may also be applicable for therapeutic strategies for medical moral injury—and perhaps vice versa.
Footnotes
Acknowledgments
My thanks to Dr Charles Sherlock and Dr Andrew Sloane for their ongoing advice, mentoring, and proofreading of the manuscript. I also thank Dr Matthew Beckmann, Research Director, Yarra Theological Union, University of Divinity, for his continued support and guidance. Morling College, Sydney, has provided me with full access to their research facilities, without which I would not have been able to complete this project.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Notes
Appendix
Military and HCWs Versions of MIES Compared.
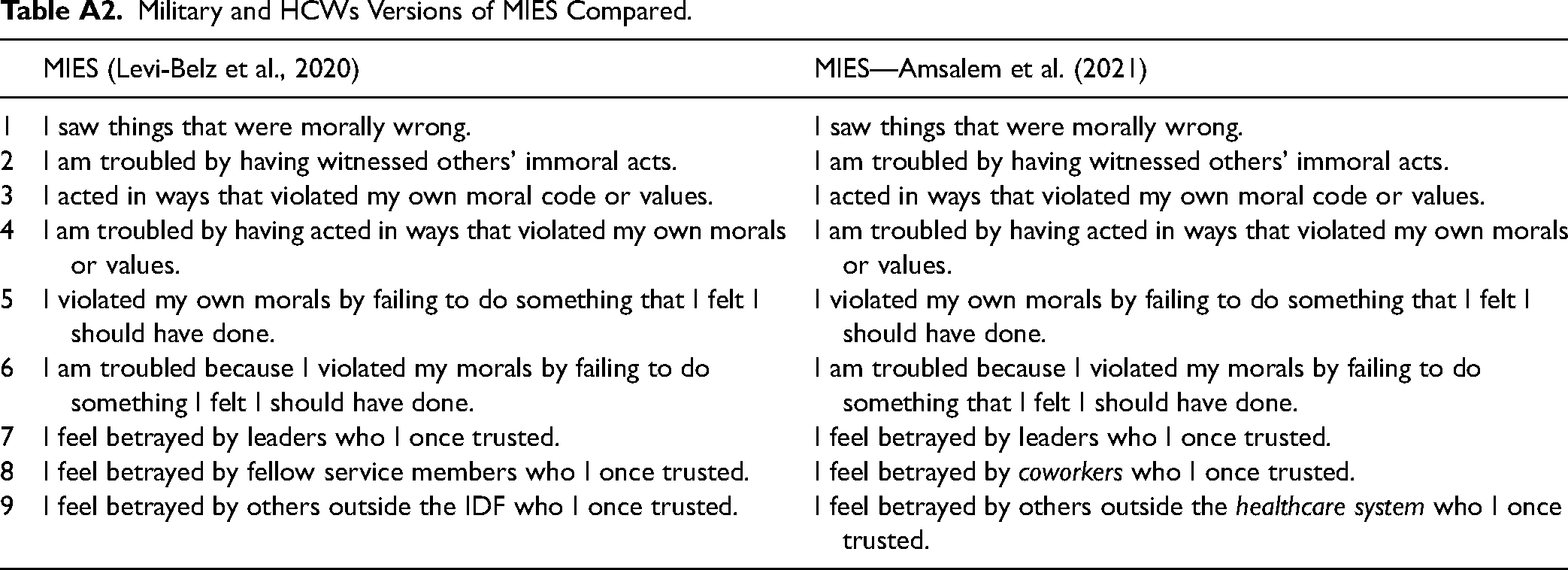
| MIES (Levi-Belz et al., 2020) | MIES—Amsalem et al. (2021) | |
| 1 | I saw things that were morally wrong. | I saw things that were morally wrong. |
| 2 | I am troubled by having witnessed others’ immoral acts. | I am troubled by having witnessed others’ immoral acts. |
| 3 | I acted in ways that violated my own moral code or values. | I acted in ways that violated my own moral code or values. |
| 4 | I am troubled by having acted in ways that violated my own morals or values. | I am troubled by having acted in ways that violated my own morals or values. |
| 5 | I violated my own morals by failing to do something that I felt I should have done. | I violated my own morals by failing to do something that I felt I should have done. |
| 6 | I am troubled because I violated my morals by failing to do something I felt I should have done. | I am troubled because I violated my morals by failing to do something that I felt I should have done. |
| 7 | I feel betrayed by leaders who I once trusted. | I feel betrayed by leaders who I once trusted. |
| 8 | I feel betrayed by fellow service members who I once trusted. | I feel betrayed by coworkers who I once trusted. |
| 9 | I feel betrayed by others outside the IDF who I once trusted. | I feel betrayed by others outside the healthcare system who I once trusted. |