
Abstract
Human and veterinary healthcare workers experience poor mental health, including burnout. However, some argue that burnout cannot fully explain their experiences. Moral distress (MD) and moral injury (MI) are gaining research attention, but there is limited consensus on their definitions and associated symptoms within healthcare. We explored how MD and MI are defined and measured in healthcare using the structure of a scoping review. Next, we conducted an item-by-item analysis to examine the instruments measuring these constructs. Our results revealed that MD focuses on antecedents, while MI emphasizes symptoms. A key gap across these instruments is the absence of a timeframe or a severity scale for distress. We also identified moral mindfulness and sensitivity to morally demanding situations as a potential third element. Finally, the potential overlap between MI and burnout’s emotional exhaustion and cynicism symptoms creates ambiguity in distinguishing whether an individual is experiencing MI, burnout, or both.
Introduction
Human and veterinary healthcare workers (HCWs) are frequently facing poor mental health, with burnout being one of the more prominent outcomes examined (Best et al., 2020; Johnson et al., 2018; Kogan et al., 2020; Lovell and Lee, 2013; Nazarov et al., 2024; Rotenstein et al., 2018). Burnout is commonly described as exhibiting emotional exhaustion, cynicism with reduced efficacy (Maslach and Jackson, 1981). Results from various studies demonstrated a staggering rise in burnout among healthcare workers. For instance, a meta-analysis of 174 studies revealed that 11.23% of nurses reported experiencing burnout (Woo et al., 2020). Similarly, researchers found that the rates of physicians experiencing at least one symptom of burnout increased from 45.5% in 2011 to 54.4% in 2014, suggesting a notable increase year-to-year (Shanafelt et al., 2022). Further, the onset of the COVID-19 pandemic caused serious adverse effects on the mental and occupational health of HCWs, causing an already high rate of burnout to surge among HCWs (Bose et al., 2023; Golu et al., 2022; McKee et al., 2021; Shanafelt et al., 2022; Stodolska et al., 2023; Torrente et al., 2021).
While burnout is commonly seen in healthcare, one question remains: Is it only burnout, or is it something else? This is particularly important since various constructs in healthcare research are sometimes described as precursors that ultimately manifest as burnout, which is then treated as the final outcome and, in practice, serves as an umbrella term (Nagle et al., 2023; Summers, 2020). Using the term too broadly may neglect the root causes and result in a less comprehensive understanding of the presented symptoms, ultimately leading to ineffective treatment (Kok et al., 2023). For healthcare workers, distinguishing burnout from other constructs is particularly important given the complexity of their work, which involves morally taxing situations that challenge decision-making and generate significant emotional distress (Nazarov et al., 2024).
Unsurprisingly, some HCWs argue that they are experiencing symptoms that could more accurately be attributed to moral distress (MD) or moral injury (MI) (Dean et al., 2019; Dean and Talbot, 2018). Unlike burnout, which can have a multifaceted and evolving root cause, MD and MI are constructs that describe psychological responses resulting from morally draining events (Dean et al., 2019; Morley et al., 2019). While the distinction between morality-related constructs and burnout can be challenging, MD and MI uniquely capture the internal dimension of clinicians’ suffering, often marked by value conflicts, perceived betrayals, or participation in actions that violate one’s moral code (Litz et al., 2009; Rushton, 2024).
Research on MD and MI in healthcare has gained popularity in recent years (Rabin et al., 2023). The COVID-19 pandemic led to a large body of work describing how healthcare workers are susceptible to such outcomes (Asadi et al., 2022; Hines et al., 2021; Maunder et al., 2023; Nagle et al., 2023; Rabin et al., 2023; Riedel et al., 2022; Rushton et al., 2022). Authors attribute their occurrence to systemic (e.g. working short-staffed), team-based (e.g. poor management), and individual (e.g. less experienced clinicians) factors, with COVID-19 exacerbating these issues (Dignos et al., 2023; Gohar and Nowrouzi-Kia, 2022; Rabin et al., 2023; Saragosa et al., 2024). However, a consistent challenge in this field is the lack of definitional clarity. Across the literature, MD and MI are conceptualized in varied and sometimes conflicting ways (Epstein and Delgado, 2010; Hanna, 2004; McCarthy and Deady, 2008; Morley et al., 2019; Wilson et al., 2024). For instance, a recent scoping review revealed that MD and MI are, at times, used interchangeably in studies (Wilson et al., 2024). In addition, it has been noted that MD and MI have been used mainly as “umbrella terms,” leading to deficiencies in how they may be conceptualized (Hanna, 2004; McCarthy and Deady, 2008; Morley et al., 2019).
Some researchers differentiated between MD and MI based on the occurrence of stress. Specifically, MD is described as the distress that occurs during the decision-making process, while MI is the psychological response resulting from the impact of the decisions made, which can affect the decision-maker or those witnessing the consequences (Čartolovni et al., 2021). Other researchers addressed a distinction based on ethical and moral codes. For instance, Day et al. (2022) hypothesized that MD results from violations of an ethical code, while MI results from violations of a moral code. However, there are certain situations when HCWs’ moral codes might contradict their ethical codes, which they must respect, leading to MI by avoiding MD (Day et al., 2022). From a severity lens, MD is described as a construct with lesser severity, but more frequently experienced, while MI can have lasting functional impairment (Čartolovni et al., 2021; Reis and Lesandrini, 2025).
While the theoretical distinctions between MD and MI are valuable, they also raise questions about how these constructs should be operationalized. The definitional variability for each construct is substantial, encompassing unclear boundaries between ethical versus moral codes, decision-making versus outcomes, and the symptoms used to characterize psychological distress. This variability complicates comparisons across studies and undermines the development of valid measurement tools. Moreover, the instruments used to assess MD and MI are highly variable, and the validity of their results largely depends on the quality of the instrument in use (Giannetta et al., 2020). Previous reviews have largely been narrative in nature and have not examined the instruments at the item level within the healthcare sector, limiting their ability to provide guidance for research and clinical applications. Our review addresses this gap by coding instruments at the item level and proposing additional concepts to better characterize these constructs. By doing so, we aim to enhance the precision of future research and inform clinical interventions that target morally relevant stressors in healthcare settings. Accordingly, this study had two primary objectives. Our first goal was to explore how MD and MI are assessed in the literature concerning HCWs. Secondly, we analyzed the primary features used to characterize these two constructs based on the available instruments in the literature.
Methods
First, we systematically searched the literature to identify studies that examined MD or MI among human and veterinary HCWs to gain clarity on how the constructs are operationalized. Next, we retrieved studies that measured these constructs psychometrically. Finally, we conducted an item-by-item analysis for each identified instrument to determine the relevant features for each construct.
Systematic search
First, we adopted a scoping review structure to search the literature to capture the necessary studies using MD and MI-related instruments. Specifically, the study followed the reporting standards Scoping Review Extension of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA Sc-R) with updated methodological guidance (Peters et al., 2020; Tricco et al., 2018). Furthermore, we registered this review in the Open Science Framework. The search and selection methods were established through consultations with a library scientist. Literature retrieval was limited to specific databases (PsycINFO, PubMed, PTSDpubs, Web of Science, and CAB Direct). An initial search strategy was developed using broad terms (e.g. “moral injury” OR “moral distress” AND “healthcare”) applied to titles and abstracts (Supplemental File 1). From this preliminary search, we identified a comprehensive list of healthcare professions represented in the literature. Using this list, we conducted iterative, profession-specific searches by combining “moral injury” or “moral distress” with each healthcare profession to ensure comprehensive coverage across disciplines. This list was used in conjunction with specific search terms related to MD and MI and applied to the five databases. All corresponding references were uploaded to the Covidence software, which underwent review following specific screening methods (Veritas Health Innovation, n.d.). Duplicates were removed, and the references were then reviewed for title and abstract. Next, a full-text review was conducted on the remaining references, which yielded the final sample of articles used in the present study.
Inclusion criteria for the title and abstract screening, as well as full-text screening, included manuscript publications in peer-reviewed journals, publication dates between January 1st, 2000 and December 31st, 2022 in English, human or animal healthcare providers, including the terms MD or MI in the title, as the main topic, defined and measured. Exclusion criteria for title and abstract screening, as well as full-text screening, included no abstract in publication, no focus on healthcare providers (no separate data for healthcare providers), a student sample of individuals with no practice autonomy at work, publication types that include opinion, commentary, editorial, letters, responses, and case studies, military samples, and knowledge syntheses (e.g. systematic reviews, scoping reviews, meta-analyses, etc.). Finally, dissertations and conference publications were also omitted.
Initial screening of titles and abstracts was conducted by one reviewer (FS). Next, data screening of full articles was conducted by two independent reviewers (FS & MG-D), yielding a reasonably good inter-rater reliability (k = 0.78). Discrepancies were collaboratively addressed by including the supervising researcher (BG). Four research team members (FS, MG-D, TH, & CS) extracted data from Covidence. Relevant data points extracted from the articles were the definitions of MD and MI, the population studied, and the instrument used to assess MD and MI. Raw data were exported from Covidence, and the finalized data were tabulated and categorized according to the definitions and instruments used. As the focus of this review was primarily to identify studies that measured MD or MI in the healthcare literature, we did not conduct quality or bias risk assessments of the studies.
Instrument analysis
The initial list of instruments for MD and MI was obtained from the systematic search. We contacted the corresponding author when we were unable to retrieve an instrument. All retrieved instruments underwent a preliminary analysis, during which duplicates were removed. Researcher-made instruments were also removed, as they lacked supporting psychometric data. Building on the work of Morley et al. (2019), who postulate that a psychological response succeeds the encounter of a moral event, we analyzed the instruments used to examine MD and MI accordingly. Using deductive and inductive analyses, we conducted an item-by-item analysis, categorizing data as antecedents or symptoms. In this study, we defined an “antecedent” as a factor, event, or situation that may precipitate a psychological, physiological, cognitive, or behavioral response. Notably, its presence alone does not imply that distressing consequences will occur, but it may increase their likelihood. We defined a “symptom” as any psychological, physiological, cognitive, or behavioral response or outcome that arises as a consequence of an antecedent. A third category, labeled “other,” was used when an item did not clearly fit into either of the previous categories. Inter-rater reliability between the two coders (TH & JN) in this stage was adequate (k = 0.77) for all three categories. Disagreements were discussed as a team with the supervising researcher (BG) until a consensus was reached. Despite the deductive approach to categorization, we scrutinized each item to extract relevant information, capturing the necessary details beyond simply selecting a single category
For both constructs, items categorized as symptoms underwent further analyses. Using an inductive, iterative approach, each item was subjected to latent content coding (Drisko and Maschi, 2015) and subsequently grouped to best represent the underlying symptomatology. Particular attention was given to the precise wording of each item to ensure its conceptual meaning was accurately interpreted. Similarly, items in the “other” category were further reviewed and then inductively recoded using a combination of semantic and latent coding to capture recurring themes. To promote rigorous discussion and shared understanding, the two coders and the supervising author (a clinical psychologist) collaboratively examined and classified each item for the “symptoms” and “other” categories. See Figure 1 for the study’s methodological overview.
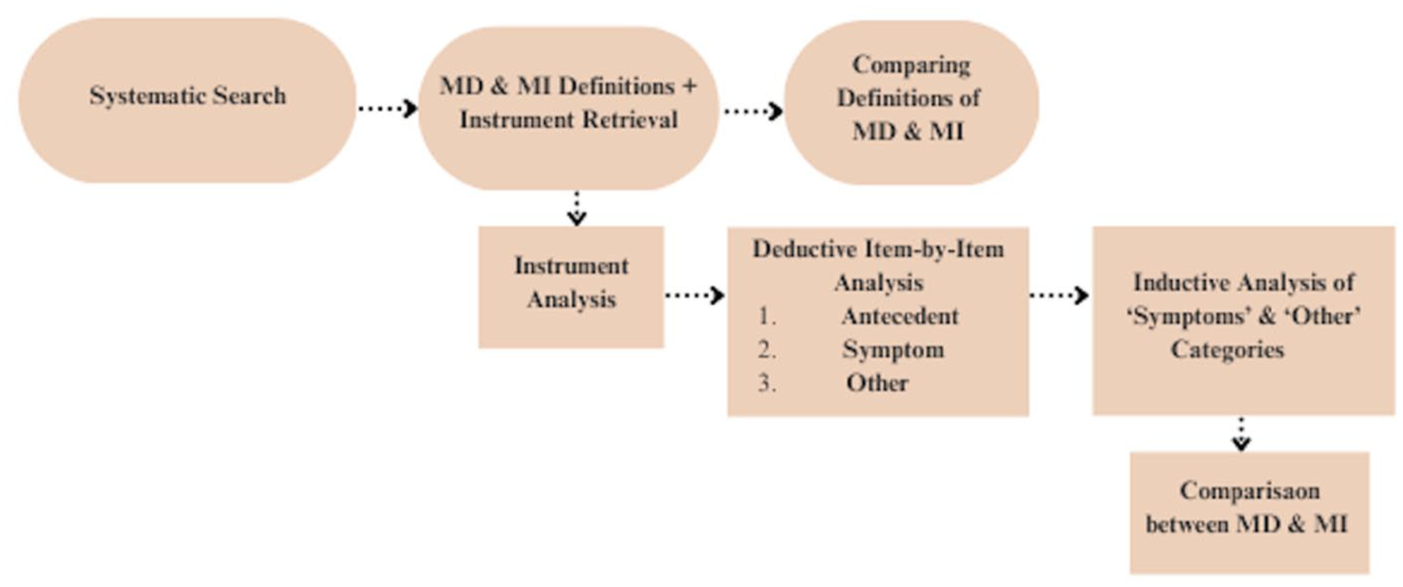
Overview of the study’s methods.
Results
Search results
An initial search yielded 19,462 studies from all databases (Figure 2). Upon removing duplicates, 2929 articles underwent title and abstract screening, whereas 2434 were omitted, and 47 studies could not be retrieved. The remaining studies (448) underwent full-text review, where 274 studies met the study’s criteria. Almost all (99%; n = 271) of the studies examined human HCWs, most of whom were nurses (64%; n = 175). Three studies examined veterinary HCWs. Most studies addressed MD (Table 1) as the construct of interest (89%; n = 245), with the remaining studies addressing MI (11%, n = 29; Table 1). Nearly half of the MD studies (Jameton, 1984, 2013) definitions (n = 117) and Litz’s definition (Litz et al., 2009) were the most common for MI (69%; n = 20).
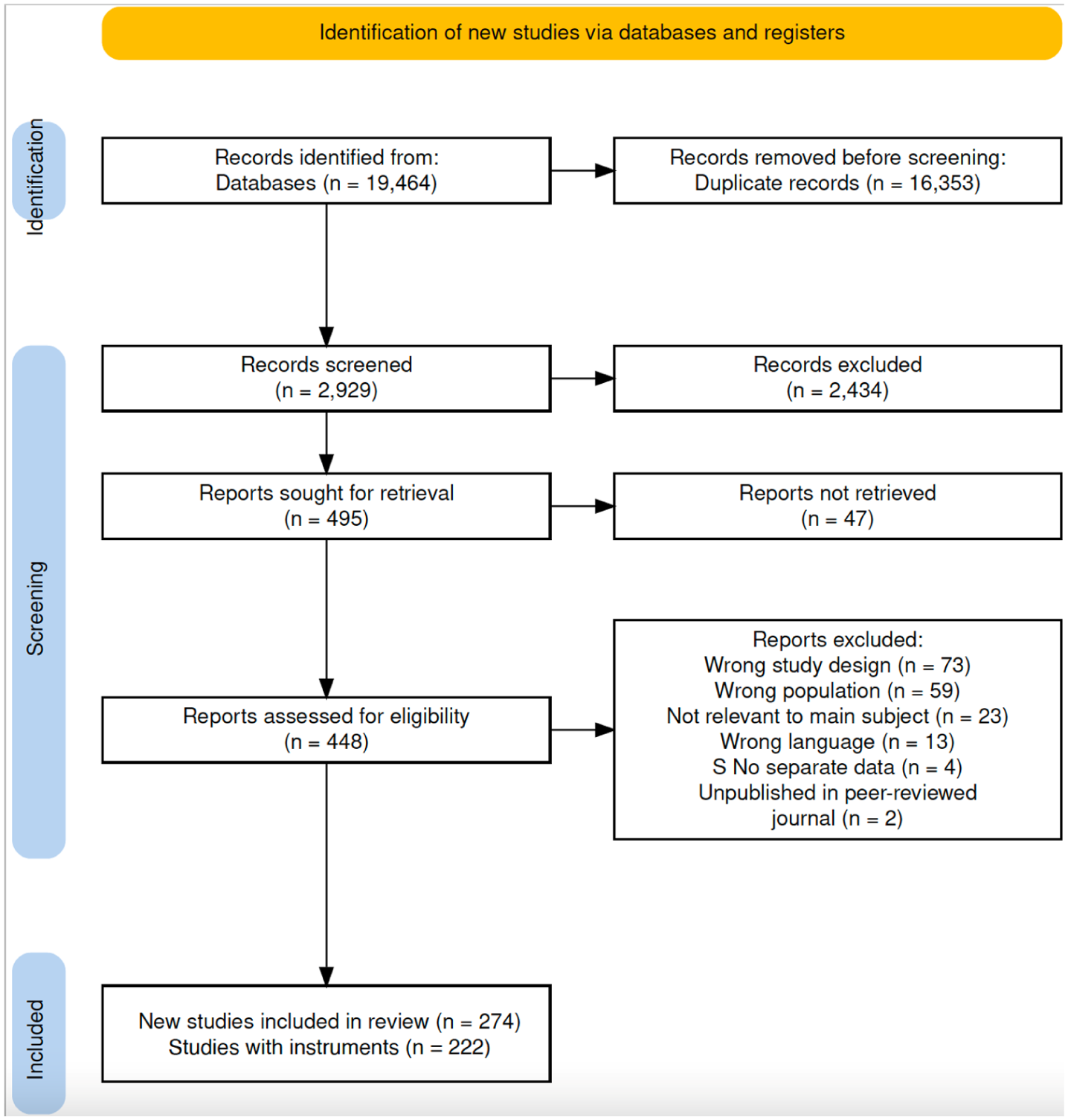
PRISMA chart for review search.
Search results for MD and MI, including study design, geography, definitions and how they were measured.
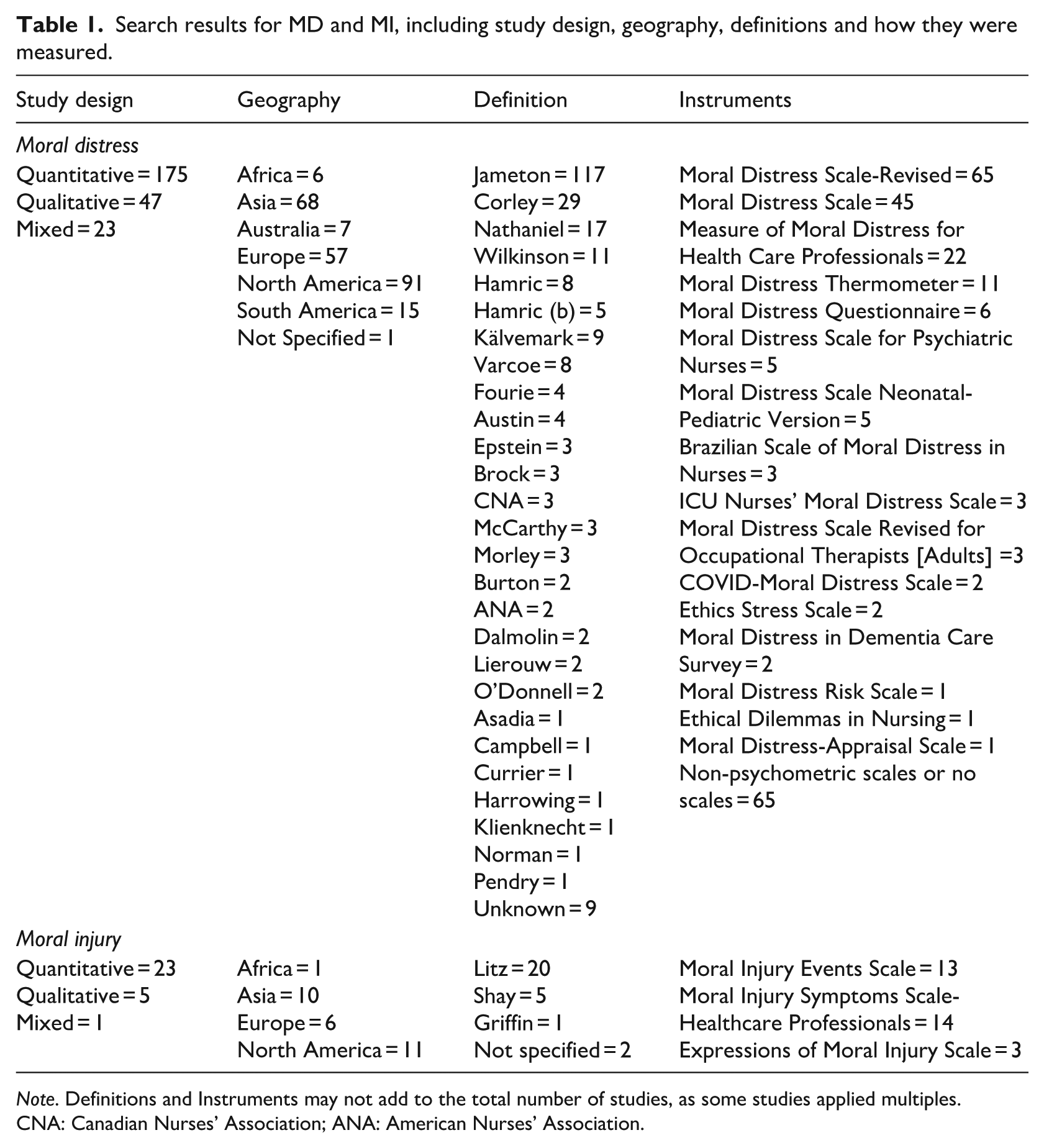
Note. Definitions and Instruments may not add to the total number of studies, as some studies applied multiples.
CNA: Canadian Nurses’ Association; ANA: American Nurses’ Association.
Most studies employed quantitative or mixed method designs, using an instrument to assess MD or MI (81.0%, n = 222). Data gathered identified 18 instruments used to assess MD (n = 15) and MI (n = 3). Initially, we could not retrieve two scales: (1) the ICU Moral Distress Scale and (2) the Ethical Dilemmas in Nursing. After contacting the corresponding authors, we successfully obtained the former scale. The most used instrument for MD was Corley’s Moral Distress Scale-Revised (MDS-R; 23.9%, n = 65). However, considering all the modified versions of Corley’s original MDS (MDS-R, IMDS, COVID-MDS, MDS-P, MDS-R-OT[A] and MDSNPV), these scales accounted for two-thirds (n = 131) of the instruments used in the 198 quantitative studies examining MD.
An updated, targeted search for MD and MI scales was conducted in PubMed with date restrictions (January 2023–November 2024). PubMed was selected based on its frequency and relevance of results compared to the other databases. This update was intended specifically to capture any additional measures identified during the review stage. The search yielded three studies and identified one additional scale: the Moral Injury Outcome Scale (MIOS). Because the update focused on scale identification and occurred after the systematic search phase, the studies themselves were not included in the review synthesis. Accordingly, a total of 19 instruments were identified (MD = 15; MI = 4).
Instrument analysis
Combining all MD and MI scales, a total of 422 items were assessed. Over 75% (n = 320) of the items among the 19 instruments focused on antecedents, 18% (n = 76) focused on symptoms, and over 6% (n = 26) were initially classified as “other.” MD scales contained 363 items (87%), and MI scales had 59 items (13.9%). Qualitatively, MD items appeared to focus on antecedents or potentially morally distressing situations (e.g. working understaffed), whereas MI items focused mostly on outcomes or consequences (e.g. self-blame), particularly symptoms.
Our analysis revealed that 87% (n = 317) of MD items were antecedent-focused, across 10 scales, totaling 223 items (Table 2). Four scales included some symptom-related items, with two having only one item each. Finally, 13 items were initially labeled as “other” (3.58%). Unlike MD, items from the MI scales focused more on symptoms (n = 43; 72.88%), with only three items (5.08%) classified as antecedents. Over 20% (n = 13) of MI items were initially labeled as “other.” Symptom-related items (n = 76) across all scales were further analyzed. Five key themes emerged: (1) Emotional/Affective Responses, (2) Cognitive/Belief-Related Responses, (3) Behavioral/Avoidant Tendencies, (4) Organizational-Related Factors, and (5) Feelings of Exhaustion and Somatic Responses (Table 3).
Item-by-item analysis of MD and MI scales.
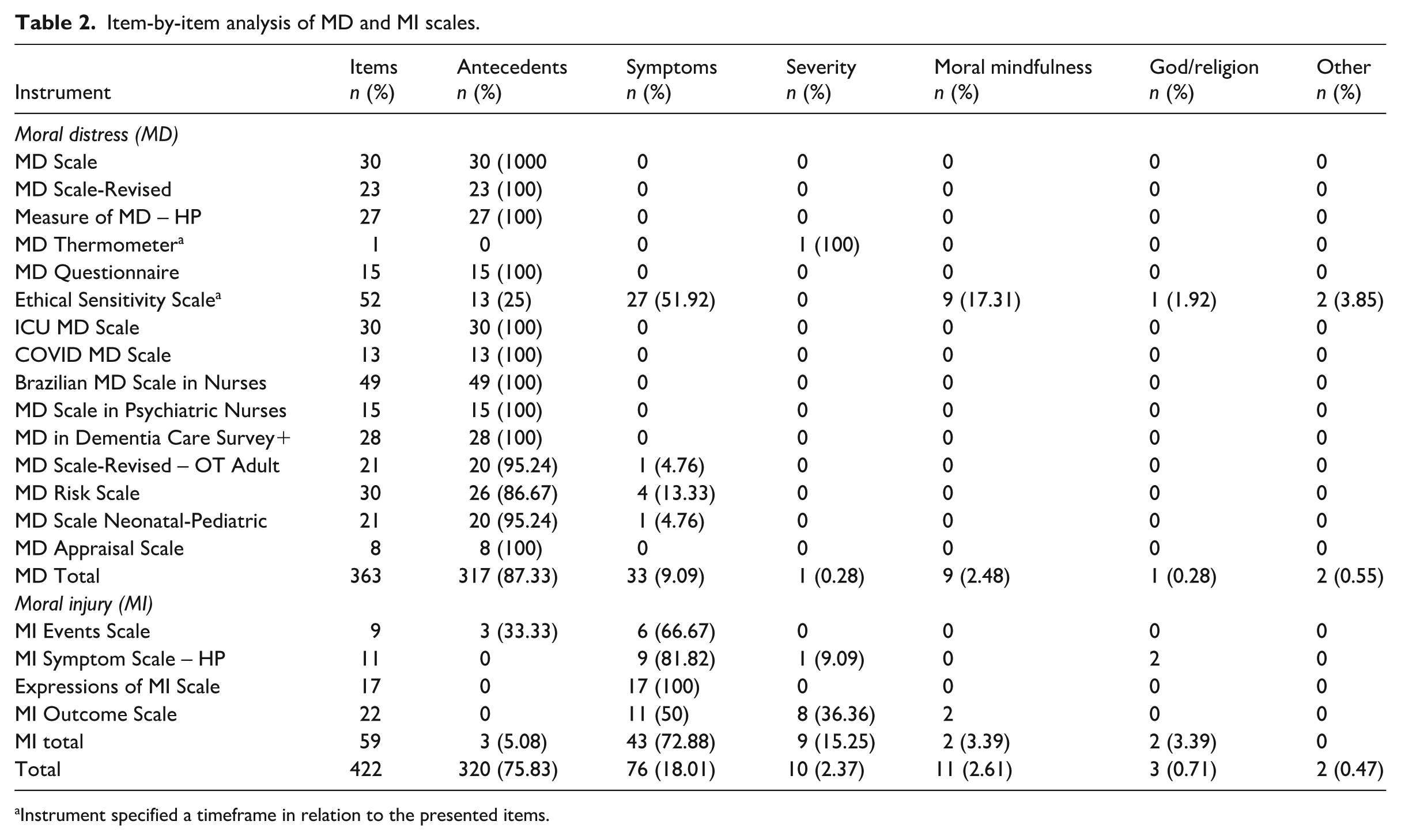
Instrument specified a timeframe in relation to the presented items.
Illustrative, paraphrased examples of items from moral distress and moral injury instruments.
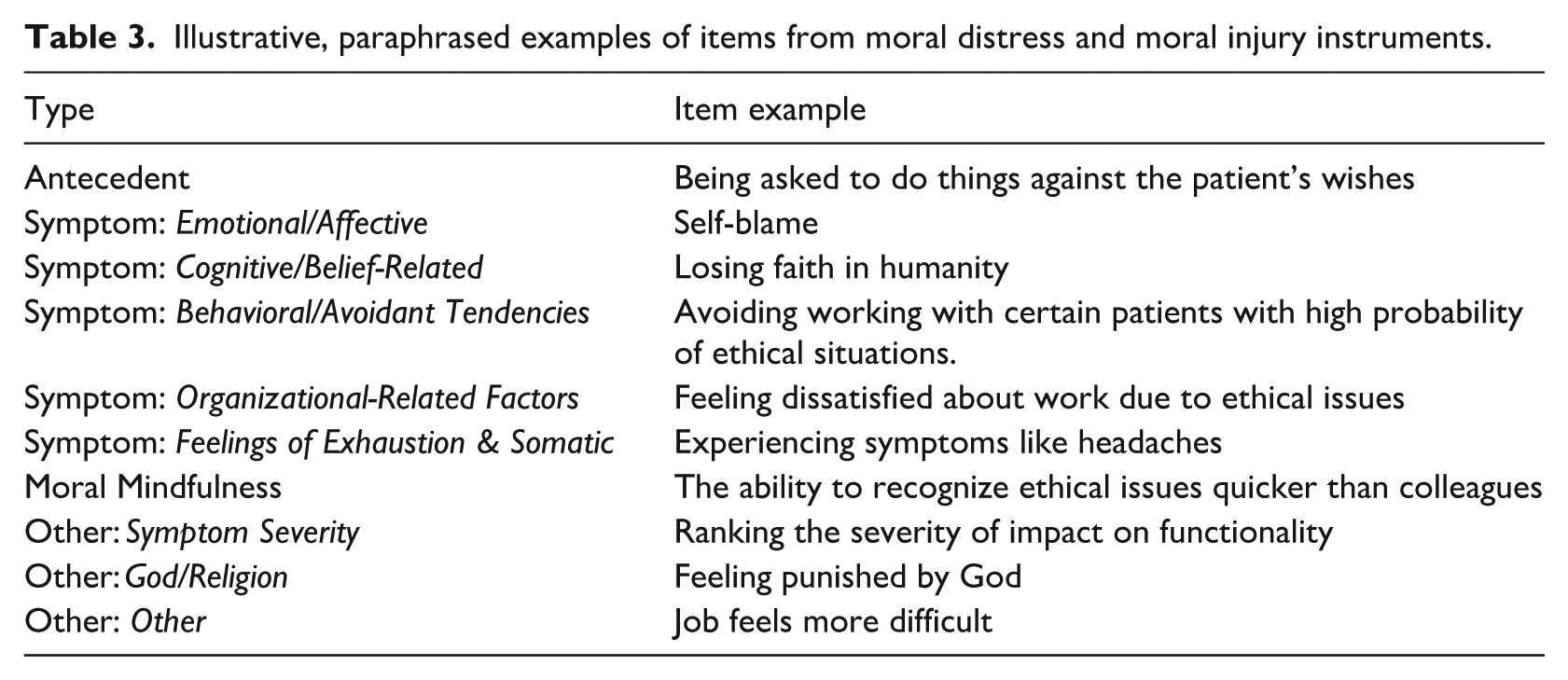
Emotional/Affective Responses (n = 48; 63%) encompassed feelings of anger, betrayal, disgust, guilt, emotional discomfort, sadness, self-condemnation, self-doubt, shame, and worry. Behavioral/Avoidant Tendencies (n = 11; 14.47%) captured avoidant behaviors and intentions to change or leave work. Cognitive/Belief-Related Responses included distrust, pessimism, loss of meaning, perceived potential for harm, and intentions to seek revenge. Organizational-Related Factors (n = 4; 5.26%) reflected work stress, job satisfaction, perceived work support, and a sense of autonomy in the workplace. Finally, Feelings of Exhaustion and Somatic Responses described feelings of fatigue and other bodily symptoms such as headaches.
The “other” category was further analyzed, and the following themes were discovered: (1) moral sensitivity and mindfulness; (2) impact/severity and timeframe of MD or MI; and (3) God/Religious. Two items remained as “other” as they did not fit within any appropriate category (e.g. the workplace is more challenging). Please see Supplemental File 2.
The theme “moral mindfulness and sensitivity” (n = 11) describes one’s awareness of an ethically and morally taxing situation and sensitivity toward it (e.g. the Ability to recognize ethical issues better than other colleagues). Additionally, three scales included items related to the severity or impact of MD or MI (n = 10). One scale, the Moral Distress Thermometer, is a one-item scale used to assess the severity of MD presented as a thermometer. The other two were MI scales (Moral Injury Symptom Scale – Health Professionals = 1; Moral Injury Outcome Scale = 8) that focused on potential functional impairment consequential to MI-related symptoms.
Furthermore, only two instruments, both MD scales, specified a timeframe. These timeframes were worded at the beginning of the scale and were not items. The first, the Moral Distress Thermometer, asked whether one had experienced feelings related to MD in the past 2 weeks, while the Ethical Sensitivity Scale asked about the past year. Interestingly, while the Moral Distress in Dementia Care Survey Instrument items were all antecedent-based, it also asked about the frequency and severity (i.e. impact) of these antecedents. Finally, there were three items related to God and religion, appearing in two MI scales and one MD scale (e.g. feeling punished by God).
Discussion
We conducted a systematic search using the scoping review structure to determine how MD and MI are defined and measured, then retrieved the instruments used to measure these constructs and qualitatively analyzed each item. The study’s results helped distinguish between the constructs and identify key features related to MI.
MD and MI in human versus veterinary healthcare
Surprisingly, only three of the 274 studies retrieved from our scoping review examined MD or MI among veterinary HCWs. Veterinary personnel often face challenging situations such as healthy euthanasia due to financial restraints or individual values (Bartram and Baldwin, 2010; Moses et al., 2018; Platt et al., 2012). Unlike human healthcare, veterinary medicine involves a triadic relationship between the animal patient, the client, and the clinician, wherein the patient cannot make autonomous decisions. This dynamic adds a unique layer of moral complexity, as practitioners must balance their ethical obligations to the animal’s welfare with the owner’s wishes and financial realities. These circumstances have been found to negatively impact veterinary healthcare workers, including an increased risk of suicidality (Bartram and Baldwin, 2010). As such, researchers recommended further investigations, including the development of instrumentation to measure MD and MI within the veterinary profession (Arbe Montoya et al., 2019). Ultimately, it is evident that MD and MI are concepts which are on the rise in both human and veterinary healthcare and have serious adverse effects on the occupational health and mental wellness of HCWs.
MD versus MI
Results from the search review revealed that more research and instruments were used to measure MD than MI among HCWs. Our instrument analysis revealed that MD focuses primarily on the events that may transgress against one’s morality, while MI focuses mainly on the result of experiencing a moral event. These findings align with a recent review that explored MD and MI across various professions (Houle et al., 2024). While certain events increase the risk of developing MD, it is insufficient to focus exclusively on antecedents for three primary reasons. First, morally distressing events may present in numerous ways not identified in the literature or in scales. Thus, the premise of developing scales for each specialization could, to some degree, be unnecessary. As an example, mood or traumatic disorders are not contingent on the characteristics of a profession but are related to universal symptoms and key features that must be present. Second, focusing solely on antecedents without considering a set of symptoms would result in lower diagnostic accuracy and, by extension, poorer treatment outcomes. Finally, focusing on antecedents alone assumes that all individuals will respond similarly in morally distressing events, failing to acknowledge individual differences (Houle et al., 2024). At the same time, some MI scales focused exclusively on symptoms without investigating certain events contributing to the injury. This mismatch among the scales requires further exploration to assess events and symptoms adequately.
Similar to clinical disorders like PTSD, a disorder where MI emerged from, exposure to an event alone does not necessarily lead to a diagnosis. Likewise, experiencing a set of symptoms without the occurrence of a traumatic event could lead to a misdiagnosis. Instead, one must exhibit a set of symptoms for a specified period following a particular event and how these symptoms affect one’s functional ability (American Psychiatric Association, 2022). The lack of measurement of the duration during which HCWs may experience these symptoms, or the severity of their impact, is also a concern. For instance, experiencing guilt briefly during or following a moral event does not necessarily lead to poor mental health outcomes. Conversely, it is problematic to ruminate over a particular event while still experiencing guilt. Thus, determining symptom duration and severity is necessary.
Notably, our analysis suggests that a third dimension is required: mindfulness and sensitivity to ethically and morally complex situations. This aligns with research demonstrating a relationship between MD and moral sensitivity (Lützén and Kvist, 2012; Reynolds and Miller, 2015), where personal traits, values, and prior experiences shape the ability to recognize moral conflicts. Individuals with higher moral sensitivity may detect morally distressing or injurious situations earlier, which could influence the intensity and progression of symptoms they experience. This dimension is particularly relevant for MI, as it captures immediate emotional responses and the longer-term consequences of morally challenging decision-making. Incorporating moral sensitivity into assessments may therefore improve predictive validity and provide a foundation for interventions aimed at fostering reflective, ethically attuned responses among healthcare professionals (Figure 3).
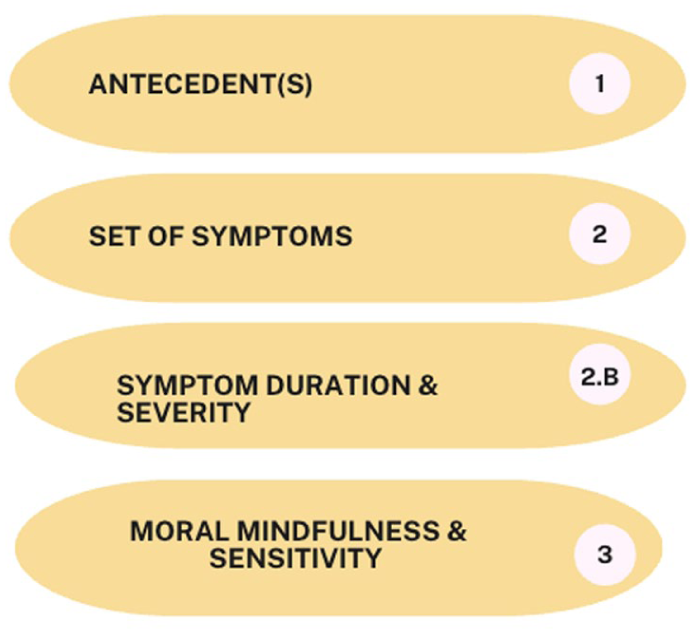
Recommended approach in assessing MI.
MD, MI, and burnout
Overall, most MD scales focused on events that could lead to distress, without specifying symptoms. However, the ones that included symptoms, similar to MI scales, focused on emotional symptoms such as guilt, frustration or anger, loss of meaning and, followed by avoidance and exhaustion. Interestingly, these highly represented categories largely mirror the symptoms of burnout, including the emotional exhaustion and cynicism components of Maslach’s burnout model (Maslach and Jackson, 1981), one of the most used scales to measure burnout. This resemblance may partly explain why some clinicians argue that burnout does not fully explain their symptoms despite some overlapping characteristics (Dean et al., 2019; Dean and Talbot, 2018). As such, it is critical to assess if distinct events occurred before symptom manifestation, and further exploring the symptoms related to morality is critical.
In a longitudinal study among hospital HCWs during the COVID-19 pandemic, the researchers examined the relation between MD, burnout, and intention to leave (Maunder et al., 2023). MD was measured using the MMD-HP (Epstein et al., 2019), an instrument we determined to be 100% antecedent-focused, and burnout was measured using Maslach’s Burnout Inventory (Maslach et al., 1996). Their results revealed that MD predicted two burnout elements, including emotional exhaustion. With emotional exhaustion symptoms mirroring some of the MI symptoms, we question whether HCWs were experiencing MI rather than burnout or both. This is an important consideration as the treatment for burnout and issues related to morality differ.
As noted, our results suggest that moral sensitivity is a potential component of the experience of MI. It is posited that sensitivity is necessary when making complex ethical decisions (Rest, 1982). Overexposure to morally challenging events may lead to feelings of pessimism, such as loss of meaning, and cynicism, a key element of burnout (Maslach and Jackson, 1981). Cynical behavior, such as an inappropriate sense of humor, may contribute to moral erosion, diminishing one’s principles and values (Aultman and Meyers, 2020). Repeated exposure to these events may intensify cynicism as a coping mechanism, ultimately reducing sensitivity to future situations as a form of psychological defense (Aultman and Meyers, 2020; Grissinger, 2017). This relationship could, in part, explain why those with burnout are more likely to engage in unethical and unprofessional behavior (Dyrbye et al., 2010, 2020). It is possible that, in some cases, these behaviors are not solely a manifestation of burnout but reflect underlying moral injury, which can be masked by outward signs of exhaustion or disengagement. Moral sensitivity may therefore serve as a protective factor, helping to preserve ethical awareness and potentially mitigating the progression from morally challenging exposure to burnout or moral injury.
Future direction
Based on our study’s findings, we recommend more research in the veterinary field related to MD and MI, given the unique triadic relationship that veterinary personnel face (Kimera and Mlangwa, 2015). Researchers and clinicians should consider three aspects when seeking to examine morally demanding situations, including (1) a specific antecedent, (2) a set of symptoms consequential to the antecedent with considerations for symptom severity and duration, and (3) moral mindfulness and level of sensitivity to ethically and morally challenging situations. Future research should also further explore the impact of individual belief systems, such as religion and spirituality, on experiences of moral distress and moral injury. Some instruments incorporated references to God or religion as moral reference points, while others did not. Understanding whether and how spirituality shapes one’s interpretation of moral events, and whether individuals who are less spiritual or non-religious experience comparable, greater, or lesser vulnerability to moral distress or moral injury, remains an important direction for future inquiry.
Future measurement tools should be designed with strong sensitivity and specificity to distinguish MD and MI from burnout and related constructs. Although symptoms such as emotional exhaustion and detachment may appear similar, burnout does not capture the moral dimensions that lead to internal conflict. More precise measurement would support targeted interventions that address the moral, rather than purely emotional, aspects of distress. For example, identifying moral transgression or value conflict as key drivers could guide peer-support programs emphasizing moral dialog, ethics consultations focused on moral repair, or resilience training tailored to ethical complexity. Conflating MD or MI with burnout risks obscuring their moral origins and may result in interventions that fail to restore moral integrity. Similar to psychiatry, where overlapping symptoms can lead to misdiagnoses, clear differentiation among burnout, MD, and MI is essential to inform effective organizational and therapeutic responses.
Limitations
As with knowledge syntheses, some limitations need to be noted. First, we only included studies published in English; therefore, there is a risk of language bias, as relevant data from non-English-speaking regions may have been excluded. This limitation is particularly important given the global nature of healthcare, where understandings of MD and MI may vary across cultural and systemic contexts. Second, we omitted studies from the gray literature, including those that were not published in peer-reviewed journals, which could have offered valuable insights. Furthermore, our updated search, conducted in pursuit of additional instruments during the instrument analysis phase, was less comprehensive than the search strategy used for the study search. As such, it is possible that MD and MI-related scales in the healthcare field may not have been retrieved. From an instrument analysis perspective, while we did not conduct a formal validity appraisal of the included instruments, we noted whether each measure had documented evidence of psychometric evaluation (e.g. reliability or validity testing). The aim of this study was to map and describe available instruments rather than to critically assess their measurement properties. Furthermore, from a content analysis perspective, it is important to acknowledge the inherent level of subjectivity when categorizing data; however, we attempted to mitigate this risk by having coders who independently analyzed the items.
Conclusions
Our analysis revealed that MD and MI are lacking in veterinary medicine. Additionally, there is more research and instruments to measure MD than MI. Furthermore, MD appears to focus on antecedents, while MI tends to focus on symptoms. Notably, measuring symptom severity and duration was largely absent from MD and MI tools. Moreover, we suggest that one’s moral mindfulness and sensitivity levels to ethically and morally demanding situations be investigated as part of MD and MI assessments. Finally, MI and burnout’s emotional exhaustion symptoms have some overlap, causing inaccuracies on whether an individual is facing MI, burnout, or both. Future studies should consider these elements when studying MD and MI, and further psychometric research is required to better assess these constructs with consideration to human and veterinary HCWs.
Supplemental Material
sj-pdf-1-hpq-10.1177_13591053251398337 – Supplemental material for Moral distress and moral injury in healthcare: A review and instrument analysis
Supplemental material, sj-pdf-1-hpq-10.1177_13591053251398337 for Moral distress and moral injury in healthcare: A review and instrument analysis by Thomas Habib, Janine Noorloos, Hayden J. R. Woodley, Frances Serrano, Michael Gardiner-Davis, Celine Said, Behdin Nowrouzi-Kia and Basem Gohar in Journal of Health Psychology
Supplemental Material
sj-pdf-2-hpq-10.1177_13591053251398337 – Supplemental material for Moral distress and moral injury in healthcare: A review and instrument analysis
Supplemental material, sj-pdf-2-hpq-10.1177_13591053251398337 for Moral distress and moral injury in healthcare: A review and instrument analysis by Thomas Habib, Janine Noorloos, Hayden J. R. Woodley, Frances Serrano, Michael Gardiner-Davis, Celine Said, Behdin Nowrouzi-Kia and Basem Gohar in Journal of Health Psychology
Footnotes
Ethical considerations
Ethics approval was not required for this review article as no data were collected from participants.
Consent to participate
Consent to participate is not applicable to this review article as no data were collected from participants.
Consent for publication
Consent for publication is not applicable to this review article as no identifiable participant data are included.
Author contributions
T.H., F.S., J.N., B.N-K, H.W., & B.G. were involved in the study’s conceptualization and methodology. T.H., J.N., F.S., M.G-D, C.S., and B.G., were involved in the analysis. T.H. was involved in the original draft, and all authors contributed to the editing and review of the final draft.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Office of the Dean, Ontario Veterinary College, University of Guelph
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Search criteria and instrument analysis data are available.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.