
Abstract
With a focus on the use of narrative approaches, this article is a commentary on decision-making support for people with profound intellectual and multiple disability (PIMD) at the end-of-life. Due to improved health care, people with PIMD are living longer lives than ever before. Therefore, they are increasingly facing decisions relating to end-of-life care and planning. Despite the increased attention that has been given to end-of-life planning, opportunities to have preferences responded to at the end-of-life are more likely afforded to people considered to have cognitive and decision-making capacity. Those supporting people with PIMD to plan for and make decisions about end-of-life care face several challenges. These challenges are rooted in difficulties with communication exchange between people with PIMD and their communication partners, leading to a widely held perception of decision-making incompetence for this population. In response to this challenge, this article draws on empirical research to discuss decision-making support within the context of palliative care and advance care planning, specifically for people with PIMD. It promotes decision-making support as an approach to assist supporters of people with PIMD to allow those people’s expressions of preferences to be acknowledged and acted upon at the end-of-life. The use of narrative is presented and discussed as a tool for enabling this responsiveness, specifically within the context of end-of-life planning.
Keywords
People with profound intellectual and multiple disability (PIMD) have relatively higher incidents of life-threatening medical conditions (e.g., aspirational pneumonia, dysphagia, and respiratory disorders), which have historically resulted in them dying earlier than their family carers. Although it is a positive evolution that people with PIMD are living longer lives, it means that they are now frequently outliving their family carers, resulting in a greater occurrence of them dying with the support of palliative care services (Heslop et al., 2014). This creates a challenge for those providing support within the context of palliative care and end-of-life decision making for people with PIMD, who traditionally have not had access to such services. These challenges are rooted in difficulties with communication exchange between people with PIMD and their communication partners. These difficulties lead to a widely held perception of decision-making incompetence for this population.
This article discusses advance care planning and end-of-life decision-making within the complex support relationships between people with PIMD and those who know, love, and support them. The authors draw on the strengthening paradigm shift created by Article 12 of the Convention on the Rights of Persons with Disabilities (CRPD; United Nations, 2008), establishing a strong legislative and moral base from which to develop mechanisms for supporting autonomy for all citizens, including at the end-of-life. The authors discuss the specific challenges faced by people with PIMD and their supporters in achieving autonomy, particularly within the context of end-of-life care. The authors respond to these challenges by drawing on empirical research to discuss the use of a narrative-based methodology for supporting decision-making within the context of palliative care and advance care planning, specifically for people with PIMD.
Advance Care Planning and End-of-Life Care
A person’s opportunity to express their autonomy at the end of life has been linked to a death that meets the psychological, spiritual, physical, and social needs of the person who is dying (Detering, Hancock, Reade, & Silvester, 2010; Granda-Cameron & Houldin, 2012). Advance care planning is designed to aid people to consider and communicate their future treatment preferences in the context of their own goals and values, including for end-of-life care (Australian Commission on Safety and Quality in Health Care [ACSQHC], 2015; Sudore et al., 2017). With provision to include value statements and treatment preferences to guide decision-makers involved in care, and/or instructional directives that explicitly detail consent and refusal for specific treatments (Advance Care Planning Australia, 2018), advance care plans are designed to honor a person’s preferences and guide substitute and supported decision-makers, particularly at the end-of-life.
Despite the importance of ensuring end-of-life care wishes and preferences are known and communicated, there is widespread reluctance among individuals, family, and health professionals to talk about end-of-life treatment preferences, dying, death, and associated existential concerns (Bloomer et al., 2018; Brazil et al., 2017; George et al., 2016). Even when it is evident that death is inevitable, health professionals report significant challenges in communicating about dying and discussing end-of-life care preferences with patients and others (Bloomer et al., 2018; Bloomer, Lee, & O’Connor, 2011; George et al., 2016). When a person’s capacity to contribute to discussions is questioned, as it may be for people with PIMD, challenges in communication between caregivers, surrogates, and supported decision-makers about care decisions may arise (Bloomer, Digby, Tan, Crawford, & Williams, 2016; Bloomer & Digby, 2012; Quinn, Gur, & Watson, 2018). In the absence of effective communication and when a person’s preferences are not known, end-of-life care may be suboptimal (Bloomer et al., 2019b; Visser et al., 2014), with the dying person likely to receive a more “generic” plan of care. Moreover, when people are given opportunities to discuss their wishes and preferences, the quality of their end-of-life care is enhanced (Detering et al., 2010).
In 2015, the ACSQHC recognized the importance of addressing the provision of end-of-life care in hospitals, correlating with increased empirical focus on end-of-life communication and planning in Australia and internationally (Anderson, Bloch, Armstrong, Stone, & Low, 2019; Turner & Flemming, 2019). Other research has examined the needs and care provision for highly vulnerable groups, such as older people (Bloomer et al., 2018; Bloomer et al., 2019b; Witham & Hockley, 2016) and those from culturally and linguistically diverse backgrounds (Bloomer et al., 2019a; Johnstone, Hutchinson, Redley, & Rawson, 2015). Yet, little attention has been paid to such planning in the lives of people with intellectual disability, including people with PIMD. This is despite the life expectancy of people with intellectual disability increasing similarly to the general population (Coppus, 2013). Where the needs of people with intellectual disability have been considered, the focus is on those with mild intellectual disability, leaving people with PIMD at most risk of not being involved in end-of-life decisions (Bekkema, de Veer, Wagemans, Hertogh, & Francke, 2014; Kirkendall, Linton, & Farris, 2017; Stancliffe, Wiese, & Read, 2017; Voss et al., 2019). Bekkema et al. (2014) reported that while people with severe intellectual disability had their end-of-life preferences taken into account only 2.9% of the time, people with mild or moderate intellectual disability had their preferences taken into account 27.8% of the time. This is despite relatively higher incidence among people with severe intellectual disability of medical conditions (e.g., aspiration pneumonia, respiratory disorders and dysphagia) that require critical decision-making relating to end-of-life care. Only recently has attention been paid to the preferences of people with PIMD within end-of-life planning and decision-making (Watson, Wilson, & Hagiliassis, 2017; Young, Hogg, & Garrard, 2017; Zaal-Schuller, Willems, Ewals, van Goudoever, & de Vos, 2016).
The Creation of a New Paradigm for Supporting Autonomy for People with Disability
The United Nations’ General Assembly adopted the CRPD on December 13, 2006, and it was implemented in May 2008 (United Nations, 2008). The CRPD was the first international human rights treaty to specifically recognize that people with intellectual disability have a right to autonomy. This Convention has served as a catalyst for reconsidering notions of decision-making support for people with intellectual disability, in all aspects of life. Article 12 of the Convention challenges all Nations’ use of substitute decision making. Substitute decision making involves the formal (legal) or informal appointment of a person to make decisions on behalf of another considered to lack decision-making capacity (Watson, 2016a). Decisions made under a substitute decision-making model are generally based on an objective assessment of the “best interests” of the person concerned. Article 12 of the Convention not only challenges the notion of decision-making incapacity, and the use of substitute decision making, but also the notion of best interest, which sits at the core of substitute decision-making practice. Article 12 states, “persons with disabilities enjoy legal capacity on an equal basis with others in all aspects of life” (United Nations, 2008). Legal capacity is the law’s recognition of a person’s right to personhood and agency before the law (Arstein-Kerslake, Watson, Browning, Martinis, & Blanck, 2017). The General Comment on Article 12 issued by the Committee on the Rights of Persons with Disabilities emphasizes the need to move away from guardianship to supported decision making (Committee on the Rights of Persons with Disabilities, 2014). It stresses the importance of supported decision making stating that all nations “shall take appropriate measures to provide access by persons with disabilities to the support they may require in exercising their legal capacity” (United Nations, 2008). Article 12 has “turned the practice of supported decision making into a human rights imperative” (Arstein-Kerslake et al., 2017, p. 1). In 2014, the Australian Law Reform Commission (ALRC, 2014) strongly supporting supported decision-making practice, articulated that a person’s “will, preferences and rights” should be at the heart of laws and legal frameworks, including those regarding supported decision making (p. 11). The ALRC also identified that the “most difficult policy challenges in this area concern those who require the most support,” notably where “a person’s will and preferences are difficult, or impossible to determine,” namely people with PIMD (ALRC, 2014, p. 33).
Realizing Article 12 for People with PIMD
Despite the strength of the paradigm shift brought about by Article 12 of the CRPD, many people with intellectual disability are denied their human right to autonomy. This denial is driven by an assumption that concepts relating to self-determination and autonomy are irrelevant to people with intellectual or cognitive disability, due to perceived limited decision-making capability (Ward & Stewart, 2008; Wehmeyer, 2005). This negative perception of decision-making capability is particularly apparent for people with PIMD.
Although highly heterogeneous, people with PIMD share many life experiences and abilities. They have severe intellectual disability coupled with comorbidities such as motor and sensory impairment making them dependent on others for support in most life areas. People with PIMD generally communicate informally using atypical and idiosyncratic behaviors such as vocalizations, facial expression, gesticulation, shifts in respiration, eye gaze, and touch (Watson, 2016a). Understanding formal communication such as sign, speech, written text, photos, or pictures is challenging for them. Many people with PIMD communicate unintentionally. This means, they appear to communicate without the intention of conveying a message to another person (Bunning, Smith, Kennedy, & Greenham, 2013; Petry & Maes, 2006). Information transfer occurs when communication partners infer meaning from the person’s behaviors. This inference is acknowledged as an ambiguous, subjective, and challenging task (Bradshaw, 2014; Grove, 2007).
These communication challenges have contributed to a historical view that people with PIMD are unable to express their preference in relation to decisions about their lives. Such a view privileges individual cognition, failing to recognize the interdependent nature of the lives of people with PIMD, resulting in the frequent removal of a person’s right to autonomy through guardianship. Guardianship (the legal mechanism by which substitute decision making is implemented) involves the appointment of a guardian to make decisions on behalf of a person with disability, removing their human right to legal capacity. In most jurisdictions, decisions to subject a person to guardianship are based on the results of cognitive assessments provided to assist in determination of legal capacity (Darzins, Molloy, & Strang, 2000). Such tools are structured around the traditional premise that decision-making capability is characterized by a set of individual cognitive abilities (problem solving, memory function, rationality, and language) serving as prerequisites for decision-making capability. These skills are often assessed independent of relational factors such as support from family, friends, and support staff. Due to the arguably narrow nature of these assessments, people with PIMD are likely to be assessed as having no or very limited decision-making capability. The legal response to this assessment is to deny legal capacity and permit a third party (legal guardian) to make decisions on behalf of the concerned person; an outcome that has been labeled as a form of “civil death” (Perlin, 2013).
This exclusion from the freedoms set out in Article 12 of the CRPD mirrors past self-determination movements, such as person-centered practice and self-advocacy, dominated by people with mild, as opposed to more severe, intellectual disability (Watson, 2016a). Some commentators equate the cognitive challenges experienced by PIMD, such as difficulties communicating preference intentionally, understanding information, and engaging in rational behavior, with the view that self-determination and autonomy have no relevance to this population (McMahan, 2002; Singer, 1993). These commentators argue that cognitive traits alone are prerequisites to so-called “full personhood.” Privileging cognition as central to personhood, they relegate people they view as without these traits to nonperson status, claiming it is reasonable to deny them the moral status and human rights of those with fuller cognitive capacity (McMahan, 2002; Singer, 1993).
The contemporary disability community refutes the idea that personhood, or humanness, should depend on an individual’s cognitive ability (Kittay, 2019; Quinn et al., 2018). The emergence of this post-guardianship view is partly due to new insights into how humans actually make decisions. These insights dispute the neoliberal constructions of individualized self-determination, which emphasize individual intellectual “capacity,” and explicitly exclude the role which environmental and social factors make to a person’s decision making. Human beings do not exercise their self-determination individually, but relationally, interdependently, and intersubjectively with others (Bach & Kerzner, 2010). Furthermore, “When self-determination is interpreted strictly to mean ‘doing it yourself,’ there is an obvious problem for people with significant disability, many of whom may have limits to the number and types of activities they can perform independently.” (Wehmeyer, 1998, p. 10).
Article 12 of the CRPD calls for a universal right to autonomy regardless of intellectual impairment, through supported decision-making mechanisms. Article 12 sets a pathway from guardianship and instead places a presumption of autonomy (with support) at its core. To uphold these obligations, there is a clear need for new tools of discovery to support people with PIMD to form and express their preferences, in relation to all life decisions, including those at the end-of-life. Specifically, there is a need for research that describes the decision-making support for people with PIMD, outlines factors that influence this support, and suggests mechanisms to enhance this support. There is a need for a reframing of the way that decision-making capacity is understood for people with PIMD. This includes a move away from the privileging of individual cognition, instead focusing on the level of supports and adjustments needed in order for people with PIMD to exercise decision-making capacity (Quinn, 2010). So, what should these supports and adjustments look like? One characterization of supported decision making goes some way toward answering this question, suggesting that the process of decision-making support should not be defined in terms of individual capacity but, rather, in terms of the quality of support available: The starting point is not a test of capacity, but the presumption that every human being is communicating all the time and that this communication will include preferences. Preferences can be built up into expressions of choice and these into formal decisions. From this perspective, where someone lands on a continuum of capacity is not half as important as the amount and type of support they get to build preferences into choices. (Beamer & Brookes, 2001, p. 4)
Supported Decision Making: A Mechanism for Realizing Autonomy
Attempts to characterize and develop supported decision-making models and frameworks to guide the practice of supported decision making are emerging (Douglas & Bigby, 2018; Shogren, Wehmeyer, Uyanik, & Heidrich, 2017). However, these models are primarily focused on decision-making support for people with mild, as opposed to more severe, cognitive disability, excluding people with PIMD.
Watson (2016a) implemented a supported decision-making approach (Watson & Joseph, 2015) with a sample of five people with PIMD and their 33 supporters. The participants with PIMD were supported through a collaborative process where their will and preferences were identified, interpreted, explored, and documented by a group of people who knew them well. This information was used ultimately to make a variety of decisions, which ranged from what color to paint a room to whether to have a lifesaving medical treatment. Interview, questionnaire, and observation data were collected and analyzed, resulting in the identification of several themes underlying participation in decision making for people with PIMD. Drawing from this research, decision-making support for people with PIMD can be defined as a process of enhancing the decision-making capacity of a person with PIMD through collaborative support from a group of people in that person’s life. A person’s circle of support, comprising a group of key people in the person’s life, who have a good understanding of the person’s life history, preferences, and personal characteristics, is an important ingredient in this process. Within this context, autonomy for a person with PIMD is viewed as a relational construct, best realized in collaboration with those in the person’s life who know him or her well (Watson et al., 2017).
Decision-making support for people with PIMD is characterized in terms of the existence of two distinct, but interdependent roles played by (a) the person with a disability (supported) and (b) the circle of support (supporters) in the decision-making process (Watson, 2016a). The role of the person with a disability in this dynamic is his or her expression of preference, and the role of the supporter is to respond to this expression of preference. Within this dynamic, supporter responsiveness is the component that can change, making the enablement of responsiveness a crucial strategy for supporting decision making relating to end-of-life care for people with PIMD.
Responsiveness: A Key Factor in Decision-Making Support for People with PIMD
Researchers have stressed the important and complex role of supporter responsiveness within the process of self-determination and decision making for people with PIMD (Finlay, Antaki, Walton, & Stribling, 2008; Johnson, Watson, Iacono, Bloomberg, & West, 2012; Watson, 2019). Watson’s (2016a) qualitative study exploring the implementation of a supported decision-making approach with five people with PIMD provided much needed insights into the complex role of communication partners in the decision-making support process. Watson characterized supporters’ role of responsiveness as a multi-faceted activity made up of three tasks. First, supporters acknowledge/notice (as opposed to ignore) expressions of preference of those they support. Second, they interpret these expressions of preference (ideally collaboratively), assigning meaning to them, and finally they assist those they support to act on this meaning. Although each of these tasks is important, none of them characterize responsiveness in isolation. Rather, supporter responsiveness is reliant on the implementation of these tasks collectively (Watson, 2016a).
Acknowledging the importance of responsiveness in the process of decision-making support for people with PIMD, Watson (2016b) identified a range of factors underlying supporter responsiveness that were organized into five overarching themes and 10 subthemes (Watson, 2016b). These overarching factors include (a) the person with PIMD’s communication, (b) supporter attitudes and perceptions, (c) relational closeness between supporter and person with PIMD, (d) functioning and make up of circles of support, and (e) characteristics of the service system. Although each of these themes are important in relation to decision-making support for people with PIMD, the remainder of this article will focus on the role of storytelling (narrative), as a mechanism found to be important in relational closeness and therefore responsiveness within supported decision-making practice for people with PIMD. The authors will explore the application of a narrative approach within the context of decision-making support relating to end-of-life planning and care for people with PIMD.
The Role of Narrative in End-of-Life Decision Making for People with PIMD
Relational closeness is an important factor by which supporters develop a picture of the preferences of those they support (Forster & Iacono, 2008; Watson et al., 2017). A tendency toward greater supporter responsiveness to preference expression has been identified within the context of intimate or very close relationships between supporters and those they are supporting (Watson, 2016a; Watson et al., 2017). Watson et al. (2017) explored the characteristics of relational closeness between a person with PIMD and their communication partners and found that the use of storytelling within interactions between people with PIMD and their supporters was central to relational closeness and therefore supporter responsiveness. The key component of this approach is supporters knowing the history of the person they support, through an exploration of their life story, and through an exploration of their identity beyond the constraints of their disability (Watson, 2016a).
The importance of knowing a person with intellectual disability’s history and personal story through narrative approaches, particularly in relation to understanding their preferences, is increasingly being established in the literature (Gjermestad, 2017; Grove, 2007; Koenig, 2012; Schepens, Van Puyenbroeck, & Maes, 2019; ten Brug, van der Putten, Penne, Maes, & Vlaskamp, 2012; Watson et al., 2017). However, for people with PIMD, opportunities for story telling are rare (Grove, 2007; ten Brug et al., 2012). A narrative approach for people with PIMD should recognize the unique nature of their communication (Grove, 2007). This recognition should include the acknowledgment of the nonsymbolic nature of their communication, which is predominantly made up of body language and vocalizations, making them highly dependent on others for the interpretation of their communication signals. A move away from the Anglo-Western approach to narration, emphasizing coherence and resolution, to the storytelling approaches used by non-Western Indigenous people is advocated (Grove, 2007; Sable & Francis, 2012). Within these cultures, where stories are often open-ended, elliptical, and concealed, Grove (2012) makes particular reference to the Mi’kmaw stories of the first peoples of Nova Scotia and the Indigenous peoples of Australia, which do not conform to Western logic for sequencing time. Rather, stories are described as open, filled with possibility, mutability, and ongoing interpretation according to personal and shared experience (Sable & Francis, 2012). Parallels can be drawn between these Indigenous perspectives and the process of interpreting preferences of people with PIMD, whose communication may lack coherence and formality, and yet be highly complex and multilayered (Grove, 2007). This highlights the interdependent nature of Indigenous narrative tradition, a reflection of a collectivist perspective that values relationships, family, and community. “Everything, every person is spoken of in relation with something or someone else . . . everything existed within a network of relationships” (Sable & Francis, 2012, p. 32). This recognition of mutual dependence is of clear relevance to decision-making support for people with PIMD, including as it is applied to the realization of autonomy at the end of life.
The value of using historical narrative within the context of decision-making support has been demonstrated with people with PIMD. Using a decision-making support process, Watson (2016a) guided circles of support to collaboratively develop an understanding of the preferences of those they supported by sharing stories about their past. They shared these stories verbally and, where available, visually, using photos and videos. This collection and sharing of historical narratives were found to facilitate understanding of a person’s preferences, a fundamental aspect of a decision-making support for people with PIMD (Watson, 2016b). These collaborative understandings of preference were responded to and built into larger life decisions.
A supporter’s willingness to see the person they supported beyond their disability was found to impact their responsiveness to the expressions of preference of those they supported (Watson, 2016a). This notion of seeing a person beyond their disability has been previously described as an important factor in responsiveness to expressions of preference. Lyng (2007) used a strategy whereby he asked supporters questions such as, “If a person you support had complete control over their life, what music might they listen to, what car might they drive or what clothes might they wear?” He found that these questions allowed supporters to view those they supported as having preferences beyond those typically associated with their support needs. Drawing from Lyng’s work, Watson (2016a) asked similar questions of circles of support. These questions facilitated the collaborative development of narratives that highlighted perceived preferences of the people with PIMD they were supporting.
A narrative approach as described can be applied to decision-making support at the end-of-life for people with PIMD. Drawing on Watson’s (2016a) data, Table 1 demonstrates how a narrative approach can be applied within decision-making support relating to end-of-life decisions.
Application of a Narrative Approach in Supporting End-of-Life Decision Making for People with PIMD.
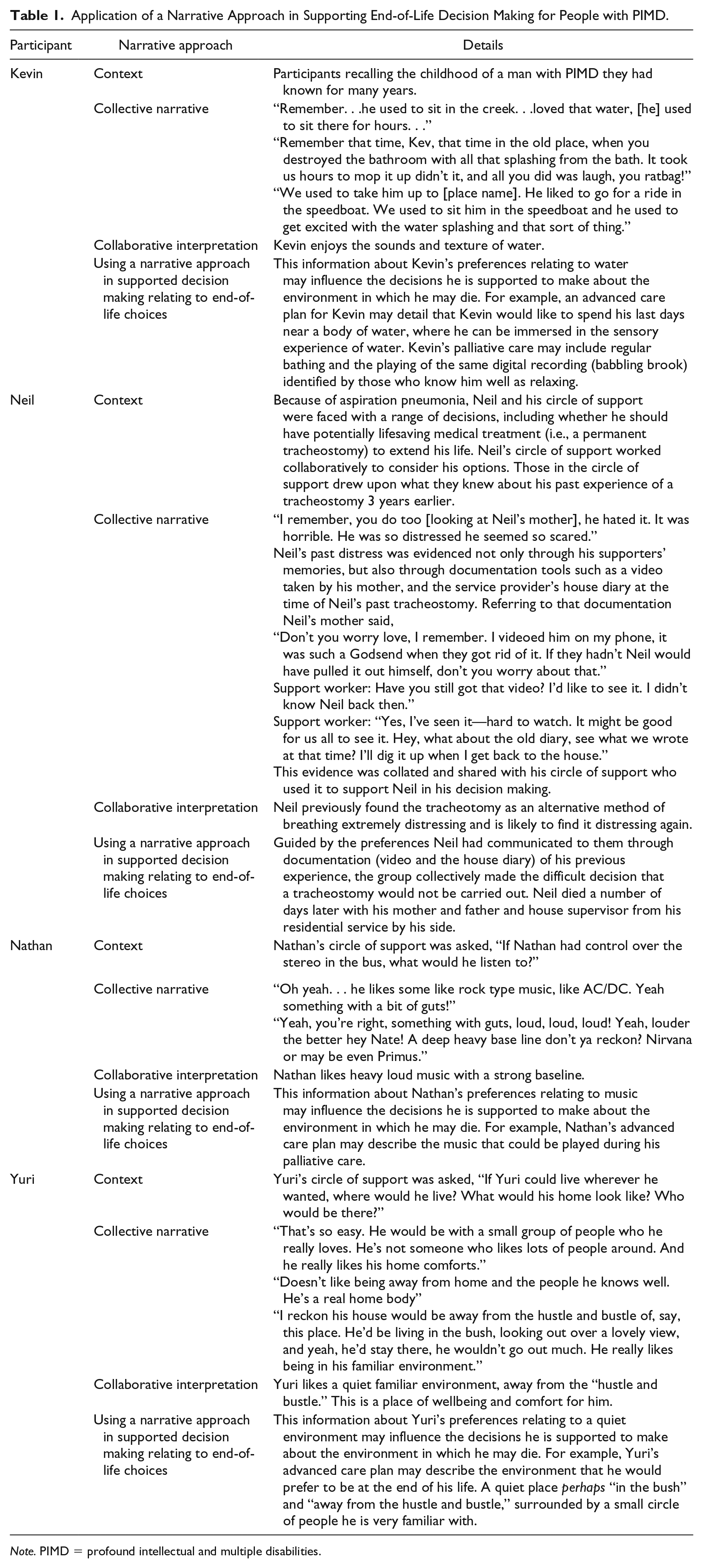
Note. PIMD = profound intellectual and multiple disabilities.
Implications for Practice
This paper has brought to life several ways practitioners can ensure meaningful end-of-life practices for people with PIMD through sharing of both historical stories as well as narratives about who a person is beyond their disability. Multimedia techniques for gathering, documenting, and sharing historical knowledge have been described and are reflected in the research and practice literature (Bunning, Heath, & Minnion, 2009; ten Brug et al., 2012). The sharing and documentation of historical information were found to be particularly effective for Neil’s circle of support (see Table 1) at the end of his life. Neil’s circle of support used tools such as a communication diary, verbal narrative, and importantly, video, to explore Neil’s previous expressions of preference, particularly in relation to his experiences of a past tracheostomy. Documentation of these historical expressions of preference was used to guide Neil’s circle of support in making a collective decision about his end-of-life care.
An additional narrative approach focused on “seeing a person beyond their disability” (Lyng, 2007) has clear application to the process of decision-making support at the end-of-life for people with PIMD. The stories collated about Yuri’s life “beyond his disability” (see Table 1) provide a picture of his ideal place of well-being. Those close to him perceive this place as away from the “hustle and bustle” perhaps “in the bush.” It is a place familiar to Yuri, where he feels comfortable. Further demonstrating this application, Nathan’s perceived music preferences “something with a bit of guts” may assist those supporting him to make decisions about the music he listens to at the end of his life. Narratives describing a person’s preferred environments, such as these, may serve as useful mechanisms for supporting people with PIMD to have their environmental preferences reflected in decisions made at the end of life and therefore may form an important part of their advance care plan.
Implications for Research
While there is an increasing focus on understanding and supporting end-of-life preferences for people with milder intellectual disability, the experiences of people with severe intellectual disability continue to be poorly represented in current empirical data (Stancliffe et al., 2017). It is hoped that this article has sparked inspiration for the development of a research agenda focused on maximizing autonomy for people with PIMD at the end of life. The authors suggest five directions for future research: (a) the development of a deeper understanding of the three components of supporter responsiveness, acknowledging, interpreting, and acting on, the expression of will and preference of people with PIMD within a supported decision-making paradigm, both at the end of and throughout a person’s life; (b) considering the established importance of relational closeness within decision-making support, further exploration of the factors that underlie the development of close and safe relationships between people with PIMD and their supporters; (c) exploration of health professionals’ perspectives, attitudes, and practice concerning people with PIMD in relation to end-of-life decision making and planning; (d) further exploration of the role that historical narrative and storytelling can play in understanding will and preference for people with PIMD, particularly in relation to decisions at the end-of-life; and (e) examination of decisions relating to end-of-life care and support (e.g., place of death, resuscitation, medication, funeral plans, assisted dying, people present at the time of death), particularly as they relate to people with PIMD and their circle of support.
Conclusion
Honoring a person’s preferences at the end of life is arguably one of the most profound gifts humans can give to one another. However, little attention has been paid to end-of-life planning for people with intellectual disability, particularly people with PIMD (Tuffrey-Wijne & Davidson, 2018; Voss et al., 2017). This is despite the life expectancy of people with intellectual disability increasing in line with the general population (Coppus, 2013). This lack of attention is arguably driven by an assumption that concepts relating to self-determination and autonomy have no relevance to people with PIMD, due to perceived decision-making incapability. There is little question that those supporting people with PIMD to plan for and make decisions about end-of-life care are faced with a challenge. However, this challenge needs to be undertaken, not only because of the human rights obligations defined in the CRPD but also due to the empirical evidence demonstrating the importance of autonomy in the creation of a good death (Granda-Cameron & Houldin, 2012). In response to this challenge, this article has drawn on empirical research to promote the value of decision-making support within the context of palliative care and advance care planning for people with PIMD. It promotes the use of storytelling, narrative, and multimedia (photos and video) as an approach to allow people with PIMD to have their expressions of preferences acknowledged and acted upon at the end-of-life. It provides practical examples of how such a narrative approach can be used to support decision making within the context of advance care planning and palliative care for people with PIMD. This article offers guidance for those providing decision making and advance care planning support for people with PIMD who traditionally have not been “heard” in this important stage of life. In addition, conversation as to how nations can live up to their obligations as defined in the CRPD in ensuring the right to autonomy is universal both throughout and at the end-of-life. Finally, the authors hope to have ignited an interest in this under researched area and opened an important conversation aimed at developing a research agenda focused on supporting decision making for people with PIMD in relation to their end-of-life care.
Footnotes
Editors-in-Charge: Meghan M. Burke and K. Charlie Lakin
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.