
Abstract
Introduction
Globally, adolescents and young adults face numerous challenges when it comes to accessing sexual and reproductive health (SRH) services. These services encompass contraception, abortion, sexually transmitted infection (STI) testing and treatment, and related counseling (Decker et al., 2021; Morris & Rushwan, 2015; Pandey et al., 2019). Young people's limited awareness of available services and the requirements for utilization, such as costs or parental consent, exacerbate these obstacles (Newton-Levinson et al., 2016). The sensitive nature of SRH matters may lead young individuals to hesitate in seeking guidance from their parents or other family members. Existing literature highlights a strong preference for confidentiality and privacy when it comes to young people seeking SRH services (Brittain et al., 2015; Pampati et al., 2019; Schapiro & Mihaly, 2021). Moreover, even family members may lack awareness of the availability of such services and the pathways for young people to access them.
Recognizing the low utilization of health services among young people, the World Health Organization has advocated for public health initiatives that enhance adolescents’ access to healthcare services, including SRH services (WHO, 2017). This global health objective aligns with the United Nations’ Sustainable Development Goals concerning the promotion of adolescent health (UN, 2015). However, the available data on effective strategies to achieve this global health goal are limited (Brisson et al., 2021, 2024). Given young individuals’ widespread use of the internet for seeking health-related information, they may also use online sources to gather information on accessing local SRH services (Beck et al., 2014; Freeman et al., 2018, 2020; Magee et al., 2012). Yet, the literature provides scant information on this subject, especially regarding young people in developing countries (Robards et al., 2018).
The concept of young people's agency in navigating healthcare systems is underexplored, particularly among those residing in developing countries like Colombia (Bundy et al., 2018). In Colombia, where comprehensive sex education is not equally accessible in school settings (Albornoz-Arias et al., 2019; Brisson et al., 2023), understanding how young Colombians seek information on accessing SRH services is important. Furthermore, this topic is timely because the Colombian Health Ministry recently implemented initiatives to enhance young people's access to SRH services. These initiatives involve promoting youth-friendly health services that educate and empower young individuals to utilize SRH services, including contraceptives, STI testing, and HPV vaccination (Colombian Health Ministry, 2021).
The Colombian healthcare system is a complex mix of public and private health insurance. Young people can access certain health services (e.g., abortion) free of charge through their parents’ health insurance plans without their parents being notified (Brisson et al., 2021, 2024; Romero & Reingold, 2013). In other instances, there are publicly funded services that offer free services to young people, such as STI and HIV testing. Yet, young people in Colombia may underutilize SRH services, as observable with high rates of adolescent pregnancy and STI transmission (Encuesta Nacional de Demografía y Salud, 2015; Mercado & Sandoval, 2017; Murad-Rivera et al., 2018). For example, the proportion of pregnancies among adolescents aged 15–19 years old in Colombia increased from 13.0% in 1990 to 17.4% in 2015 (Profamilia, 2010, 2018; Uribe et al., 2010). During 2015–2021, Colombia saw a 21.5% reduction in births among adolescents aged 15–19 years old; however, in 2021, there were still 106,695 adolescents aged 15–19 years who gave birth (Departamento administrative nacional de estadistica – DANE, 2023). Hence, it is important to understand how young Colombian people access SRH services. Specifically, the factors that enable access, such as searching online. Initiatives focused on providing comprehensive youth-friendly online material explaining how to access such services may help improve SRH outcomes. Such material could include clear descriptions of the steps needed to obtain contraceptives and STI testing, clarify if there are fees for services, and confirm if confidentiality is respected.
The objective of this cross-sectional study was to reveal, among young Colombian people visiting a clinic specialized in SRH services, how they inquired to access the clinic, and to explore their interest in the availability of online material (e.g., videos) explaining how to access SRH services. The findings were compared across sexes, age groups, socioeconomic groups, and types of services sought at the clinic. In 2016, Colombia was one of two countries in Latin America, following Venezuela, where the majority of internet users were people aged 15–24 years old (López Ponce & Arcila Calderón, 2016). In 2021, 84.1% of 12–24-year-olds in Colombia were internet users (Ministerio de Tecnologías de la Información y las Comunicaciones, 2022). Given the substantial internet usage among young Colombian people, and its confidential nature, it was hypothesized that they predominantly utilize online platforms to inquire about accessing SRH services (Martin et al., 2020; Mustanski et al., 2023; Park & Kwon, 2018).
Methodology
Design
The study took place in two Profamilia clinics in the cities of Medellin and Cali (Colombia's second and third most populous cities after Bogotá). Profamilia is a network of nonprofit clinics across Colombia specializing in SRH and a member of the International Planned Parenthood Federation. Clinics in large city centers have “Youth Centers” specializing in the provision of services for people under age 25 (e.g., psychological counseling and teaching about safe sex practices).
From August 21, 2019 to February 14, 2020, receptionists invited patients aged 10–24 years old to answer the survey while they waited for their appointment. This extended age range represents the new definition of adolescence in global health (Sawyer et al., 2018). At Profamilia, young people requesting STI/HIV testing must fill out paperwork and discuss testing with a nurse. Since this process is already time consuming, patients requesting STI/HIV testing were not invited to answer the survey. Instead, the survey was specifically targeted at young patients accessing all other health services (e.g., abortion, contraceptives, sterilization procedures, HPV vaccinations). To avoid disrupting the quality of services offered, receptionists invited patients to participate during less busy periods. The invitation detailed the study's purpose and clarified that participation was voluntary (i.e., no remuneration) and that the quality of clinic services they received would not be influenced by whether they participated or not. Receptionists documented the number and dates that invitations were made thereby allowing us to quantify the level of participation. Participants’ anonymity was preserved—participants inserted the completed survey into a locked box that only the first author had access to.
The survey (in Spanish) contained three parts. The first part contained 28 multiple-choice questions designed to gather information on the participants’ autonomy and opinions about their access to SRH services. This section asked about the methods participants used to gather information about the clinic's services, and whether they were visiting the clinic alone or if they brought a companion. Additionally, participants were asked: ¿Qué tan interesado estarías en tener acceso a videos de YouTube y/o contenido en línea explicando en detalle cómo utilizar los servicios de salud sexual y reproductiva en tu comunidad? (“How interested are you in accessing YouTube videos and/or online content that provides detailed explanations on using SRH services available in your community?”).
The second part of the survey contained 19 sociodemographic questions, including sex, age, estrato (socioeconomic classes assigned by the Colombian government based on residency; one is the lowest and six the highest), education level, and relationship status. The third part contained one open-ended question accompanied by a space for participants to provide their written response: ¿Hay algo que quieres agregar sobre el tema de la autonomía de los adolescentes para acceder a los servicios de salud sexual y reproductiva? (“Is there anything you would like to add on the theme of adolescent autonomy in accessing SRH services?”). Since only seven participants provided responses related to the internet, a qualitative analysis was not conducted. Instead, we present these seven responses (translated from Spanish) to highlight participants’ viewpoints and to complement the quantitative data collected.
Data Analysis
Participants were asked to select the ways they learned to access the clinic that day. It was possible to select more than one option. For instance, it was possible for a participant to have asked their friend and searched online. As such, data had to be recoded to help with data analysis and the responses were categorized based on the following priority order: (1) internet, (2) parents, (3) family members other than parents, and (4) friends or partners. For example, if the participant asked their father and their cousin, the answer was categorized once under the “parent” category and not in the “cousin” category. Given the different level of participation by age groups, the variable age was categorized as “younger adolescents” (11–16 years old), “older adolescents” (17–19 years old), and “young adults” (20–24 years old). Due to smaller counts, the upper three estratos were combined for analysis.
The four independent variables were sex, age group, estrato, and type of service sought at the clinic that day. We assessed whether there were statistically significant differences between the levels in each of the four independent categorical variables and how participants learned how to access the clinic (dependent variable coded as binary; e.g., internet vs all other sources) and second on their level of interest (very interested, interested, and not interest) in having online content explaining how to access SRH services. Statistical significance was assessed by performing Pearson chi-square tests of independence or Fisher's exact tests, as appropriate. P-values of <.05 were considered statistically significant, and 95% confidence intervals for proportions were calculated. Data analysis was performed in SPSS version 29 (IBM Corp, 2023).
Ethics
The University of Montreal's Research Ethics Board (REB) first evaluated and approved the research project. Then, Profamilia's REB (which included a lawyer) evaluated and approved the research project. The REBs determined that the level of risk for participating was low. Parental consent was not required; it would have been challenging for patients who came alone to the clinic to obtain parental consent. Guideline 17 (Research Involving Children and Adolescents) from the International Ethical Guidelines for Biomedical Research Involving Human Subjects (Council for International Organizations of Medical Sciences, 2017) informed the decision to forego requesting parental consent. This guideline asserts that under specific conditions, the waiver of parental permission is permissible when obtaining it is neither feasible nor desirable, and when the research poses minimal risk to participants.
Results
Characteristics of Participants
Among 1,272 individuals invited to participate, 812 (63.8%) completed the survey. Seventy-three percent of participants answered the survey in Medellin's clinic (63.4% participation rate), and 27.0% in Cali's clinic (65.0% participation rate). Although there were more than two sex/gender options, all but six participants selected male or female (Table 1). Most participants were female (91.4%), reflecting the sex distribution of Profamilia patients in Colombia (Profamilia, 2018). There was a lower proportion of younger participants, and half were aged 16–20 years old (50.3%). Most participants were from the lower three estratos (86.0%), which is reflective of the distribution of the population in estratos across Colombia, where only a minority are in the upper three estratos. A tenth of participants were displaced because of violence, which is slightly less than the proportion of internally displaced people in Colombia (15.3% ∼7.7 out of 50.2 million people) (Reyes & Fattori, 2019). Most participants were Colombian (92.7%), a minority Venezuelan (1.7%), and the rest did not answer the question on nationality. The majority (75.9%) of participants aged 17 and younger reported being enrolled in school. Close to half (48.1%) of respondents aged 18 and older had attended postsecondary education.
Characteristics of Survey Participants, N = 812.
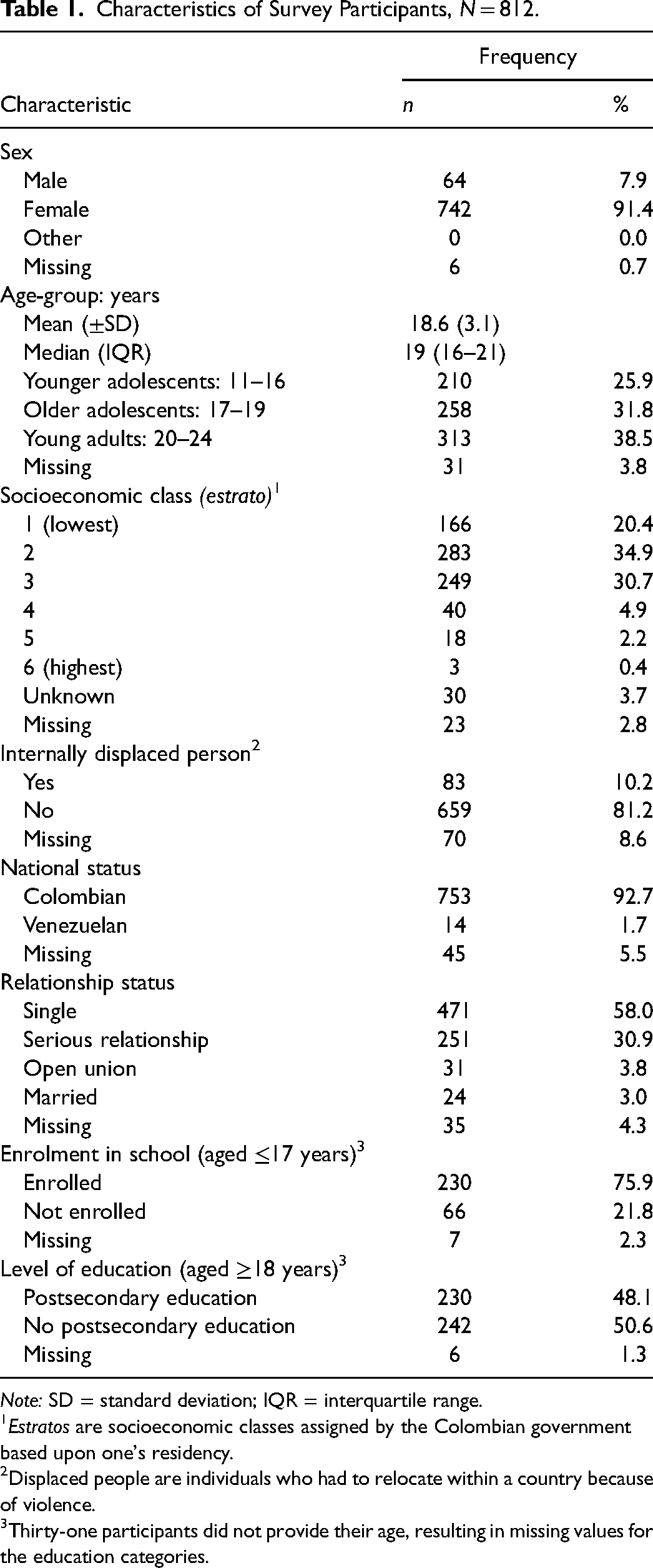
Note: SD = standard deviation; IQR = interquartile range.
Estratos are socioeconomic classes assigned by the Colombian government based upon one's residency.
Displaced people are individuals who had to relocate within a country because of violence.
Thirty-one participants did not provide their age, resulting in missing values for the education categories.
Source of Information
There were 735 (90.5%) participants who provided one answer, 64 (7.9%) provided two answers and 13 (1.6%) provided three answers on the source of information they used to learn how to access the clinic (Table 2). Close to a quarter (24.0%; CI: 21.2%–27.0%) of participants used the internet to inquire about how to access the SRH clinic that day (Table 3), which was smaller than hypothesized. The most common source of information was “parent(s)” with 30.7% (CI: 27.6%–33.9%) having inquired to at least one parent on how to access Profamilia that day. Specifically, 27.4% responded “mother” and 2.3% “father” only (Table 2). Participants from the upper estratos were more likely to have used the internet to inquire about accessing Profamilia that day than those in lower estratos (p = .011). There were no significant differences between sexes in terms of sources, except that females were more likely to ask a family member (p = .010) or “other” sources (p = .027). Young adults (aged 20–24 years old) were more likely to use the internet to inquire on how to access the SRH clinic (p < .001).
Sources Survey Participants Used to Learn How to Access Profamilia, Frequency, and Distribution.1
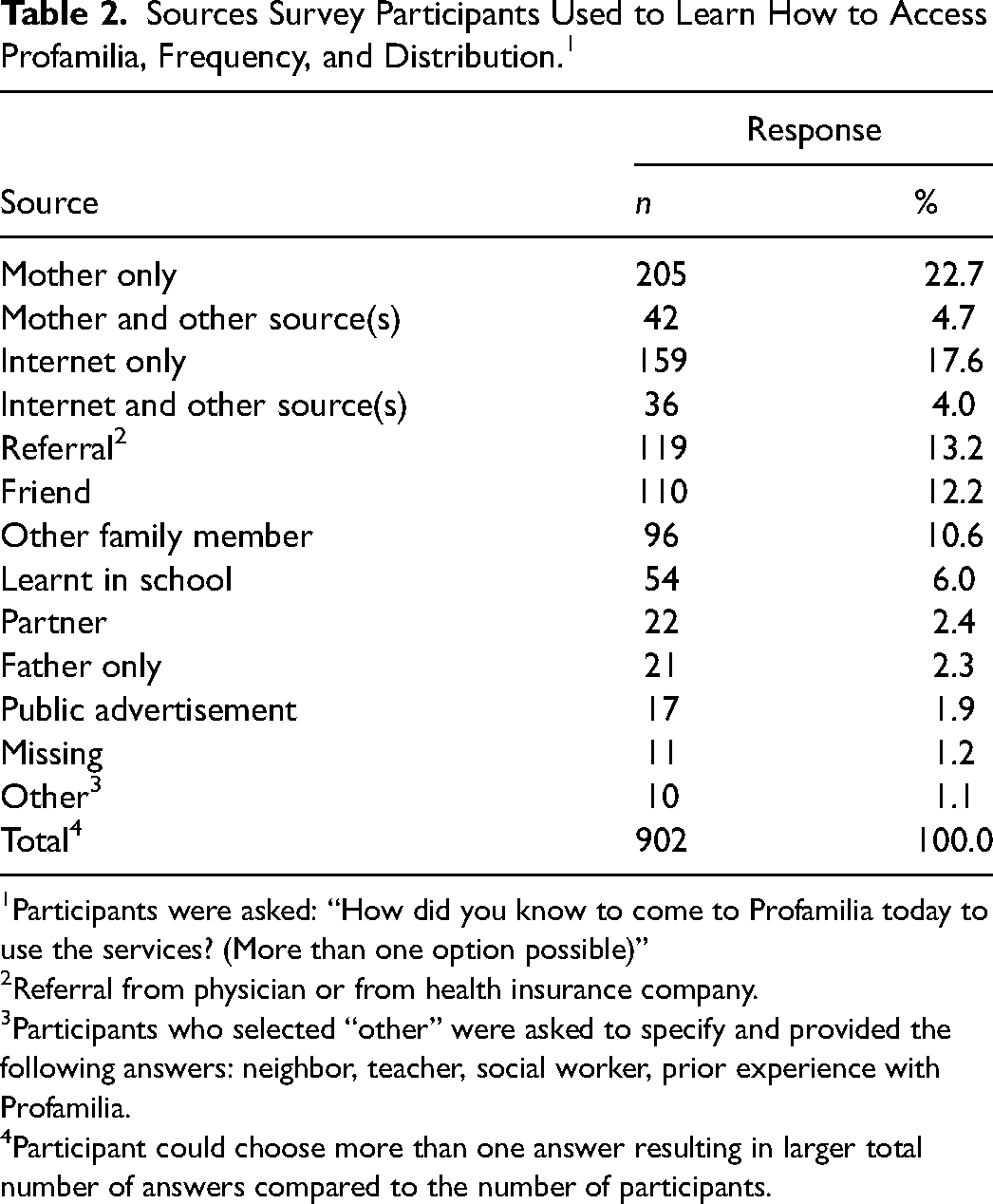
Participants were asked: “How did you know to come to Profamilia today to use the services? (More than one option possible)”
Referral from physician or from health insurance company.
Participants who selected “other” were asked to specify and provided the following answers: neighbor, teacher, social worker, prior experience with Profamilia.
Participant could choose more than one answer resulting in larger total number of answers compared to the number of participants.
Sources Survey Participants Used to Learn How to Access Profamilia, by Sociodemographics and Type of Service Sought.
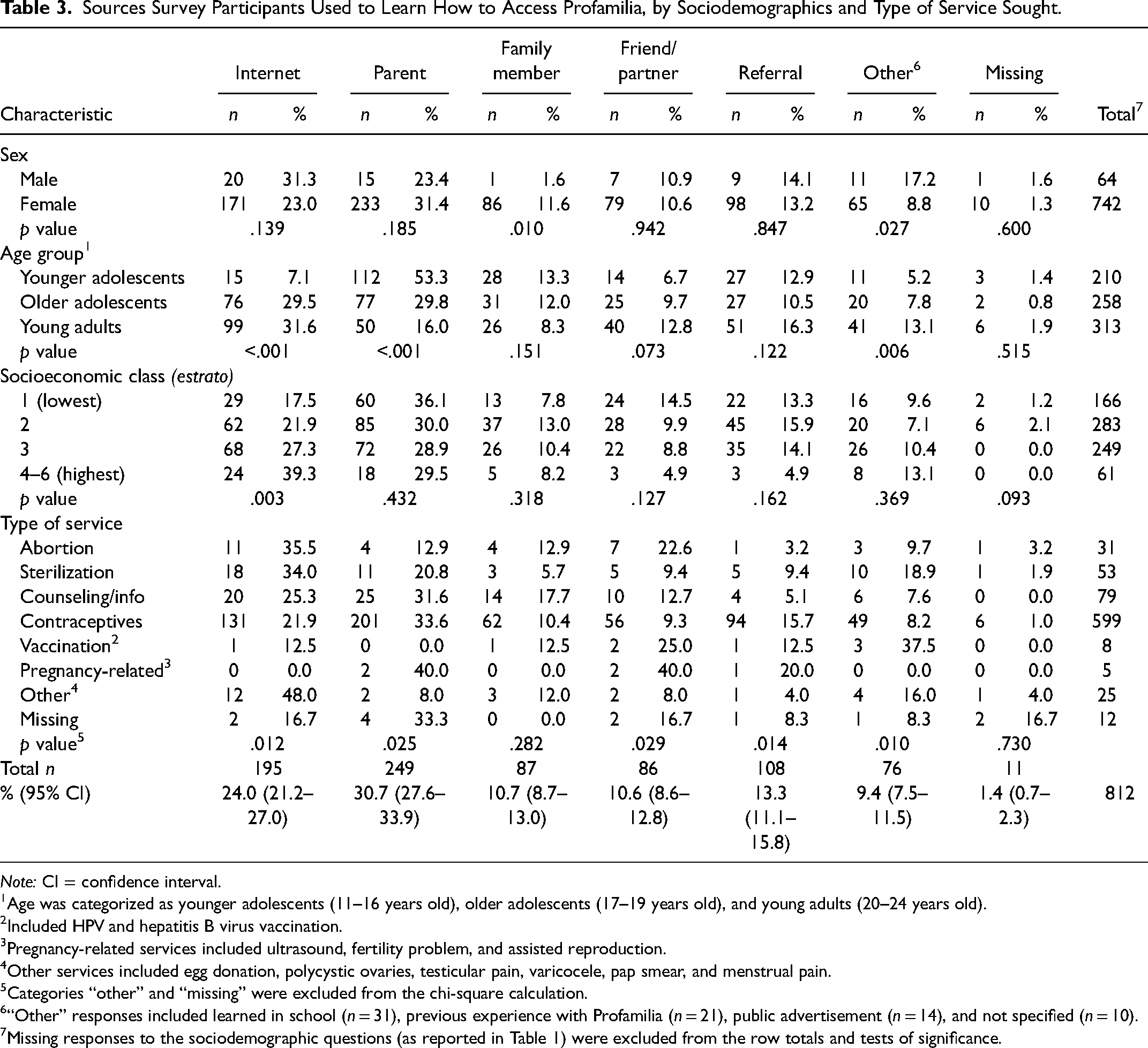
Note: CI = confidence interval.
Age was categorized as younger adolescents (11–16 years old), older adolescents (17–19 years old), and young adults (20–24 years old).
Included HPV and hepatitis B virus vaccination.
Pregnancy-related services included ultrasound, fertility problem, and assisted reproduction.
Other services included egg donation, polycystic ovaries, testicular pain, varicocele, pap smear, and menstrual pain.
Categories “other” and “missing” were excluded from the chi-square calculation.
“Other” responses included learned in school (n = 31), previous experience with Profamilia (n = 21), public advertisement (n = 14), and not specified (n = 10).
Missing responses to the sociodemographic questions (as reported in Table 1) were excluded from the row totals and tests of significance.
Table 3 also provides information on the type of service that the participant sought at Profamilia on the day they took the survey. The most frequently sought service was contraceptives (73.8%), followed by counseling and access to general SRH information (9.7%) and sterilization (6.5%). Note that sterilization can only be legally provided to individuals 18 years of age or older in Colombia. There were statistically significant differences for the categories: internet (p = .012), parent (p = .025), friend/partner (p = .029), referral (p = .014), and “other” (p = .010).
Interest in Online Content
Most participants indicated interest (81.5%; CI: 78.7%–84.1%) in having access to online material explaining how to access SRH services (Table 4). There were no statistically significant differences between sexes, estratos or type of service sought. Older participants were more likely to use the internet to inquire how to access Profamilia (Table 3), and they were more likely to be interested in having access to online material compared to younger participants.
Participants’ Interest in Having Online Content Explaining How to Access SRH Services.1
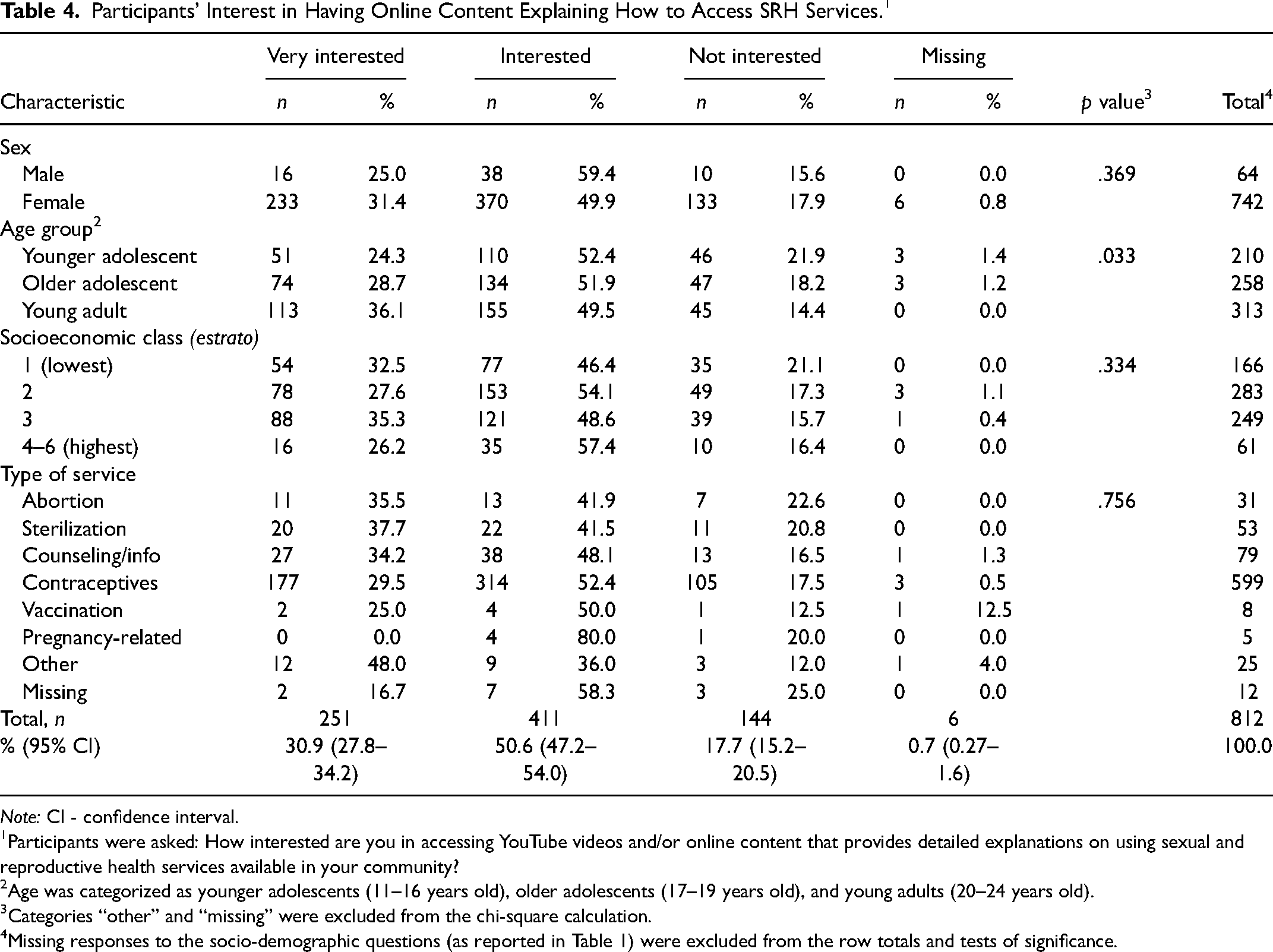
Note: CI - confidence interval.
Participants were asked: How interested are you in accessing YouTube videos and/or online content that provides detailed explanations on using sexual and reproductive health services available in your community?
Age was categorized as younger adolescents (11–16 years old), older adolescents (17–19 years old), and young adults (20–24 years old).
Categories “other” and “missing” were excluded from the chi-square calculation.
Missing responses to the socio-demographic questions (as reported in Table 1) were excluded from the row totals and tests of significance.
Participants’ Comments on the Internet
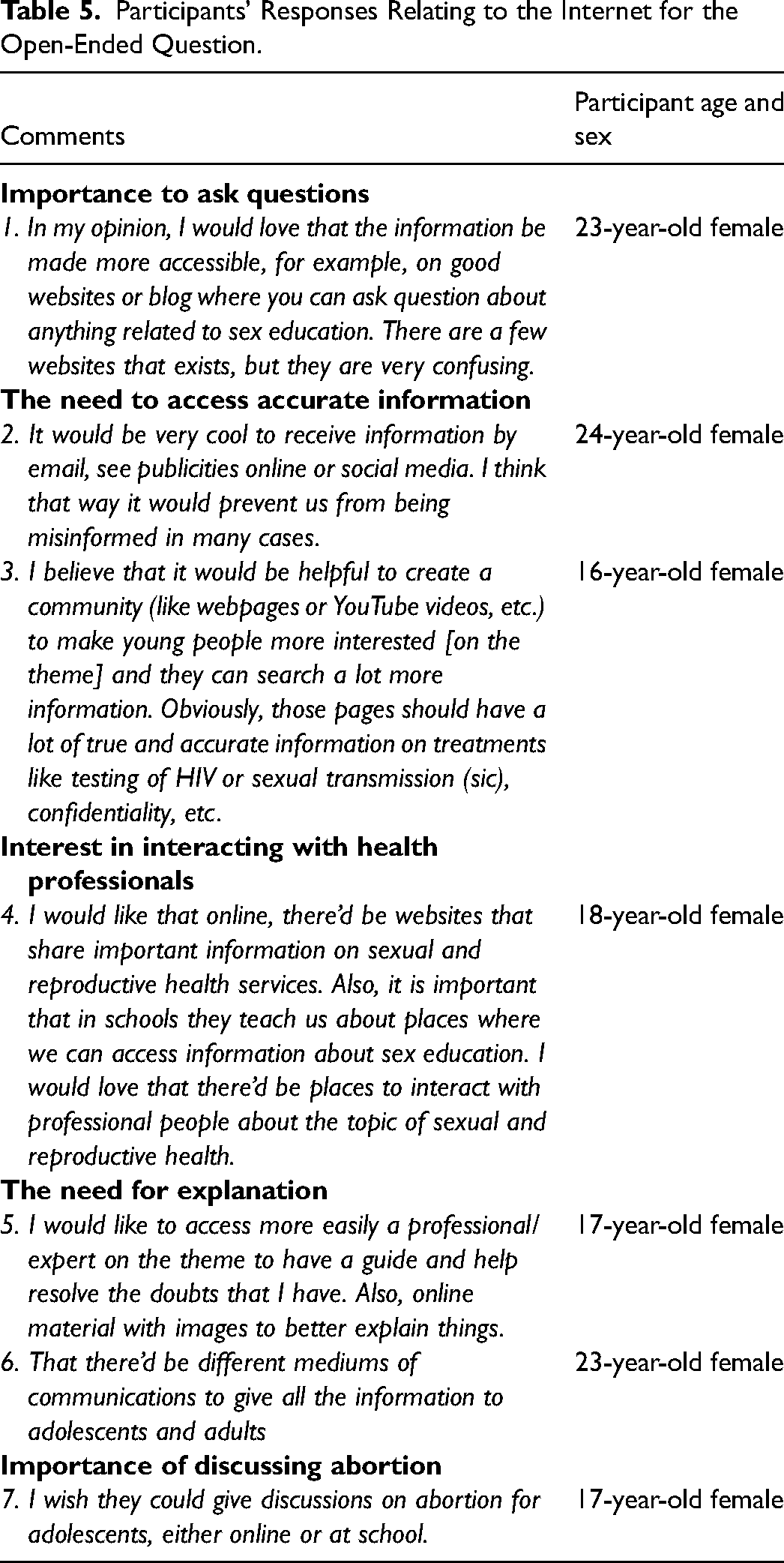
In total, 113 (13.9%) participants provided feedback to the open-ended question. Participants’ comments touched on different themes, including parental consent, health fees, sex education in school, health professionals’ behavior, asking for free contraceptives, and stigma around sexuality. However, only seven (6.2%) of the 113 participants made comments related to the internet (Table 5). The comments suggest that accessing understandable information is a concern for some participants.
Participants’ Responses Relating to the Internet for the Open-Ended Question.
Discussion
The main source of information for participants to learn how to access SRH was their parents, predominantly mothers. This corresponds to findings in studies conducted in various regions, suggesting that adolescents tend to discuss sex-related matters more frequently with their mothers compared to their fathers (Scull et al., 2022; Usonwu et al., 2021; Wilson & Koo, 2010). Studies conducted in different cultural contexts have shown parents can be a main source to discuss general SRH with their adolescents (Jerman & Constantine, 2010; Evans et al., 2020; Rose et al., 2016). For example, Evans et al. (2020) reported that among 901 parents in the United States, 97% discussed topics about sexuality with their adolescent. This highlights the importance of ensuring parents possess adequate knowledge on informing their adolescents on how to access SRH services. While parents were the most commonly reported source, participants reported learning how to access SRH services from a diversity of sources, including friends, partners, other family members, and school. This diversity underscores the complexity of the networks through which youth navigate to obtain health-related information, highlighting the multifaceted nature of their efforts to access healthcare services.
Empirical literature reporting on young people's sources of information to inquire how to access health services is scarce (Amanu et al., 2023; Chekol et al., 2023). Most research has been conducted in high-income countries (Robards et al., 2018) and focused on young people's general health-seeking information behavior (Jia et al., 2022), as opposed to the source of information young people use to access health services.
The age span (10–24 years old) within our sample reflects the transition phase known as youth, where substantial developmental differences, particularly in independence, can be observed between individuals. Our results highlight substantial variations among these age groups, with older participants demonstrating a greater propensity to utilize the internet for inquiries about accessing the SRH services than their younger counterparts. Consequently, it would be beneficial for health education programs to tailor their approaches according to age.
A critical barrier young people face in utilizing SRH services is the lack of knowledge on how to access SRH services (Newton-Levinson et al., 2016). One measure to address the issue would be to include explanations to youth on how to access their local SRH services as part of comprehensive sex education programs in schools as highlighted in UNESCO's International Technical Guidance on Sexuality Education (UNICEF, 2018). However, in Colombia, young people do not have equal access to comprehensive sex education in schools (Mercado & Sandoval, 2017; Murad-Rivera et al., 2018), hence, the need for alternative measures to assist young people, such as through educational online material. Our research focused on Colombian youth attending SRH clinics, which means that these individuals received enough information to be able to access the clinic on the day they were surveyed. However, the broad spectrum of information sources utilized by them underscores the need for a nuanced understanding of information-seeking behaviors among Colombian youth. Future research should explicitly explore the various channels through which adolescents acquire information about accessing SRH services and validate its content. This measure is particularly important given the potential for youth in receiving inaccurate or insufficient information, which could subsequently hinder their ability to access these critical services.
Almost one-fifth of participants reported no interest in online content explaining how to access SRH services. Participants were not asked to explain the reasons behind their choice of answer; however, it is possible that they are not regular internet users or that they might prefer parents or other trusted individuals to explain how to access such services. Future research should investigate through which other means youth would like to be taught how to access SRH services.
Research in the United States has shown that young people can be distrustful of sexual health information found online and may prefer to obtain information in school or peers and parents (Cohn & Richters, 2013; Freeman et al., 2020; Jones & Biddlecom, 2011). Young people's use of the internet to search for health-related information represent different risks and opportunities (Comulada et al., 2021; Hollis et al., 2020; Jain & Bickham, 2014). The internet can be a useful source of information for young people, but misinformation is a risk (Madden et al., 2016). To help mitigate risks, public health initiates could explore integrating parents into online health initiatives for adolescents. With most participants (81.5%) showing interest in online resources for SRH service access, future public health efforts should aim to develop secure and reliable digital platforms that effectively engage youth in learning about SRH services, ensuring these platforms are designed to be informative and accessible to young people.
This study has multiple strengths. The sample size was large enough to provide meaningful insights into young people's experiences accessing SRH services in Colombia. Given the sensitivity of the subject matter, this survey achieved a respectable response rate of 63.8%. This may be attributed to the anonymity afforded to participants, which likely facilitated greater candor in responses. Furthermore, the study employed a range of response options to ensure participants could effectively communicate their experiences and perceptions, thereby enhancing the richness and depth of the data collected.
Limitations
This study has limitations. First, the study sample was drawn from young people attending a SRH clinic for scheduled and walk-in appointments, which means they have already accessed SRH services and are as a result likely not representative of those who have not. For this reason, we caution readers in extrapolating the findings here to populations that have not accessed SRH services. Future research can explore the same topic with young people who have not accessed SRH services. Also, patients at Profamilia are not necessarily representative of patients who may access SRH services with their family physician or other clinics. While the survey garnered a respectable response rate, volunteer bias, where those who agree to participate and complete a survey differ from those who did not, may influence the results obtained. Originally, the recruitment approach was intended to be systematic, with receptionists inviting every patient between 10 and 24 years old to answer the survey. However, due to the workload of the receptionists, a convenience sampling approach was adopted, which may introduce selection bias. It is important to acknowledge that this change in sampling strategy could affect the representativeness of the sample. Furthermore, young patients present for HIV/STI testing were not invited to participate and they might have different answers on the subject. Finally, the survey did not undergo official piloting prior to dissemination.
Conclusion
This study investigated how young individuals in Colombia access SRH services, focusing on their use of the internet. Findings showed that only 24.0% of participants utilized the internet for this purpose, while 30.7% relied on their parents as a primary source of information (mostly mothers), indicating the critical role of parents in helping young people to access to SRH services. However, 81.5% expressed interest in accessing online resources to learn about accessing SRH services. These findings highlight the importance of parents and the internet in improving the accessibility of SRH services for young people in Colombia and should be considered by healthcare professionals and policymakers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by JB's Canadian Doctoral Award to Honour Nelson Mandela awarded by the Canadian Institutes of Health Research (201610GSD-385545-283387).