
Abstract
Introduction
At the beginning of the third year of the COVID-19 (COVID) pandemic, Peru had the world's highest death rate (over 6,450 deaths per million) from COVID with more than 213,000 deaths and counting (Beaubien, 2021). Hospitalization and care for COVID patients, particularly in rural and remote areas with limited resources and few ICU beds, added stress to the growing shortage of frontline workers. In Peru, this resulted in pre-health professional students filling in the gap in acute care clinical settings to support and provide patient care during the pandemic. While pre-health professional students are defined as any students pursuing a career in healthcare (Mosca & Grossman, 2019), many of these students in Peru were nursing and pharmacy students providing direct patient care, who often contracted and carried the virus resulting in the infection of their families and friends. The purpose of this international, collaborative study was to examine the impact of COVID on depression, anxiety, stress, coping, and grief on pre-health professional undergraduate nursing and pharmacy students in Lima, Peru.
Background
As of December 2022, more than 6.6 million people, globally, have died from COVID (Statista, 2022; WHO, 2022). Unique to the COVID pandemic is the increased severity of grief that was worsened due to the physical isolation protocols associated with quarantine, isolation from social support and meaningful family interactions, restricted funeral practices, and other socioeconomic considerations that may have led to protracted or complex grief following a loss (Breen et al., 2021). Furthermore, recent research has indicated that acute grief is being rated as more severe as compared to acute grief prior to the current pandemic (Eisma & Tamminga, 2020) and that loss from COVID results in more severe grief than with loss from natural causes (Eisma et al., 2021).
In recent research on the pandemic's impact on pre-health professional students, the need to explore students’ psychosocial wellbeing has become a major theme (Michel et al., 2021). Internationally, among nursing students, participants have reported challenges related to stress, anxiety, coping, and learning logistics (Michel et al., 2021). Pre-health professional students face similar risks and mental health challenges as frontline workers, without the same level of employee resources, education, and support (Blake et al., 2021). Increasingly high numbers of pre-health professional students reported feeling mentally unwell and anxious and expressing fear of COVID (Blake et al., 2021).
At the onset of our study's launch, there was limited published research exploring this phenomenon. However, one recent study indicated undergraduate students had increased mental health problems (e.g., depression, anxiety, and stress), which were associated with lower self-report levels of resilience and higher self-reports of insomnia, during the pandemic (Alyoubi et al., 2021). Another study found that nursing students reported higher rates of PTSD and insomnia amid COVID (Gao et al., 2021). A more recent study exploring the mental health and resilience of pharmacy students found that depression, anxiety, and stress were reported among participants, while resilience was reported as low (Halat et al., 2022). This growing body of evidence suggests more research is needed to explore the mental health and grief of pre-health professional students, particularly during times of crisis as with the COVID pandemic.
Objectives
Few studies have explored the impact of the COVID pandemic on pre-health professional students’ mental health. This exploratory study assesses the mental health challenges of undergraduate nursing and pharmacy students in Lima, Peru. The purpose of this study was to examine the impact of COVID on mental health challenges (i.e., depression, anxiety, stress, and coping) and grief on undergraduate nursing and pharmacy students. The reporting of such research is often inadequate, which hampers the assessment of its strengths and weaknesses and of a study's generalizability.
The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Initiative developed recommendations for the accurate and complete reporting of observational studies. The STROBE guidelines are part of the Equator Network that has been established to enhance the quality of publications. These guidelines are globally accepted as standards of evidence-based research. The guidelines are too extensive to provide examples, but they can be reviewed via the weblink listed on the reference page. STROBE guidelines include a checklist of 22 items that should be addressed in research articles (Vandenbroucke et al., 2007), and these guidelines were followed to report the research and its findings.
For this study, the research questions were:
What differences in depression, anxiety, stress, coping, and grief are attributable to demographic characteristics among nursing and pharmacy undergraduate students? To what extent is exposure to COVID associated with levels of depression, anxiety, stress, coping, and grief? Does experiencing death or significant loss due to COVID moderate the relationship between exposure to the virus and its association with depression, anxiety, stress, coping, and grief?
Methods
Study Design
This quantitative, descriptive study used convenience sampling to examine students’ self-reports of mental health (e.g., depression, anxiety, stress, and coping) and grief of pre-health professional students at baseline during data collection. This study design was used to capture how participants’ mental health and grief may have been impacted in response to the COVID pandemic. The sample was limited to undergraduate nursing and pharmacy students given their accessibility and proximity to the research team.
Setting
The study took place in Lima, Peru, at the María Auxiliadora University (UMA), a private university licensed by the National Superintendence of Higher University Education (SUNEDU), located in the district of San Juan de Lurigancho. The district of San Juan de Lurigancho has a population of more of 1.2 million (INEI, Peru, 2022), which accounts for over 12% of Lima's population, and it is also one of the poorest districts within Lima.
Currently, UMA serves the educational needs of around 3,570 undergraduate students divided into seven programs – pharmacy and biochemistry (1,836), nursing (1,114), psychology (193), nutrition (108), international business (121), business and marketing (57), and accounting and finance (138) – and over 600 graduate students in the 5 specializations in nursing and its master's degree in public's health. Currently, 77% of students enrolled in all UMA undergraduate programs are female and 81% of students work to pay for their college tuition and fees.
Participants
For this study, the sample was students enrolled in the nursing and pharmacy programs at UMA. Participant eligibility included (a) currently enrolled as an undergraduate in either the nursing or pharmacy program, (b) 18 years of age or older, and (c) able to read and understand Spanish. Students enrolled in graduate programs were excluded from this study to control for confounding factors. Graduate students and undergraduate students differ in age and life experience, which may influence their coping mechanisms and resilience in response to the COVID-19 pandemic. By limiting the study to undergraduate nursing and pharmacy students, we sought to minimize these potential sources of variability in our results. Participation was voluntary, and informed consent was obtained following Ethics Board approval at UMA and Institutional Review Board (IRB) approval at The University of Alabama.
Measurements
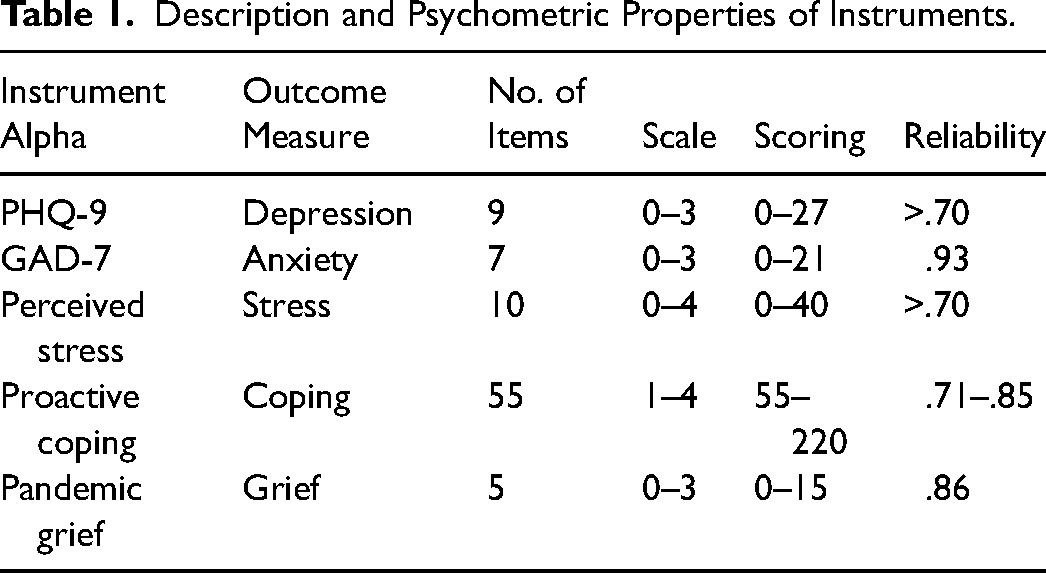
Sociodemographic data was collected and analyzed to determine generalizability of the study findings. Sociodemographic data collected included age, gender, race, ethnicity, marital status, family income, religiosity/spirituality, healthcare insurance, self-report grade point average (GPA), and history of COVID. Self-reported data on depression, anxiety, stress, coping, and grief was also collected. The instruments used to measure these constructs were depression, PHQ-9 (Kroenke et al., 2001); anxiety, GAD-7 (Spitzer et al., 2006); stress, the Perceived Stress Scale (Cohen et al., 1983); coping, the Proactive Coping Scale (Sohl & Moyer, 2009); and grief, the Pandemic Grief Scale (Lee & Neimeyer, 2020). All the instruments have reported reliability and validity in both Spanish and English. Additionally, the instruments have been validated with a Peruvian sample. A post-hoc power analysis was done to determine reliability for the sample, as reported as depression (α = .92), anxiety (α = .91), stress (α = .73) coping (α = .96), and grief (α = .89).
Depression: The Patient Health Questionnaire-9
The Patient Health Questionnaire-9 (PHQ-9) scale is a brief assessment that is used to determine the presence or severity of depression symptomology. The PHQ-9 is a nine-item measure with a four-point Likert scale. The survey asks questions related to mental health and depression over a period of the last 2 weeks. A score of 1 to 4 results indicates “minimal depression,” and a score of 20 to 27 indicates “severe depression.” The PHQ-9 is considered a reliable and valid instrument. Diagnostic validity of the PHQ-9 was established via patient screenings, and results showed that individuals who scored high (≥10) on the PHQ-9 were between 7 and 13.6 times more likely to be diagnosed with depression by the mental health professional; conversely, individuals scoring low (≤4) on the PHQ-9 had a less than a 1 in 25 chance of having depression (Kroenke et al., 2001). Internal consistency of the PHQ-9 is considered high as evidenced by a study involving two different patient populations with Cronbach alphas of .86 and .89 (Kroenke et al., 2001). Examples of the items include the following statements: “Little interest or pleasure in doing things”; “Feeling down, depressed, or hopeless”; and “Trouble falling or staying asleep, or sleeping too much.”
Anxiety: Generalized Anxiety Disorder-7
The Generalized Anxiety Disorder-7 (GAD-7) scale is a seven-item survey used to measure the presence and severity of anxiety. Anxiety is typically defined as a feeling of worry, nervousness, or unease (Spitzer et al., 2006). The GAD-7 is widely viewed as a reliable and valid instrument (Spitzer et al., 2006). Research on the GAD-7 indicates that it has good internal validity (Cronbach α = .92), good test–retest reliability (intraclass correlation = 0.83), and criterion, factorial, and procedural validity (Spitzer et al., 2006). Examples of the items include: “Feeling nervous, anxious, or on edge”; “Not being able to stop or control worrying”; and “Worrying too much about different things”.
Stress: The Perceived Stress Scale
The Perceived Stress Scale (PSS) is a widely used measure of stress. The PSS is a 10-item survey with items that are measured using a four-point Likert scale (Cohen et al., 1983). The PSS items, as a global stress measure, are general rather than event-specific and evaluate individuals’ perceptions of their lives as being “unpredictable, uncontrollable, and overloading” (Cohen et al., 1983, p. 387). Internal consistency reliability for the PSS total scores was adequate for the sample (α = .82). The questions in this scale ask about participant thoughts and feelings in the last month. Examples of the items include the following: “In the last month, how often have you been upset because of something that happened unexpectedly?”; “In the last month, how often have you felt that you were unable to control the important things in your life?”; and “In the last month, how often have you felt nervous and ‘stressed’?”.
Coping: The Proactive Coping Inventory
Coping was measured using the Proactive Coping Inventory (PCI). The PCI is an inventory, consisting of seven subscales, to assess skills in coping with distress, as well skills to promote wellbeing and greater life satisfaction. Proactive coping is defined as a method of assessing future goals and setting the stage to achieve them successfully (Sohl & Moyer, 2009). The PCI is a 14-item subscale with items that are measured using a four-point Likert scale. The subscales of the PCI have high internal consistency (Cronbach alphas reported range from .71 to .85 for all seven scales), good item–total correlations, and acceptable skewness as an indicator of symmetry around the mean (Sohl & Moyer, 2009). Examples of items from the PCI subscale include the following: “I am a ‘take charge’ person”; “I try to let things work out on their own”; and “After attaining a goal, I look for another, more challenging one”.
Grief: The Pandemic Grief Scale
The Pandemic Grief Scale (PGS) is a brief mental health screener to identify probable cases of dysfunctional grief associated with COVID-19 death and loss. The PGS is a five-item scale, which was based on 831 adults who lost someone to COVID-19 and demonstrated solid reliability (αs = .86), factorial validity (PCA and CFA support), and construct validity with strong correlations with suicidal ideation and substance use coping (Lee & Neimeyer, 2020). The PGS measures COVID-19 grief across demographic groups and discriminates well between persons with and without dysfunctional grief using an optimized cut score of ≥7 (87% sensitivity and 71% specificity) (Lee & Neimeyer, 2020). The PGS also demonstrates incremental validity in functional impairment due to a COVID-19 loss beyond measures of depression and generalized anxiety (Lee & Neimeyer, 2020). These findings support the PGS as an efficient and valid screening tool for clinical research and practice during a pandemic. Participants rated how frequently they experienced each grief symptom within the last 2 weeks. Examples of the items include the following: “I wished to die in order to be with the deceased”; “I experienced confusion over my role in life or felt like my identity was diminished because of the loss”; and “Nothing seemed to matter much to me because of this loss”. Table 1 presents descriptive information about each instrument.
Description and Psychometric Properties of Instruments.
Procedure
Data was collected in the Fall of 2021 using an online survey emailed to participants via a listserv with prior approval from the Ethics Board, IRB, and University Administration. The authors of this manuscript served as the research team, which was comprised of internal and external researchers from Peru and the United States representing the disciplines of nursing, social psychology, social work, and higher education administration. Undergraduate nursing and pharmacy students were recruited via recruitment emails, flyers, and social media to participate in the study during data collection in the Fall of 2021. The research team members based in Peru were responsible for the recruitment process, data collection, data maintenance, and data analysis to expedite the study.
Questionnaires were sent out by email through Microsoft Forms on a secure network. Surveys were in Spanish and completion of the online survey was considered implied consent. All questionnaires were voluntary and anonymous. Students were not penalized for not participating in the survey nor were extra benefits provided to students who participated in the survey.
Bias
Anonymity of participants was used to control bias. Researchers were blind to the data. Data was collected online through a private, secure database. Selection bias was addressed by randomized student selection.
Study Size
A power analysis was calculated, using G*Power Software, to determine 300 students were needed for adequate power. G*Power is a free tool that can be used to calculate statistical power for various statistical methods (t-tests, F-tests, χ2 tests, z-tests, and some exact tests) (Erdfelder et al., 1996). This software is helpful for researchers to estimate the sample size and to conduct power analysis.
Statistical Analysis
As a first step, descriptive analyses for the study variables were performed. In these analyses, we observed that the database had a 10.9% of missing values. To determine if data was missing completely at random (MCAR) Little's test (1988) was performed showing that there was not enough evidence to reject MCAR (p = .40). To address missing data for the latter steps of the analysis, multiple imputation was carried out. Using Predictive Mean Matching (PMM), 20 complete databases were generated.
To address the first study question, five multiple linear regression models were estimated with ethnicity, age, gender, marital status, income, religion, health insurance type, career, study cycle, GPA, and vaccine status as predictors. Each of these models had a different outcome variable: coping, anxiety, grief, stress, and depression. To address the second study question, two variables (COVID diagnosis and significant loss due to COVID) were added to each one of the regression models. To address the third study question, an interaction term between COVID diagnosis and significant loss due to COVID was added to all the regression models.
For each of the outcome variables, the three models were compared. Only the models with a significant increase in variance explained are reported and interpreted. All statistical analyses were carried out in R v4.1.2 (R Core Team, 2021) and RStudio v2021.09.0 (RStudio Team, 2021), using the following packages: psych (Revelle, 2021), car (Fox & Weisberg, 2019), naniar (Tierney et al., 2021), and mice (van Buuren & Groothuis-Oudshoorn, 2011).
Results
Participants
Participants were asked to report their age, gender, race, ethnicity, marital status, family income, religiosity/spirituality, healthcare insurance, and self-report GPA. Additionally, participants were asked to report any history of a COVID diagnosis for themselves and their family members. Participants were also asked if they know anyone, personally, who had died of COVID.
Descriptive Statistics
A total of 281 students participated in the study, and 82.92% of participants reported to be females. The most prevalent ethnicity was Mestizo (62.63%), followed by Quechua (19.22%), 5.34% reported to be White, and 12.91% reported to have other ethnicities. Most of the sample were between 25 and 49 years old, and near a fourth of the sample were between 18 and 24 years old (23.57%); only 2.5% of the sample reported an age between 50 and 64 years. Two-thirds of the sample reported to be single (59.79%), 37.37% reported to be married, and 2.86% reported to be divorced. In terms of income, 55.52% of the sample reported that they did not know their family income, 39.50% reported to have an income lower than $12,000 a year, and only a 4.98% of the sample reported to have an income higher than $12,000 a year. In terms of religiosity, 78.65% of the sample reported to be religious, while 21.35% reported to be nonreligious. Finally, 58.01% of the participants reported having public health insurance, 38.08% of the participants reported having mixed health insurance, and only a 3.91% reported having private health insurance.
Main Results
More than half the sample studied were pharmacy students (53.21%), and 46.79% were nursing students. Participants were evenly distributed across the 10 different study cycles of their professional programs. In terms of COVID diagnostic, nearly half of the sample reported to be diagnosed with COVID (47.54%). Most of the sample reported to have had a family member diagnosed with COVID (78.14%), and almost half reported having lost a significant family member due to COVID (43.01%). Only 7.47% of the sample reported that they did not receive a COVID vaccine with 8.19% reported receiving the first dose, 65.48% reported receiving the second dose, and 18.86% reported receiving the booster shot.
Descriptive statistics and correlations coefficients for the study variables can be observed in Table 2. Coping was negatively correlated with stress (Rho = −0.24, p < .01), but no other significant correlations for this variable could be observed. Nevertheless, anxiety was positively correlated with grief (Rho = 0.35, p < .001), stress (Rho = 0.53, p < .001), and depression (Rho = 0.76, p < .001). Grief was also positively correlated with stress (Rho = 0.25, p < .001) and depression (Rho = 0.39, p < .001). Finally, stress was also positively correlated with depression (Rho = 0.51, p < .001).
Mean, Standard Deviations, and Spearman Correlations of Coping, Anxiety, Grief, Stress, and Depression.
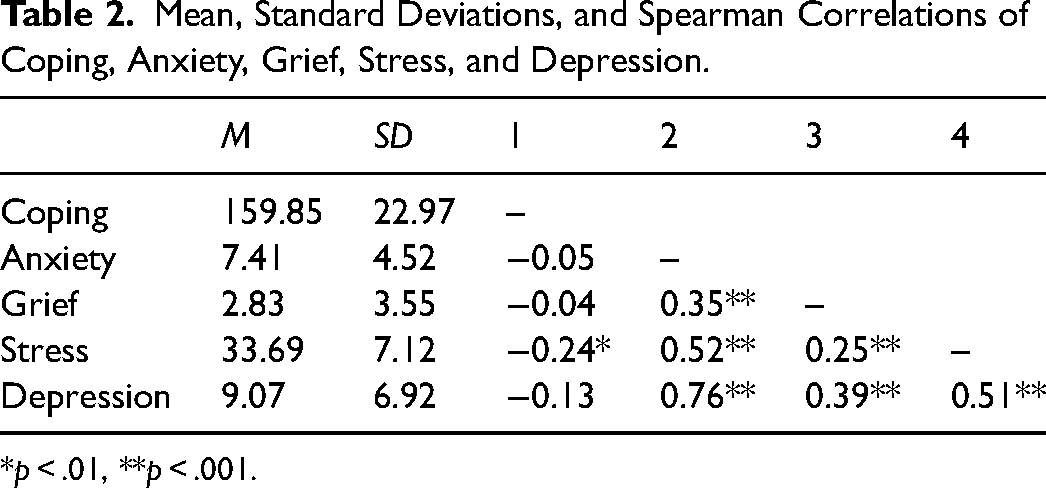
*p < .01, **p < .001.
The final regression model for coping, anxiety, grief, stress, and depression can be observed in Table 3. First, in terms of the demographic characteristics, female participants reported significantly lower levels of coping than male participants (b = −0.25, SE = 0.08, p < .01). There were also differences for marital status; married participants reported higher levels of coping than divorced participants (b = 0.59, SE = 0.18, p < .01); similarly, single participants reported higher levels of coping than divorced participants (b = 0.54, SE = 0.18, p < .01). In terms of income, participants with incomes >$12,000 a year reported higher levels of coping than those with smaller incomes <$12,000 a year (b = 0.37, SE = 0.15 p = .01). Religious participants also reported higher levels of coping than nonreligious participants (b = 0.18, SE = 0.08, p = .02). Finally, participants that reported having two doses of the COVID vaccine showed higher levels of coping than those that have not received any vaccine (b = 0.30, SE = 0.12, p = .01); similarly, participants with the booster dose showed higher levels of coping than the participants that have not received any vaccine (b = 0.29, SE = 0.14, p = .04).
Multiple Regression Models for Coping, Anxiety, Grief, Stress, and Depression Predicted by Demographic Characteristics, Exposure to COVID-19, and Significant Loss Due to COVID-19.
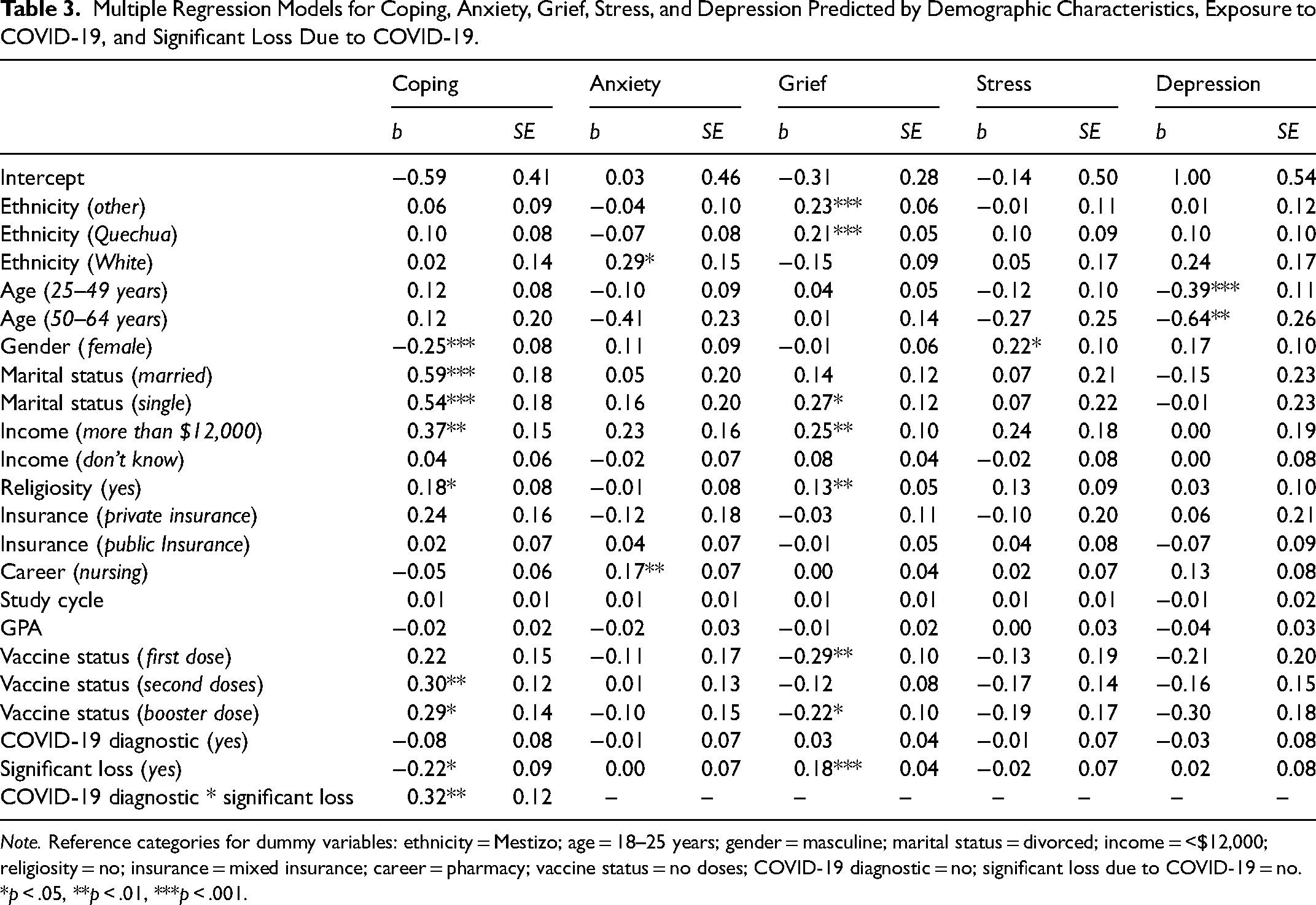
Note. Reference categories for dummy variables: ethnicity = Mestizo; age = 18–25 years; gender = masculine; marital status = divorced; income = <$12,000; religiosity = no; insurance = mixed insurance; career = pharmacy; vaccine status = no doses; COVID-19 diagnostic = no; significant loss due to COVID-19 = no.
*p < .05, **p < .01, ***p < .001.
For this model, the interaction term between COVID diagnostic and significant loss due to COVID was significant. This indicates that when a participant was diagnosed with COVID but did not lose a significant person due to COVID, there is no effect in coping (b = −0.08, SE = 0.08, p = .30). Furthermore, when the person was not diagnosed with COVID but lost a significant person, their levels of coping decrease (b = −0.22, SE = 0.09, p = .02). Nevertheless, when the person was diagnosed with COVID and lost a significant person, there is a significant increase in coping (b = 0.32, SE = 0.12, p = .01). This model explained 19% of the total variance of coping (R2 = 0.19).
In the regression model for anxiety, observed in Table 3, participants identified as White reported higher levels of anxiety than participants identified as Mestizo (b = 0.29, SE = 0.15, p = .05). Nursing students reported higher levels of anxiety than pharmacy students (b = 0.17, SE = 0.07, p = .01). No other demographic characteristics showed any significant difference in anxiety. For anxiety, the interaction effect between COVID diagnostic and significant loss due to COVID was not significant, so it was not included in the final model. In the model, COVID diagnostic and significant loss due to COVID did not show any significant effect. This model explained 13% of anxiety's variance (R2 = 0.13).
For regression model predicting the participant grief, ethnicity differences could be observed. Participants with other ethnic identifications showed higher levels of grief than participants identified as Mestizo (b = 0.23, SE = 0.06, p < .01). Also, participants identified as Quechua showed higher levels of grief than participants identified as Mestizo (b = 0.21, SE = 0.05, p < .01). On the other hand, single participants showed higher levels of grief than divorced participants (b = 0.27, SE = 0.12, p = .03). Income was also relevant for grief levels; participants that reported incomes >$12,000 a year showed higher levels of grief than participants that reported lower incomes (b = 0.25, SE = 0.10, p = .01). Religious participants reported higher levels of grief than nonreligious participants (b = 0.13, SE = 0.05, p = .01). For the vaccine status, participants with the first dose of the COVID vaccine reported lower levels of grief than participants with no vaccines (b = −0.29, SE = 0.10, p = .01); also, participants with the booster dose showed lower levels of grief than participants with no vaccines (b = −0.22, SE = 0.10, p = .02). For this model, the interaction term between COVID diagnostic and significant loss due to COVID was not statistically significant, so it was not included in the final model. However, participants that reported a significant loss due COVID reported higher levels of grief than participants (b = 0.18, SE = 0.04, p < .01). This model explained 28% of the total variance of grief (R2 = 0.28).
For the model predicting participant stress, the only demographic characteristic that resulted statistically significant was gender. Female participants reported higher levels of stress than male participants (b = 0.22, SE = 0.10, p = .03). COVID diagnostic and significant loss due to COVID did not show any direct significant effect or interaction effect. This model explained a 6% of the stress variance (R2 = 0.06).
In the final regression model for depression only, the participant age was significantly associated with depression. Participants that ranged from 25 to 49 years reported lower levels of depression than participants ranged from 18 to 24 years (b = −0.39, SE = 0.11, p < .01); furthermore, participants ranged from 50 to 64 years reported lower levels of depression than participants ranged from 18 to 24 years (b = −0.64, SE = 0.26, p = .02). No direct effect or interaction effect could be observed from COVID diagnostic and significant loss due to COVID-19. This model explained 18% of the total variance of depression (R2 = 0.18).
Discussion
Key Results
Recent research exploring the pandemic impact on pre-health professional students indicates the need to explore student mental health and psychosocial wellbeing (Michel et al., 2021). Study participants from international nursing student populations have reported challenges related to anxiety, stress, coping, and learning logistics (Michel et al., 2021). Increasingly high numbers of students report concerning indicators of poor psychosocial wellbeing including feeling mentally unwell, anxious, and fearful of COVID (Blake et al., 2021).
Given the limited number of studies exploring this phenomenon, the purpose of this study was to examine the impact of COVID on depression, anxiety, stress, coping, and grief on undergraduate nursing and pharmacy students in Lima, Peru. This is the first study of its kind to explore and analyze nursing and pharmacy students’ perceptions on how the COVID pandemic impacted their mental health and grief. The results yielded important findings that indicate nursing and pharmacy students in this population are experiencing mental health challenges and grief due to the COVID pandemic.
This study findings indicate a need to provide pre-health professional students with targeted psychological support and professional mental health counseling specific to grief. It is imperative to highlight the specific impact of the research findings on Latino communities. A potential barrier to accessing grief support may be the predominant hesitancy within Latino culture to seek professional help beyond the family, church, and community. Given this hesitancy, it may be important to embed the mental health support services for pre-health professional students in community centers and churches, where the students live and worship.
We maintain that this study may increase awareness surrounding mental health needs and grief responses inherent in the healthcare profession, while dissemination of these findings may serve as a conversation starter for shared mental health challenges and grief experiences. We implore healthcare professionals and educators to be mindful of and responsive to potential mental health challenges and grief responses not only in themselves but also in their colleagues and pre-health professional students to help reduce the adverse impact of COVID noted in the study findings. Recommendations for additional student support include academic student support services, academic coaching, student mentoring, and mental health resources.
Ultimately, this study's findings have the potential to advance our knowledge of mental health and wellbeing of pre-health professionals amid the COVID pandemic and beyond. This project has provided data needed to inform and develop a mental health program for students at the research site. In addition, preliminary data will allow the research team to apply for external funding to explore the relationship of mental health and grief within a larger pre-health professional student population.
Depression
The relationship between age and depression is complex and not yet fully understood. In the present study, age is the only significant variable associated with depression. Participants aged 25 to 49 and participants aged 50 to 64 both reported lower levels of depression than participants aged 18 to 24. These results suggest that older students are less susceptible to depression, consistent with the National Institute of Mental Health (NIMH, 2022) and other studies reporting that older age is a buffer against depressive symptoms in specific communities (Lara-Cinisomo et al., 2023).
One possible explanation for our findings is that older individuals develop more robust and stable social support networks that protect them from depression (Chao et al., 2018; Gariépy et al., 2016; Tang et al., 2022; Turner et al., 2022). However, this hypothesis requires further research to understand this relationship's mechanisms.
It is important to note that Stordal et al. (2003) reported increased depression among older individuals, which contrasts with our findings. While our study offers interesting findings, more research is needed to understand the complex relationship between age and depression. Future studies could investigate the role of social support and other factors that may contribute to lower levels of depression among older individuals.
Anxiety
A considerable number of UMA students (81%) work to support their studies. Many of these students also have technical careers in the same fields as their professional studies. This intersection of technical and academic activities is particularly evident in nursing, where many students also work as technicians. These students were particularly exposed to frontline work during the COVID pandemic. Under this context, we might understand the results from the present study that showed that nursing students reported higher anxiety levels than pharmacy students. It has been reported that nurses are among the most affected health workers regarding mental health, especially anxiety and burnout (Søvold et al., 2021), because of the exposure, workload, and stigma they experience. A proportion of nursing students in the context of our study that also works as nursing technicians may have experienced the same levels of exposure as professional nurses, leading to our results. It is important to note that pharmacy students also had a degree of exposure during the COVID pandemic. The proportion of pharmacy students that worked during the COVID pandemic is similar to that of nursing students. However, the nature of the work is different, even though both are in hospital settings.
Furthermore, the specific difference in anxiety between nursing and pharmacy students has been underexplored. A recent study has compared anxiety in pharmacy and medical students, but little research has shown a comparison between pharmacy and nursing students (Fischbein & Bonfine, 2019). Future studies should further explore these differences to test if our results were due to contextual factors or inherent differences in the study programs.
Another noteworthy result showed that participants who identified as White reported higher levels of anxiety than participants who identified as Mestizo. Reports from other countries showed that the Hispanic and Mestizo populations showed higher probabilities of developing anxiety than the White population (Nguyen et al., 2022). Nevertheless, in those reports, the Mestizo and Hispanic populations are ethnical minorities. In the Peruvian context, Mestizo population represents 60.2% of the ethnical representations (Instituto Nacional de Estadísticas e Informática, 2018). This fact is insufficient to affirm that the White population, a racial minority in Peru, was prone to develop more anxiety than Mestizos. Moreover, we could not find reliable statistics on ethnical differences in anxiety for Peruvian population. In consequence, it is necessary to investigate further the ethnical differences in mental health problems in Peru to better understand the results found in the present research.
Stress
The literature reports that there are gender differences in perceived stress between men and women, indicating that women are in danger of reporting higher levels of stress (Graves et al., 2021). The present research found a similar result; women reported higher stress levels than males. These consistent results confirm that gender is a risk factor that should be considered when designing programs to address the impacts generated by the COVID pandemic. Our model also showed that no other sociodemographic variable has a significant association with stress.
Coping
One of the main findings for coping was related to the moderation effect of significant loss and COVID contagion. These results show that students that were infected with the virus and lost a significant person during the pandemic reported higher levels of coping. One possible explanation for this association is that some people experience personal growth after adverse experiences (Tedeschi & Calhoun, 1996), which also increases resilience and coping. Thus, it is possible that part of our sample had personal characteristics that led them to increase their coping styles after the death of their significant ones. Luo et al. (2022) reported that among medical students, posttraumatic growth was more prevalent in students who established supportive social networks and were cognitively flexible. However, it is impossible to test this hypothesis in the present research, so we recommend that future research address this specific idea.
Female participants also reported significantly lower levels of coping than male participants, which is supported by extant literature (Graves et al., 2021). In contrast, married and single participants reported higher levels of coping than divorced participants, consistent with the literature. This study reveals new findings related to coping and COVID. Participants with higher levels of income (>$12,000 a year), participants who reported having two doses of the COVID vaccine, and participants who self-identified as religious all reported higher levels of coping than their counterparts.
Grief
The COVID pandemic is one of the largest health crises in contemporary history (Albuquerque et al., 2021), generating more than 526 million diagnosed cases and more than 6.2 million deaths (WHO, 2022). Notably, Latin America has experienced more than 3.5 million deaths (Caycho-Rodríguez et al., 2021). Ethnic identifications played a role in higher levels of grief with Mestizo participants reporting higher levels of grief than White participants and Quechua participants reporting higher levels of grief than Mestizo participants. Single participants showed higher levels of grief than divorced participants. Participants with incomes >$12,000 a year reported higher levels of grief than those below that income threshold. Religious participants reported higher levels of grief than nonreligious participants. Those with at least one vaccine dose and those with a booster showed lower levels of grief than participants with no vaccines. And finally, participants who reported a significant loss due to COVID reported higher levels of grief. These findings are new and add to the growing body of literature exploring the COVID pandemic.
Limitations
There are limitations to this study. One important limitation for the study is the unknown baseline of participants’ current and prior mental health challenges. In this study, a convenience sample was used, which may impact representativeness of the population and generalizability of the findings. Virtual access to the population via email recruitment may have impacted the number of participants reached and recruited for the study.
Interpretation
This study took place at the end of 2021 and the beginning of 2022, during the outbreak of the omicron variant, which began the third wave of the COVID pandemic. It was a time of heightened stress as both vaccinated and unvaccinated individuals began quickly and more easily contracting and spreading the new variant, which was associated with increased severity of illness (CDC, 2022). It is important to note that there were several sociodemographic variables associated with depression, anxiety, stress, grief, and coping; all these variables should be considered when addressing the problems generated by the COVID pandemic. Especially regarding interventions and social services in the university, they should be oriented toward the most vulnerable populations identified in the present research. Interventions should also be oriented toward personal growth as it might be an essential predictor of coping. Thus, the importance and interpretation of the research findings are intimately connected to the context and timeframe of data collection. This research study is also notable in that it is an international study with attention to cultural considerations, and its findings have the potential to transcend culture while also identifying commonalities among various cultures.
Generalizability
Due to the sample population and the potential for selection bias, generalizability to the wider pre-health population may be impacted. A future research study that includes a larger, more representative sample population is needed to improve generalizability of the research findings. This will potentially allow for a broader understanding of the impact of COVID on mental health challenges and grief.
Summary
At the time the study was conducted, it was the first to explore and analyze nursing and pharmacy students’ perceptions on how the COVID pandemic impacted their mental health and grief, making this study novel. Furthermore, the interrelationships between depression, anxiety, stress, coping, and grief continue to be underexplored. The findings from this study may serve to inform future research aimed at improving pre-health professional students’ mental health support. The next steps for future research may include the exploration of the relationship between resilience and grief and resilience and mental health. If positive relationships exist, targeted initiatives to foster resilience and support mental health may help to improve the students’ social–emotional and mental health throughout their programs of study.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.