
Abstract
Oral feeding is a complex multidimensional process that preterm infants often face challenges achieving due to their immaturity, medical complexity, and environmental influences in the neonatal intensive care unit. The objective of this study is to describe a framework and clinical guide of the oral feeding process. Evidence from current literature on preterm infant oral feeding was synthesized and integrated. The proposed framework identifies core skills (sucking, swallowing, breathing, and aerodigestion), which are influenced by intrinsic factors (musculoskeletal, respiratory, cardiovascular, gastrointestinal, sensory, and neurological) and extrinsic factors (physical surroundings, policies, parent attributes, health care provider, and feeding equipment). The framework and clinical guide offer an evidence-based approach for understanding oral feeding in preterm infant. Recognizing oral feeding as a multidimensional occupation enables occupational therapists to address the range of factors influencing infants’ oral feeding performance.
Introduction
For all infants, oral feeding by breast or bottle is a fundamental occupation needed for their growth and development (Viswanathan & Jadcherla, 2020). However, for preterm infants born before 34 weeks’ gestation, achieving oral feeding competence is often a challenge due to their neurophysiologic immaturity, medical complexity, and environmental influences related to the neonatal intensive care unit (NICU; Bolea et al., 2025; Casey et al., 2018; Crapnell et al., 2013; Griffith et al., 2019; Park et al., 2015; Viswanathan & Jadcherla, 2020). Up to 40% of preterm infants may experience oral feeding difficulties, such as a disorganized sucking pattern and uncoordinated suck–swallow–breathe, which impede on their ability to achieve independent oral feedings (Dodrill et al., 2008; Hawdon et al., 2000; Jadcherla et al., 2010; Lau, 2016; Muir et al., 2022). Consequently, this prolongs their hospitalization, increasing parent stress, and raising their risk of long-term neurodevelopmental disabilities (Aagaard et al., 2015; Dodrill et al., 2008; Ionio et al., 2019; Li et al., 2020; Medoff-Cooper et al., 2009; Mizuno & Ueda, 2005; Muir et al., 2022; Yi et al., 2019).
Several recent surveys revealed that management of oral feeding in preterm infants in the NICU is often the role of the occupational therapist(s) acting either individually or as part of multidisciplinary team (Alguire et al., 2025; Borges Nery et al., 2019; Hardy et al., 2018). Furthermore, these surveys demonstrated that most occupational therapists conceptualize oral feeding primarily in terms of the infant’s ability to coordinate the suck–swallow–breathe sequence only and commonly use oral feeding protocols, such as cue-based feeding or custom unit-based guidelines to manage oral feedings (Alguire et al., 2025; Borges Nery et al., 2019; Hardy et al., 2018). However, these approaches are used without a clearly defined overarching framework and concentrate mainly on infants’ intrinsic abilities (Alguire et al., 2025; Borges Nery et al., 2019; Hardy et al., 2018).
Research demonstrates that oral feeding is a complex, multidimensional occupation influenced by both intrinsic neurophysiologic systems and extrinsic environmental factors (Bolea et al., 2025; Briere et al., 2015; Casey et al., 2018; Crapnell et al., 2013; Fucile et al., 2022; Hwang et al., 2013; Kowalska et al., 2025; Park et al., 2015; Pickler et al., 2013; Silberstein et al., 2009). For occupational therapists to effectively assess and treat oral feeding in preterm infants, a sound understanding of the underlying intrinsic and extrinsic factors is needed. An oral feeding framework may help occupational therapists acquire this knowledge. In this article, we will extend on a conceptual model that we previously published incorporating recent published research that is important for clinical practice (Fucile et al., 2020). Therefore, the aims of this article are to (a) describe the underlying intrinsic and extrinsic factors affecting oral feeding performance, (b) present an updated framework of the underlying factors involved in the oral feeding process, and (c) provide an updated clinical guide for occupational therapists to utilize when managing oral feedings in preterm infants.
Oral Feeding Process
The occupational therapy practice framework: Domain and Process 4th Edition identifies feeding as an occupation essential to health and participation in infants. Based on this model, the oral feeding process entails performance skills, including motor, sensory, and regulatory capacities and is influenced by intrinsic and extrinsic factors. For preterm infants, the oral feeding process entails sucking on bottle or breast safely and efficiently (Gewolb & Vice, 2006; Lau, 2016; Muir et al., 2022; Viswanathan & Jadcherla, 2020). Safe and efficient oral feeding is defined as the ability of the infant to complete the prescribed volume of milk with no adverse events, including episodes of apnea, bradycardia, and oxygen desaturation and with adequate weight gain.
To achieve safe and efficient oral feeding requires coordination of sucking, swallowing, and breathing as well as proper aerodigestive functions (Gewolb & Vice, 2006; Qiu & Hu, 2023; Sakalidis & Geddes, 2016; Viswanathan & Jadcherla, 2020). Sucking comprises two components: suction and expression (Lau, 2016). Suction is the negative intraoral pressure created by the lips tightening around the breast or bottle, the soft palate raises to block off the nasal passages, and the jaw lowering. Expression is the positive intraoral pressure created by the stripping of the tongue against the nipple and hard palate (Lau, 2016; Lau et al., 2003; Mizuno & Ueda, 2003; Pineda et al., 2020; .
Swallowing involves the transport of a bolus of milk from the oral cavity to the stomach (Gewolb & Vice, 2006; Lau, 2016; Viswanathan & Jadcherla, 2020). The swallow process is divided into three phases: oral, pharyngeal, and esophageal. In the oral phase, the bolus is formed and pushed onto the posterior wall of the oropharynx by the tongue to initiate the swallow. In the pharyngeal phase, the bolus travels from the pharynx to the esophagus; the soft palate rises to block the nasal passage, while the epiglottis covers the larynx to protect the airway. In the esophageal phase, the bolus is transported from the esophagus to the stomach for digestion and absorption. The key features of this phase include effective peristalsis and airway protection (Gewolb & Vice, 2006; Jadcherla et al., 2025;; Lang et al., 2016; Lau, 2016; Sultana et al., 2021; Viswanathan & Jadcherla, 2020).
Aerodigestion is an equally important supportive function of the esophagus in the oral feeding process (Jadcherla et al., 2025; Lang et al., 2016; Sultana et al., 2021). Aerodigestion is the integrated function of the esophagus in coordinating both digestive (bolus transport and reflux clearance) and aerodigestive protective (airway protection and aspiration prevention) mechanisms (Jadcherla et al., 2025; Lang et al., 2016; Sultana et al., 2021). Aerodigestive protection refers to the function of the esophagus involved in the neuromuscular coordination and antireflux defense mechanisms. Several esophageal and airway reflexes, mediated by vagal afferent and efferent pathways, ensure safe swallowing and prevent aspiration (Hasenstab-Kenney et al., 2020; Jadcherla et al., 2025; Lang et al., 2016; Sultana et al., 2021). The airway reflexes are coordinated to promote downward bolus movement, prevent retrograde flow, enhance esophageal clearance, and maintain airway integrity. Notably, glottal closure, triggered by pharyngeal or esophageal stimuli, is essential in preventing pulmonary aspiration (Hasenstab-Kenney et al., 2020; Jadcherla et al., 2025; Lang et al., 2016; Sultana et al., 2021).
Respiration involves gas exchange to maintain a balance of oxygen and carbon dioxide in the blood to meet infants’ changing metabolic needs (Hasan et al., 2020; Mayerl et al., 2019; Viswanathan & Jadcherla, 2020). Respiration is always interrupted when swallow occurs (Lau, 2016). With an increase in the occurrence of swallows during oral feeding, there is a change in respiratory status (Bamford et al., 1992; Vice & Gewolb, 2008). Specifically, there is a marked decrease in minute ventilation and oxygenation, associated with an increase in respiratory frequency, a reduction in inspiratory tidal volume, and a decrease in inspiratory time (Vice & Gewolb, 2008). These changes are prominent during the initial continuous period of sucking. However, during the intermittent sucking period, recovery of minute ventilation and oxygenation generally occurs (Bamford et al., 1992; Lau et al., 2003; Mizuno & Ueda, 2003; Sakalidis & Geddes, 2016; Vice & Gewolb, 2008).
Oral Feeding Framework
The oral feeding framework presented in this article is an updated version of our previous model, incorporating new evidence on aerodigestive function, the sensory system, feeding equipment, and parent–infant bonding. We conducted a narrative literature review, with support from an expert librarian, to ensure a comprehensive and up-to-date synthesis of the evidence. A narrative review was selected because it allows for a broad and integrative examination of the literature to capture the most current developments in the field (Pare, 2016).
The achievement of safe and efficient oral feeding necessitates the generation and integration of sucking, swallowing, breathing, and aerodigestion. The generation and coordination of these functions depends on the maturation and precisely timed interaction of a multitude of intrinsic and extrinsic factors (Bolea et al., 2025; Briere, McGrath, et al., 2015; Casey et al., 2018; Crapnell et al., 2013; Fucile et al., 2022; Griffith et al., 2019; Park et al., 2015). Figure 1 illustrates an oral feeding framework displaying the intrinsic and extrinsic underlying factors involved in the oral feeding process.
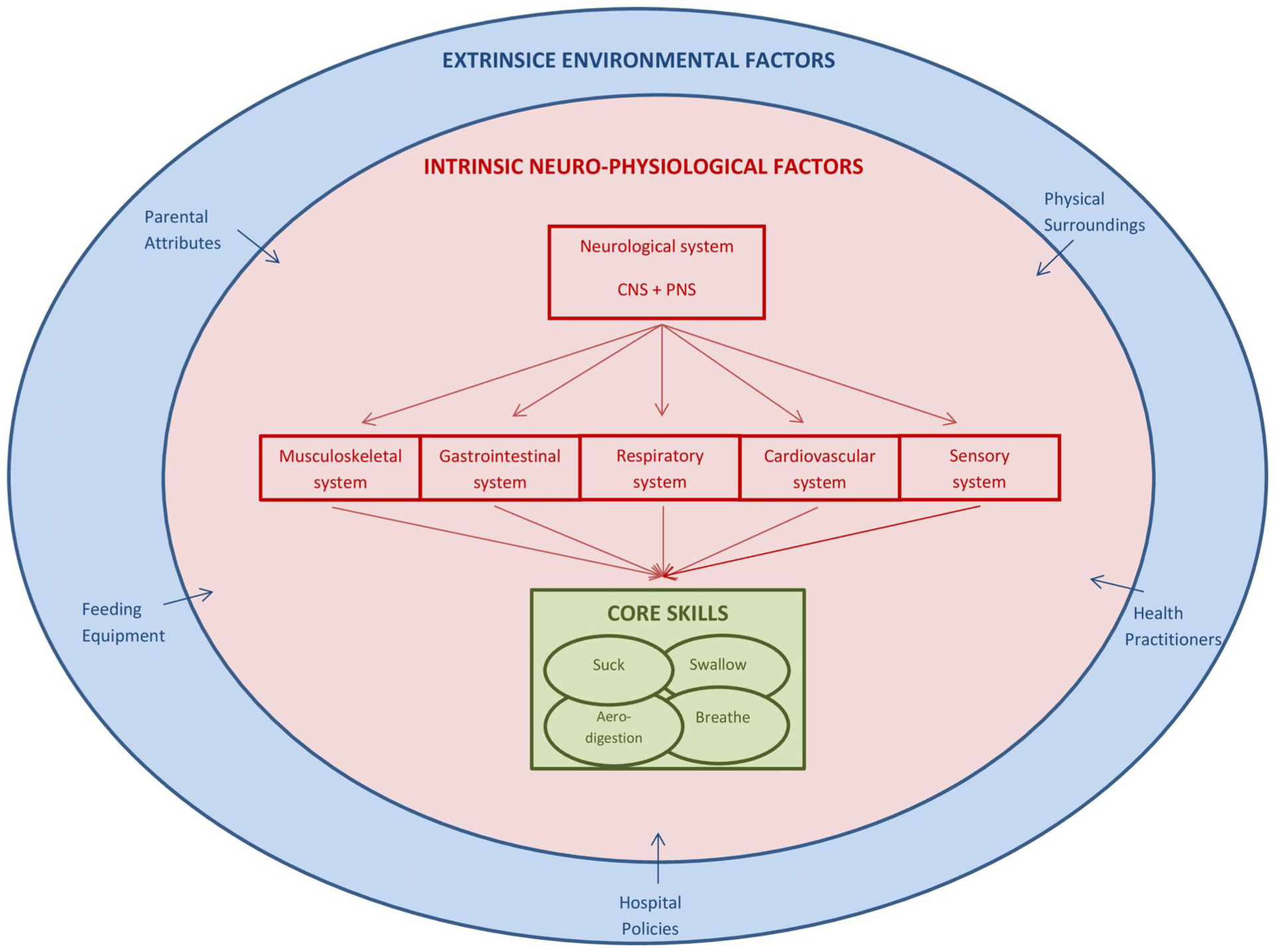
Oral Feeding Framework.
Intrinsic Neurophysiological Factors
The following section explains the intrinsic neurophysiological systems required in the oral feeding process, demonstrated in Figure 1. The musculoskeletal system encompasses the anatomical structures, muscles, and motor control necessary for producing suck, swallow, breathe, and aerodigestion (Kowalska et al., 2025; Lau, 2016; Park et al., 2015; Viswanathan & Jadcherla, 2020). The anatomical structures consist of the nose, mouth, pharynx, larynx, trachea, esophagus, stomach, and lungs. Numerous muscles contribute to the processes of sucking, swallowing, breathing, and aerodigestion, including those found in the cheeks, lips, tongue, pharynx, esophagus, and abdomen. Adequate motor control for postural alignment plays a crucial role in oral feeding (Kowalska et al., 2025; Mizuno et al., 2000). Specifically, head stability and alignment of the neck and trunk are important for the generation of sucking and swallowing (Wahyuni et al., 2025). The physiologic flexion posture, which includes ability to maintain the arms near midline, flexing the hips and knees, and flexing the head and neck, provides a stable foundation for effective sucking, swallowing, and breathing (Crapnell et al., 2015; Fucile et al., 2011, 2012; Wahyuni et al., 2025).
The gastrointestinal system is responsible for digesting food, absorbing nutrients, and expelling waste. The components of the gastrointestinal system include the mouth, pharynx, esophagus, stomach, small intestine, colon, and rectum. Effective oral feeding depends on the proper anatomical and physiological development of the upper and lower esophageal sphincters, esophageal peristalsis, aerodigestive protection function, gastric emptying, and intestinal motility (Viswanathan & Jadcherla, 2020). An immature gastrointestinal tract can contribute to oral feeding difficulties in this population. In preterm infants, the esophagus shows reduced propagation speed and extended contraction duration compared with term infants. In addition, the tone of the lower esophageal sphincter is reduced in preterm infants, which gradually reaches adult levels at full-term age (Jadcherla et al., 2025; Sultana et al., 2021; Viswanathan & Jadcherla, 2020). Both the incomplete development of esophageal peristalsis and decreased sphincter tone contribute to ineffective aerodigestive protection functions consequently, resulting in the development of gastroesophageal reflux (GER) (Jadcherla et al., 2025; Sultana et al., 2021; Viswanathan & Jadcherla, 2020). GER in infants may present with symptoms such as frequent vomiting, coughing, episodes of apnea, slowed heart rate (bradycardia), aspiration, and refusal to feed all of which affect oral feeding performance (Hasenstab-Kenney et al., 2020; Jadcherla et al., 2025; Sultana et al., 2021; Viswanathan & Jadcherla, 2020). Furthermore, delayed gastric emptying and disorganized or immature motility of the small intestine, which are more commonly seen in preterm infants can result in larger amounts of gastric content remaining in the stomach (Jadcherla et al., 2025; Sultana et al., 2021; Viswanathan & Jadcherla, 2020). This, in turn, often presents as feeding intolerance in preterm infants (Jadcherla et al., 2025; Sultana et al., 2021; Viswanathan & Jadcherla, 2020).
The respiratory system is responsible for bringing oxygen into the body and for expelling carbon dioxide and cellular waste from the body’s cells, which are essential for organ function. The structures that make up the respiratory system include the nose, pharynx, larynx, trachea, bronchi, and lungs (Viswanathan & Jadcherla, 2020). Precise coordination between swallowing and breathing is crucial to safeguard the airway (Gewolb et al., 2001; Viswanathan & Jadcherla, 2020). Research has indicated that full-term infants follow the most protective pattern of swallow–breathing coordination during oral feeding, which involves inhalation, followed by swallowing, and then exhalation (Gewolb & Vice, 2006; Lau et al., 2003; Mayerl et al., 2019, 2020). This sequence is considered the safest because it ensures that milk is cleared from the shared pharyngeal space lowering the likelihood of aspiration. However, this optimal swallow–breathing pattern is not typically developed until after full-term age. In preterm infants <34 weeks gestation, the most common patterns involve swallowing during extended breathing pauses (known as apneic swallows) or swallowing during inhalation (Gewolb & Vice, 2006; Lau et al., 2003; Mayerl et al., 2019, 2020; Mizuno & Ueda, 2003). The latter may help explain why preterm infants experience higher rates of aspiration than full-term infants. The timing and frequency of swallowing also influence breathing rate and oxygenation. During feeding, full-term infants demonstrate an initial phase of continuous sucking with long bursts, followed by intermittent sucking with multiple swallows. Minute ventilation and oxygen levels decline during the continuous phase but typically recover during the intermittent phase. Preterm infants similarly exhibit an early continuous sucking phase followed by intermittent sucking during oral feeding (Kron, 1996; Medoff-Cooper et al., 2002). However, their sucking bursts are shorter during the continuous phase, and minute ventilation only partially recovers during the intermittent phase (Kron, 1996; Medoff-Cooper et al., 2002). As a result, preterm infants often demonstrate difficulty sustaining adequate respiration, presenting clinically as apnea, bradycardia, and oxygen desaturation (Gewolb & Vice, 2006; Lau et al., 2003; Mayerl et al., 2019, 2020; Mizuno & Ueda, 2003; Pineda et al., 2020).
The cardiovascular system is made up of the heart, arteries, and veins that transport blood to and from the heart. Within this system, the heart functions as a pump that works in tandem with the respiratory system; both the heart and lungs must operate together to deliver oxygenated blood to body tissues and remove carbon dioxide through respiration. During oral feeding, it is essential that the cardiovascular system functions efficiently to supply the oxygen required to sustain oral feeding (Clemente et al., 2001; Imms, 2001; Pereira et al., 2015; Viswanathan & Jadcherla, 2020). An underdeveloped cardiovascular system has been linked to decreased oral feeding efficiency (mL/min), shorter sucking bursts, longer pauses between sucking bursts, and reduced milk consumption (Hasenstab-Kenney et al., 2020; Pereira et al., 2015; Suess et al., 2000). Furthermore, the actions of sucking, swallowing, and breathing require energy expenditure. Due to the immaturity of their cardiovascular system, preterm infants tend to have limited endurance and become fatigued quickly (Clemente et al., 2001; Fucile et al., 2005; Lau & Smith, 2011). Fatigue becomes a concern in this population when they are unable to consume an adequate volume of milk before tiring.
The sensory system refers to the interconnected processes through which an infant receives and interprets sensory information, maintains physiological stability, and organizes behavioral responses during oral feeding (Pineda, 2016; Pineda et al., 2023). For preterm infants, whose neurological and sensory systems are still developing, this system plays a central role in oral feeding readiness and competence (Pineda, 2016). Specifically, sensory regulation involves how the infant processes tactile, gustatory, olfactory, proprioceptive, and vestibular input encountered during oral feeding, such as the feel of the nipple, the taste and smell of milk, and the sensations associated with holding and positioning (Pineda, 2016; Pineda et al., 2023). Physiological regulation encompasses the infants ability to sustain stable autonomic functions (e.g., heart rate, respiratory rate, oxygen saturation) in response to sensory experiences and is important for the core feeding skills of aerodigestion and suck–swallow–breathe processes (Hasenstab-Kenney et al., 2020; Sakalidis et al., 2013; Sakalidis & Geddes, 2016; Vice & Gewolb, 2008). Behavioral regulation reflects the infant’s capacity to manage arousal and state transitions, demonstrate hunger and engagement cues, and signal stress or disengagement when overwhelmed by the sensory inputs (Byers, 2003; Pickler et al., 2005). Together, these components influence whether an infant can integrate sensory experiences and maintain physiological stability and an optimal behavioral state during oral feedings.
The neurological system is a key system involved in oral feeding. The function and interaction of the previously mentioned musculoskeletal, gastrointestinal, respiratory, cardiovascular, and sensory systems are dependent on the degree of maturity of the neurological system. At the peripheral nervous system level, the oral, nasal, pharyngeal, laryngeal, and tracheal structures are primarily innervated by motor and sensory branches of cranial nerves V, VII, IX, X, and XII, as well as branches from the upper cervical roots C1–C 5 (Barlow, 2009). In addition, the neck, shoulder girdle, heart, lungs, and digestive organs are innervated by the upper cervical roots and cranial nerve X. At the level of the central nervous system, the brainstem governs neurological functions of respiration, digestion, heart rate, and arousal (behavioral state). The brainstem, particularly the pons and medulla, is critical for suck–swallow–breathe coordination (Barlow, 2009). Most afferent inputs related to sucking, swallowing, and breathing are processed in the nucleus of the tractus solitarius, and the efferent controls are primarily located in the nucleus ambiguous (Barlow, 2009). The extensive overlap between peripheral and central neural control forms the foundation for the reciprocal influences among suck, swallow, and breathe (Barlow, 2009). It is further theorized that the rhythmic patterns of sucking, swallowing, and respiration originate within the brainstem (pons and medulla) through neural circuits known as central pattern generators (CPGs) (Barlow, 2009). These CPGs are conceptualized as flexible, organized neural networks comprising multifunctional nerves responsible for specific motor behaviors. It is proposed that CPGs coordinate not only the individual activities of sucking, swallowing, and breathing but also the precise neural integration among all three processes. The integration of afferent sensory feedback into these CPGs enables rapid adaptation to external disturbances in the oral, pharyngeal, laryngeal, and respiratory regions (Barlow, 2009). Therefore, mature sensory and motor neural connections are essential for establishing and sustaining suck–swallow–breathe coordination.
Extrinsic Environmental Influences
The following section describes the extrinsic environmental factors for safe and efficient oral feeding process in preterm infants, illustrated in Figure 1.
Research on extrinsic environmental factors suggests that elements of the physical surrounding in the NICU, such as ambient noise, lighting levels, and the structural layout of unit, can affect oral feeding performance by causing distractions and undue stress for infants (Hernández-Salazar et al., 2020; Pickler et al., 2013; Sankar et al., 2022). Exposure to high noise levels and intense lighting in the NICU has been found to be physiologically stressful for preterm infants, leading to increased heart and respiratory rates and changes in behavioral state (Hernández-Salazar et al., 2020; Pickler et al., 2013; Sankar et al., 2022). In addition, the structural design of the NICU itself can have an impact on feeding outcomes (Casey et al., 2018). Traditionally, many NICUs have followed an open-bay design, which, due to its lack of separation, exposes infants to greater environmental stimuli like loud sounds and bright lights. More recently, there has been a shift toward the use of single-family rooms. Studies have shown that this single-room layout is associated with improved oral feeding outcomes, likely due to a reduction in environmental distractions (Cheong et al., 2020).
The NICU policies, which are often reflected in their standard care plans, feeding practices, visitation rules, and hospital discharge criteria, may influence an infant’s oral feeding outcomes. Research suggests that standard care plans emphasizing family-centered practices, particularly those that encourage early family engagement with the infant, can reduce parental stress and enhance infants’ oral feeding abilities (Melnyk et al., 2006; Nieves et al., 2021; O’Brien et al., 2018). The oral feeding practices within the NICU can significantly affect oral feeding outcomes, particularly regarding the timing of initiation and the progression of feedings (McCain, 2003; McFadden et al., 2021). Specifically, units may follow scheduled feedings, demand/cue-based feeding, or semi-demand feeding. Among these three feeding approaches, current research provides the strongest support for demand/cue-based feeding, demonstrating that it can lead to a faster transition to full oral feeding, reduce feeding intolerance, and promote parental involvement (McFadden et al., 2021; Ofek Shlomai et al., 2024; Whetten, 2016).
Several NICUs across North America have adopted, either fully or in part, the Baby-Friendly Hospital Initiative, which prioritizes exclusive breastfeeding. In NICU settings, implementation of the Baby-Friendly Hospital Initiative has been associated with increased breastfeeding initiation and exclusivity at hospital discharge, along with reduced formula during and after hospitalization (Abugov et al., 2021; do Nascimento & Issler, 2005; Nyqvist et al., 2013). Some neonatal units have adopted Kangaroo Care as part of their standard practice, given its well-documented benefits for both infants and parents (Ciochetto et al., 2023). Research shows that Kangaroo Care enhances parental mental health, supports breastfeeding success, and promotes infant weight gain (Ciochetto et al., 2023). NICU visitation rules can also significantly influence oral feeding outcomes. Studies indicate that implementing open 24-hr visitation improves both infant and parent outcomes by providing greater flexibility for family involvement in care (O’Brien et al., 2018). In many NICUs, a hospital discharge requirement is that infants must be able to complete all oral feeds independently without any adverse events. Given that achieving oral feeding competency is a necessary milestone for hospital discharge, NICUs often adjust their feeding practices to facilitate earlier hospital discharge. These adjustments may include favoring bottle feeding over breastfeeding, as bottle feeding is erroneously perceived to promote a faster transition to independent feeding (Briere et al., 2015, 2016).
The NICU environment often limits early bonding due to physical separation, which may disrupt the development of secure parent–infant attachment (Feeley et al., 2016; Pickler et al., 2013; Pineda et al., 2025). Early, consistent, and emotionally attuned parent–infant interactions are foundational for their attachment, and to support the infant’s capacity for sensory regulation, physiological stability, and behavioral organization, for successful oral feeding (Cheng et al., 2021; O’Brien et al., 2018; Pineda et al., 2018; Xie et al., 2019). Disruptions in parent–infant bonding or limited parental engagement may, therefore, interfere with the dyad’s ability to establish the rhythmic, reciprocal interactions needed for effective oral feeding. Conversely, promoting early parental involvement in infant care has been shown to positively influence oral feeding outcomes (Cheng et al., 2021; O’Brien et al., 2018; Pineda et al., 2018; Xie et al., 2019). Such involvement strengthens parent–infant bonding, enhances parents’ confidence and emotional attunement, and reduces their anxiety, thereby supporting more responsive, and successful oral feeding interactions (Hernández-Salazar et al., 2020; Pickler et al., 2013; Sankar et al., 2022).
Health care providers can have a significant impact on an infant’s oral feeding performances. Variability in the neonatal team has been associated with increased parental stress (Fucile et al., 2023). Maintaining consistency among team members may enhance the NICU experience for families. Moreover, a multidisciplinary and family-centered approach to managing oral feeding within the unit has been associated with numerous benefits (Hardy et al., 2018). Such an approach not only promotes coordinated care but also empowers parents, enhances their understanding of feeding cues and strategies, and ultimately contributes to more successful oral feeding outcomes (Hardy et al., 2018; Wakeham et al., 2024).
There is strong evidence demonstrating that the type of feeding equipment used to feed the infant, including direct breastfeeding tools, artificial nipple features, type of bottle, and thickening of milk may affect infants’ sucking, swallowing, breathing, and aerodigestion functions during oral feeding. For direct breastfeeding, nipple shields are often recommended for preterm infants who struggle to latch properly due to factors such as underdeveloped oral motor structures and respiratory difficulties (Kair et al., 2015; Maastrup et al., 2014; Nyqvist et al., 2013). Positive breastfeeding outcomes have been reported for nipple shield use with preterm infants, including increased duration of sucking as well as improved milk transfer and volume of milk intake. In addition, having breast pumps and designated pumping areas within the NICU supports mothers in maintaining their milk supply and helps promote successful transition to oral feeding (Kair et al., 2015; Maastrup et al., 2014; Nyqvist et al., 2013).
For bottle feeding, various attributes of the nipples (such as hole type, shape, material, firmness, and flow rate) and bottle (shape, standard or vacuum free) contribute to oral feeding performance. With regard to the nipple, there are five-hole types; these include traditional single round hole, cross-cut opening, y-shaped opening, slotted, and antivacuum nipples. Several studies have shown that the nipple hole type influences the sucking pressure generated, rate of milk flow, amount of milk ingested, and overall physiological stability of the infant, but the evidence on which type is safest for preterm infants varies (Cresi et al., 2024; Perrella et al., 2019). Nipple shapes generally fall into three categories: standard, breast-like, and orthodontic. Like nipple hole type, the shape effects oral feeding performance (Ziegler et al., 2020). The material and firmness of the nipple also impact oral feeding performance (Zimmerman & Barlow, 2008). Most nipples are made from latex or silicon with varied firmness ranging from soft, standard, or medium, to firm. Medium or firm nipples are preferred since they help the infant’s tongue latch properly and provide better control over milk flow (Scheel et al., 2005). There are three nipple flow rates, including slow, medium, and fast. Nipple flow rate refers to the volume of liquid delivered per unit of time and is influenced by nipple design and material, with substantial variability reported even within the same labeled flow category. Slow or medium flow nipples are generally recommended for infants because they support physiological stability, accommodate immature suck–swallow–breathe coordination, allow adequate time for bolus formation and airway protection, and reduce the risk of choking and aspiration (Pados, 2021; Scheel et al., 2005). Faster flow rates can overwhelm oral motor control and respiratory regulation, particularly in preterm, whereas slower flow rates promote self-regulation and safer feeding (Pados, 2021; Scheel et al., 2005). Optimal nipple flow should, therefore, be determined based on infant-specific feeding skills, and physiological responses rather than age or product labeling alone.
The type of bottle used can significantly influence an infant’s feeding effectiveness. Bottles that eliminate hydrostatic pressure and minimize negative pressure allow infants to better regulate milk intake, resulting in faster milk transfer, shorter feeding times, greater intake, and improved safety (Fucile et al., 2009; Lau et al., 2015). Several designs achieve this, including controlled-flow vacuum-free bottles, vented systems that allow air entry during feeding, gravity-flow bottles requiring minimal suction, and breast-like nipples with anticolic or one-way airflow valves. Some are also adapted for side-lying feeding with pressure-regulating vents. Collectively, these designs support a more physiologically appropriate feeding experience by reducing the effort needed to extract milk (Cresi et al., 2024).
Thickening of milk for preterm infants is sometimes used to manage gastroesophageal reflux or difficulties with controlling the flow of milk out of the nipple during oral feeding (Gulati & Jadcherla, 2019; Jadcherla et al., 2025; Mizuno et al., 2002; September et al., 2014; Sultana et al., 2021). Gastroesophageal reflux is common in preterm infants due to the immaturity of the lower esophageal sphincter and delayed gastric emptying, which can lead to frequent regurgitation, discomfort, and sometimes feeding intolerance (Gulati & Jadcherla, 2019; Jadcherla et al., 2025). Difficulty controlling milk often reflects immature oral motor skills or poor suck–swallow–breath coordination, which can result in coughing, choking, or aspiration during oral feeding (Mizuno et al., 2002). Thickened milk is intended to slow the flow, improve bolus control, and reduce regurgitation, thereby facilitating safer and more efficient oral feeding (September et al., 2014). Instrumental swallowing assessments, such as video fluoroscopic swallow studies or fiberoptic endoscopic evaluation of swallowing, can be used to objectively identify aspiration risk, characterize swallowing physiology, and guide clinical decision-making regarding the need for and appropriateness of thickened liquids in this population. However, evidence regarding its effectiveness is mixed. Some studies suggest modest benefits in reducing regurgitation and improving oral feeding tolerance, while others highlight potential risks, such as altered nutrient absorption, delayed gastric emptying, or interference with micronutrient intake (Gulati & Jadcherla, 2019). Clinical guidelines, therefore, recommend cautious, individualized use, with careful monitoring of growth, tolerance, and overall feeding development.
Framework
An oral feeding framework is presented, in Figure 1, to provide a visual representation of the various factors influencing an infant’s ability to feed orally. The proposed framework is adopted from a previous conceptual model developed by the author (Fucile et al., 2020). In alignment with the OTPF-4, this framework reflects the dynamic interaction between the infant, their performance skills, the environment, and the feeding activity itself, emphasizing the holistic approach foundational to occupational therapy practice. This framework is intended for use with preterm infants in any hospital setting, including NICUs (Levels I–IV) and Special Care Nurseries. At the center of the framework, are the core feeding skills including sucking, swallowing, breathing, and aerodigestion. The successful execution of these skills depends on the proper functioning and integration of all intrinsic neurophysiologic systems. The neurological system governs and controls all the other intrinsic systems because the brain receives sensory input from the other intrinsic systems and environmental factors, integrates these inputs, and then sends motor signals back to the systems to carry out the response. For preterm infants, achieving safe and efficient oral feeding is a more gradual developmental process. This progression relies on the appropriate functioning and integration of intrinsic neurophysiologic systems, along with well-aligned extrinsic environmental factors. This framework elucidates the multiple interacting factors that influence oral feeding performance in preterm infants.
Clinical Guide
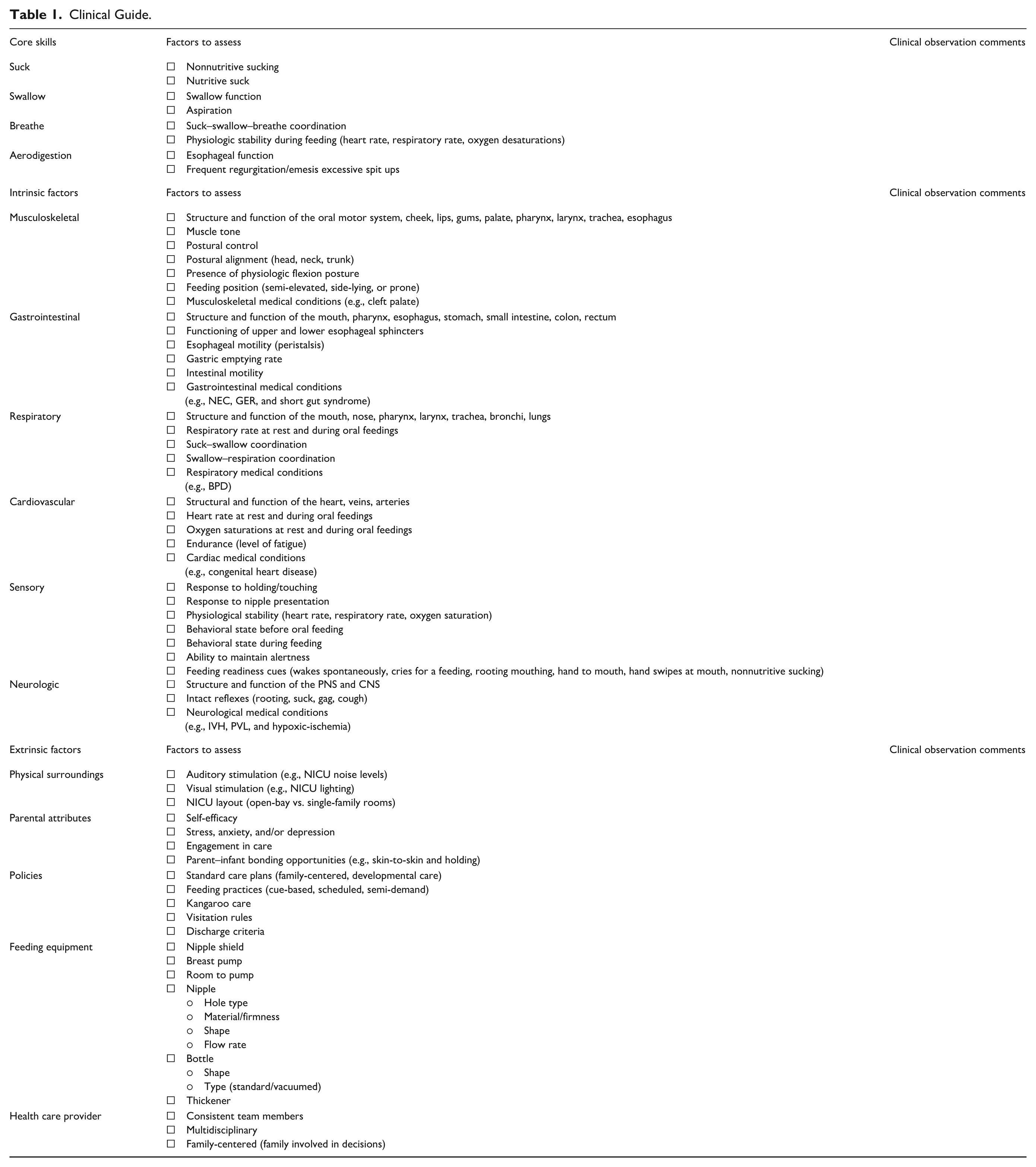
A clinical guide, is presented in Table 1, for oral feeding is provided to assist occupational therapists in managing the oral feeding performance of preterm infants in any hospital setting, including NICUs (Levels I–IV) and special care nurseries. This guide serves as a quick-reference tool, highlighting key factors to consider during assessment and treatment. It is important to note that this guide is not intended to function as a screening instrument or formal assessment tool but rather as an aid to help practitioners broaden their focus beyond the basic suck–swallow–breathe coordination pattern and recognize additional elements that may impact oral feeding competence in preterm infants.
Clinical Guide.
Conclusion
The oral feeding process is a complex, multidimensional activity influenced by a variety of intrinsic and extrinsic factors. An oral feeding framework and accompanying clinical guide are presented to support occupational therapists in identifying and addressing factors impacting oral feeding performance in preterm infants, enabling client-centered, developmentally supportive care to optimize outcomes.
Footnotes
Acknowledgements
The authors would like to thank the librarians at Queen’s University, for their assistance with the literature review.
Ethical Considerations
Ethical approval not applicable because this is a narrative review study.
Consent to Participate
Informed Consent also not applicable because this is a narrativereview study.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Not applicable because this is a review study.