
Abstract
Public safety personnel (PSP) have higher rates of work-related psychological injuries compared to the general public. Occupational therapists frequently provide rehabilitation and return to work (RTW) services for PSP. In order to understand the usage of occupational therapy (OT) treatment with psychologically injured PSP from British Columbia, Canada, a descriptive quantitative approach was used to explore summary data provided by WorkSafeBC (WSBC) for psychologically injured PSP who had an accepted mental disorder injury claim between 2019 and 2023, comparing those who received community OT treatment and those who did not. The data revealed that PSP with greater injury severity and longer lengths of time away from work more frequently received OT treatment as part of their WSBC mental disorder injury claim; it is possible that this higher degree of claim complexity influenced their RTW outcomes. Workers’ compensation organizations should review their RTW processes to ensure prompt access to relevant treatment and supports, including occupational therapy.
Plain Language Summary
Public safety personnel like police officers and firefighters have more work-related mental health issues than the general public. Occupational therapists often help these workers recover and return to work. This study aimed to understand how community-based occupational therapists are used to treat public safety personnel with work-related mental health issues in British Columbia, Canada. The study found that public safety personnel with more complex claims and more time off work were more likely to receive occupational therapy treatment. This claim complexity might affect their return to work success. Workers’ compensation organizations should review their return to work processes to ensure quick access to necessary treatments and support, including occupational therapy.
Introduction
Public safety personnel (PSP) are workers who ensure the safety and security of the public, including communicators/dispatchers, correctional workers, firefighters, paramedics, and police, among other personnel (Canadian Institute for Public Safety Research and Treatment [CIPSRT], 2023; Carleton et al., 2018). Exposure to potentially psychologically traumatic events, such as medical emergencies, threatened or actual physical assaults, fires/explosions, and critical incidents, put PSP at increased risk of work-related psychological injury—mental disorders or conditions attributed to exposure to one or more traumatic events (Carleton et al., 2018; CIPSRT, 2023). Symptoms of psychological injury most frequently include altered mood and cognition, sleep disturbances, and increases in general alertness or the sense of an imminent threat (Carleton et al., 2018; Gross et al., 2021). These symptoms can have a significant impact on individual functioning, contributing to reduced work performance and productivity, increased workplace safety risks, the need for time away from work, and decreased quality of life overall (Torchalla et al., 2019).
It is challenging to determine exactly how many PSP currently work in the Canadian province of British Columbia (BC), as PSP are employed by a variety of organizations across jurisdictions, and reporting may undercount workers who do not work full-time as well as those employed in support roles. In their 2021 national census, Statistics Canada reported almost 25,000 PSP working in full-time, full-year positions in BC, serving the province’s growing population of over 5,600,000 people (Statistics Canada, 2023).
In BC, workers who sustain a work-related injury can file a claim with WorkSafeBC (WSBC, 2025a), a provincial agency that upholds the province’s Workers Compensation Act. WSBC is funded by BC employers and provides no-fault, collective liability insurance for BC workers who have sustained injuries, illnesses, or diseases in the workplace. WSBC provides resources for injury prevention and workplace safety, coverage of health care and rehabilitation services costs post-injury, and wage loss benefits for workers injured in the workplace (WSBC, 2025a). Under section 135 (2) of the BC Workers Compensation Act, some workers who experience one or more traumatic work-related events, and are subsequently diagnosed with a mental health disorder, are eligible for worker’s compensation under the presumption that the disorder is work-related (King’s Printer, 2025). In 2018, the PSP included in this work-related injury presumption were correctional officers, firefighters, paramedics, police officers, and sheriffs, and in 2019 this was expanded to include communicators/dispatchers as well as wildland firefighters (WSBC, 2024a). In parallel, between 2019 and 2023, WSBC (2024a) saw an increase in allowed psychological injury claims in the presumption category (504 in 2019 versus 624 in 2023); however, this category includes workers beyond PSP, such as nurses and health care assistants. In 2023, WSBC (2024b) health care payments increased by $53 million CAD (12.5%), which was partially attributed to the increased use of occupational therapy (OT) and mental health services.
Many workers who make a psychological injury workers’ compensation claim will require time away from the workplace to recover from their injury, necessitating an eventual return to work (RTW). For example, in the last 5 years, 94% of psychological injury claims approved by WSBC (2025c) have involved time lost from work. Timely RTW has been shown to benefit workers’ physical and mental health, while protecting income, job security, employment benefits, social contacts, and general routine (WSBC, 2025b). Inability to work can exacerbate functional health concerns related to psychological injury and has been shown to contribute to behavioral disruption (e.g., sleep disturbances), lack of routine, as well as reduced self-efficacy and self-esteem (Figueredo et al., 2020). Inability to work can also create new life stressors, such as financial burden related to a lack of reliable and consistent income and/or related interpersonal conflict (Figueredo et al., 2020). Further, work leave due to psychological injury can impact the employer-employee relationship through real or perceived conflict related to work leave and/or altered workplace duties (Muijzer et al., 2011). The longer an injured worker is away from work, the less likely they are to return to employment, which is attributed to a myriad of factors (Canadian Centre for Occupational Health and Safety [CCOHS], 2022; Saskatchewan Workers’ Compensation Board, 2020).
Occupational therapists (OTs) are known to support the RTW journeys of PSP who have experienced psychological injury (Edgelow et al., 2023, 2024; Torchalla et al., 2019). Supporting a return to daily activities, developing RTW plans specific to the workplace requirements and the worker’s needs, and implementing cost-effective work accommodations are just some of the ways OTs may be involved in RTW (Canadian Association of Occupational Therapists [CAOT], 2018). WSBC (2025d) uses contracted OTs to visit injured workers in their home, community, and/or their workplace, to offer a spectrum of services during all stages of an active claim, including recovery, reintegration, and RTW. Contracted OTs can provide assessments of baseline function, implement a treatment plan to address barriers to function, increase safety and independence, and implement a RTW or stay-at-work plan, among other services (WSBC, 2025d). These services are tailored to the individual needs of the injured worker, and specific interventions provided by the OTs may include psychoeducation, activity engagement, social reintegration, work simulation and hardening, job coaching, and RTW planning (Edgelow et al., 2023b, 2024; Mackoff et al., 2025; Torchalla et al., 2019; WSBC, 2025c).
Despite the reported growing use of OT treatment with PSP in Canada (Edgelow et al., 2024; Edgelow & Fecica, 2025), no data specific to BC are currently available. Thus, the goal of the current study was to investigate the usage of OT treatment in accepted WSBC mental disorder injury claims for PSP in BC, using available data from between 2019 and 2023. This study, utilizing similar research objectives and methodology to the recent Edgelow and Fecica (2025) study on the usage of OT treatment within the Ontario workers’ compensation system, sought to answer three questions: What are the characteristics of PSP who received OT treatment as part of their WSBC psychological injury claim? How do their characteristics compare to those who did not receive OT treatment? How do the RTW outcomes compare for those who received OT treatment and those who did not?
Method
This descriptive quantitative study explored WSBC mental disorder injury claim data documenting OT involvement in the treatment of work-related psychological injuries among PSP between January 1, 2019, and December 31, 2023. The data captured the first 5 years after a legislation change in BC in 2019 expanded eligibility for PTSD claims for PSP. To protect the privacy of the study population, summary data, and not individual claim-level data, were provided by the WSBC data analysis team. Continuous variables were provided as means and standard deviations, and categorical variables were provided as counts and percentages. This study received ethical review and approval through the Queen’s University Health Sciences Research Ethics Board.
The data consisted of 2,621claims with an accepted mental disorder injury categorized as an acute reaction to stress or an adjustment reaction. The claim data included three categories of variables: (1) claimant-specific variables (PSP career category, age, sex), (2) claim-specific variables (nature of injury, mean number of days off work), and (3) RTW variables (RTW successful, RTW unsuccessful, no RTW participation, or unclear RTW outcome). To facilitate statistical analysis, smaller career categories were merged into one of five larger career categories: communicators, correctional workers, firefighters, paramedics, and police officers. See Data Variable Table for further details (Appendix A, Supplementary Material).
Analyses focused primarily on exploring claims that included OT treatment and how these claims differed from those that did not include OT treatment. Data analysis was carried out using R (version 4.3.1). One-way ANOVA was used to determine if there was a difference between groups (e.g., OT vs. No OT, communicators vs. firefighters) for numerical features (e.g., age and treatment lag); Chi-Square Tests of Independence were used to determine if the groups had similar behaviors (e.g., RTW outcomes for OT vs. No OT, and for different career groups). T-tests, Games-Howell tests, and z-tests were used to investigate the difference between two groups, where t-tests and Games-Howell tests were used for averages, and z-tests for standardized score were used for proportions.
Results
Of the 2,621 PSP claims, 45.8% of claims (n= 1,199) included occupational therapy treatment. Data on treatment status, average age, and sex for claimants were provided by WSBC for each career category (Table 1). On average, claimants were 40.6 years old (SD 10.3), but claimants who received OT treatment were significantly older (42.2, SD 10.1 years) than those who did not (39.4, SD 10.3 years), t(2,563.1) = 7.03, p < .0001. Information regarding the biological sex of claimants was available for 2,615 claims. Females made up 39.6% (n = 1,039) of the total sample, but 41.9% (n = 502) of the claimants who received OT treatment were female vs. 37.8% (n = 537) who did not receive OT, representing a significant difference between the groups (z = 2.143, p = .016). Further, males made up 60.1% of the total sample (n = 1,576), but 57.7% (n = 692) of the claimants who received OT treatment were male vs. 62.2% (n = 884) who did not receive OT, representing a significant difference between the groups (z = -2.32, p = .01).
Demographics.
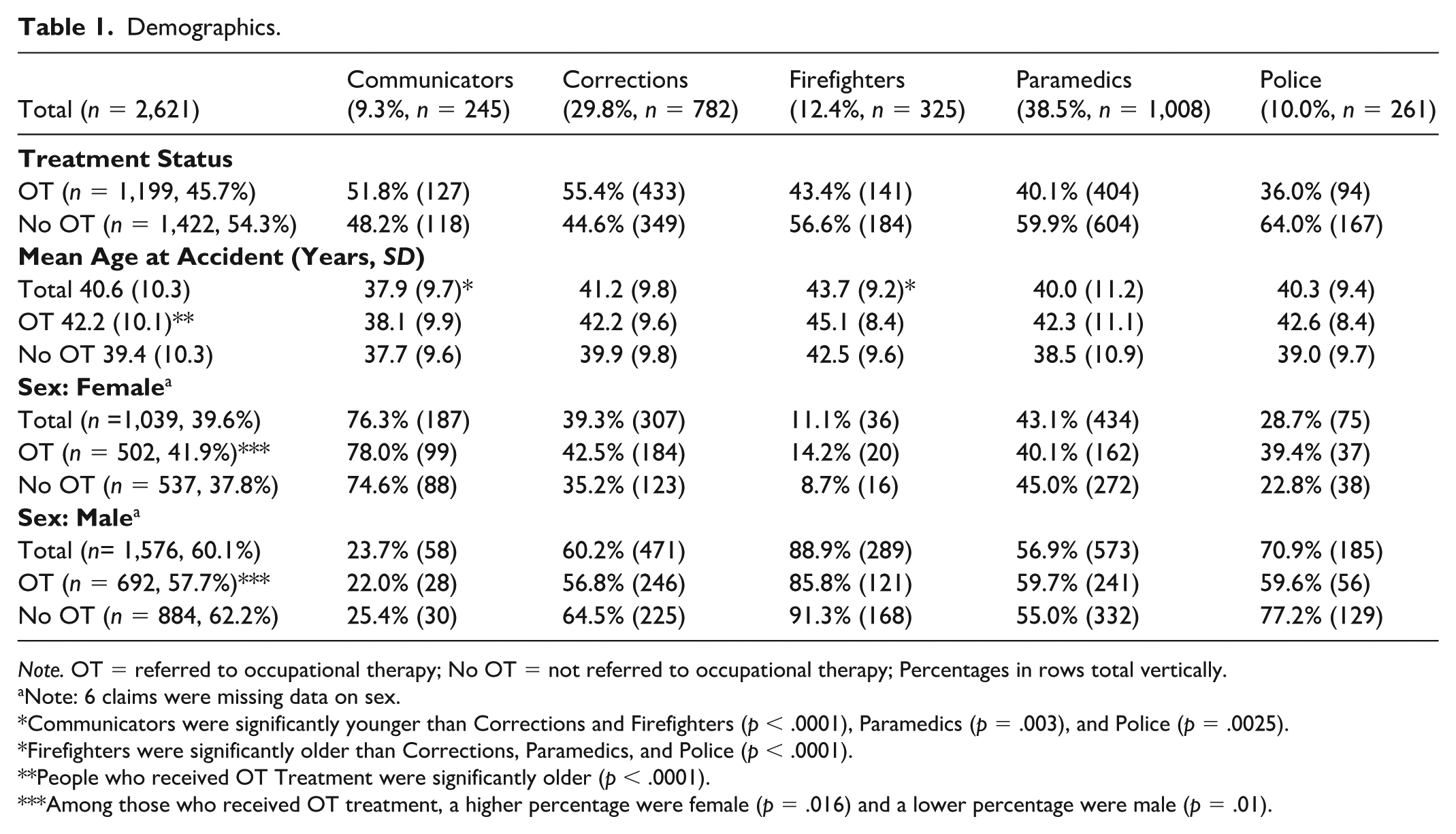
Note. OT = referred to occupational therapy; No OT = not referred to occupational therapy; Percentages in rows total vertically.
Note: 6 claims were missing data on sex.
Communicators were significantly younger than Corrections and Firefighters (p < .0001), Paramedics (p = .003), and Police (p = .0025).
Firefighters were significantly older than Corrections, Paramedics, and Police (p < .0001).
People who received OT Treatment were significantly older (p < .0001).
Among those who received OT treatment, a higher percentage were female (p = .016) and a lower percentage were male (p = .01).
Table 2 summarizes differences between careers categories in access to OT treatment as well as treatment lag, number of OT treatment sessions, and the duration of OT treatment. Significantly fewer workers in the sample received OT treatment, 45.7% vs. 54.3%, χ2 (1, N = 2,621) = 36.131, p < .0001. Of the 1,199 of PSP who received OT treatment, communicators were significantly more likely to receive OT treatment than firefighters (z = 3.67, p = .027), paramedics (z = 10.681, p < .0001), and police (z = 12.224, p < .0001). In addition, correctional workers were significantly more likely to receive OT treatment than firefighters (z = 12.74, p < .001), paramedics (z = 40.75, p < .0001), and police (z = 28.56, p < .0001). There was a significant difference in the mean treatment lag between different groups, F(4, 354.5) = 12.38, p ≤ .0001. Communicators had access to OT treatment earlier than correctional workers, firefighters, and police (p < .0001), and paramedics (p = .006), and paramedics had access to OT treatment earlier than firefighters (p = .002) and police officers (p < .00001) (using Games-Howell post hoc tests). There was a significant difference in the mean number of OT sessions between the groups, F(4, 380.59) = 5.10, p = .0005. Correctional workers participated in more OT sessions than communicators (p = .041), firefighters (pp = .009), paramedics (p < .0001), and police officers (p = .025) (using Games-Howell post hoc tests).
Access to Occupational Therapy Treatment.
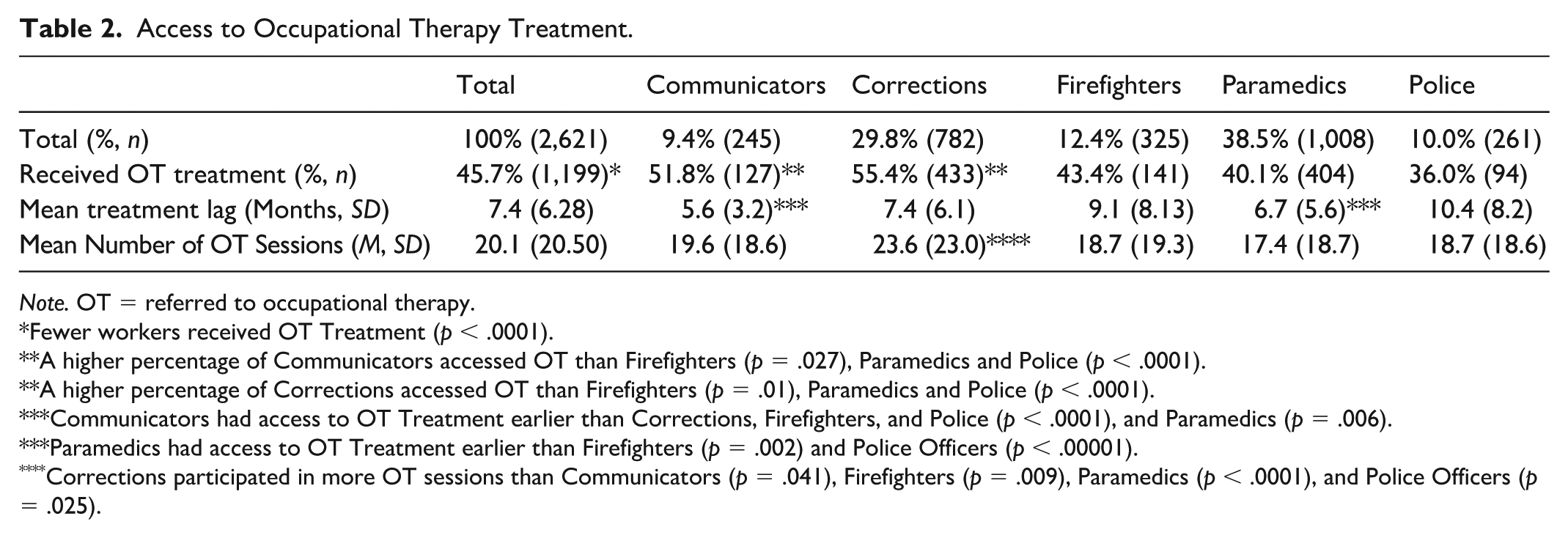
Note. OT = referred to occupational therapy.
Fewer workers received OT Treatment (p < .0001).
A higher percentage of Communicators accessed OT than Firefighters (p = .027), Paramedics and Police (p < .0001).
A higher percentage of Corrections accessed OT than Firefighters (p = .01), Paramedics and Police (p < .0001).
Communicators had access to OT Treatment earlier than Corrections, Firefighters, and Police (p < .0001), and Paramedics (p = .006).
Paramedics had access to OT Treatment earlier than Firefighters (p = .002) and Police Officers (p < .00001).
Corrections participated in more OT sessions than Communicators (p = .041), Firefighters (p = .009), Paramedics (p < .0001), and Police Officers (p = .025).
Table 3 reports claimant data, including the number of accepted injuries, the number of PTSD diagnoses, and claim duration. Various statistical tests were conducted and showed a significant difference between the two groups; Games–Howell post hoc tests revealed that claimants who received OT treatment were significantly more likely to have multiple accepted injures (1.5 vs. 1.3, p < .0001), had a higher percentage of PTSD as an accepted diagnosis (60% vs. 40%, p < .0001) and had a longer claim duration than the rest of the cohort (336 days vs. 122 days, p < .0001).
Claims Data.
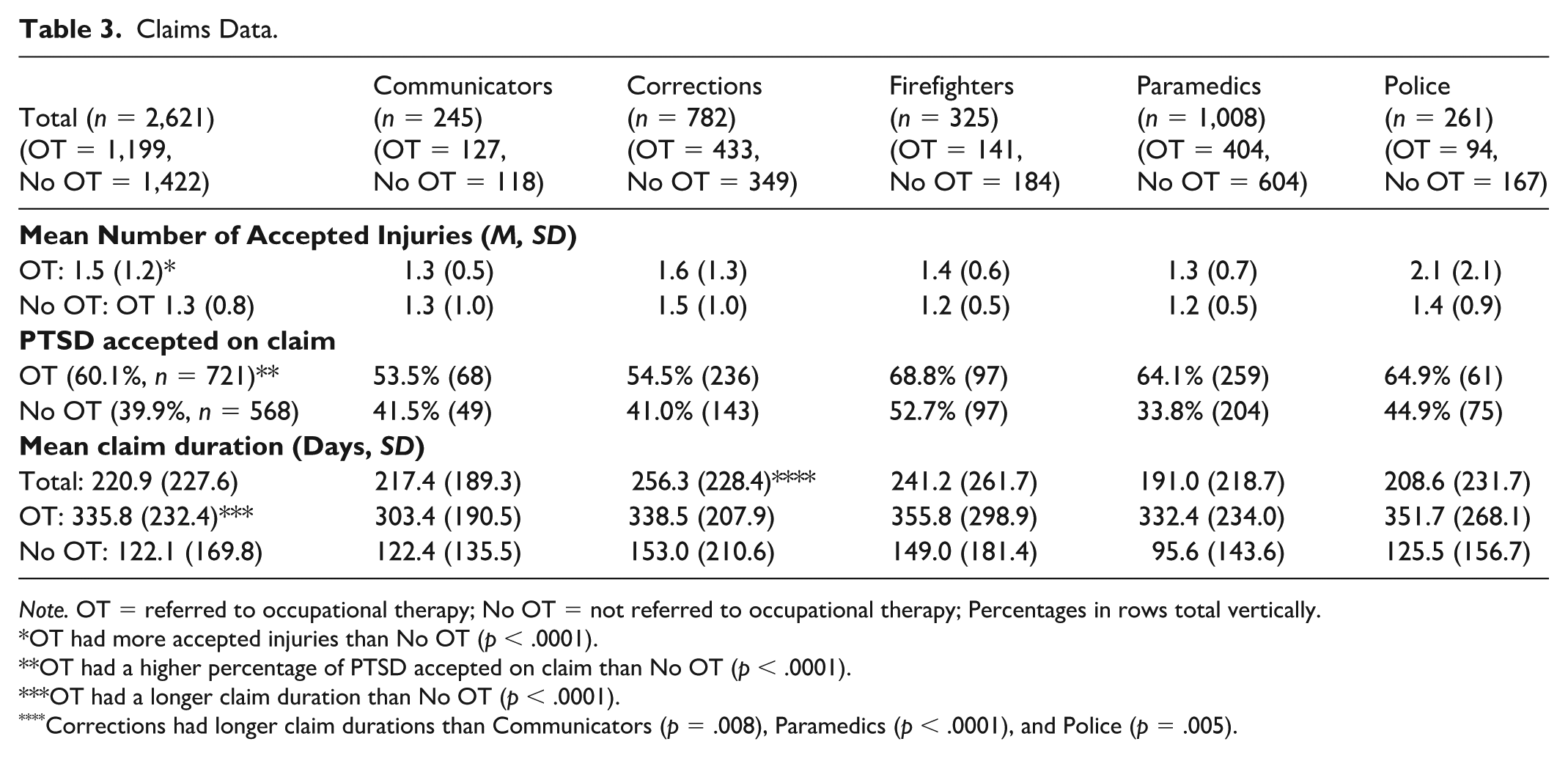
Note. OT = referred to occupational therapy; No OT = not referred to occupational therapy; Percentages in rows total vertically.
OT had more accepted injuries than No OT (p < .0001).
OT had a higher percentage of PTSD accepted on claim than No OT (p < .0001).
OT had a longer claim duration than No OT (p < .0001).
Corrections had longer claim durations than Communicators (p = .008), Paramedics (p < .0001), and Police (p = .005).
Table 4 summarizes RTW outcomes across career categories and OT treatment status. WSBC reported four types of RTW outcomes: RTW attempted (successful), RTW attempted (not successful), and RTW not attempted, and unclear outcome. Over two-thirds of the total claimants had successfully RTW (71.7%, n= 1,879), while one-quarter (24.6%, n = 644) had not yet made a RTW attempt at the time of data collection. Of the claims that had OT treatment (n = 1,199), 61.4% (n= 736) had successfully RTW, while 30.4% (n = 365) had not yet made a RTW attempt. Overall, for those who attempted to RTW (n = 1,910), success rates were high with 98.4% (n = 1,879) successful in RTW, while 1.6% (n = 31) did not RTW successfully. In addition, 2.6% (n = 67) of claimants had an unclear RTW outcome. Regardless of OT treatment status, paramedics had a higher percentage of successful RTW than all other career categories (compared with correctional workers: z = 74.19, p < .0001, with dispatchers: z = 44.95, p < .0001, with firefighters: z = 40.13, p < .0001, with police officers: z = 34.25, p < .0001) and a lower percentage of unattempted RTW than all other career categories (compared with correctional workers: z = 63.66, p < .0001, with dispatchers: z = 28.99, p < .0001, with firefighters: z = 35.09, p < .0001, with police officers: z = 26.31, p < .0001). PSP who received OT treatment had a higher percentage of unattempted RTW and a lower percentage of successful RTW (z = 40.52, p < .0001). In addition, communicators who had OT treatment had a lower percentage of successful RTW (z = 2.8, p = .03), as did firefighters (z = 5.96, p = .005). Correctional workers, paramedics, and police who had access to OT treatment had a lower percentage of successful RTW (corrections: z = 27.25, p < .0001, paramedics: z = 44.6, p < .0001, police: z = 27.98, p < .0001) and a higher percentage of unattempted RTW (corrections: z = 9.62, p < .0001, paramedics: z = 21.99, p < .0001, police: z = 9.98, p < .001). A causal relationship cannot be concluded from the above (i.e., that those workers who received OT treatment had poorer RTW outcomes), given the data shows a difference in complexity of claims that are referred to OT treatment.
Return to Work (RTW) Outcomes.
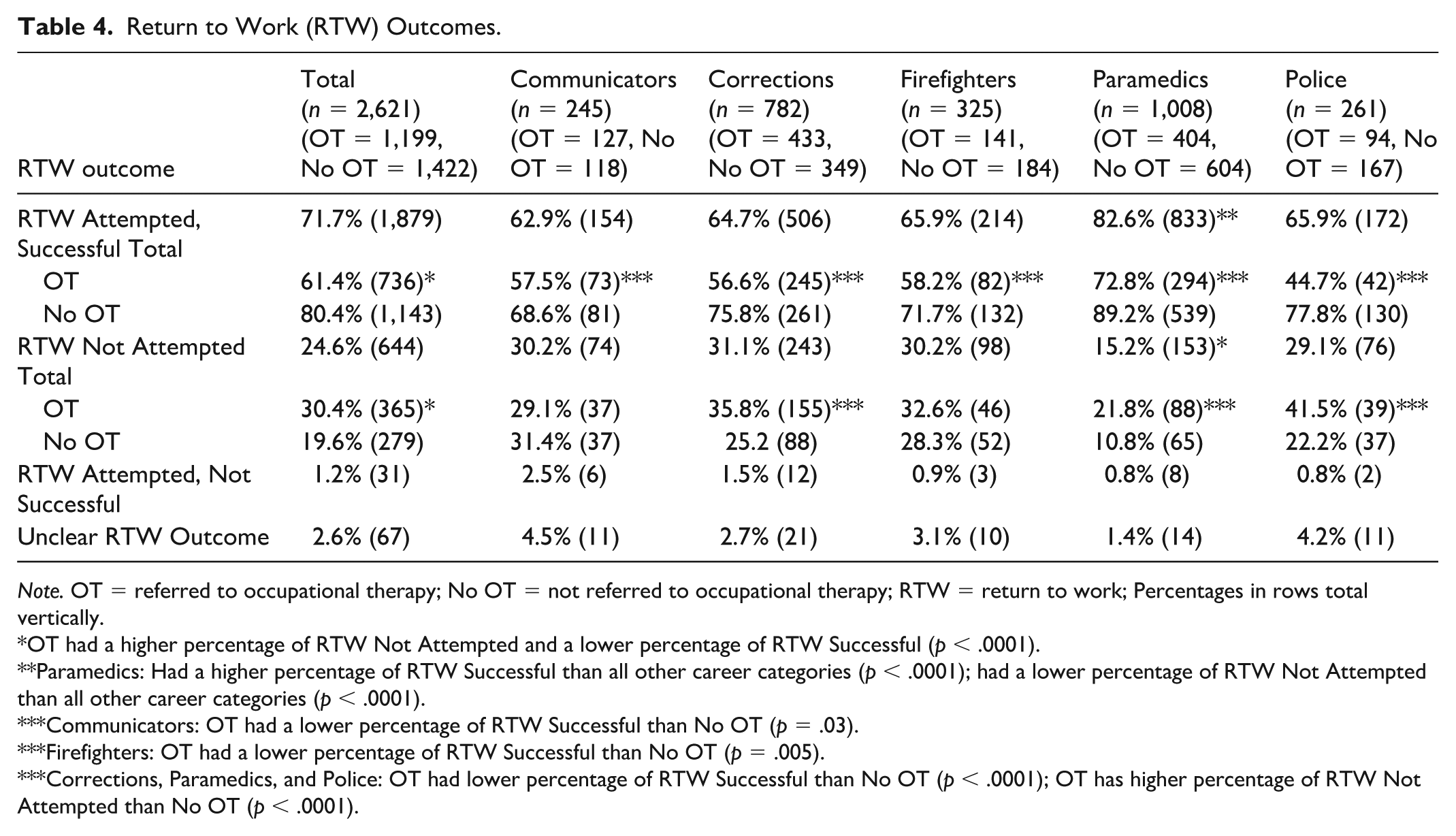
Note. OT = referred to occupational therapy; No OT = not referred to occupational therapy; RTW = return to work; Percentages in rows total vertically.
OT had a higher percentage of RTW Not Attempted and a lower percentage of RTW Successful (p < .0001).
Paramedics: Had a higher percentage of RTW Successful than all other career categories (p < .0001); had a lower percentage of RTW Not Attempted than all other career categories (p < .0001).
Communicators: OT had a lower percentage of RTW Successful than No OT (p = .03).
Firefighters: OT had a lower percentage of RTW Successful than No OT (p = .005).
Corrections, Paramedics, and Police: OT had lower percentage of RTW Successful than No OT (p < .0001); OT has higher percentage of RTW Not Attempted than No OT (p < .0001).
Discussion
Differences Between Public Safety Professions
Of the 2,621 PSP claims analyzed, 46% included occupational therapy treatment, and communicators (52%) and correctional workers (55%) received the highest proportion of OT treatment in comparison to firefighters (43%), paramedics (40%), and police (36%). Data collected also show that communicators and correctional workers had the highest rates of unsuccessful RTW attempts, although the overall rate of unsuccessful RTW was low for all PSP (1.2% on average). Ontario data on RTW claims in PSP parallel these findings, with correctional workers and communicators more frequently receiving OT treatment than other PSP groups, while being slightly less successful in their RTW efforts (Edgelow & Fecica, 2025). A higher proportion of OT treatment access in corrections and communications may reflect operational and organizational-specific barriers and facilitators to RTW, leading to increased use of OT treatment in these claims.
Organizational factors describe job context, structures and culture of the workplace external to the worker. Lack of supervisor support, negative workplace culture, and lack of co-worker support are some of the main organizational factors impacting mental health in PSP (Edgelow et al., 2022). Communicators and correctional workers have been found to have less cohesive work teams and less peer support, when compared to groups like firefighters, police, and paramedics (Edgelow et al., 2022). Several studies have cited a “culture of silence” in corrections and communications, highlighting social experiences as those that emphasize worker toughness and depreciate the perceived value of seeking mental health supports (McKendy & Ricciardelli, 2022; O’Dare et al., 2024). Lack of peer support, negative workplace culture and mental health stigma in corrections and communications organizations may delay help-seeking, contribute to case complexity, and delayed RTW, which may lead to more OT referrals in these claims.
Operational factors describe direct job content and exposures of workers, and the most common operational stress factor for PSP is exposure to critical incidents (Edgelow et al., 2022). Correctional workers are exposed to violence, direct threats, and workplace injury at rates higher than other PSP groups in Canada (Regehr et al., 2021; St Louis et al., 2023). For communicators, exposure to critical incidents is high due to the nature of being a first point of contact in emergency services (Birze et al., 2022; Edgelow et al., 2022). PSP exposure to critical events has been shown to increase mental health symptoms, making these groups at higher risk of requiring work leave (Carleton et al., 2018). Further, compared to other PSP groups, communicators and correctional workers are more likely to report a perceived lack of autonomy over workload and control over client outcomes (Birze et al., 2022; Regehr et al., 2021). Communicators are pressured with making time-sensitive decisions and have little power over or knowledge on caller outcomes, while correctional workers may witness self-harm, death, and violence, also having little influence on events and their outcomes (Edgelow et al., 2022). Unlike many other PSP, both communicators and correctional workers return to the same environment daily, aggravating stressors by continuing to work in spaces where traumatic events occurred (Coulling et al., 2024). High exposure to critical incidents, lack of control over workload and client outcomes, and returning to the environment where a traumatic event happened may contribute to claim complexity and thus increase the perceived need for OT treatment.
Lack of gender parity in PSP professions could underpin increased OT access in communicators, a group where females are overrepresented (Karunakaran, 2022). In our sample, communicators were disproportionately female (78.3%)—this finding, coupled with evidence that females are more likely to screen positive for mental disorders and to access mental health supports, could help to explain why communicators accessed OT at higher rates (Carleton et al., 2018; Cox, 2014).
Moreover, our sample shows that communicators had access to OT treatment earlier than corrections, firefighters, and police, while correctional workers participated in more OT sessions than communicators, firefighters, paramedics, and police officers. One possible explanation for these findings is that most communicators and corrections officers work in the same spaces every day, and their work may be office-based in comparison to other PSPs who often work off-site or in unpredictable environments (Birze et al., 2022; Coulling et al., 2024). This ease of access to the workplace may influence rates of referral to OT and may facilitate OT involvement in job demands analysis, workplace visits, and the implementation of workplace accommodations. These assessments and interventions may call for earlier and/or prolonged OT involvement in claims made by communicators and correctional workers. Moreover, higher rates of screening for mental health disorders and higher intention to use mental health services in correctional workers could explain why they participated in more OT sessions than other PSP groups (Krakauer et al., 2020). Further research might be conducted to understand how PSP work environments may influence the timing of OT treatment and related return to work processes, along with the type of intervention provided.
Furthermore, in our sample, paramedics were shown to successfully RTW at least 16.7% more frequently than all other PSP professions who accessed OT. They were also shown to have access to OT treatment earlier than firefighters and police officers. Paramedics have also been found to make claims after fewer traumatic incidents, to be more likely to complete the RTW process, RTW earlier, and be more successful in their RTW than other PSP groups (Edgelow et al., 2023a). It is recognized that individuals in fields requiring a base of knowledge in health and wellness may exhibit increased awareness of personal health concerns (Edgelow et al., 2023a). When compared to other PSP groups, increased knowledge of health and wellness, more cohesive team environments/peer support, environmental change, and a sense of value/social status found in paramedicine could explain findings that paramedics accessed OT services earlier than firefighters and police officers and exhibited greater successful RTW outcomes (Krakauer et al., 2020). Ontario data support these findings, as paramedics have been found to access OT earlier, and are more successful in RTW efforts than other PSP (Edgelow & Fecica, 2025).
Claim Complexity and Occupational Therapy Treatment
Generally, across all professions, study results suggest that claims that had access to OT treatment were more complex for a variety of reasons. They were made by older PSP, and proportionally more of these claimants were female. In addition, claims that included OT treatment had a higher number of injuries and more days away from work. These factors contribute to increased claim severity and lower likelihood of RTW, supporting the notion that OT treatment was offered to more complex cases requiring more intensive RTW support. More broadly, we also know that OTs were introduced into claimants’ care teams later than other health care professionals, and that claims including OT services had a longer duration. These results parallel studies that show that expansion of RTW rehabilitation teams and longer time spent away from work are markers of greater injury and symptom severity in claims, as well as worse RTW outcomes (Gross et al., 2021). Thus, OTs have been shown to be introduced in more complex RTW cases, where clients show a greater number and intensity of RTW barriers.
PSP in our study who accessed OT treatment were older on average than those who did not. Older PSP are more likely to report symptoms of mental disorders, likely due to the cumulative exposure to potentially traumatic events over their careers, which increases case complexity (Carleton et al., 2018). Furthermore, in a systematic review of barriers to RTW in individuals with common mental disorders (CMD), older age was identified as a predictor of reduced RTW rates (Gragnano et al., 2018), which may explain the greater perceived need for OT services among this group. Ontario data support these findings, as PSP groups who were older on average had less success in RTW efforts than other PSP (Edgelow et al., 2023; Edgelow & Fecica, 2025).
In our sample, more females than males accessed OT in every profession except for paramedicine. This finding is similar to Ontario data, showing that more female than male PSP accessed OT between 2017 and 2021 (Edgelow & Fecica, 2025). Several factors could explain this. Research demonstrates that female PSP may be more likely to screen positive for mental health conditions and seek help (Carleton et al., 2018; Cox, 2014), which may make them more likely to access OT services. Moreover, females in first responder organizations often face unique stressors related to their gender, compounded by the male-dominated organizational structure of first responder organizations (Jasper et al., 2023; Krakauer et al., 2020). While workplace culture is typically seen as a protective factor in PSP roles, it can also act as a barrier to belonging and trust for females in these professions (Jasper et al., 2023; Khan, 2022). These challenges may contribute to increased case complexity and reduced RTW likelihood for female PSP. This aligns with research showing worse RTW outcomes for females with CMDs compared to males (Gragnano et al., 2018).
Workers who accessed OT services also had longer absences from work before referral, which may reflect the severity of their psychological injuries. These findings echo those of a similar analysis in the Ontario workers’ compensation context (Edgelow & Fecica, 2025). Prolonged work absence is a well-documented predictor of reduced RTW likelihood (Gross et al., 2021). Furthermore, by the time the workers in this study accessed OT services, they had often spent more time within the mental health system than PSP who did not access OT treatment, reflecting more advanced RTW challenges in these clients. PSP commonly report dissatisfaction and a lack of trust in mental health professionals, particularly those unfamiliar with first responder culture (Edgelow et al., 2024; Isaac & Buchanan, 2021; O’Dare et al., 2024). This prolonged exposure to the mental health system may erode trust and confidence in mental health services, affecting engagement in OT treatment and reducing RTW likelihood.
Return to Work Outcomes
PSP who received OT treatment as part of their WSBC claim had slightly lower rates of successful RTW and a higher likelihood of not having attempted RTW compared to those who did not receive OT treatment. However, these outcomes should be interpreted in the context of the severity and complexity of their cases. As previously discussed, workers who accessed OT services often face factors that significantly decrease their likelihood of successful RTW. Consequently, the lower RTW rates in this group likely reflect the challenges of managing complex cases rather than the effectiveness of OT itself.
Differences and similarities in the length of claims and PSP interaction with OT were found between this study’s findings and data on the same population and context in Ontario, another province in Canada with its own worker’s compensation system (Edgelow & Fecica, 2025; Edgelow et al., 2023a). In Ontario, more PSP claims were made (n=6,674) than in Ontario, BC (n=2,621) (Edgelow et al., 2023a); these findings align with differences in population size. In BC, a larger proportion of PSPs accessed OT than in Ontario; 46% of BC claims (n = 1,199) included occupational therapy, compared to 15% (n = 991) in Ontario (Edgelow & Fecica, 2023). In Ontario, PSP waited on average 1.5 years to begin OT treatment, and those who received OT treatment spent an average of 913 days off work (Edgelow & Fecica, 2025). In BC, PSP waited on average 7.4 months to begin OT treatment, and those who received OT treatment had an average of 336 days off work. In both provinces, claims including OT were significantly longer than claims that did not include OT; however, in BC, PSP waited approximately half as long to access OT and went back to work almost three times more quickly. On the whole, PSP in BC had an average claim duration of 221 days off work (regardless of treatment status), while PSP in Ontario had an average claim duration of 422 days off work (regardless of treatment status) (Edgelow et al., 2023). Overall, it is interesting to note that BC appears to use OT treatment three times more frequently than Ontario, takes half as long to provide access to OT treatment, and has average claim durations that are half as long as Ontario’s (Edgelow et al., 2023a; Edgelow & Fecica, 2025).
Recommendations
These findings underscore the importance of early identification and intervention to mitigate the impacts of psychological injuries and facilitate timely RTW—areas where OT services can play a pivotal role (Brown et al., 2019; Gross et al., 2021). A scoping review by Nowrouzi-Kia et al. (2023) found that “health-focused” and “multi-domain” interventions are the most effective in supporting RTW for individuals with work-related mental health conditions. Health-focused interventions include therapies such as psychological therapy and occupational therapy, while multi-domain interventions integrate two or more components across health-focused, service coordination, and work-modification domains. Service coordination interventions enhance communication between employees, employers, and health care providers through RTW plans, case management, education, and addressing workplace stressors (Nowrouzi-Kia et al., 2023). Work-modification interventions involve adjustments to work environments and conditions (Nowrouzi-Kia et al., 2023). Moreover, a systematic review by Cullen et al. (2018) found that cognitive therapy interventions alone, without workplace modifications or service coordination, are ineffective in supporting RTW for workers with mental health conditions. OTs are uniquely positioned to deliver health-focused interventions while also coordinating services and recommending workplace modifications. These findings emphasize the need to incorporate OT services earlier in the RTW process within worker’s compensation systems.
Study Limitations
In this study, the data provided by WSBC did not include demographic variables like socioeconomic status, race, and marital status, and their impact on outcomes could not be analyzed. Claims registered in the WSBC system prior to 2018 did not have PTSD diagnosis coded in the claims management system, so the number of PTSD diagnoses captured in this data is likely lower than it would otherwise be. In addition, WSBC claims staff have not been consistently indicating RTW success if a worker has returned to modified work; as such, the RTW rates may be higher than what the data show. Since the data set is from 2019-2023 and included all open claims from that five-year period, recent changes to this data are unknown. It is possible that more recent claims in the data set did not have the same opportunity to RTW that longer claims had. However, for those who had not attempted RTW, the proportion is quite similar across the groups, except for paramedics (who are different from other career groups across most variables). This suggests that in general, RTW processes start at similar times for communicators, correctional workers, firefighters, and police.
The results draw on data from BC, Canada, which may limit generalizability to other contexts and workers’ compensation systems. It is important to note that the discussion section refers to study data by sex rather than gender, while the cited research often addresses gender; this is because the WSBC data report on sex rather than gender. As workplace stressors and cultural factors primarily relate to gender rather than biological sex, it is possible that some PSP in our study sample experience gender-based work factors that differ from their biological sex.
Conclusions
This study is the first to report on the usage of OT treatment with PSP with work-related psychological injuries in BC, Canada, and builds on the findings of a similar study from Ontario, Canada (Edgelow & Fecica, 2025). In both cases, PSP who had access to OT treatment had more indicators of claim complexity and longer claim durations. However, RTW outcomes were more favorable in BC, where PSP had earlier access to OT and more access to OT treatment, pointing to the possibility that earlier OT intervention may improve RTW outcomes. Policy makers and workers’ compensation leadership should review referral pathways for injured workers to health professionals and consider the potential positive impact of earlier intervention that includes access to occupational therapy. Further research should investigate if these findings are consistent across other jurisdictions, in Canada and beyond.
Supplemental Material
sj-docx-1-otj-10.1177_15394492251397844 – Supplemental material for Analyzing British Columbia Workers Compensation Occupational Therapy Usage With Public Safety Personnel
Supplemental material, sj-docx-1-otj-10.1177_15394492251397844 for Analyzing British Columbia Workers Compensation Occupational Therapy Usage With Public Safety Personnel by Megan Edgelow, Catherine Boudreau and Kayla Beren in OTJR: Occupational Therapy Journal of Research
Footnotes
Acknowledgements
Thank you to Daniela Fisher, Program Manager for Occupational Therapy Services at WorkSafeBC, who provided input as Subject Matter Expert (SME). This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical Considerations
This study received ethical review and approval through the Queen’s University Health Sciences Research Ethics Board (REH-843-22) and was conducted in accordance with national legislation and institutional requirements. This is a secondary data study; written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The original data set used in this study is owned by WorkSafeBC and is not publicly available due to privacy guidelines.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.