
Abstract
Introduction:
Approximately 100,000 people in the United Kingdom experience a stroke each year, with one in four being of working age. One-third do not return to work. Occupational therapists support stroke survivors return to work, but specific practices are unclear. This study aimed to explore occupational therapists’ perceptions, current practices and confidence levels when working with people with stroke who wish to return to work.
Methods:
A mixed-methods study was completed. A survey explored occupational therapy practices and confidence levels. A focus group explored the experience and perceptions of occupational therapists. Participants were occupational therapists in the United Kingdom working with individuals with stroke for a minimum of 6 months.
Results:
Sixty-eight respondents completed the survey. There were four focus group participants. Traditional stroke rehabilitation assessments and interventions were reported more frequently than work-related interventions. Participants reported being less confident liaising with employers and identified lack of resources, training and flexibility in delivery of stroke services as challenging.
Conclusion:
This study suggests that current occupational therapy practice does not consistently provide work-specific interventions. Flexibility in services is needed to address the vocational rehabilitation needs of stroke survivors with recommendations for post-graduate training and specialist roles in stroke-related vocational rehabilitation.
Keywords
Introduction
The prevalence of stroke in working age adults is increasing with up to one in four stroke survivors being of working age (Public Health England, 2018). Returning to work is frequently identified as a challenge for working age adults with stroke, with over one-third of stroke survivors leaving their job due to its consequences (Stroke Association, 2022). Work provides meaning in life and is a vital component of health and wellbeing (Martin-Saez and James, 2021; Royal College of Occupational Therapy, 2018). The inability to return to work can lead to mental and physical ill health, reduced quality of life and loss of self-identity (Busch et al., 2009, Daniel et al., 2009, Teasell et al., 2000). The economic consequence of people with stroke not returning to work is substantial, with loss of productivity estimated at £1.6 billion per year in the United Kingdom (Patel et al., 2020).
Vocational rehabilitation (VR) is any activity or intervention that supports a person with ill health or disability return to or remain in work (Waddell, 2008). The necessity for support for people with stroke who wish to return to work has been recognised by policymakers (Department for Work and Pensions and Department of Health, 2017; NHS England, 2021) and in recent clinical guidelines (National Institute for Clinical Excellence, 2023; National Clinical Guideline for Stroke, 2023). Despite these recommendations specialist VR services are not commonplace and people with stroke continue to have difficulties returning to work (Stroke Association, 2022).
Return to work after stroke is difficult to measure and occurs because of the interaction of multiple systems (Grant et al., 2014). Positive predictors of return to work include younger age, male sex, ischaemic stroke and independence in daily activities (Mascarenhas et al., 2024). Higher education and employment in larger organisations further facilitate earlier return (Palstam et al., 2018). The absence of executive dysfunction, fatigue and mood disorders is also important (Brannigan et al., 2017).
Occupational therapists are experts in activity analysis, making the profession well suited to provide interventions facilitating return to work (American Occupational Therapy Association, 2017). Two randomised control trials demonstrated that occupational therapy- led interventions can increase return to work rates using a case coordination approach (Ntsiea et al., 2015; Trexler et al. 2010), although further high-quality studies with larger sample sizes and longer follow-up periods are needed (Coutts and Cooper, 2023; Pearce et al., 2023).
Although the importance of occupational therapists in facilitating return to work following stroke is widely acknowledged, there remains a limited body of evidence detailing clinical practice. Scott and Bondoc (2018) surveyed occupational therapists to explore assessment and intervention practices in the United States and reported the most frequent areas assessed and treated in practice related to biomechanical, cognitive and visual perceptual deficits. Participants reported less employer and occupation-based practices. Less participants addressed the emotional demands of returning to work, despite evidence identifying this as a barrier (Brannigan et al., 2017). Holistic and occupation focused practices may be more consistent with occupational therapists models of practice and are evidenced in literature (Donker Cooles et al., 2016; Ntsiea et al., 2015).
Few studies have explored the opinions of occupational therapists’ working with this population. In Australia, healthcare professionals lacked confidence in setting work-related goals and felt uncomfortable making return to work recommendations for people with acquired brain injury (O’Keefe et al., 2021). This study was not specific to stroke or occupational therapists. Occupational therapists in South Africa perceived VR as complex and identified a need for further training (Drier and Van Niekerk, 2020). As occupational therapists are key professionals in supporting this population, a deeper understanding of their experiences may help identify challenges and opportunities in facilitating return to work after stroke.
This study aims to explore how occupational therapists support individuals with stroke in returning to work. It will examine the assessments and interventions used, occupational therapists’ confidence levels and their perceptions and experiences of delivering VR in this context. The specific objectives are to (1) identify the assessments and interventions used when supporting people with stroke who wish to return to work, (2) identify confidence levels of occupational therapists working with this group, and (3) explore occupational therapists perceptions and experiences in delivering VR.
Method
Design
A sequential explanatory mixed-methods study was undertaken. Occupational therapists assessment, intervention and confidence levels were explored via an anonymous, cross-sectional survey. This was followed by a focus group (FG) using a qualitative descriptive design to explore the experiences of occupational therapists. Mixed-methods studies allow for the shortcomings of both approaches to be overcome (Caruth, 2013) and allows for the topic to be explored in more depth (Bowen et al., 2017). Ethical approval for this study was granted by a University Ethics Committee in 2021.
Survey design
The survey allowed for data to be collected from a greater number of participants than if a qualitative study was completed in isolation. The survey was adapted from an American study (Scott and Bondoc, 2018) with permission. It was adapted to align with this study’s aims and reduce participant burden by removing questions related to insurance and revising wording to reflect UK healthcare environments. The Checklist for Reporting Results of Internet E-Surveys (CHERRIES) was followed (Eysenbach, 2004). The survey was piloted with six occupational therapists experienced in stroke. The wording of one question was updated post pilot for clarity.
Focus group
A focus group explored the experience and perceptions of occupational therapists working with this population. A structured interview guide based on findings from survey data was used to guide discussion. The FG method is appropriate to generate in depth data on the knowledge and experiences of healthcare professionals (Then et al., 2014). FGs allow time for reflection before answering therefore are less pressurising than individual interviews (Tiberius, 2006). The primary researcher, with prior experience of qualitative interviews facilitated the group, adapting the methodological approach to a group context.
Eligibility criteria
Inclusion criteria were UK-based occupational therapists with a minimum of 6 months experience of working with individuals with stroke. Other healthcare professionals and occupational therapists who had not worked with individuals with stroke for at least 6 months were excluded.
Recruitment
The survey was hosted on SurveyMonkey and shared via the Royal College of Occupational Therapy (RCOT) Specialist Section for Neurological Practice (SSNP) monthly newsletter in January 2022 and on social media (Twitter and Facebook). Consent was gained at the beginning of the survey, and it was available for 6 weeks. Two reminders were provided.
At the conclusion of the survey, participants were invited to provide their contact information via a link if interested in participating in the FG. All respondents who expressed interest were included. Written consent was obtained. The primary researcher moderated the session, supported by a note taker (Phillipi and Lauderdale, 2017). A research diary was maintained to ensure neutrality and reflexivity.
Sample size
At the end of 2021, the SSNP had 850 members who received the RCOT-SSNP newsletter. There were 3595 followers on its Twitter page. Assuming a potential population size of 1245, a sample size of 294 was calculated to achieve a 5% margin of error with a 95% confidence level, using an online sample size calculator (SurveyMonkey, 2021).
The researcher initially planned to conduct three FGs of 6–8 participants to allow for a range of opinions, while also enabling meaningful contribution (Kreuger and Casey, 2015). However, only one was held due to time constraints related to the research being part of a taught master’s degree, and pressures faced by the health service during the research period.
Data analysis
Quantitative survey data were analysed using STATA 17 statistical software package. Descriptive analysis was used to report participant demographics and to describe frequencies in approaches to intervention and assessment. Subgroup analysis using a Wilcoxon rank-sum test was completed to compare differences between assessment and interventions used based on years of experience and work setting (inpatient and outpatient).
The FG was recorded and transcribed on MS Teams. Qualitative data were analysed using the six stages of thematic analysis (Braun and Clarke, 2021). Transcripts from MS Teams were read and re-read by the researcher to allow for familiarisation and interpretive and reflexive reading. Data were initially coded by hand and then transferred to N-Vivo 12 data analysis software to identify themes and categories. To ensure rigour, data were also analysed by a colleague with experience in qualitative research. Member checking was completed where a copy of pseudonymised transcripts was provided to each participant. Participants were offered 2 weeks to suggest amendments. Following this, it was assumed that participants agreed with the transcript. This process aimed to reduce bias (Cresswell and Plano Clarke, 2011).
Quantitative and qualitative data were subsequently triangulated to support interpretation. This involved listing the findings from both parts of the study and looking for similarities or contradictions. It allowed the researcher to explore if findings from the survey were also reflected in the focus group.
Results
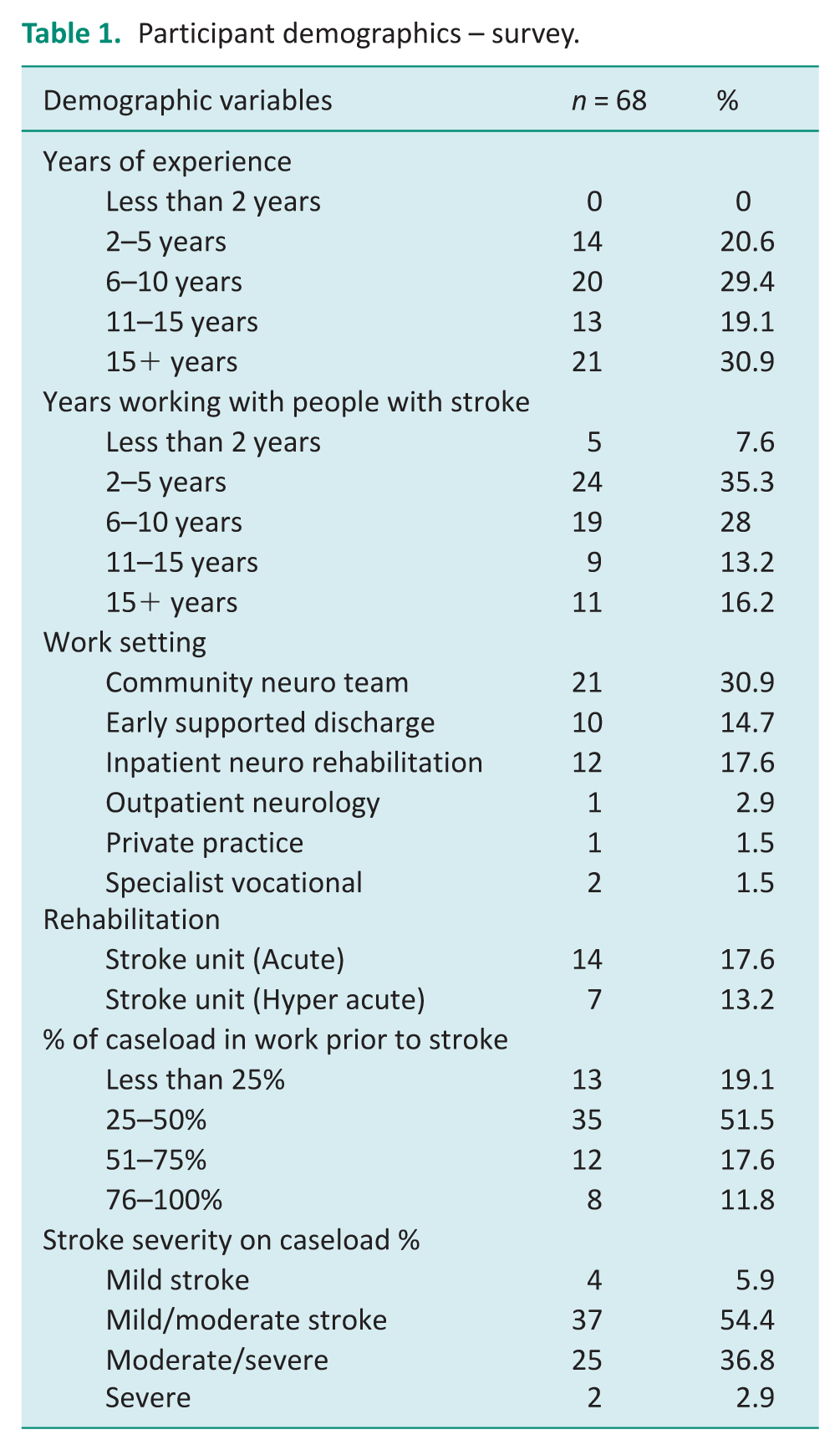
Sixty-eight occupational therapists completed the survey, representing a 70% completion rate among participants initiating it. Respondents worked in outpatient/community settings (51%) and inpatient settings (49%). The majority (79%) had over 6 years’ experience as qualified occupational therapists and 57% had more than 6 years’ experience working with people with stroke. Fifty-one percent reported that 25%–50% of their caseload were working prior to stroke. Mild/moderate stroke was the most reported level of stroke severity. Table 1 outlines respondents’ work experience and clinical caseload.
Participant demographics – survey.
A FG (44 minutes) with four participants was carried out in February 2022. Table 2 outlines participant demographics. Four categories related to the research aims were identified from thematic analysis: occupational therapy assessment, occupational therapy intervention, challenges when working in this clinical area and opportunities when working in this clinical area.
Participant demographics – focus group.
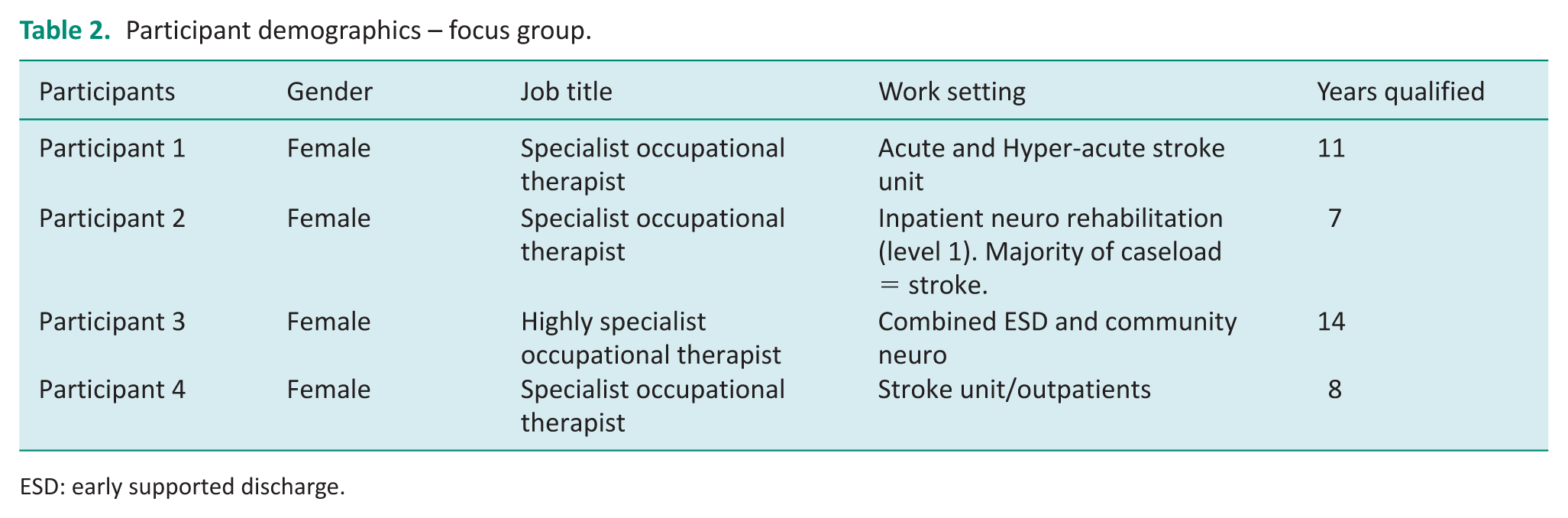
ESD: early supported discharge.
Information gathering and assessment
Ninety percent of occupational therapists reported they always or frequently ask people with stroke about their employment status (figure 1), while 83% gathered information about job roles. FG participants confirmed they all conduct a subjective initial assessment asking people with stroke about work, employment type and desire to return to work.
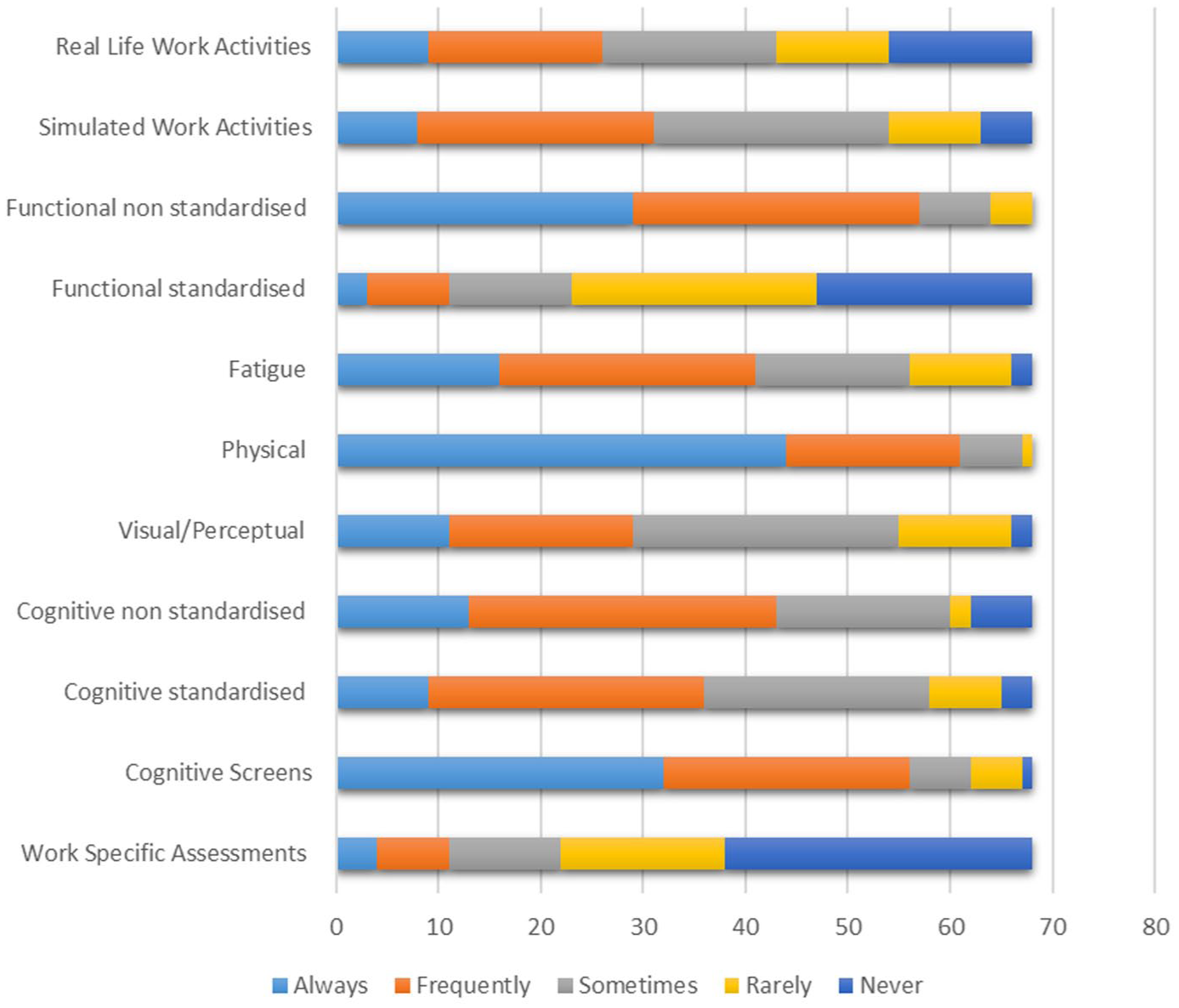
Types of assessment.
Most respondents gain information about the physical and cognitive demands at work (90%) but slightly less asked about emotional demands (76%), supportiveness of employer (73%), the social environment (54%) and supportiveness of colleagues (50%). The importance of support from colleagues and the workplace environment was discussed during the FG where one participant raised challenges faced by stroke survivors concerning colleagues’ perceptions upon returning to work: P4: It’s the communication and the rapport you have with your colleagues. It was affecting their [the patient’s] self-worth and their belief and why they should be going to work.
Sixty percent of participants asked people with stroke about their commuting needs and 73% asked about financial concerns. Participants in the FG spoke about how lack of financial support can pose challenges when making recommendations: P2: From a financial point of view . . . they may be pushing themselves to go back to work too soon, earlier than they would like.
Most participants gathered information primarily from clients (82%) while only 23% gathered information from employers.
Ninety percent of occupational therapists reported they always or frequently complete non-standardised physical assessments. Non-standardised functional assessments (84%) and cognitive screens (82%) were the next most frequently used. FG participants working in acute settings also referred to using a general approach to assessing neurological impairments: P1: I think more generalised neuro assessments in the acute setting anyway, and I think it’s kind of starting at the very early stages
Work specific assessments and standardised functional assessments were the least frequently reported assessments with 66% of respondents reporting ‘rarely’ or ‘never’ completing these. Participants in the FG reported not using or being familiar with work-specific assessments. One participant explained that this was because they rarely address work: P1: I think generally I’m not too familiar with formalised assessments through work, because I suppose I largely haven’t had to deal with an awful lot of that.
Significant differences were observed in the use of work-specific assessments between respondents with less than and greater than ten years’ experience (p < 0.001), and between those who worked in inpatient and outpatient settings (p = 0.02). Respondents working less than ten years (n = 34), and those working in in-patient settings (n = 33) completed significantly fewer work assessments. The appropriate setting and timing for assessment was discussed in the FG where two occupational therapists working in an in-patient setting reporting they believed this setting was too early for assessment of work ability: P2: This is kind of early anyway, because sometimes I might not even be thinking about going back to work. The goals may be just to get dressed
Participants also identified multiple areas that require assessment, possibly explaining why work-related assessments are rarer: P1: I suppose it’s so multi factorial, isn’t it? From the kind of assessment process that you’re having to think about absolutely everything – environmental, fatigue, cognitive, physical. There’s so many different areas.
Occupational therapy interventions
The intervention reported most as being used ‘Always’ or ‘Frequently’ was ‘cognitive rehabilitation – education’ (91%). Other commonly used interventions included ‘upper limb rehabilitation’ (87%), ‘cognitive rehabilitation – compensatory strategies’ (85%) and ‘functional mobility – transfers’ (84%) (Figure 2).
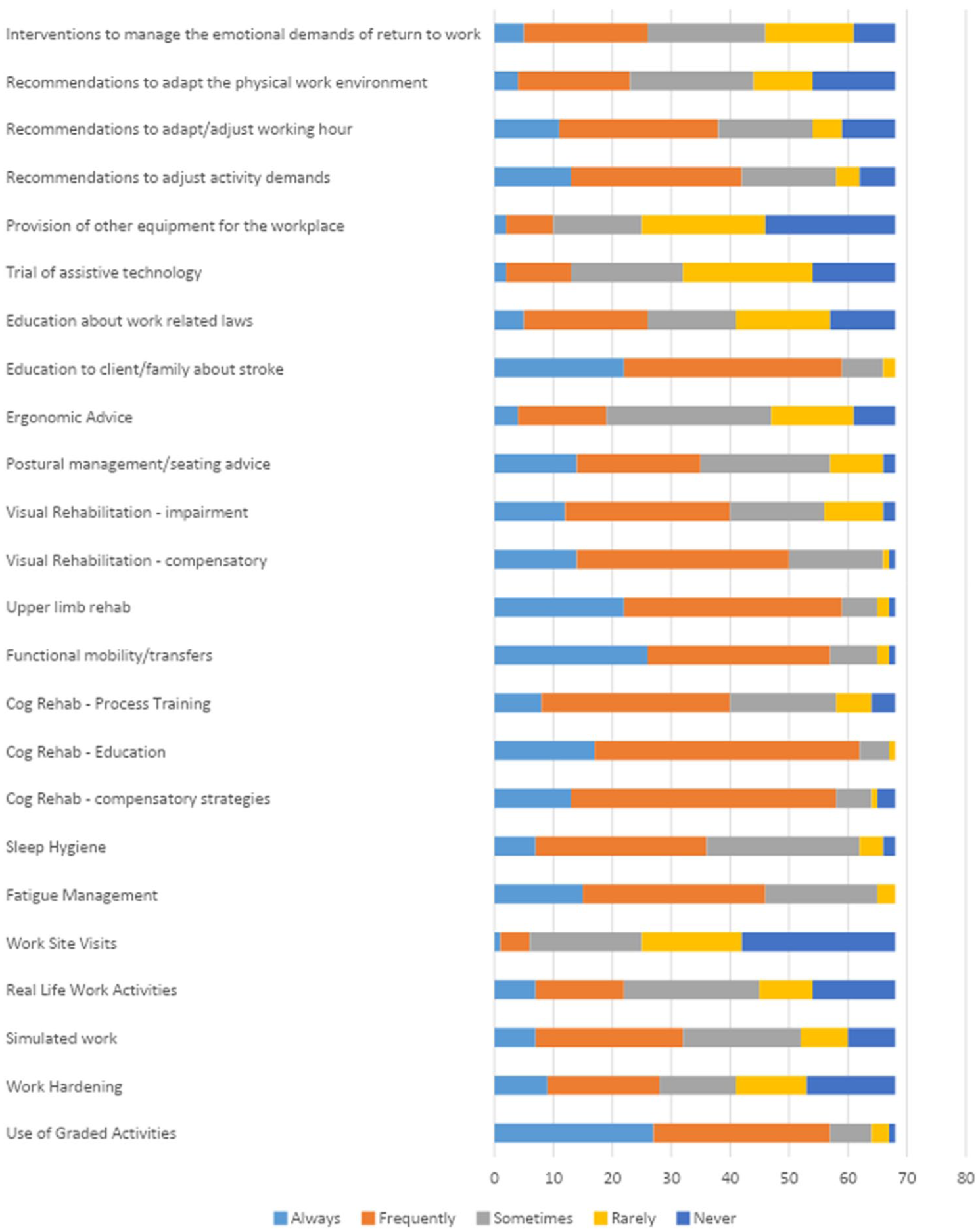
Types of intervention.
Significant practice differences were noted with occupational therapists with more than 10 years’ experience using several interventions more frequently than those with less experience. These include work hardening (p = 0.005), work site visits (p = 0.02), providing ergonomic advice (p = 0.05), recommendations to adapt working hours (p = 0.002) and the working environment (p = 0.03) and interventions to manage the emotional demands of return to work (p = 0.03). There were also differences between practice contexts, with those who work in outpatient settings providing more work hardening interventions (p < 0.001), work site visits (p = 0.001), simulated work activities (p < 0.001), real-life work activities (p < 0.001), equipment for the workplace (p = 0.02), education about work-related laws (p < 0.001) and interventions to manage the emotional demands of return to work (p < 0.001). Interventions to manage fatigue (p = 0.003) and sleep (p = 0.012) were also reported more by outpatient occupational therapists.
Interventions reported as being delivered ‘rarely’ or ‘never’ included ‘provision of equipment for the workplace’ (63%), ‘work site visits’ (63%) and trialling assistive technology (53%).
Difficulties in providing equipment for return-to-work purposes was discussed in the FG with one participant identifying a lack of availability of work-related equipment: P1: When we think about things like getting someone home, you know there’s an array of equipment we can order to put in place in the house to support with that. But when it comes to the work situation, it’s harder to be able to order that equipment.
It was also discussed that sometimes people with stroke do not provide consent for employer-based interventions, even though they are considered important by occupational therapists: P3: We would try to do that with the employer, but it is the patient’s decision about whether they want us to get in contact with the employer P2: Sometimes patients don’t want you to involve the employer.
All FG participants regarded occupational therapists reports for the workplace as an important intervention. These reports summarise occupational therapists treatment and provide recommendations for return to work. They were considered an important way of advocating for the person and making practical recommendations: P4: I think the letters and the reports can be very helpful for them, that’s where occupational therapy has that key role in the practical accommodations.
However, only 35% percent of respondents in the survey reported providing reports ‘always’ or ‘frequently’.
In relation to reasonable adjustments, there were some opportunities identified post the Covid 19 pandemic where two participants felt that normalisation of home working and flexible working patterns had helped people with stroke return to work: P1: The lockdowns and the working from home has actually helped in some ways as well. Helped with managing fatigue because they don’t have to worry about the commute there. P4: Covid has actually helped a little bit as well to get the employer in the mindset of making adjustments on the wider scale.
Participants also discussed how having local community therapy teams who provide VR interventions was positive: P2: I think if every community service addressed vocational needs, then there wouldn’t be such long waiting list for vocational rehab clinics.
Challenges arise when employers cannot support recommended workplace adjustments. These may include adapting working hours, conditions or job role or facilitate a phased return to work: P2: If you make the recommendations and then the employer for whatever reason is unable to support those.
From an occupational therapists’ practice perspective, FG participants identified that a lack of flexibility regarding their working hours was a barrier in providing intervention, particularly for individuals who had already returned to work: P3: Sometimes it’s really difficult, because if they’re working until five o’clock and you finish work at 4:30, it’s really difficult to try and fit them in then to address those difficulties.
Factors impacting therapists’ decision-making regarding assessment and intervention
Ninety-seven percent of respondents reported that client preference ‘always’ or ‘frequently’ impacted their decisions regarding choice of assessments and interventions. Advice from occupational therapists colleagues (81%) and MDT members (78%) also frequently influenced decision-making (Figure 3). Fifty percent reported that time frames in patient pathways always or frequently affect their choices and 35% report that pressure to discharge from the service always or frequently affect how they assessed or treated people with stroke. FG participants reported similarly in relation to patient pathways: P1: You have a patient for six weeks or whatever amount of time it is. But sometimes even that’s still very early days to be thinking about work.
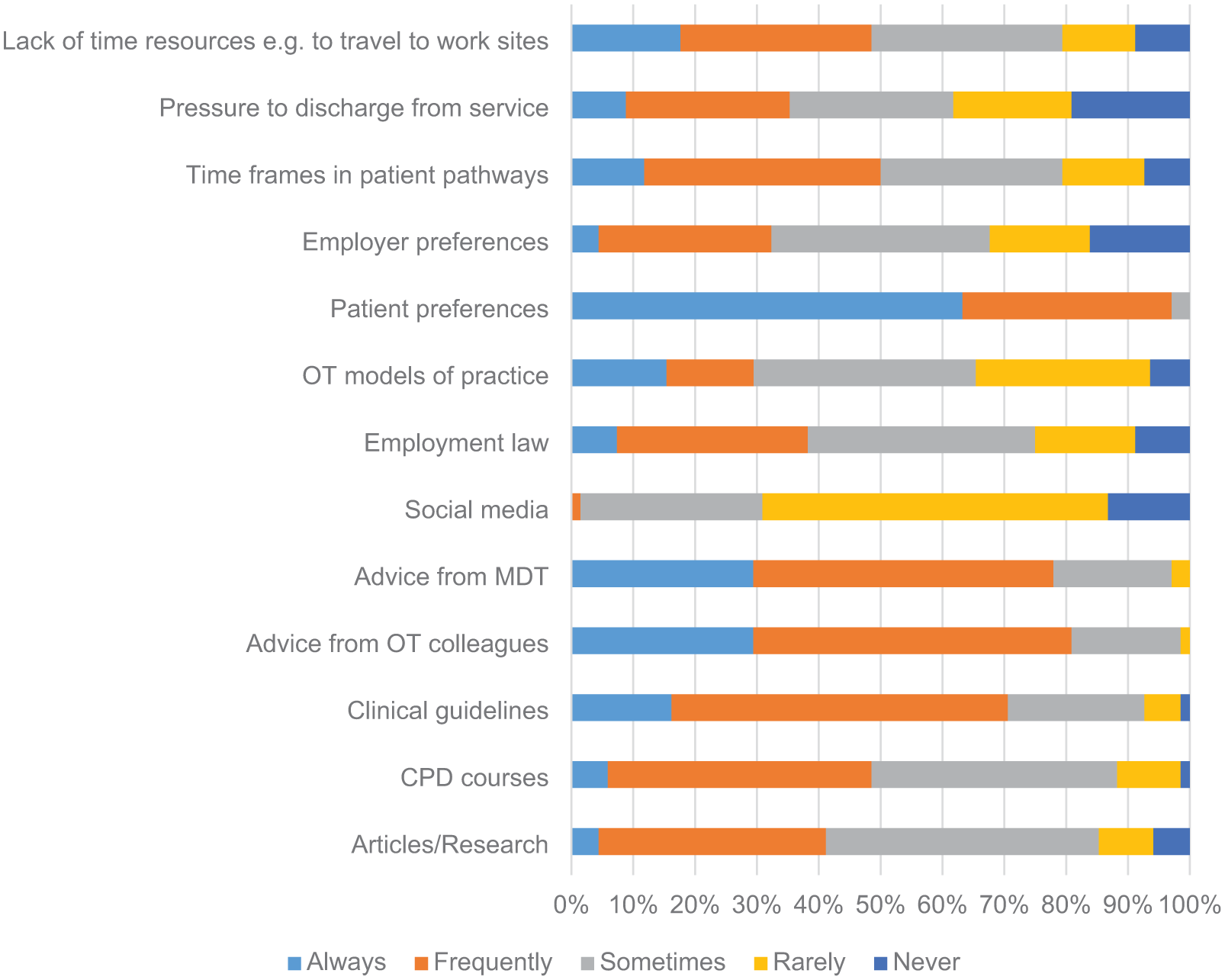
Factors affecting clinical reasoning.
Waitlists were mentioned by all participants as being challenging, particularly for patients on ‘Early Supported Discharge’ (ESD) rehabilitation pathways. These stroke survivors may require ongoing intervention after a period of intense rehabilitation, involving referral to specialist VR services, which often have lengthy wait lists: P1: Sadly the services end when the services end generally, and I think that’s the hard bit and I think for me it’s definitely that in between the ESD and the vocational rehab services.
Prioritising work-related goals over other areas of occupational therapists intervention within limited resources was also reported by one participant as impacting choice of intervention: P4: You’re so focused on discharge planning and all those other things and when you’re working on your priority list
Perceived confidence levels
Survey respondents strongly agreed that occupational therapists have a key role in supporting people with stroke return to work (98%) and that it is their professional responsibility (90%). Overall, occupational therapists felt confident working with this group, with 71% ‘agreeing/strongly agreeing’ with this statement. When asked about confidence in relation to how their clients will manage on return to work based on recommendations made, less respondents felt confident (47%). Survey respondents were considerably more confident providing client-related interventions than employer-related interventions, 74% and 47%, respectively. Only 37% reported being confident to discuss work-related legislation. All FG participants agreed that they learned mostly while ‘on the job’ and stated that they needed more education at university level and continuous professional development opportunities: P4: I can’t recall ever learning or having any of that experience from the university so it’s more experience through learning whilst on the job P1: I think certainly more training will be good . . . having more conferences around vocational rehab.
Discussion
The purpose of this mixed-methods study was to describe occupational therapists practice with people with stroke who wish to return to work, identify confidence levels and explore occupational therapists perceptions and experience of working in this area.
The most frequently reported practices generally assessed and treated impairments associated with stroke such as physical weakness and cognitive impairment. Interventions which specifically address work and employers were completed less frequently, with participants feeling less confident with employer-related interventions. These findings align with those of Scott and Bondoc (2018) in the United States, and with Radford et al. (2025) in relation to usual care in the United Kingdom. The lower frequency of employer and work-related practices is concerning as research and guidelines recommend both liaison with employers and work specific interventions (Donker Cooles et al., 2016; NICE, 2023; Ntsiea et al., 2015 and Trexler et al., 2010).
As identified in the current study, a possible explanation may be related to issues regarding consenting to employer contact, anxiety about workplace perceptions and limited resources and flexibility
Timing of assessment and intervention is considered important. Focus group occupational therapists felt the acute setting was too early to address return to work, echoing O’Keefe et al. (2021) in Australia. Similarly, Radford et al. (2025) found mixed views on early intervention among occupational therapists. Pressure to discharge from services and requirements to prioritise discharge-related tasks were discussed as barriers to providing VR in inpatient settings. Wolf et al. (2009) agreed that occupational therapists have had to conform to medical models of practice with a focus on impairment and activity, rather than participation in daily life. O’Keefe et al. (2021), Van Velzen et al. (2016), and Grant (2016) found early work-related assessment and intervention to be feasible, although more trials are required to determine effectiveness (Radford et al., 2025). Occupational therapists in leadership and management roles can consider how work-related interventions can be prioritised and appropriate resources made available to allow conversations about return to work to commence as early as possible.
The most frequently reported assessment of cognition was a cognitive screen. The recent National Clinical Guidelines for Stroke (2023) recommend people with stroke returning to work receive a cognitive assessment. Studies suggest that more sensitive cognitive assessment, exploring higher-level cognitive functions may be required for people who wish to return to work (Westerlind et al., 2019). As cognitive impairment is a known predictor of poor outcome for return-to-work post-stroke (Edwards et al., 2018), it is positive that this is being addressed by UK occupational therapists, but consideration to the sensitivity of the chosen tool is required, to ensure cognitive difficulties in people with mild stroke are detected. The unique expertise that occupational therapists can provide by employing standardised functional assessments may be helpful, as each stroke survivor’s job role will be unique. This type of assessment was reported less frequently in this study and may indicate additional training requirements.
Assessments and interventions addressing physical impairments post-stroke were reported frequently, as in Scott and Bondoc’s (2018) US study. Despite addressing physical impairments, fewer occupational therapists made recommendations to adapt the physical environment at work or order equipment/assistive technology. Discussion in the focus group of this study may explain this. Occupational therapists spoke about difficulties sourcing work-specific equipment to support people with stroke. The UK Government’s Access to Work scheme offers specialist equipment aimed at facilitating individuals’ return to work (Department for Work and Pensions, 2024). However, the scheme has faced criticism. Prolonged waiting times, ineligibility of individuals employed by government-funded organisations and the requirement for employers to make partial financial contributions are common barriers faced by people with disabilities (Disability Rights UK, 2025). It may also be possible that stroke survivors and occupational therapists in non-specialist VR services have limited awareness of it.
Fewer participants reported completing interventions that address the emotional demands of returning to work, although anxiety when returning to work has been identified as a challenge (Brannigan et al., 2017). Occupational therapists, with unique training in physical and mental health, can play a leading role in addressing these difficulties. Miles and Morley (2013) suggested that occupational therapists sometimes view their roles as either ‘physical health’ or ‘mental health’ and separation of NHS services into physical and mental health settings has likely contributed to this.
Few participants reported that they always or frequently complete work site visits. Post-pandemic, people are more likely to be home working; therefore, work site visits may not be as indicated. The expansion of telehealth and virtual technologies may also reduce time and cost associated with work site visits to make these interventions more feasible, although occupational therapists must remain cautious regarding digital exclusion and advocate for equitable access to digital technology.
Stroke survivors also report feeling worried and embarrassed about stroke symptoms on return to work (Brannigan et al, 2017) which may impact their decision to have a workplace assessment and liaison with employers/colleagues. Radford et al. (2025), in a large randomised controlled trial (n = 583), reported that only 40% of individuals with stroke consented to occupational therapists contacting their employers, although the reasons for this were not discussed.
Participants of the focus group outlined how flexible working during the pandemic benefitted people with stroke as employers became more receptive to home working and differing work patterns. Flexible hours, phased return periods and home/hybrid working can help to manage symptoms such as fatigue and cognitive change. Flexible working is considered a reasonable adjustment, which is a legal requirement under the Equality Act (2010). Employee advocacy groups are campaigning for flexible working patterns to be considered as the default option for all workers (Chartered Institute Personnel and Development, 2023; Trade Union Congress, 2021). A Trade Union Congress report in 2021 reported that 63% of workers with a disability found that home working in 2020 gave them greater control of their working conditions, 40% reported that it reduced fatigue levels and 90% reported they would like to continue home working. Occupational therapists’ awareness of changes in working patterns/culture will be important in advocating for people with stroke.
Many challenges were reported in both survey and focus group aspects of this study, one of which was lack of specialist training. Due to the complexities of returning to work post-stroke, it is a complex intervention and thus more training and specialist roles should be considered. Results of this study also suggest that those with more years of experience have increased knowledge of work-specific practices and confidence in this complex area. Since data collection, a VR toolkit (NHS England, 2024) has been launched, aiming to describe differing levels of VR in stroke rehabilitation. Further research regarding its implementation is needed.
Implications for practice
Occupational therapists in this study reported reduced confidence when engaging with employers and conducting work-specific assessments and interventions with younger stroke survivors. This appears to be linked to gaps in knowledge and limited experience in this complex area of practice. Addressing this issue requires targeted training and continuing professional development. This should include training in the use of standardised functional assessments, appropriate work-related assessment, VR and occupation-focused interventions that address the emotional aspect of returning to work.
Remote and technology-assisted interventions present potential avenues for reducing time and resource constraints. Further high-quality research and trials are required to establish their efficacy. It is essential that occupational therapists remain aware of evolving patterns of work and workplace cultures, enabling them to effectively advocate for flexible and inclusive employment opportunities for individuals with stroke.
The implementation of these approaches will necessitate investment in training, resources and sustained supervision, particularly in contexts where VR services are underdeveloped. Leadership within the profession is vital and occupational therapists in senior or managerial positions play a critical role in developing practicing occupational therapists confidence, promoting VR as a priority and facilitating the development of specialist roles within this complex area of practice.
Limitations of the study
There were several limitations to this study including a smaller sample size of 68 respondents in the survey and a single FG of four participants. Recruitment was limited by a narrow timeframe due to the research being associated with a taught master’s program. The researcher initially planned for RCOT to email members directly, but changes in RCOT’s communication policies and specialist section structures at this time prevented this, possibly reducing responses. The UK’s third national lockdown on 6th January 2022 further pressured the NHS workforce, increasing stress and imposing rapidly changing clinical demands (Limoges et al., 2022), which also possible affected recruitment. The focus group was moderated by the researcher, who is a practicing occupational therapists specialising in stroke rehabilitation. Despite several efforts to minimise bias, unintentional researcher bias may remain.
Conclusion
This mixed-methods study offers insight into UK occupational therapy practice in the assessment and treatment of people with stroke who wish to return to work, as well as the experiences of occupational therapists working in this field. The findings indicate that impairment-based assessments and interventions are most used particularly amongst occupational therapists in acute settings, and those with less experience. Evidence suggests that case coordination and work-focused interventions may yield more effective outcomes and align more closely with the core principles of OT. A lack of confidence among occupational therapists when engaging with employers was identified. Developing specialist roles, providing targeted training and prioritising VR may help to address this gap and enhance practice in this area.
Key findings
Occupational therapists’ complete impairment-based assessments and interventions most frequently.
Occupational therapists are less confident to liaise with employers.
Lack of resources and flexibility in stroke services are challenges.
What the study has added
Occupational therapists can consider incorporating more work-specific practices in line with current evidence. This study highlights the need for further training, flexible service delivery and the development of specialist roles.
Supplemental Material
sj-pdf-1-bjo-10.1177_03080226251372738 – Supplemental material for Exploring occupational therapists’ perceptions, current practices and confidence levels in supporting return to work after stroke: A mixed-methods study
Supplemental material, sj-pdf-1-bjo-10.1177_03080226251372738 for Exploring occupational therapists’ perceptions, current practices and confidence levels in supporting return to work after stroke: A mixed-methods study by Paula Reddan, Deirdre Connolly and Louise Keating in British Journal of Occupational Therapy
Supplemental Material
sj-pdf-2-bjo-10.1177_03080226251372738 – Supplemental material for Exploring occupational therapists’ perceptions, current practices and confidence levels in supporting return to work after stroke: A mixed-methods study
Supplemental material, sj-pdf-2-bjo-10.1177_03080226251372738 for Exploring occupational therapists’ perceptions, current practices and confidence levels in supporting return to work after stroke: A mixed-methods study by Paula Reddan, Deirdre Connolly and Louise Keating in British Journal of Occupational Therapy
Supplemental Material
sj-pdf-3-bjo-10.1177_03080226251372738 – Supplemental material for Exploring occupational therapists’ perceptions, current practices and confidence levels in supporting return to work after stroke: A mixed-methods study
Supplemental material, sj-pdf-3-bjo-10.1177_03080226251372738 for Exploring occupational therapists’ perceptions, current practices and confidence levels in supporting return to work after stroke: A mixed-methods study by Paula Reddan, Deirdre Connolly and Louise Keating in British Journal of Occupational Therapy
Footnotes
Acknowledgements
We give our sincere thanks to the participants in this research who shared their time and experiences so generously.
Research ethics
Research ethics was approved by the Royal College of Surgeons Ireland Research Ethics Committee in October 2021. REC 202105011.
Consent
This study consisted of an online survey and focus group. Consent was gained via a question at the beginning of the survey. An invitation at the end of the anonymous survey provided a link to share contact details if interested in taking part in the focus group. Written consent was attained for this part of the study.
Patient and public involvement data
During the development, progress and reporting of the submitted research, Patient and Public Involvement in the research was not included at any stage of the research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors declared no financial support for the research, authorship and/or publication of this article.
Contributorship
PR was the primary researcher and completed the research as part of completion of an MSc in Neurology and Gerontology at the Royal College Surgeons Ireland. LK and DC were PR’s research supervisors and provided guidance on study design, methodology and data analysis. All authors reviewed and edited the manuscript and approved the final version.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.