
Abstract
Participatory research is critical for developing appropriate and effective programs for specific communities. Suicide is a health inequity for autistic people and prevention is a high priority for autistic community members. Using community-based participatory research with autistic partners, we aimed to develop a research-informed, conceptually grounded, and community-supported suicide prevention program for the autism community. The participatory, multistep program development process included regular meetings to integrate existing research with an established intervention framework and was informed by 38 qualitative research interviews with autistic adults, family members, and mental health providers. The development process resulted in a four-part, virtual, education and community empowerment program—Forming Love around Autistic People to Prevent Suicide (FLAPS)—aimed at supporting organizations to engage in multilevel suicide prevention efforts. Participatory research that meaningfully engages autistic community partners can support the development of promising programs to promote suicide prevention for autistic people.
Plain Language Summary
This paper describes work to make a new program to promote suicide prevention for the autistic community. Our team includes autistic people and academic researchers working together as partners. We worked together over several years to make a program based on research and community experience. We learned from an existing program for suicide prevention for Alaska Native youth. We also learned from interviews we did with 38 people including autistic adults, family members, and mental health providers. Through our process, we developed a four-part online program to educate and empower autism community organizations for suicide prevention. The program is called Forming Love around Autistic people to Prevent Suicide (FLAPS). The program has not been tested yet.
Keywords
Introduction
Suicide risk and mental health rank among autistic people’s highest research priorities (Benevides et al., 2020). There is critical need for development in this area, because autistic individuals have an elevated risk of suicidality, including death by suicide and increased suicidal thoughts and behaviors (Cassidy et al., 2021; Santomauro et al., 2024). Recent reviews have identified that elevated suicidality risk is associated with various factors such as autistic traits, co-occurring mental health conditions, constructs from the Interpersonal Theory of Suicide (e.g., thwarted belongingness, perceived burdensomeness), autistic burnout, camouflaging, and emotion dysregulation (Arqueros et al., 2025; Brown et al., 2024; Reid et al., 2024). These experiences of suicidality can begin in early childhood (Schindel et al., 2024) and persist into adulthood, emphasizing the need to consider ways to support autistic people across their entire lifespan.
Historically, most suicide prevention efforts focus on individual screening, crisis care, and direct mental health services for people already experiencing suicidality. Recent autism-suicide efforts have focused attention in these same directions (Reid et al., 2024). While there is clearly a need for improved individual-level suicide prevention tailored to the autistic community and notable recent advancements (e.g., Rodgers et al., 2024), these types of interventions do not address the complex intersecting external influences on suicide risk (e.g., environmental factors such as stigma and discrimination). Thus, there is also a need for advancements that address the full spectrum of prevention, including primary (i.e., preventing onset of suicidality), secondary (i.e., support for those at elevated risk), and tertiary (i.e., treatment for those experiencing suicidality) prevention. Evidence suggests that multilevel community-based interventions addressing a range of community members and their social, environmental, and educational needs are needed to promote broad suicide prevention (Platt & Niederkrotenthaler, 2020).
In alignment with principles of disability justice and advocates’ calls for “nothing about us without us,” it is necessary to partner with autistic people to address topics of importance to the community (Autistic Self-Advocacy Network [ASAN], 2024). Furthermore, the World Health Organization (WHO, 2012) states that effective suicide prevention strategies should involve stakeholders from the outset. Suicide prevention must also be based on a comprehensive understanding of the target community’s needs (WHO, 2012) and address multiple socioecological factors (Centers for Disease Control and Prevention [CDC], 2022). Given these gaps and needs, the current project set out to use a participatory research approach to develop a multilevel program to advance suicide prevention for the autistic community. We considered a broad range of influences on suicide risk and addressed multiple levels of prevention (especially primary and secondary; i.e., suicidality prevention for all autistic people, rather than only for those already experiencing suicidality). This manuscript describes our CBPR approach to program development, which contributes to our team’s long-term goal of reducing suicidality for autistic people throughout the lifespan.
Methods
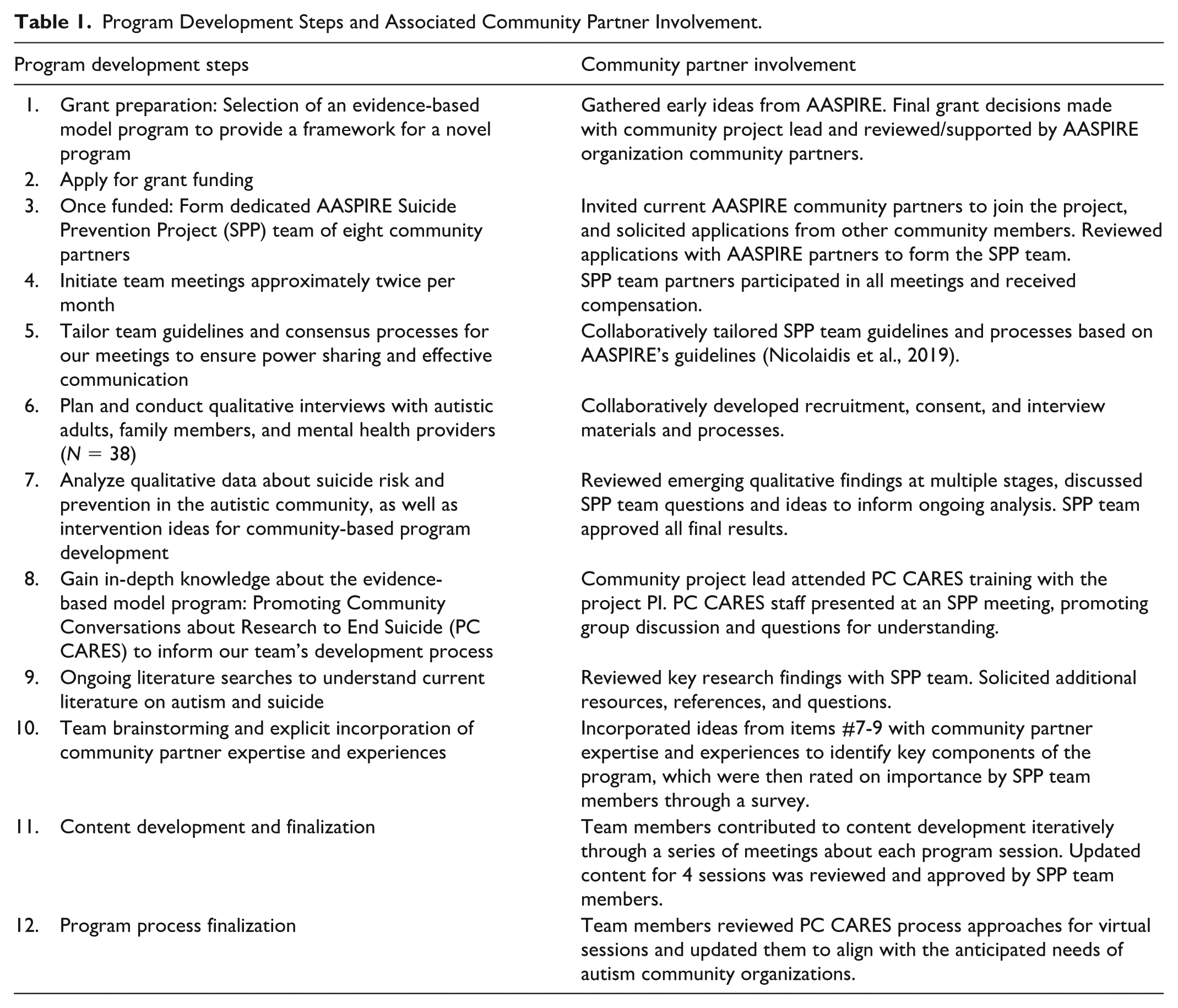
Over a 3-year period, our team used a community-based participatory research (CBPR) approach to develop an autism community-based suicide prevention program in partnership with a group of autistic community partners. Table 1 provides an overview of our team’s 12-step approach and outlines the involvement of community partners at every step.
Program Development Steps and Associated Community Partner Involvement.
CBPR Approach
CBPR is an approach to scientific inquiry involving collaborative partnerships between community members and traditional researchers, leveraging the strengths of both to support every aspect of the research process (Israel et al., 2003). For this project, we partnered with an established organization, Academic Autism Spectrum Partnership in Research and Education (AASPIRE), which has been doing CBPR with the autism community since 2006 (Nicolaidis et al., 2019). In 2022, we formed a project team within the larger organization called the AASPIRE Suicide Prevention Project (SPP). The SPP team includes a non-autistic principal investigator, non-autistic research staff, and eight autistic community partners who collaborate on every aspect of the project. Our team members are diverse in terms of gender (e.g., men, women, nonbinary, transgender), sexual orientation, age (19–62 years), location in the United States, race and ethnicity, age of autism diagnosis, nonspeaking status, and co-occurring mental and physical health conditions. Each team member contributes their varied personal and professional expertise throughout the course of the research.
Our CBPR team held regular meetings over the course of 3 years to inform this program development process (see Supplement 1 for details about our >45 engagement activities). Our approach aligned with PCORI’s Foundational Expectations for Partnerships in Research (Patient-Centered Outcomes Research Institute [PCORI], 2025; see Supplement 2) and followed the AASPIRE guidelines for partnership with autistic adult co-researchers (Nicolaidis et al., 2019). Meetings were conducted via Zoom, and integrated speaking and typing. Together, we tailored AASPIRE’s guidelines to promote our team’s ability to work on the emotionally difficult topic of suicide, aligned with the unique needs of our team members. Our approach included full permission to miss or leave meetings for any reason, opportunity to participate in alternative ways (e.g., individual meeting, over email), invitations to be comfortable during meetings (e.g., stimming, camera on/off), and regular reminders that everyone makes mistakes. We ended each meeting with a “Well-being Wrap-up,” dedicated time to share about things that are personally important to members of the team. All team members’ ideas were listened to and discussed. Final decisions at every stage of the process were made by the group via consensus (i.e., five-finger method; Nicolaidis et al., 2011), which maximizes the integration of each member’s input.
Selection of a Model Program
We selected a model program early in our process to support our funding application. We sought to develop an educational program that could address a broad range of suicide prevention needs within the autistic community. During early planning meetings, AASPIRE members emphasized the importance of environmental influences on suicide risk within the autistic community. Around the same time, the study PI learned about a research-based, multilevel program called Promoting Community Conversations About Research to End Suicide (PC CARES; Wexler et al., 2016). PC CARES is a strengths-based education and community capacity building program that was developed with Alaska Native partners to support suicide prevention at the community level (Wexler et al., 2019). Upon learning about it, the AASPIRE members were extremely enthusiastic about the approach because of its emphasis on discrimination as a contributor to suicide risk and its application of a strengths-based approach that is respectful of the community. This was seen as distinct from many other suicide prevention efforts that focus on individual-level risk factors.
The PC CARES model aims to engage a variety of people who can be a part of promoting mental wellness and reducing suicide risk. It focuses on sharing research information with community members to spark self-directed actions that fit the roles and context of participants, and work to prevent suicide before and after a crisis (i.e., primary, secondary, tertiary), and at multiple levels (i.e., individual, relational, community, societal). PC CARES is organized as a series of learning circles that follow a pattern of activities that include sections focused on: “what does the research show?” “what do we think?” and “what do we want to do?” about different aspects of suicide prevention (White et al., 2022). A central aim of PC CARES is to support the development of strategic communities of practice (Wenger, 1999) which harness the social nature of learning to effect change within participants’ unique environments (Wexler et al., 2016). Evidence for PC CARES demonstrates increases in perceived knowledge, self-efficacy related to suicide prevention, preventive actions, and social networks for prevention (Wexler et al., 2019).
Following AASPIRE members’ enthusiasm and the promising evidence base, we decided to begin the project with PC CARES as a model, acknowledging that our team’s directions and ideas could diverge from PC CARES over time as we prioritized the CBPR development process over adherence to an existing model. Our team received permission and guidance from the PC CARES developers to support our program development efforts. They helped us promote relevant carryover of the core aspects of the model while considering the unique context and needs of the autistic community.
Interviews to Inform Program Development Based on the PC CARES Model
As part of our larger project, our team conducted a qualitative study using semi-structured interviews focused on suicide risk and protective factors, as well as experiences of suicidality, with 38 individuals (N = 16 autistic adults, N = 8 family members, and N = 14 mental health providers). The qualitative interviews are described in full elsewhere (Kirby et al., 2025). The interview results revealed the following core influences on suicidality: negative societal attitudes and social experiences; negative life experiences and stressors, including a lack of appropriate services and supports; and challenging emotions (Kirby et al., 2025). These findings reflect a socioecological model of suicide prevention (Ullman et al., 2021), pointing to the importance of addressing societal attitudes (societal), daily stressors and lack of services (community), negative social experiences (relationship), and emotion regulation (individual) layers throughout the lifespan for autistic people.
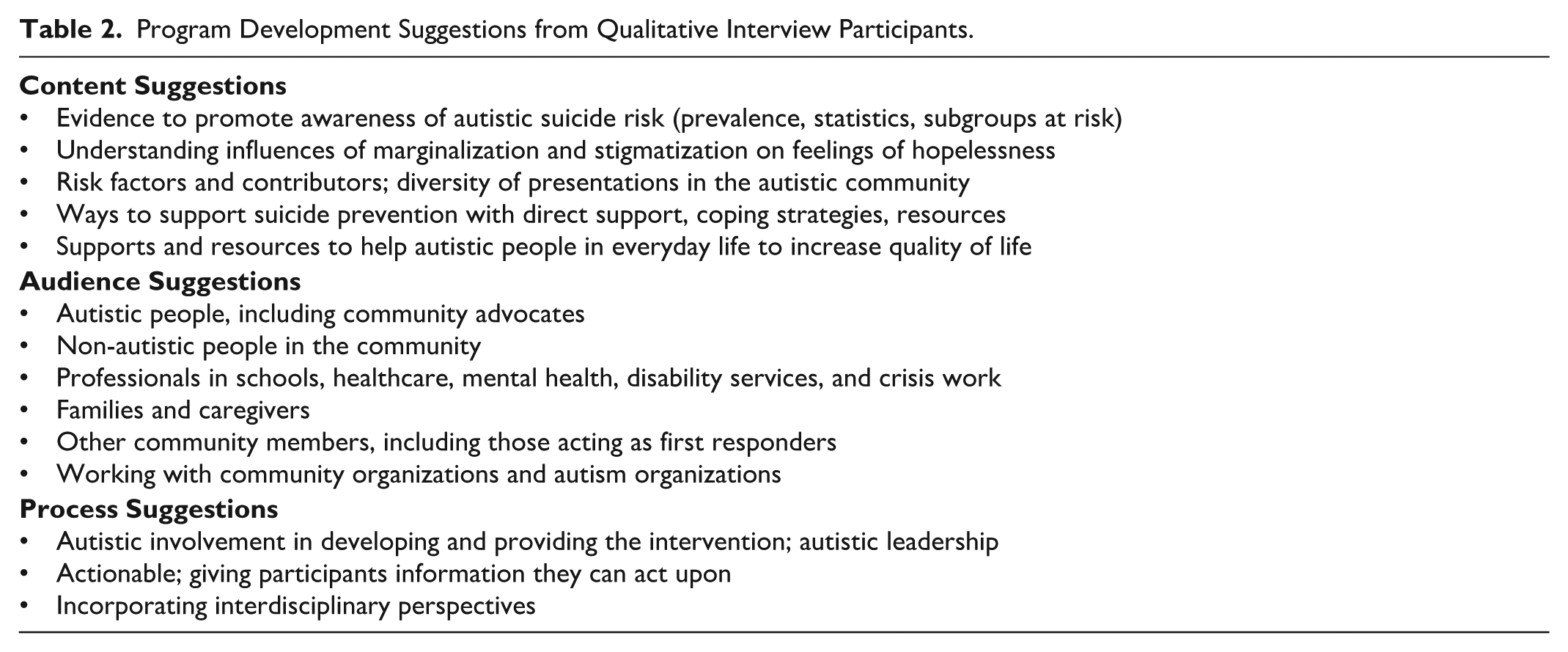
During the last 5 to 15 min of each interview, the interviewer asked the participant about recommendations for a community-based suicide prevention program for the autism community to inform our program development based on the PC CARES model. We conducted a conventional content analysis (Hsieh & Shannon, 2005) of those interview segments and coded participant suggestions. One staff member coded the data, and a second member reviewed them to ensure the codes comprehensively and accurately captured participant responses. The participant recommendations are outlined in Table 2, and include suggestions for program content (e.g., statistics on risk, understanding marginalization, risk factors), audiences (e.g., autistic people, professionals, families), and process (e.g., autistic leadership, interdisciplinary perspectives).
Program Development Suggestions from Qualitative Interview Participants.
Results
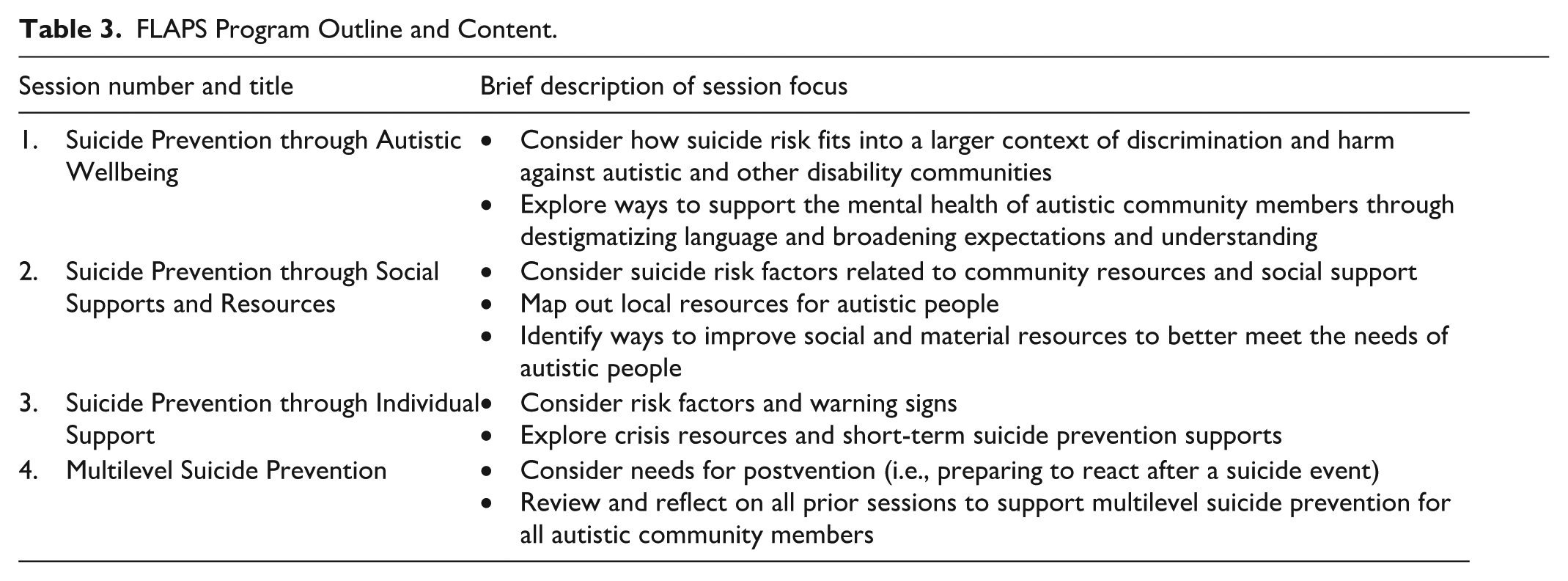
Through our collaborative process, our team produced a four-part virtual training program called Forming Love around Autistic People to Prevent Suicide (FLAPS). The target audience for the program is community organizations already doing autism-focused work (with autistic people of any age), as these types of organizations often integrate several of the specific audience member suggestions and are positioned to make a sustainable difference by leveraging their existing resources and infrastructure. In alignment with interview recommendations as well as the priorities of our team, the program emphasizes autistic community knowledge and should be facilitated by autistic leaders. The overarching goal of FLAPS is to educate and empower community organizations to support broad-based suicide prevention through supporting safe, healthy, and meaningful lives for all autistic people in society.
Each session is designed to provide organizational teams with guidance to engage with research findings and community partner insights based on lived experience (“what do we know?”), their own perspectives (“what do we think?”), and plan contextually relevant actions (“what do we want to do?”). Sessions follow a socioecological perspective (CDC, 2022)—beginning from the outer level influences of societal-level treatment and working inwards toward individual influences and needs. Program materials include slides showing key content and other handouts to assist organizations with reflection and action planning. Table 3 contains an outline of the program sessions.
FLAPS Program Outline and Content.
Discussion
This brief report describes the CBPR process undertaken to develop a community-based suicide prevention program for organizations serving the autistic community. Our team included academic researchers and community partners who worked together to develop a research-informed, conceptually grounded, and community-supported program. Our process aligned with recommendations from the WHO (2012), CDC (2022), and existing research knowledge (e.g., Platt & Niederkrotenthaler, 2020) about promising avenues for suicide prevention by incorporating community partners in every stage of the process, addressing multiple levels of influences using a socioecological perspective, and developing a multilevel community-based program.
The program name was chosen by SPP community partners to emphasize the aim of providing information and resources to form support around autistic people through more caring and understanding throughout their lives. The acronym FLAPS also has meaning to the community partners, as flapping—a form of stimming—is a stigmatized action (Turnock et al., 2022) that some autistic people engage in. Choosing a name that re-claims a word previously used against the community could be seen as a subversive act.
Our team had previously identified the importance of neurodiversity-affirming perspectives for promoting suicide prevention in the autistic community (Kirby et al., 2025). Based on these findings, we infused neurodiversity-affirming language and conceptualizations about influences on suicidality throughout the FLAPS program. The autistic community partners were critical in ensuring this framing was accurate and respectful throughout every component of the program. The values of neurodiversity align with occupational therapy values of person-centered practice by promoting individuals’ strengths and capabilities, creating supportive environments that promote meaningful participation in occupations, and moving away from practices that focus on normalizing autistic individuals to align with neurotypical standards (Patten et al., 2024).
Our team’s planned future directions include pilot testing the FLAPS program for community organization participants and led by autistic facilitators. Limitations of the current report include that the program has not yet been tested. However, it is based on research findings, incorporates community expertise, and is built upon an evidence- and theory-informed framework that has demonstrated success with forming effective communities of practice for suicide prevention with marginalized populations. Therefore, it is a promising direction for community-based suicide prevention for the autism community.
Conclusion
Through an active partnership between autistic community partners and academic researchers, our team produced a virtual training program for autism community organizations ready for pilot testing. The program’s focus on community empowerment and education with organizations already working with autistic populations offers an opportunity to create sustainable, supportive environments that can help reduce suicide risk and enhance well-being for autistic individuals. The programs’ strengths include its incorporation of community priorities and research findings (published and from our own interviews), a broad prevention approach, and addressing multiple levels of influence on suicidality for the autistic community. Initial pilot testing and refinement will allow for evaluation of its potential for effectiveness and broader implementation.
Supplemental Material
sj-docx-1-otj-10.1177_15394492251391675 – Supplemental material for Participatory Development of a Suicide Prevention Program for Autism Community Organizations
Supplemental material, sj-docx-1-otj-10.1177_15394492251391675 for Participatory Development of a Suicide Prevention Program for Autism Community Organizations by A. V. Kirby, K. Feldman, B. Duncan-Ishcomer, R. Kripke-Ludwig, A. Joyce, W. Lee, K. Rodriguez, Z. Siddeek, A. Darlington, A. Atisme, W. Clark, K. Murthi, L. Wexler and C. Nicolaidis in OTJR: Occupational Therapy Journal of Research
Supplemental Material
sj-docx-2-otj-10.1177_15394492251391675 – Supplemental material for Participatory Development of a Suicide Prevention Program for Autism Community Organizations
Supplemental material, sj-docx-2-otj-10.1177_15394492251391675 for Participatory Development of a Suicide Prevention Program for Autism Community Organizations by A. V. Kirby, K. Feldman, B. Duncan-Ishcomer, R. Kripke-Ludwig, A. Joyce, W. Lee, K. Rodriguez, Z. Siddeek, A. Darlington, A. Atisme, W. Clark, K. Murthi, L. Wexler and C. Nicolaidis in OTJR: Occupational Therapy Journal of Research
Footnotes
Acknowledgements
This work was supported by the Academic Autism Spectrum Partnership in Research and Education (AASPIRE) and their Community Council. The authors thank Allison Charba and Francesco Vales who contributed during the early stages of this study. We also thank the PC CARES team and Steering Committee members.
Ethical Approval
This study was approved by the University of Utah IRB (Number: IRB_00127173).
Informed Consent
All participants provided informed consent.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the National Institute of Mental Health under Award Numbers K23MH123934. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statements
Given the sensitive and personal nature of the interviews, the data is not publicly available.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.