
Abstract
People with mental health issues are three times more likely to be unemployed. The purpose of this community-engaged research project was to address an issue brought up by our community partner that people with mental health challenges were restricted from participating in employment. A photovoice study was conducted to answer the research question: what facilitating factors and hindering factors of employment were encountered by people with mental health challenges? Seven participants recruited by our community partner completed three rounds of photo assignments and group meetings. Study findings revealed that mental health conditions presented challenges in finding, acquiring, and retaining employment, and that self-management strategies and a safe work environment were critical to facilitate employment participation. A community advisory group was informed about the study findings. We then hosted photovoice exhibit events to increase awareness about the employment issue for community people. Recommendations for conducting community-engaged research are discussed.
Plain Language Summary
Through partnering relationships, university researchers and community organizations worked side by side with a big goal to solve the job issue experienced by many people who experience mental health challenges. Using a research method called photovoice, a small group of people took a series of photos that represented their experiences of finding and keeping a job. Through facilitated group discussions, this group created photos and told stories behind them. Another group of community advisors got together and used their skills and resources to solve the issue. They decided to host photo gallery events using the photos and stories created by the photovoice group. The photos were displayed at three different locations and online, and more community organizations supported the project by using their resources to make more people learn about the events. This university-community project provided great opportunities for community people to take part in addressing the community issue.
Introduction
Employment is a major life domain valued by society. It provides not only financial stability but also health benefits, including social connectedness, daily structure and routine, a sense of worth, higher self-esteem, better mental well-being, and community inclusion (American Occupational Therapy Association [AOTA], 2020; Drake et al., 2022; Modini et al., 2016).
Most people with mental health challenges want to engage in meaningful work (Harvey et al., 2013; Modini et al., 2016). However, employment rates in European countries were only 40-60% for people diagnosed with bipolar disorders, and 10-30% for people diagnosed with schizophrenia (Holm et al., 2021). In the US, approximately 80% of people receiving mental health services were unemployed (National Alliance on Mental Illness, 2014). People lived with mental health issues are at least three times more likely to be unemployed than people without (Brouwers, 2020).
Many barriers to participation in employment have been identified for people with mental health issues, including educational disadvantage due to age of onset, social discrimination toward mental health issues, discriminatory attitudes among employers and co-workers, benefit disincentives, and lack of support from mental health professionals (Brouwers, 2020; Harvey et al., 2013; Secker et al., 2001). For facilitating factors, Individual Placement and Support (IPS) is an example of an evidence-based approach of supported employment (SE) for people with mental health challenges (Drake et al., 2012). The IPS intervention was developed to help people with mental health issues gain competitive employment by placing them in a workplace with on-the-job training that is gradually decreased as people acquire relevant skills and confidence. Multiple randomized-controlled trials (RCTs) and systematic reviews have confirmed efficacy and effectiveness of the IPS, showing favorable employment-related outcomes such as finding jobs faster, working longer hours, earning more money, and achieving longer job tenure (Drake et al., 2012, 2022; Frederick & VanderWeele, 2019; Modini et al., 2016). Unfortunately, many people with mental health issues in the US still do not have access to the IPS intervention due to funding; unemployment remains an urgent public health crisis and a major social determinant of health for people with mental illness (Brouwers, 2020; Compton & Shim, 2014; Drake et al., 2022).
Occupational therapy (OT) is a complementary behavioral health service that helps people recovering from mental health issues achieve their full potential, including participating in employment (AOTA, 2020; Persch & Fossey, 2025). OT practitioners view employment as a fundamental area of human occupation. They collaborate with clients to address barriers to employment by identifying occupational performance issues and creating individualized adaptive strategies. Interventions involving self-analysis and developing and practicing strategies have shown preliminary evidence in supporting employment for people with mental health challenges (Edgelow et al., 2020).
The purpose of this community-engaged research (CER) project was to address the issue that people with mental health challenges were restricted from participating in employment. This was an issue that was brought up by and of great concern for our community partner. Informed by community-based participatory research (CBPR), an academia-community partnership was established and a community engagement grant was secured to address the employment issue. The partners jointly decided to conduct a photovoice study (see Methods for details) to explore the experience of employment participation through the lens of people with mental health challenges. The research question of the photovoice study was: what facilitating factors and hindering factors of employment were encountered by people with mental health challenges? With the grant, a community advisory group was then formed, of which the majority of members had lived experience. The group was informed of the findings of the photovoice study and met regularly to identify a plan of action to address this community issue.
CBPR was the framework of this project. It is a collaborative research approach involving equal partnership between researchers and people of the community (Minkler & Wallerstein, 2008). CBPR builds upon strengths and resources in the community to promote social change and improve health. Solving employment issues cannot rely solely on government-funded services or the expertise of a single health profession such as OT. CBPR offers an alternative framework to examine the employment issue and develop solutions to address it.
This paper will present the results of the photovoice study as well as the preliminary advocacy work by the community advisory group. Lessons learned through this academia-community partnership will also be discussed.
Methods
Research Design
Guided by CBPR, the partners of this project decided at an early stage to use the photovoice method to depict the lived experiences of people with mental health challenges. Photovoice is a qualitative research method that involves giving cameras to research participants to take photos of community issues (Wang & Burris, 1997). As a method of CBPR, photovoice sees research participants as people with the most knowledge of phenomena under study. Photovoice values community strengths, collaborative relationships between researchers and community partners, and empowering community people (Teti et al., 2012; Walton et al., 2012). Photovoice empowers study participants from marginalized groups like people with mental health challenges to share their perspective through photos and their narratives. This perspective is often overlooked in research, health service delivery, and elsewhere in society. Photovoice is an appropriate research design in studies involving people with mental illness (Han & Oliffe, 2016).
The photovoice study was the first step in this CER project. The study results were used to inform a community advisory group to develop a plan of action to address the employment issue.
Participants: Photovoice Study and Community Advisory Group
Participants of the photovoice study were recruited from the community partner, a consumer-operated services program (COSP; Substance Abuse and Mental Health Services Administration [SAMHSA], 2019) for “peers,” or people with lived experience who have navigated mental health services. Peers who met the inclusion criteria were invited to participate in the study: (1) 18 years of age or older, (2) capable of operating a digital camera after a brief instruction, (3) capable of participating in group discussions, and (4) willing to complete all study tasks including an orientation session, three photo assignments, and five group meetings. The targeted sample size was 6 to 8, which was determined to achieve rich opinions and experience during group discussions while allowing for optimal engagement by individual participants.
Members of the community advisory group were individuals, whether affiliated with the community partner or not, who cared about the employment issue. The project partners decided that the majority of this group would be people with lived experience.
Research Instruments
Digital Cameras
Simple point-and-shoot digital cameras were given to each of the participants to take photos for the photovoice study. Using a cord that came with the camera, study photos were transferred onto a computer and then shared on a smartboard for group discussion. No photos were printed throughout the study. As a token of appreciation, participants got to keep their camera after the study.
SHOWED Discussion Guide
The SHOWED discussion guide (Wallerstein & Bernstein, 1988) was used during the photovoice study to facilitate group discussions. The discussion guide contained the following questions:
What do we
What is
How does the story relate to
How can we become
What can we
Study Procedure
Figure 1 depicts the procedure of the photovoice study. During participant recruitment, a peer support specialist electronically circulated the study flyer to peers through emails and newsletters. The peer support specialist also assisted in identifying peers who met the study criteria and encouraged them to attend the study’s Information Session, which was held at the community partner’s building for potential participants to meet the research team and ask questions. The peer support specialist also assisted in participant retention by providing encouragement and making reminder phone calls during the study period.
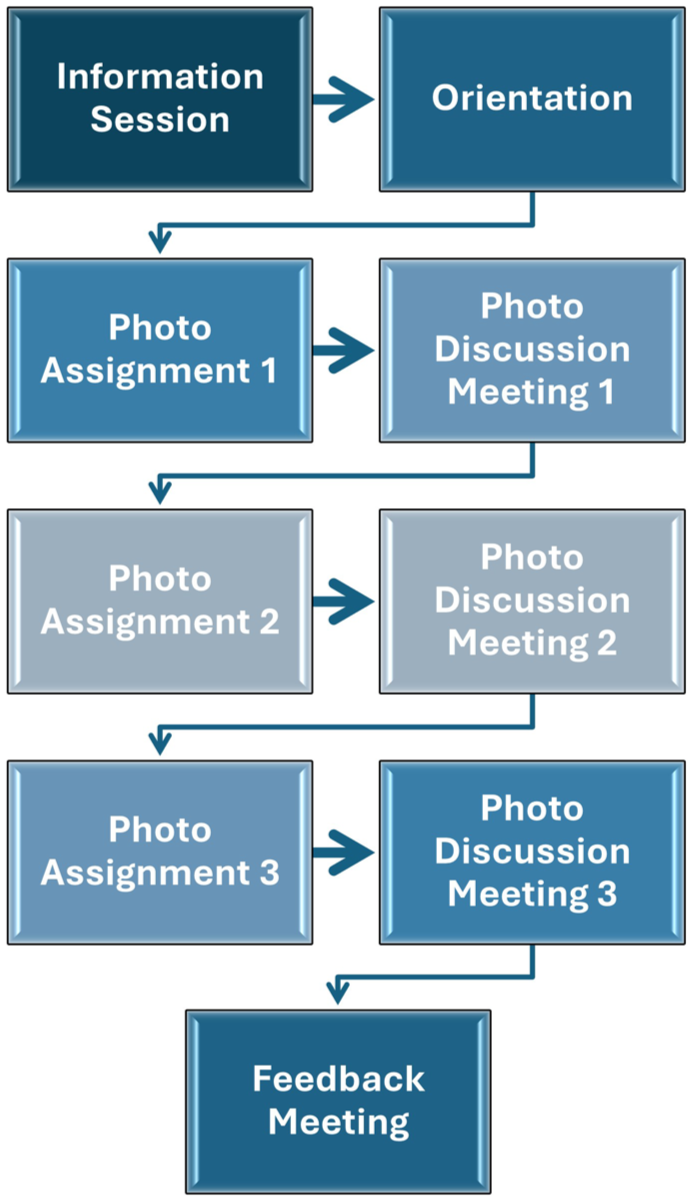
Photovoice Study Procedure
An Orientation Session (Week 1) was held one week after the Study Information Session. Informed consent was obtained and participants received instructions for operating the digital camera and tips to ensure privacy and confidentiality while taking photos for the study. At the end of the Orientation Session, a group discussion was facilitated to determine a topic related to employment for Photo Assignment #1. The participants were asked to take 6 to 24 photos on their own to complete the photo assignment. One week later, the participants convened for Photo Discussion Meeting #1 (Week 2) to share and describe photos they took. The researcher used the SHOWED discussion guide to facilitate group discussion. At the end of the meeting, participants selected another topic for the next photo assignment to further capture their employment-related experience. The above procedure was repeated until the participants completed three rounds of photo assignments and photo discussion meetings (Weeks 3 and 4). The data collection was concluded with a Feedback Meeting (Week 5), during which the researcher presented preliminary results to participants for feedback to ensure accurate interpretation of data. This is a strategy of member checking used in qualitative research to increase credibility of study findings (Creswell & Miller, 2000). All three photo discussion meetings and the feedback meeting were video recorded, and verbatims of group discussions were transcribed.
A community advisory group was formed after the study. The group met regularly to review the photovoice findings and identify a plan of action.
Data Analysis
A computer program, NVivo 14, was used to assist in analyzing qualitative data gathered in the photovoice study, including meeting transcriptions and photos. All photos were assigned with a unique number and coded based on participant narrative (e.g., the reason a photo was taken or the meaning presented by a photo).
Grounded theory methods including open coding, axial coding, and selective coding (Corbin & Strauss, 2008) were used to derive categories and themes as they emerge from the research data. Based on relationships identified among categories and themes, a theoretical description of participant experience of employment participation was developed. Following investigator triangulation (Farmer et al., 2006), the Principal Investigator and a doctoral OT student independently coded a transcript and then met to review and find consensus for codes and their meaning. The evolved codebook was used to code the next transcript. The process was repeated until all transcripts were analyzed. As new codes were added, previous codes were revised, and emerging relationships and theoretical descriptions were deliberated. Analysis results evolved over time were shared with the community partner for input.
The photovoice study was approved by the institutional review board (IRB) of the academia partner of this community-engagement research project.
Results
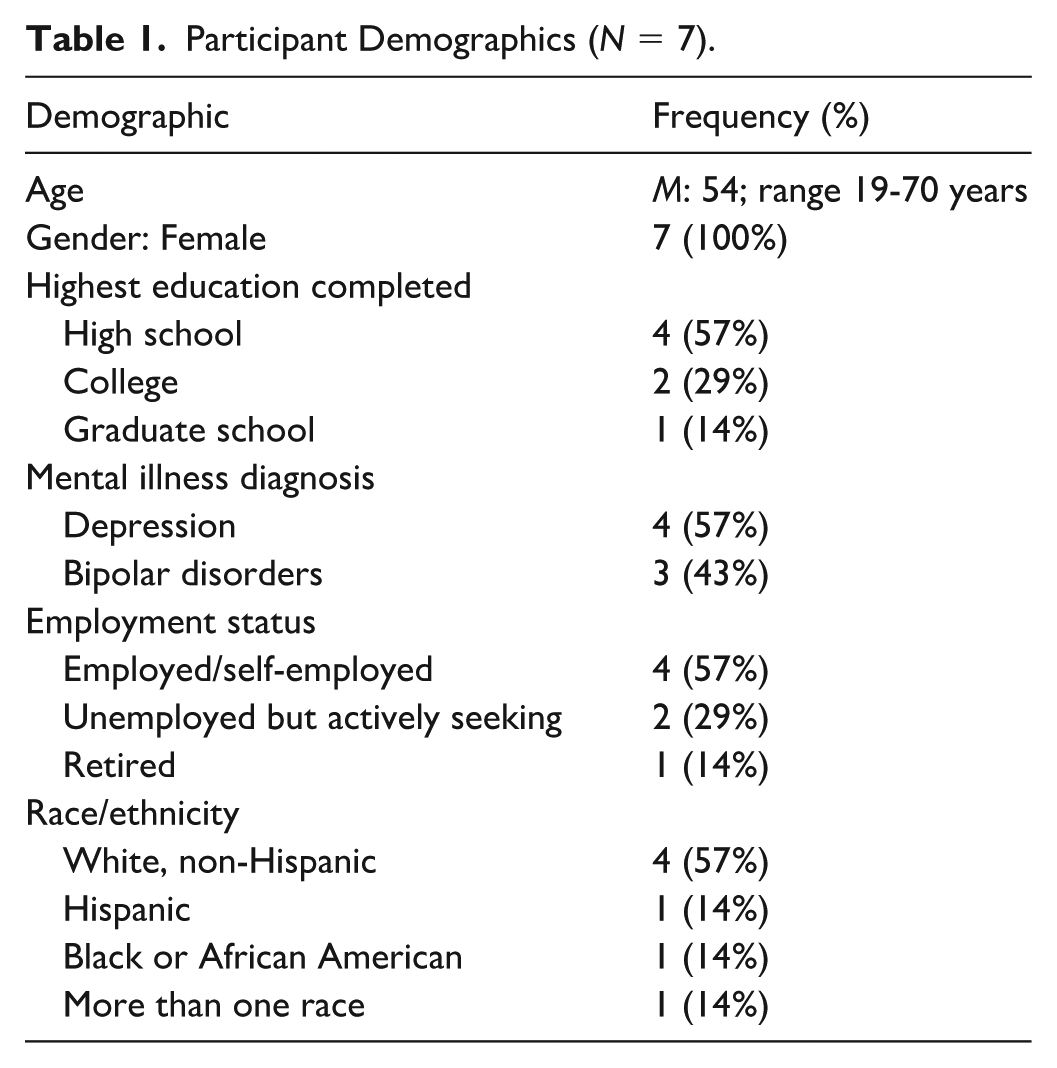
Although the photovoice study did not target any specific gender, all our participants happened to be female. They were aged between 19 and 70 years, with high school education or higher. The self-reported mental disorder diagnoses included depression and bipolar disorders. They were either employed, unemployed but actively seeking, or retired. Refer to Table 1 for additional demographic details.
Participant Demographics (N = 7).
The topics for the three photo assignments chosen by the photovoice participants were: (1) journey to employment, (2) resilience- fighting against the odds, and (3) things to help me maintain composure. The seven participants produced a total of 218 digital photos, and each took 3 to 24 photos for an assignment. All photos were shared during group meetings. A total of 66 codes emerged with 561 references (i.e., text parts in the transcripts assigned with a code), and 40 relationships (i.e., connections of two codes) with 72 references were identified. This paper describes the three key themes emerged from the photo discussion meetings: impact of mental health challenges on employment, employment-related self-management for health and wellness, and envisioning a better workplace.
Theme 1. Impact of Mental Health Challenges on Employment
Mental health challenges impose a negative impact on seeking, retaining, and engaging in employment. The study participants captured several photos of mental health challenges that had negatively impacted their employment journeys, including depression, anxiety, and insomnia. For example, “I do excessive sleeping as a form of avoidance. When I’m stressed, I curl up in my bed. My bed is my safe place”; “This (an analog clock with arms) is anxiety going on. It just keeps going round and round. You’re rapid through thoughts and you can’t stop it”; and “That (a phone screen showing time) was at 3:25 in the morning. I have really bad insomnia. . . you know, not everyone is just lazy. Some people are exhausted because they can’t go to sleep.”
“There Is Not Much Out There for Me”
Given their mental health challenges, the study participants reported scarce employment opportunities that they could apply for or be competitive in the job seeking process. “I graduated in 2013, back at the Workforce (the state’s vocational rehabilitation [VR] program) looking for a job. . . all the things that public admin can do and I’m still unemployed.”
The prolonged unemployment presented a financial desperation that led multiple study participants to seek alternative methods to make ends meet, such as donating plasma. It also led to a sense of hopelessness that they would never be able to gain employment. “That was my dog’s cage. . . to represent being stuck, locked in place, and having trouble breaking out of the wrath. . . All that stuff comes up when I start looking for jobs and there’s not much out there (see Figure 2)”.
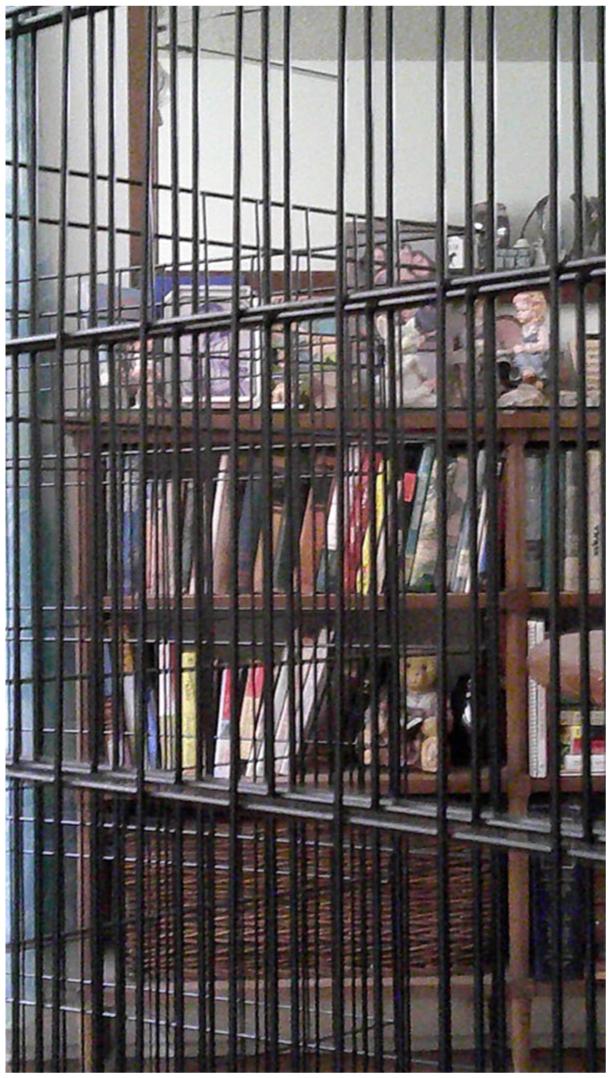
Employment Barriers as a Wrath Unable to Break Out
Difficulties to Retain a Job and Frequent Job Changes
For those study participants who had been hired and participated in work, they had difficulties retaining a job and experienced frequent job changes.
I didn't have a vehicle. . . I live with anxiety. I would start a job, get through two or three days of training. They would give us tests and quizzes. It would give me anxiety so bad that I would leave during lunch and wouldn’t come back. I have a lot of memories of bus stops.
Homelessness and Incarceration in the Past
Multiple participants of this study had experience of homelessness and incarceration, both of which are often associated with or secondary to mental health challenges. For participants who experienced homelessness, employment was a goal beyond reach.
I have a hard time thinking about employment. I mean I have that in mind, but for a long time I didn’t have any work because I was homeless. Now that I have a place to live, maintaining that life is my job.
Past incarceration presented an additional barrier during the employment seeking process. “That is a birdcage, reflecting I did my time in the federal prison. . . the background check came back and I’m told that I either have to separate or . . . So definitely a barrier to me.” Having a criminal record can make it even more challenging to get a job.
Theme 2. Employment Related Self-Management
This theme represents the practices that the study participants engaged in to support seeking and retaining employment as they lived with mental health challenges. This includes problem-solving strategies, for example, “This is the time (a photo showing an analog clock) that I have to leave to get to work on time. So I have a clock 30-inches big throughout my house for my time management.”
Seeking Self-Growth and Developing Positive Self-Concept
Additional self-management practices included seeking self-growth and developing positive self-concept as the participants overcame barriers of employment participation.
Sometimes we have to look at ourselves in the mirror. And understand who we are and where we are in life. It’s not always easy, but you have to know yourself before you can do anything. . . And that’s where you begin. That bridge. . . is a symbol of me crossing over. You know, I left my old life behind. I don’t have to apologize for it. To me, that’s also growth and moving forward and that bridge signifies what I keep looking ahead to and that’s what keeps me calm because I gotta keep moving forward. So I just have to keep going.
“Stop and Slow Down”
This refers to several self-management practices shared by the participants that support seeking and retaining employment by taking the time for self-care and maintaining health and well-being. “To me, that’s taking a walk, going outside. . . stopping to smell flowers. Stopping this to notice the bees, to notice everything.” The participants engaged in various hobbies such as painting, listening to music, reading, beading, and collage making, which served as their coping mechanism, self-affirmation, and motivator. A participant commented that “sometimes we don’t give ourselves permission to just do something fun,” an especially critical reminder for people struggling with employment.
The study participants shared additional self-management practices such as connecting with others including family, friends, peers, and pets; maintaining physical health including healthy eating, getting enough sleep and rest, swimming, getting annual physicals and blood work done; and spiritual practices including meditation and bible study.
Theme 3. Envisioning a Better Workplace
The study participants shared a couple of workplace setup examples that would support employees with mental health challenges: (1) “That (water fountain) is a hidden gem in our office. Going out there and just listening to the waterfalls, I can let the world just go away. Center myself and meditate and bring myself back to where I need to be”; and (2) a “Zen Room” with “plants and calming lights and music. . . that you could go to (calm and re-center yourself).”
In addition to physical setups, the study participants expressed the importance of being able to “have a safe place where we can talk about things that may not be the most comfortable” and “work somewhere you feel safe enough if you lose your composure, you’re not gonna lose your livelihood (see Figure 3).” The participants commented that the notion of trauma-informed care may have applications to the workplace and some people could be trained to properly respond to mental health issues at the workplace.

Calling for A Safe Space in the Workplace
The participants discussed some alternative forms of employment that may benefit people with mental health challenges, such as part-time jobs, remote working, as well as the recently emerging option of being a peer support specialist. Yet the participants also noted the pros and cons for each form of alternative employment. For example, part-time jobs may come with less time commitment, but the earnings may not satisfy one’s financial goals; and remote working allows one to work flexibly from anywhere, but it requires good time management and skills of virtual communications and using technology. Some study participants expressed interest in exploring vocational programs such as one offered by a local psychosocial clubhouse.
Preliminary Work of the Community Advisory Group
After the photovoice study was completed, a community advisory group was formed and informed with the study findings. The advisory group comprised of 7 members, including a board member of the community partner, two photovoice participants, a mental health professional, a staff member from another organization, an OT student, and the Principal Investigator. Five of the members have self-identified as having mental health challenges.
The group met bi-weekly to identify a plan of action to address the issue that people with mental health challenges were restricted from participating in employment. Although there were many possible ways to address this community issue, the group focused on developing two advocacy projects: (1) seeking grants to provide training to help demystify mental health challenges for employers and employees, and (2) increasing the community’s awareness about this issue through photo exhibit events. The latter project made some progress through the funding support of another grant and is summarized below.
With the continuing academia-community partnership, we hosted three photo exhibit events using the photos collected during the photovoice study. While maintaining confidentiality of the study participants, a narrative card was displayed by each of the photos to tell the story behind it. The photo exhibit events took place in a university library, a public library, and a non-profit organization on workforce inclusion for people with disabilities. The public library not only publicized the photo exhibit event on their website but also sponsored a kick-off reception, during which a representative from our community partner spoke to the audience on behalf of people with lived experience. The photo exhibit event at the non-profit organization was hosted during the National Disability Employment Awareness Month, and we were invited to speak during their employer’s recognition ceremony to promote employment participation for people with mental health concerns. A web version of the photo exhibit was launched to reach viewers far and wide.
As part of this advocacy project, an online survey was conducted to explore people’s attitudes toward mental health challenges in the workplace, and a QR code to the survey was posted during the events as well as on the virtual photo exhibit. The online survey will remain open until it reaches the targeted sample size.
Figure 4 depicts the academia-community partnership involved in this CER project thus far.

The Academia-Community Partnerships in This Community-Engaged Research Project
Discussion
The purpose of this project was to address the issue that people with mental health challenges were restricted from participating in employment, an issue our community partner was concerned with. Through the photovoice study, participant resilience was evident in the self-management practices developed as they overcame employment barriers. The preliminary work by the community advisory group was advanced by the support of additional community entities who also cared about the issue. In the section below, we will discuss the following points: system barriers to employment, OT in mental health and VR, study limitations, and recommendations for future CER.
System Barriers to Employment
Although not our study focus, homelessness was discussed by multiple participants and presented a system barrier to employment. In a 2023 U.S. Department of Housing and Urban Development (HUD, 2023) report, people with mental illness accounted for 21% unduplicated point-in-time (PIT) counts of the homeless population in the US. A recent systematic review suggested that employment interventions for people experiencing homelessness were at an early stage of development and that collaborating with people with lived experience of homelessness in co-designing employment interventions may help to improve the outcomes (Marshall et al., 2022).
Incarceration was another system barrier shared by multiple participants. There is a high prevalence of mental health issues in the US jail and prison systems, estimated at 44% and 37% respectively (SAMHSA, 2024a). It is critical to promote cross-sector collaboration among behavioral health and criminal justice systems to ensure successful community reentry.
While assisting clients who have experienced homelessness and/or incarceration, OT practitioners must be mindful and apply trauma-informed care (TIC) as they interact with the clients. TIC is a practice framework that is strengths-based and strives to provide a safe space when working with people with trauma histories (Champagne, 2019), including those who have experienced homelessness and incarceration. In peer support, it is understood that many behaviors and thought processes that get diagnosed a serious mental health issues, are in fact trauma responses due to compound trauma. OT can be instrumental in raising awareness that not all behaviors are symptoms and that trauma sensitive approaches can support people being successful in employment. In addition, OT practitioners may educate employers about TIC and promote a safe space in the workplace.
OT in Mental Health and VR
For OT practitioners in mental health, the findings of the photovoice study helped to fuller understand the perspective of people with lived experience. The findings reaffirm the importance of collaborating with clients to develop strategies for managing demands associated with seeking and retaining employment. To strive for optimal outcomes, practitioners must also understand the VR services in their state. VR for people with disabilities is mandated by federal laws (State Vocational Rehabilitation Services Program, 2016), and its program operations and names vary by state. In the state of this partnership, the VR program is named “Workforce Commission.”
This project provided a great opportunity to identify and bridge gaps in services for OT practitioners in mental health and VR. While it is more customary to accommodate physical disabilities at workplaces, job accommodation for mental health conditions such as depression and anxiety is not as commonly known and may not even be considered when needs arise. At the minimum, OT practitioners may help to promote the awareness of job accommodation for mental health conditions among employers and society in general. To assist their clients in seeking and retaining employment, OT practitioners in mental health may support local VR programs by providing assessments needed to support recommendations for job accommodation. OT practitioners in VR must incorporate their expertise to work with clients with physical disabilities and those with mental health challenges. As peer support workers receive more recognition in mental health services (SAMHSA, 2024b), OT practitioners may recommend this employment option to their clients.
Study Limitations
The findings of the photovoice study were based on a small group of participants and thus may not have reached data saturation. Given all the participants were female, findings of the photovoice study may not be transferrable to men. For future research, it is recommended that more participants with diverse demographic characteristics (e.g., males) are recruited. Due to the early stage of partnership, this project has not yet successfully placed anyone to work. Although not the study focus, we recognize other system barriers to employment including benefit disincentives and access to competitive employment, which require further research.
Recommendations for Future CER
Protecting Confidentiality for Community Partners
We were privileged to work with a group of people who participated in the photovoice study and the subsequent advocacy work. It is critical that CER researchers do their best to protect confidentiality of community partners. For example, in response to the public library’s inquiry for one of the photovoice “photographers” to speak at the kick-off reception, we first let the community partner, a peer organization, decide if they wanted to entertain the inquiry. Once an individual admirably accepted the invitation, we responded to the library that the speaker would be a representative from the organization that assisted in participant recruitment, without referencing whether the individual participated in the photovoice study.
Honoring Values and Preferences of Community Partners
Collaborating with community partners requires researchers to strip jargon and let go of their medical-model mind-set to achieve equitable partnerships. In an early stage of the collaboration, we quickly learned a lesson about how common terms used by OT practitioners such as “people with mental illness” convey a power hierarchy, and that our community partner preferred the term “people with mental health challenges,” as evident in the language used for this article. It is critical that CER researchers invest time and effort in understanding and honoring the values and preferences of community partners throughout the collaboration process.
Collaborative Community Building
CER provides a great opportunity for researchers to collaborate with community partners in identifying and addressing pressing issues in the community, which oftentimes do not have easy solutions. Through this academia-community partnership, we were able to rely on expertise that different members brought to accomplish our common goals. For example, a member of the advisory group was from an organization that promoted workforce inclusion for people with disabilities; it allowed us to tap into their planned event to advocate for hiring people with mental health challenges. The OT researcher must recognize the expertise of community members and facilitate a solution owned by the community.
CER vs. the Professional Identify of OT
Conducting CER is likely to apply a non-OT-specific conceptual framework. In this project, CBPR was the guiding framework. This kind of conceptual frameworks may not be fully covered in the OT education, and mastery of such frameworks may benefit from mentorship. Conducting CER may also involve non-traditional OT roles with unclear relevance to OT. For example, we served as a member of the community advisory group and coordinated with local libraries for photovoice exhibit events. The OT researcher must be able to explain to community members what OT is and to the OT audience how they retain their professional identity by applying non-OT paradigms.
Conclusion
People with mental health challenges encounter barriers to employment participation. Through community-engagement research, we were able to collaborate with a peer organization to address this dire issue in the community by conducting a photovoice study to explore the experience of employment participation through the lens of people with lived experience as well as by forming a community advisory group to address the issue. Following the photovoice study, we held three photovoice exhibit events to increase the awareness of this issue, during which two additional community organizations contributed their resources to further elevate the visibility of our advocacy work. CER provides a great opportunity for OT researchers to collaborate with community partners in addressing community issues.
Footnotes
Acknowledgements
The authors are grateful to the study participants for sharing their lived experience. Earlier versions of this project were presented at 2023 Institute for the Integration of Medicine & Science’s (IIMS) Community Engagement Symposium, San Antonio, TX; 2024 AOTA INSPIRE Annual Conference & Expo, Orlando, FL; and 2025 Community Engaged Learning Conference, San Antonio, TX. The authors would like to express their gratitude to the anonymous reviewers of an earlier version of this manuscript for their insightful comments and constructive feedback.
Ethical Considerations
This study was approved by the Institutional Review Board (IRB) of University of Texas at San Antonio Health Science Center (D# 23-447H) on July 20, 2023.
Consent to Participate
All research activities complied with ethical regulations. All participants in this study provided written informed consent prior to enrollment in the study.
Consent for Publication
Informed consent for publication was provided by all study participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this work was made possible by a Community Engagement Small Project Grant (CESPG) Award from the Institute for the Integration of Medicine & Science (IIMS) and the Community Engaged Learning (CEL) grant award from the Charles E. Cheever, Jr. Center for Medical Humanities & Ethics at University of Texas at San Antonio Health Science Center.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.