
Abstract
Clubhouses are an international community-based psychosocial approach to mental health recovery. The aim of the study was to investigate whether the current and future needs of Kindred Clubhouse members were being met. A co-design ethnographic methodology was used. Kindred Clubhouse met many needs of its members. It provides a collaborative, consistent, supportive and inclusive environment fostering connections, skill development, a sense of purpose and the maintenance of health and well-being through peer support and participation in meaningful activities and occupations. Areas for development were expanded operating hours, sufficient meaningful work to sustain a work-ordered day, and support for employment and housing. Lack of stable funding limits Kindred’s ability to fully meet the needs of its members. Despite insecure funding, Kindred Clubhouse is a valued community service offering a member-led recovery approach supporting many of the occupational, social and community needs of people with mental health challenges.
Plain Language Summary
Clubhouses are nonclinical mental health recovery-focused community services where members and staff work together on the many daily life activities that improve and sustain the mental health and well-being of members. Clubhouse principles and standards strongly align with the knowledge and practice of occupational therapy. There are more than 370 clubhouses across 32 countries. This article reports a study of the current and future service needs of the members and staff of Kindred Clubhouse in Hastings, Victoria, Australia. Kindred operates as a not-for-profit community mental health programme offering open flexible access and a place to belong for as long as members choose. This study found that Kindred Clubhouse was providing a valued community service that met many needs of its members. However, there is a need for the expansion of the opening hours of the service, increased opportunities for meaningful work, supported employment and housing. The current lack of secure funding limits the ability of the service to fully meet the current and future needs of its members.
Introduction
The Clubhouse International Model (CIM) is a community-based psychosocial approach to mental health recovery. Originating in the late 1940s in New York as a mutual support group for those facing mental health challenges (Anderson, 1998), it later evolved to Fountain House, leading to its structured programme governed by 37 standards detailed in the International Standards for Clubhouse Programmes (ISCP; Clubhouse International, 2023). The CIM has expanded to more than 370 clubhouses across 32 countries, including six in Australia. While not accredited, Kindred Clubhouse is a community mental health service in Victoria, Australia, that is a member of Clubhouse International and adopts the principles of the CIM.
Clubhouses by design seamlessly integrate into the lives of their members, offering continuity of care that extends beyond time-limited interventions (Clubhouse International, 2023). Membership is open to anyone with a history of mental illness and is voluntary, without time limits (Clubhouse International, 2023). Service users are referred to as ‘members’ rather than the traditional healthcare terms of ‘patients’ or ‘clients’ (Anderson, 1998). The emphasis is on empowerment and equality by viewing members as active participants in their recovery journeys, rather than passive recipients of healthcare services (Gregitis et al., 2010). The clubhouse programme follows a task-focused 9-to-5 ‘work-ordered day’, where members and staff work side-by-side in meaningful community work within and beyond the clubhouse.
Previous research has explored reasons for attending clubhouses. Pernice et al. (2021) found that Clubhouse participation helps reduce isolation and alleviate symptoms through social connection. The respectful, nonjudgemental environment fosters normalisation, belonging (Rouse et al., 2017) and engagement in purposeful activity via the work-ordered day (Pernice et al., 2021). This structure supports skill development (Rouse et al., 2017) and the formation of an occupational sense of self (Tanaka & Davidson, 2015).
Autonomy and choice were significant motivators for Clubhouse participation, allowing members to individually tailor their experience (Rouse et al., 2017; Tanaka et al., 2021). The model is consistently linked to recovery-oriented practice (Fekete et al., 2021; Hancock et al., 2015; Raeburn et al., 2016, 2017), with a focus on self-determination, community reintegration and equal member–staff partnerships (McKay et al., 2018).
Qualitative research is an important approach in CIM research. Systematic reviews by Battin et al. (2016) and McKay et al. (2018) suggest qualitative research designs are better suited to investigate the flexible and adaptable nature of the model compared with traditional quantitative research designs. Despite the well-established model philosophy, limited research explores unique clubhouse practices (Chen, 2017). There is a need to understand the components of the CIM and how they influence member outcomes (Fekete et al., 2020).
This article describes findings of an ethnographic study conducted at Kindred. The study aimed to inform Kindred’s service development by using ethnographic methods to explore the Kindred Clubhouse programme as it is experienced by its members. The research questions were as follows: What CIM components are adopted and experienced by members of the Kindred Clubhouse? What are the needs of the members at the Kindred Clubhouse? Which aspects of the Kindred Clubhouse programme meet the needs of its members? Which needs of the members are currently not being met?
Method
Study Design
Ethnographic methods, including active participant observations, interviews and document review, were adopted. Ethnography explores socially constructed knowledge (Spradley, 1979) and emphasises researcher immersion (Brewer, 2000). The unstructured and explorative nature of ethnography (Sharkey & Larsen, 2005) aligned with Kindred’s flexible and participatory approach and allowed for the inclusion of members and staff in the study.
Institutional consent was granted by Kindred’s Board. Monash University Human Research Ethics Committee approved the study.
Setting
Kindred’s programme adopts many of the principles outlined by the CIM, servicing adults aged 18 years and above with a history of mental illness. The programme takes place from 10 a.m. to 3 p.m. on Wednesdays through Fridays and from 10 a.m. to 2 p.m. on Saturdays. Funding is obtained from multiple sources, such as government grants and philanthropic contributions.
Participant Recruitment
The first author’s (MKL) initial field entry to establish rapport, understand Kindred’s operations and co-design the study was made through weekly attendance for 3 months. Following ethics approval, data collection was conducted by the first author over a further 4 months. All members and staff were invited to participate voluntarily, and only those who were acutely unwell at the time of the study were excluded. Information about the study was provided on noticeboards, through daily meetings and explanatory written statements. In addition, eight participants were purposively selected for semistructured interviews for their ability to offer rich and contextually grounded insights relevant to the study’s aim. This sampling is consistent with ethnographic methodology, prioritising depth of understanding over breadth, and was sufficient to achieve data saturation in conjunction with the analysis of observation and document data.
Participants
Kindred membership comprised 150 members at the time of research. The average daily attendance was 16 members, as well as three paid staff members, volunteers, allied health students, support workers and community visitors. Member’s attendance patterns varied from daily participation to multiple times or once a week, with some attending on a more ad hoc basis. Most members were aged between 30 and 70 years and travelled from various local regions, with some travelling up to 50 km. Members experienced diverse mental health challenges, including diagnoses of schizophrenia, anxiety, depression, bipolar affective disorder, personality disorder and post-traumatic stress disorder, often with co-morbidity.
Data Collection
Participant Observation
The first author (MKL) actively participated alongside members and staff in Kindred’s daily programme, accumulating 31 hours of observations. Observations were documented through detailed field notes and reflexive journaling following each visit.
Interviews
Five members and three staff participated in semistructured audio-taped interviews with (MKL) using an interview guide informed by the research questions and participant observations. Interviews were conducted at Kindred after obtaining written informed consent from participants. A brief demographic questionnaire was completed at the start of the interviews. The semistructured format allowed flexibility to explore participants’ experiences, perspectives and engagement with the programme. Interviews varied in duration, ranging from 20 and 45 min, and were transcribed verbatim. See Table 1 for demographic characteristics of interview participants.
Interview Participant Demographic Characteristics.
Document Review
The purpose of the document review was to triangulate with findings from interviews and observations, identify recurring themes and gain insight into the formal structures and stated goals of the service. Documents were gathered throughout (MKL’s) visits to Kindred and included internal reports, policy documents, monthly newsletters, member project documents and the website. In addition, government mental health policies and the International Standards for Clubhouse Programmes (ISCP) were reviewed alongside the other data sources. Relevant content from documents was coded and recorded in a table.
Data Analysis
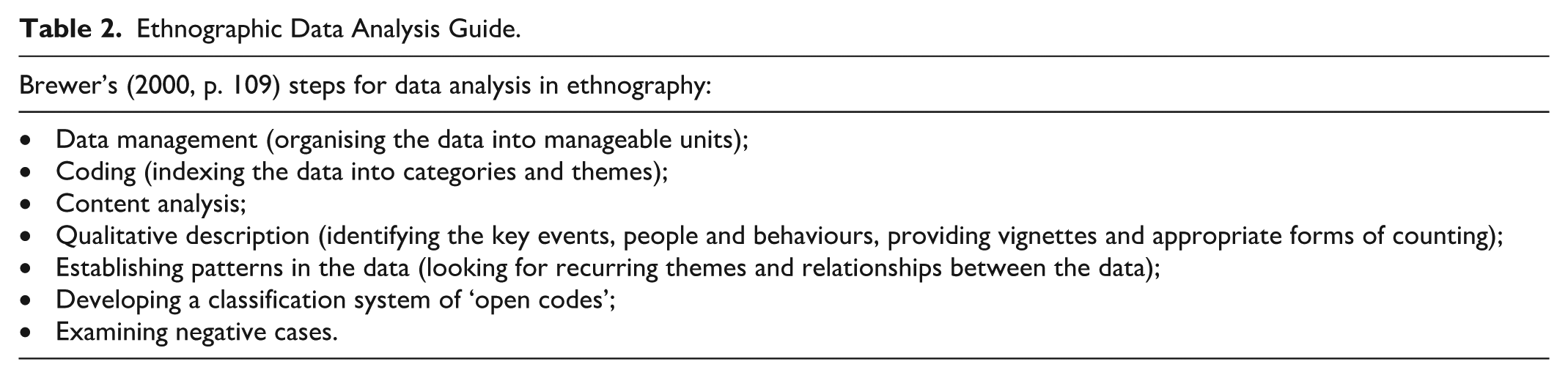
Data analysis followed Brewer (2000) and Sharkey and Larsen (2005) methods in two phases. The first involved ongoing collection, organisation and informal analysis of data during fieldwork, with information from observations and documents being included in interviews (Sharkey & Larsen, 2005). The second phase involved a review and analysis of all data sets, which included information from reflexive journal and field notes, interview transcripts and documents (see Table 2). The first (MKL) and second authors (PL) used an iterative constant comparison approach, analysing the separate data sets independently before comparing them. The findings were then discussed with the third author (KD) before reporting them at Kindred to member check their interpretation and support the accurate application of the data’s meanings.
Ethnographic Data Analysis Guide.
Trustworthiness
Trustworthiness strategies (Lincoln & Guba, 1985) included prolonged engagement to deepen (MKL’s) understanding of the topic, setting and data. Triangulation was achieved using multiple perspectives (members, staff and researchers) and methods (observations, interviews and document review). Member checks through informal discussions, interview summaries and formal reporting of findings ensured accuracy. Peer review meetings with the second and third authors throughout the study promoted methodological rigour, reflexivity and minimised bias.
Results
Exploring the daily activities, experiences and interactions of members, staff and the environment reveals how Kindred uses components of the CIM to offer a supportive community hub for adults with mental health concerns. The synthesised qualitative analysis derived from observations, semistructured interviews and documents generated four themes with 11 subthemes related to the research questions (see Figure 1).
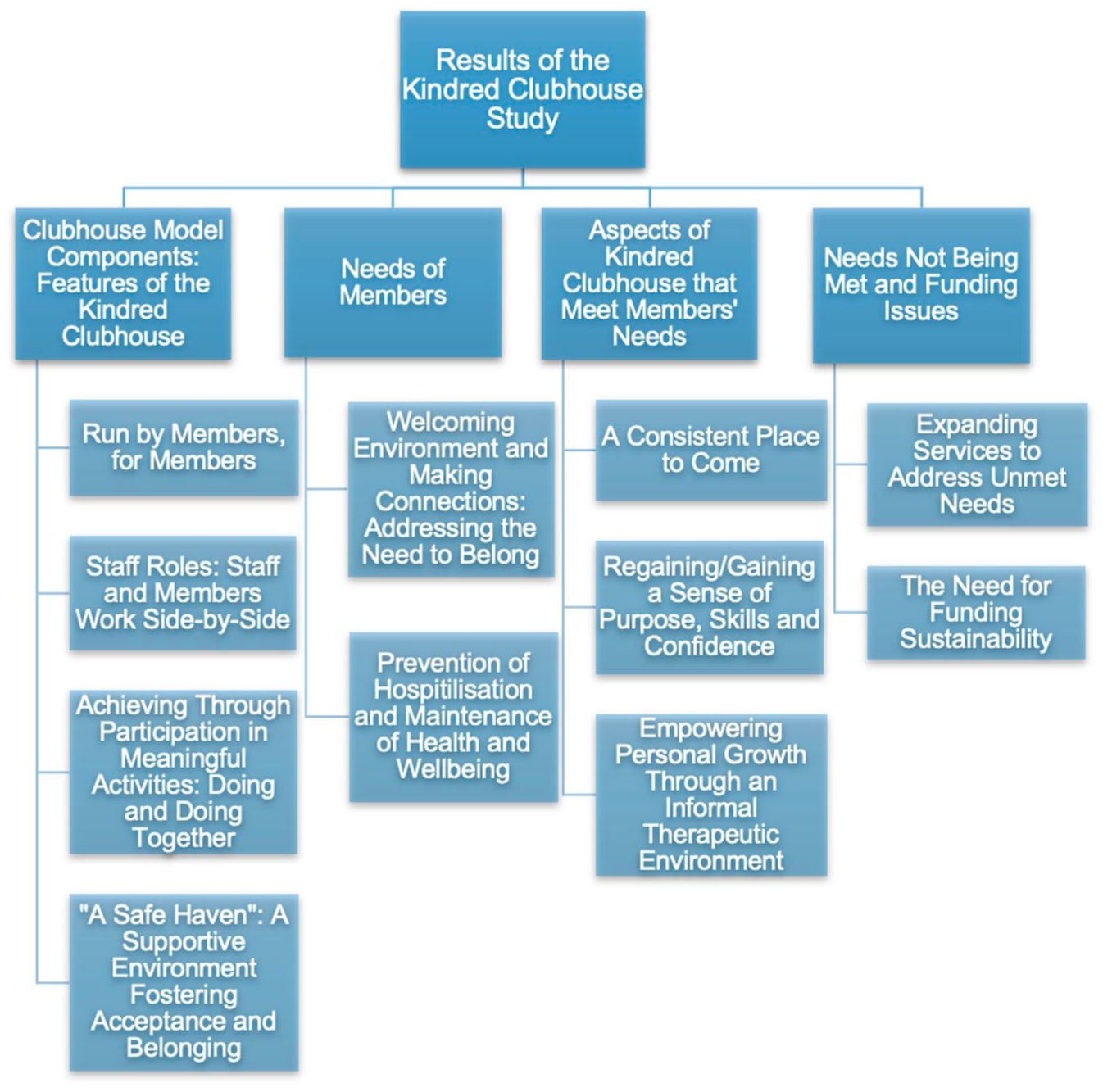
Themes and Subthemes Derived From the Data.
Clubhouse International Model Components: Features of the Kindred Clubhouse
Run by Members, for Members
Kindred’s communication materials consistently featured the phrase ‘Run by members, for members’, reflecting Kindred’s interpretation of the application of the CIM’s collaborative approach. Members were observed to play pivotal roles in shaping Kindred’s community and its various activities. Members were not passive observers but rather active contributors, participating in decisions ranging from lunch menus, daily operations, strategic plans, to being on the Board. ‘We could be making decisions about what’s for lunch or it could be decisions about where the clubhouse is going . . . everything is important – making coffee . . . cleaning . . . vacuuming . . . someone just keeping the general upkeep or doing the cooking. It’s all necessary to keep the clubhouse running’ (James, member).
Members reported experiencing a sense of ownership and pride in Kindred’s success. Members assume responsibility for day-to-day operations for the benefit of others, nurturing a sense of autonomy and self-determination within their community: ‘It’s really empowering, you know, being part of the steering of the clubhouse’ (Michael, member).
Staff Roles: Staff and Members Work Side-by-Side
The principle of staff and members working ‘side-by-side’, as outlined in the ISCP, was consistently enacted at Kindred. Staff adopted roles that extended beyond traditional hierarchies; they were observed to be facilitators, embracing members as equals and championing collective decision-making. This dynamic was also reflected in staff narratives. As Susan (staff) explained, ‘They are always willing to help and be there and support the staff, so it’s not only that we support them, they support us too’, highlighting the reciprocal nature of support within the clubhouse.
Fieldnotes documented the use of strategies such as modelling, where staff demonstrated positive communication, task engagement and problem-solving. Staff were frequently seen participating alongside members or standing by their side while they completed tasks. Amber (staff) illustrated this approach: ‘It’s like watching me make the coffee, or maybe they’re making the coffee and we’re there with them, and we’re there to kind of just help but are not doing it for them’. Furthermore, this ethos of side-by-side practice extended beyond staff, as experienced members were observed modelling and supporting peers during Kindred’s activities.
Achieving Through Participation in Meaningful Activities: Doing and Doing Together
The structured work-ordered day fostered hands-on learning, emphasising active occupational participation in real work tasks. Members consistently expressed a sense of accomplishment derived from witnessing tangible outcomes of their contributions. Activities selected by members ranged from administrative duties, maintenance tasks and preparing meals to providing peer support, each playing a vital role in the overall functioning of the programme.
We work as a team. It’s like that sense of community for me. And you know, the positive possibilities that you can achieve by being part of that team (Linda, member).
The clubhouse environment was observed to provide a safe and supportive setting where members could engage in tasks that might otherwise feel overwhelming or isolating, particularly those related to daily living skills. ‘Things like self-care . . . eating . . . cooking are all really important parts of life and getting better but sometimes can be really hard on your own’ (Daniel, staff). For instance, one member who initially felt unconfident in their cooking skills began by participating in simpler tasks, such as washing dishes and gradually built up contributing to group meal preparation.
Through the collaborative support of both staff and fellow members, individuals were seen to gradually build confidence and overcome challenges in self-care, leisure and productive occupations.
‘A Safe Haven’: A Supportive Environment Fostering Acceptance and Belonging
Kindred was consistently described as a place where members felt accepted and valued, with both members and staff facilitating this environment. One member described Kindred as: A safe-haven, a non-judgemental environment, a place to be accepted, just a place to belong. I don’t know what I’d do without Kindred in my life. Kindred got me off drugs and everything. It gave me a purpose in my life and gave me somewhere to come and be part of something and get to know other people (Kerry, member).
The role of peer support was central to this environment and foundational in creating a welcoming and nonjudgmental atmosphere. This enabled members to share both their challenges and successes openly, fostering mutual understanding and collective resilience.
Kindred was found to have a well-established outreach programme that was consistent with the outreach principles outlined in the ISCP. Both staff and members proactively engaged members who were less active or less visible, reinforcing the programme’s ongoing commitment to their support and well-being.
Needs of Members
Welcoming Environment and Making Connections: Addressing the Need to Belong
Entering Kindred Clubhouse was reported to be a daunting experience for some, often involving multiple visits before feeling ready to fully engage: I sat over the road at the barbecue hut for two months, I think, before I walked through the door . . . and I’m so glad I did, it is one of the best choices I’ve ever made . . . as soon as I walked through the door it was like I walked into my own home (Linda, member).
Within the clubhouse, members described forming meaningful connections that resembled an ‘extended family’. This sense of belonging was particularly significant for those who had experienced social isolation, highlighting the clubhouse as a vital place for relational support and sense of community.
Prevention of Hospitalisation and Maintenance of Health and Well-being
Kerry (member) described attending Kindred as a form of ‘maintenance’, emphasising the programme’s role in providing ongoing support that reflects the long-term nature of maintaining mental health. This perspective was also reflected by staff: ‘I think with maintenance, for example, you are in the hospital and then you’re discharged, so what are you doing after that? I think this is a place where people can maintain their mental health’ (Amber, staff).
Observations within the clubhouse revealed that this ongoing support is embedded in the daily routines and interactions of the clubhouse, where members engage in activities and social connections at their own pace, free from the pressures of time-limited treatment models. ‘It’s so important if I didn’t have this, I would’ve been, I don’t know how many times back in the hospital without a doubt’ (Michael, member). In contrast to traditional mental health service interventions that frequently impose timelines, members consistently emphasised the importance of Kindred’s continuous availability, reflecting an ISCP principle.
Aspects of Kindred Clubhouse That Meet Members’ Needs
A Consistent Place to Come
Members and staff identified the reliability of the Kindred programme as fundamental in providing stability, predictability and a consistent environment for members. Although Kindred was not open every single day, there was a clear organisational commitment to maintaining accessibility as consistently as possible. This ongoing effort was perceived as critical in ensuring members could depend on the programme as a stable resource. As one member, James, explained, In the last 12 months, they have tended not to close the clubhouse with the outings or different courses or activities . . . for people that might drop in so it’s here for them. I think it’s good because it gives the opportunity for people that may have lapsed to come. And if the clubhouse is closed when it should be opened it’d be quite disappointing for someone (James, member).
In recognising that mental health concerns do not adhere to a specific timetable, the knowledge of having a reliable sanctuary available held immense importance to members, even when they might choose not to access it.
Regaining/Gaining a Sense of Purpose, Skills and Confidence
A recurring theme across data sets was the role of Kindred in fostering a sense of purpose and supporting the re-development of vocational and daily life skills. When asked about why people attend, Rob (member) shared, ‘for me, it is the purpose and getting out of the house. . . I find purpose here, and purpose gives people hope’. This sense of purpose was reflected in observed daily routines and structured tasks, where members consistently engaged in activities requiring punctuality, time management and collaboration, skills foundational to vocational readiness.
Regaining prevocational skills such as punctuality, time management, teamwork and active participation are vital components of the rehabilitation process, that Kindred was observed to embrace. Participation and skill development assisted in rebuilding confidence and preparing for employment or educational opportunities, which can seem unattainable amid challenges posed by poor mental health: ‘Being a member of Kindred, I’ve now been back in the workforce for a year . . . and that was just learning to get some self-confidence and everything back again, and trust’ (Kerry, member).
In addition to informal skill-building, several members had completed vocational certificates, with two members successfully transitioning into paid employment during the study period.
Empowering Personal Growth Through an Informal Therapeutic Environment
Kindred was observed to foster a nurturing environment characterised by informal therapeutic relationships and shared engagement in meaningful activities. These collective experiences appeared to support the development of confidence, self-love, self-empowerment, compassion, empathy and adaptive coping among members. Compared with traditional therapy, participants described feeling more comfortable discussing personal matters within the Clubhouse. For example, Linda (member) reflected earlier that day that she ‘was feeling overwhelmed. And was thinking oh no, I am not going to get through this. And the more I sort of got into doing a project and chatting with others, it just lifted me out of it’.
Needs Not Being Met and Funding Issues
Expanding Services to Address Unmet Needs
The most significant unmet need identified by members pertained to the operating hours of Kindred. This topic regularly emerged in conversations observed between members, as well as between members and staff or stakeholders. Members consistently expressed their desire for extended service hours during weekdays, weekends and holidays: There are people that might need that connection every day, whether it’s just coming in for five minutes or ten minutes it’s a connection, it’s I’ve got somewhere to go, I’ve got meaning . . . We need to be open for seven days . . . On the weekend, my mental health doesn’t take a break or the day off (Michael, member).
The current programme schedule presented limitations for those who worked part-time, attended appointments or were engaged in other activities on the days Kindred operated. The conversations suggested that the existing schedule may not fully meet the social and occupational needs of all members. It is worth noting that the ISCP stipulate a minimum of 5 operating days per week, along with the provision of social events and celebration of holidays on their designated dates. Currently, Kindred is only open from Wednesday to Saturday.
Participants identified a need for a broader range of activities to reflect diverse interests and preferences, gaps in employment and housing support were identified in interviews, observations and document analysis.
Kindred operates as one working unit, which limits the variety of tasks and activities available to members. A notable gap observed relates to the absence of employment support, specifically the lack of Transitional and Supported Employment programmes. Although this issue was not explicitly raised by members during interviews, it was evident through staff perspectives, observations and analysis of documents. This gap is particularly significant given that employment support is a core component of the CIM, as outlined in the ISCP.
The Need for Funding Sustainability
Lack of regular ongoing funding was found to have significant implications for the security and continued sustainability of Kindred’s operations. Observations and interviews revealed members’ confidence in ongoing service availability, development and sustainability of the organisation was directly tied to financial security. Participants emphasised the importance of these aspects in their interviews, stating without Kindred, many people would be left without support.
Discussion
Findings from this study provide evidence of the effectiveness of the components of the CIM adopted by Kindred Clubhouse in Australia in facilitating the ongoing recovery journey of people with mental illness living in the community. Kindred met members’ needs by providing a dependable, safe, supportive and inclusive environment, facilitating meaningful connections with others through the cooperative participation in occupations within the clubhouse community. Participation in the clubhouse promoted a sense of belonging, the restoration of purpose and hope and the maintenance of health and well-being in members. Both members and staff had a positive perception of the Kindred programme. This was evident across all three data sets. However, members and staff expressed the need for (a) expanded operating hours to enhance accessibility, (b) sufficient meaningful diverse working units and activities available to sustain a full and engaging work-ordered day, and (c) secure funding for Kindred’s development, and long-term sustainability. The need for further development in areas of employment and housing is required to ensure Kindred aligns with the CIM’s mission.
A significant finding was members’ need for ongoing maintenance of health and well-being to support recovery and prevent hospitalisation. Kindred offers an environment that effectively facilitates this enduring need. This is congruent with Kinn et al. (2018), where members viewed a clubhouse as a place to ‘establish an anchor’ underscoring the important role nonclinical community-based programmes play in supporting individuals with mental illness to maintain their well-being. This reflects recovery as a lifelong process (Fekete et al., 2021).
The sustained support offered by Kindred has been identified as a crucial feature contributing to the reduction in hospitalisations and alleviating pressures on the healthcare system. Participants in this study reported a decrease in hospital admissions, a finding consistent with other research on clubhouses (Battin et al., 2016; Bouvet et al., 2021; Fjeldsoe et al., 2025; McKay et al., 2018; Russell et al., 2021) linking membership to lower hospitalisation rates.
Our research findings echo Coniglio et al. (2012), emphasising the pivotal role of service users (members with mental health concerns) in aiding their peers’ recovery within the CIM through peer support. Similarly, it highlights the significant contributions made by members who share their personal experiences, provide their ‘expert’ knowledge and extend care and empathy towards one another, reinforcing the significance of peer support within this context. Our findings build upon this, showcasing a shift from members being self-focused to taking a broader clubhouse community perspective. Although clubhouses do not label themselves as occupational therapy programmes their focus on a ‘work-ordered day’ and members’ active participation in the daily occupations required to deliver the programme, aligns well with the fundamental theories of occupational therapy. Occupational therapists have long explored doing, being, becoming and belonging as fundamental concepts of health and well-being (Hitch et al., 2014). The importance of an affirming place to belong has been shown to provide opportunities to improve occupational performance (Rebeiro, 2001) and develop a sense of community. Furthermore, for people with mental health challenges, a place to belong can contribute to mental health recovery by offering a sense of membership (Doroud et al., 2018; Rebeiro Gruhl et al., 2021).
It is recognised that there is a lack of services, and funding for services, tailored to support the recovery of people living with mental health concerns within the community (Lawn et al., 2021; Petrie et al., 2021), often referred to as the ‘missing middle’. The ‘missing middle’, as defined by health professionals in the work by Petrie et al. (2021), refers to individuals who are moderately unwell and struggling with their mental health but do not meet the criteria for crisis services. One approach to improve support for people living in the community that has been implemented throughout Australia is the introduction of peer support roles (Lawn et al., 2021). Peer support provided by members plays a central role within Kindred. Our findings revealed that members actively participated in peer support daily, fostering an inclusive environment where they mutually support one another through shared lived experiences. Research by Smit et al. (2023) and White et al. (2020) reported the importance of peer support in reducing stigma, enhancing social connections, promoting personal recovery and empowering individuals.
The concept of social connectedness and a sense of belonging is widely recognised as a fundamental human need (Haim-Litevsky et al., 2023; Lim et al., 2021; O’Rourke et al., 2018). Our findings concur with previous literature, exploring this within clubhouses (Desai et al., 2021; Fekete et al., 2020; Fjeldsoe et al., 2025; Tanaka et al., 2018). Haim-Litevsky et al. (2023) provide further empirical support for the intricate link between meaningful engagement, belonging and well-being. Our study’s findings, where members actively engaged in meaningful activities while experiencing a strong sense of belonging and connectedness to a supportive community, align with the idea that nurturing a sense of belonging and connectedness can significantly contribute to an individual’s well-being. This supports the CIM’s focus on promoting mental health recovery and social inclusion through participation (Desai et al., 2021; Tanaka et al., 2018).
The question arises as to whether the positive benefits within the clubhouse of having a place to belong, where one can participate in occupations within a supportive community and recover as shown in our study, extend beyond the clubhouse boundaries to the wider community. Desai et al. (2021) identified this issue, portraying the clubhouse as an ‘oasis’ within the ‘desert’ that remains outside. Kinn et al. (2018) emphasised the clubhouse’s role as a ‘stepping stone’ for members to build skills and confidence before venturing outside. However, Gumber and Stein (2018) stressed the need for enhanced community integration beyond the clubhouse, echoing concerns raised by Raeburn et al. (2013) about the risk of service dependence and membership without time limits.
Clinical Implications
There is a need for nonclinical community programmes to (a) facilitate the recovery process; (b) maintain the mental and physical health, well-being and wellness of people with mental illness living within the community; and (c) help them develop skills to connect and participate in the larger community in which they live (State of Victoria, 2021). Within the Australian mental health context, Kindred serves as a bridge, catering to the ‘missing middle’ population, filling the service gap for those who are too unwell to stay at home but not unwell enough to go to hospital. Kindred offered a daily destination and a hub for developing the skills for maintaining mental health and well-being necessary for participating in the community. The first clubhouse, established by individuals with lived experience, aimed to address a systemic gap in the United States (Anderson, 1998). Similarly, clubhouses have the potential to fill the existing ‘missing middle’ service gap in Australia.
Limitations and Future Research
The study participants held positive attitudes towards Kindred, corresponding with other research, which also reflected similar positive opinions (Fekete et al., 2020; Ritter et al., 2019; Roth, 2017). It is important to acknowledge that the participants in these studies, including this one, were active clubhouse members. The inclusion of predominantly active members in data gathering may limit generalisation of the findings to wider populations of individuals living with mental illness in the community. Future research should aim to include individuals who are less actively engaged with the Clubhouse and at different stages in their recovery to capture a broader range of experiences.
This study focused on a single Clubhouse, and while it offers valuable insights, variations in structure and governances across accredited Clubhouses may limit the generalisation of the findings in these settings. However, the identified needs, such as belonging, social connection, a sense of purpose and meaningful activity engagement, are likely to be relevant to broader populations of individuals living in the community with mental health challenges.
Globally, the CIM continues to grow, yet it is relatively new in the context of Victoria, Australia. This study provided Kindred’s programme, which has not been the subject of prior research, and relevant stakeholders with an external perspective to better understand its strengths, identify areas for growth and inform future service development.
Conclusion
The components of the CIM adopted by Kindred make it a key community service for individuals facing mental health challenges. Kindred’s informal community-based therapeutic setting that fosters recovery through meaningful occupational and social participation offers a member-led approach that can be individually tailored to the needs of people with mental health challenges living in the community. Findings revealed the significance of having a physical, safe and supportive space for individuals to gather, fostering a sense of belonging and purpose that is instrumental in maintaining their mental health and well-being. This research emphasises the pivotal role-played by nonclinical programmes in addressing the diverse needs of individuals with mental illness in the community.
Footnotes
Acknowledgements
The authors would like to thank the staff, members and Board of Directors of Kindred Clubhouse for their collaboration and participation in this research.
Ethical Considerations
Ethics approval was obtained from Monash University HREC on 20/1/23 ID: 36009.
Consent to Participate
Verbal and written informed consent procedures were followed. All participants were informed of the study’s risks and benefits, and that their participation was voluntary before their consent was obtained.
Consent for Publication
All participants were informed that the research would be published and that their identity would not be disclosed. Pseudonyms are used for all participants throughout the article.
Author Contributions
All authors certify their responsibility for the article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: The authors declare that they have no conflict of interest. Karen Dixon’s potential conflict due to joint affiliations with Monash University and with Kindred Clubhouse was managed by Monique Lee and Primrose Lentin conducting the research data collection and analysis.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author subject to appropriate ethical and legal considerations.