
Abstract
Novice occupational therapists struggle with clinical reasoning when interpreting cognitive assessments and planning interventions for patients with an acquired brain injury (ABI), impacting patient rehabilitation outcomes. This study aimed to establish expert consensus on a self-directed learning package (SDLP) for novice occupational therapists to support clinical reasoning when planning cognitive rehabilitation. A mixed-methods design consisting of an initial survey, then three virtual Nominal Group Technique focus groups, including 21 expert occupational therapists, prioritized SDLP content and teaching methods. Experts identified: “neuroanatomy,” “evidence-based practice guidelines”, “interpretation of functional errors,” “delivery of cognitive rehabilitation,” “goal setting,” and “progress measurement” as the most important content. They prioritized video demonstrations, case studies, online modules, and practical assignments as methods to deliver the SDLP. The virtual focus groups enabled rapid consensus of the content and teaching methods for an SDLP which can now be developed to support novices’ clinical reasoning when planning cognitive rehabilitation.
Plain Language Summary
This study wanted to find out what support new occupational therapists need when learning to plan rehabilitation for patients with acquired brain injuries (that is, people who have an injury to their head) so we can make a new learning package for these occupational therapists. Previous studies found that some occupational therapists find it hard to plan rehabilitation, which might mean patients do not reach their goals. The study involved 21 expert occupational therapists who answered a survey and then talked together via video conference. The experts agreed that the learning package should include information on how rehabilitation can improve thinking skills and goal setting. They also agreed that new occupational therapists should be taught using videos, case studies, and practical homework. Using the video conference, the experts decided on the information to include and the types of teaching methods to use in the new learning package.
Introduction
Cognition describes the brain’s complex information processes completed consciously or unconsciously (American Occupational Therapy Association [AOTA], 2019). Cognition is essential for everyday occupations such as self-care, domestic activities, work, play, and leisure (Champagne et al., 2019). After an acquired brain injury (ABI), that is, a stroke or brain injury, cognitive impairment is a common occurrence, negatively impacting functional performance (Stolwyk et al., 2021; Stroke Foundation, 2019). Cognitive rehabilitation involves education to facilitate self-awareness of cognitive deficits and strategy training to re-learn activities or learn new ways of completing tasks (van Schouwen-van Kranen, 2014). Occupational therapists play a key role in cognitive rehabilitation by enabling patients with an ABI to learn to manage their cognitive impairments and participate in valued occupations (Giles et al., 2020). Failure to provide appropriate and accurate assessment and treatment of functional cognition may result in poorer patient outcomes postdischarge from the hospital (Giles et al., 2020).
Internationally, evidence-based practice (EBP) guidelines for ABI provide general recommendations for cognitive rehabilitation but lack information on how to transfer these recommendations into practice (Jeffay et al., 2023; Stroke Foundation, 2019). Moreover, occupational therapists face challenges in planning cognitive rehabilitation, such as difficulty interpreting assessment findings (Goodchild et al., 2023). In addition, occupational therapists struggle with pragmatic reasoning and prioritizing areas of cognition to address (Nott et al., 2020) and reasoning to implement evidence into practice (Holmqvist et al., 2012). Occupational therapists report low confidence in planning cognitive rehabilitation, due to the complexity of clinical reasoning required (Wheatcroft et al., 2024).
Planning cognitive rehabilitation is a complex process that involves multiple modes of clinical reasoning (Holmqvist et al., 2009). Clinical reasoning, also known as professional reasoning, encompasses the thinking processes that guide clinical practice (Unsworth, 2004). This process is dynamic, complex, and multifaceted, developing not solely from years of experience but also through reflective practice and experiential learning (Sánchez-Zamorano et al., 2025). Clinical reasoning is fundamental to our professional ability to manage the complex process of integrating assessment, therapy planning, and intervention (Márquez-Álvarez et al., 2019). It may be influenced by an individual’s worldview, political and health care environment and resources available (Sánchez-Zamorano et al., 2025; Unsworth, 2025). In one of the foundation studies of clinical reasoning in occupational therapy, Mattingly and Fleming (1994) described how experts could simultaneously keep track of their reasoning around the very different aspects of patient issues, which they called the “three-track” mind. Thinking with a “three-track mind” is particularly evident among clinicians working in complex practice areas such as cognitive rehabilitation, where occupational therapists integrate research evidence with assessment findings while considering the patient’s context (Nott et al., 2020). This approach to explicating clinical reasoning draws on Ryle’s (1946) philosophy of “knowing that” and “knowing how.” The practical “knowing how” to plan cognitive rehabilitation and the “ways and methods of doing things” depends on the “ knowing that” of the underlying cognitive impairments and the evidence-base for practice around these impairments to apply this theory in practice (Ryle, 1946). Novice occupational therapists may find the “knowing how” to plan cognitive rehabilitation difficult due to the complex interplay between the person and their cognitive impairments, environment, and occupation factors. Thus, clinical reasoning is key to enhancing novice occupational therapists’ work with patients who require cognitive rehabilitation following ABI (Unsworth, 2017), and methods to facilitate expert clinical reasoning are required.
Clinical reasoning develops through experience, training, reflection, self-monitoring, and practice with mentorship (King et al., 2007); however, the majority of the research conducted in this area has been in nursing rather than occupational therapy (Pérez-Perdomo & Zabalegui, 2023). An occupational therapist’s cognitive skills are crucial for connecting and interpreting information to create “scripts” or “frames” (Carr & Shotwell, 2018) to develop therapy. These frames are mentally gathered, stored in long-term memory, and used by occupational therapists with a range of patients (Benner & Tanner, 1987). Building clinical reasoning capability in novice clinicians in the area of cognitive rehabilitation can be facilitated through mentorship, group education or self-directed learning (SDL; Paterson et al., 2002). Evidence on effective educational methods for improving clinical reasoning in occupational therapy is limited, especially for graduate clinicians (Unsworth & Baker, 2016). Burke and colleagues (2024) developed educator consensus on teaching reasoning, reflective practice, and evidence-based strategies for student occupational therapists. Case studies, simulations, and problem-based learning were essential strategies for advancing students’ clinical reasoning development (Burke et al., 2024). However, this work has not been replicated in qualified occupational therapists. Case-based learning shows positive effects in clinical practice, noting that mentorship and reflection are important (Maruyama et al., 2024).
SDL supports health professionals in enhancing their performance and clinical reasoning (Mamary & Charles, 2003). This cost-effective approach leverages self-assessment to enhance knowledge and reasoning skills (Paterson et al., 2002). SDL may include case studies, which can be presented in video format, for clinicians to engage with Neistadt (1998; Rodríguez-Bailón et al., 2021; Schettino & Capone, 2022). Once developed, case-based education/learning packages must be evaluated for effectiveness. A recent study by Behrendt and Smallfield (2024) describes the development of an e-learning module for functional cognition for occupational therapy students, but the training’s effectiveness is unclear. Similarly, SDL education courses on cognitive rehabilitation exist, such as the American Congress of Rehabilitation Medicine (ACRM; https://cognitiverehabilitation.org/), Braintree (https://www.braintreetraining.co.uk/), and Multicontext (https://multicontext.net/workshops), but their effectiveness remains unknown.
Powell et al. (2020) surveyed paraprofessionals working with brain injury patients to identify their training needs, finding cognition to be a top priority. Consequently, an online training program was provided to 79 paraprofessionals, most with less than 5 years of experience. The online program showed promising results; however, the study lacked objective measures of clinician improvement (Powell et al., 2021).
When considering the development of SDL education for novices, it is essential to consider the characteristics of this group. Dreyfus and Dreyfus (1980) developed a theory of the development of skills such as clinical reasoning, which poses five key stages: novice, advanced beginner, competent, proficient, and finally, expert. This work was translated into nursing by Benner and Tanner (1987) and subsequently across allied health (King et al., 2007; Unsworth, 2021). Novice therapists may have basic knowledge of cognitive theories, practices, and patient characteristics but may be unable to apply this knowledge (Benner, 1982). As a result, they require expert supervision to identify and develop rehabilitation plans (Jeffery et al., 2020), such as those addressing cognitive impairments. Novice occupational therapists in hospitals must develop clinical reasoning skills for effective inpatient cognitive rehabilitation. Neglecting this will ultimately impact patient recovery. Therefore, drawing insights from expert occupational therapists in cognitive rehabilitation to guide novice therapists is essential for shaping SDL education content. Through years of experience with novice therapists, expert occupational therapists can guide the delivery of SDL to support clinical reasoning in busy hospital environments. Definitions of expertise are complex (Dewitt et al., 2021) and have not been well developed in occupational therapy. An emerging perspective of this concept is adaptive expertise (Benfield, 2025). This perspective views adaptive experts as those who progress beyond routine expertise by engaging in reflection and critical analysis to expand their knowledge and become innovative practitioners (Gube & Lajoie, 2020). Further research is required to explore this perspective and identify the hallmarks of adaptive expertise within occupational therapy practice. However, occupational therapy experts in cognition are often defined as those employed in a specialist setting working with people with cognitive impairment, seeking opportunities for experiences that enhance their understanding of EBP and self-improvement, and acting as mentors to others in this specialized area (Halle et al., 2018; King et al., 2008; Nott et al., 2020; Rassafiani, 2009; Thomas et al., 2023).
This study aimed to establish expert consensus on the content and teaching methods of a self-directed learning package (SDLP) targeted at novice occupational therapists working with people with ABI within the hospital setting. This work focuses on the content and methods that assist novice inpatient occupational therapists in developing their clinical reasoning rather than researching the reasoning process themselves. Specifically, expert consensus was sought regarding the following: (a) What core content should be included in an SDLP to support novice inpatient clinicians in developing their clinical reasoning when planning cognitive rehabilitation for patients with an ABI? and (b) what methods or teaching tools should be considered within the SDLP to support the development of clinical reasoning in relation to cognitive rehabilitation?
Method
Study Design
The project used a mixed-methods research design with pragmatic epistemology (Creswell, 2018). Methods included an initial survey followed by focus groups using a virtual Nominal Group Technique (vNGT) format to facilitate the involvement of a wide geographical range of occupational therapy experts in cognitive rehabilitation (Mason et al., 2021). The NGT is a highly flexible technique that generates and prioritizes ideas to facilitate group consensus on a topic (McMillan et al., 2014; Thier & Mason, 2019). This study followed Potter et al.’s (2004) adaptation of the original NGT protocol, which includes five stages: (1) introduction, (2) silent idea generation, (3) round robin, (4) clarification, and (5) scoring (Potter et al., 2004; see Figure 1). This procedure was adapted for an online or virtual nominal group technique (vNGT), thus facilitating participation from experts across Australia (Mason et al., 2021). The NGT was selected over other consensus methods, like the Delphi method, due to greater flexibility in scoring and rapid capacity to gain consensus (McMillan et al., 2014; Thier & Mason, 2019). While the literature presents various descriptions of the ranking or scoring process in the NGT, it is commonly performed individually through Likert-type ratings that are subsequently ranked and then aggregated (Thier & Mason, 2019). Federation University Human Research Ethics Committee (2022/055) approved this study, and all participants provided informed consent before participating.
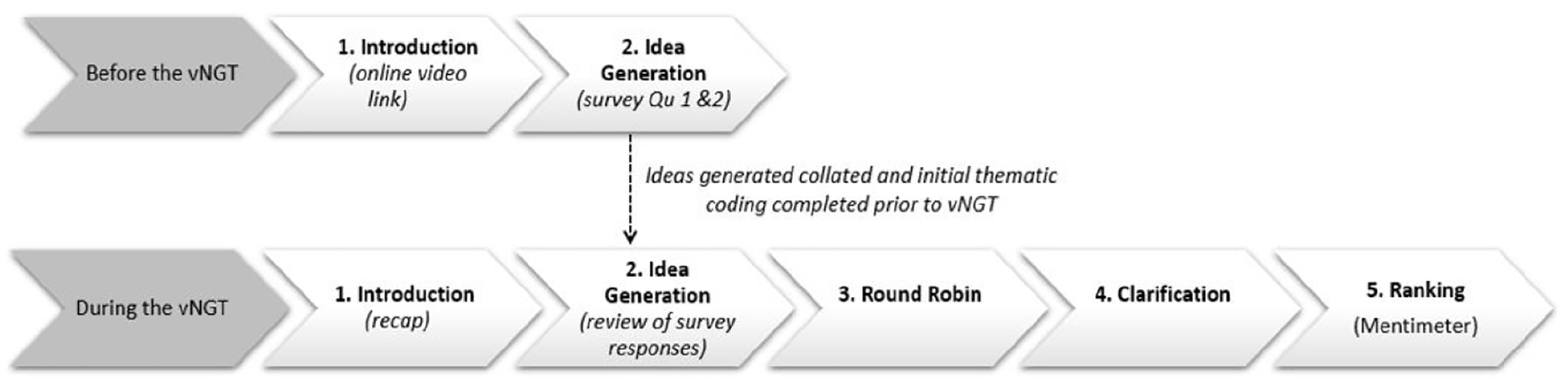
Adapted Nominal Group Technique (NGT) Process (Potter et al., 2004)
Participants
Snowball recruitment with Australian occupational therapists was completed over 8 weeks through social media, that is, X, Facebook, the Occupational Therapy Listserv, and the Occupational Therapy Australia (OTA) research webpage. Experts in cognitive rehabilitation were also purposefully recruited via email through the researchers’ established clinical and academic networks. Therapists received a AU$20 voucher, a participation certificate, and a learning package overview upon completion.
Participants self-identified as experts if they currently work or have worked in a hospital setting with people with ABI cognitive impairment; have a high level of specialist knowledge, skills, and ability in cognitive assessment and rehabilitation; have completed relevant courses in neurological rehabilitation; and act as a mentor in cognition.
Instruments
1. Survey—Before the vNGT focus group, an online survey was sent via Qualtrics to collect consent, demographic information, and initial content ideas for an SDLP and its delivery methods. The two key questions asked were:
Q1. What core content should be included in a learning package to support novice clinicians in developing their clinical reasoning in relation to planning cognitive rehabilitation for inpatients with an ABI?
Q2. What methods or teaching tools should be considered within the learning package to support the development of clinical reasoning in relation to cognitive rehabilitation?
2. vNGT Focus group Guide—The three focus groups were conducted by asking participants to respond to the two research questions.
3. Mentimeter—Ideas from the vNGT focus groups in response to the two questions were entered into Mentimeter (www.menti.com), and participants rated them on a Likert-type scale (1 = very unimportant, 2 = unimportant, 3 = neutral, 4 = important, 5 = very important).
Procedure
The five stages of the vNGT process were amended by completing Stages 1 (introduction) and 2 (silent idea generation) via online survey before the group to enable rapid assimilation of information (Figure 1). The three vNGT focus groups took place online via Microsoft Teams over 2 weeks. Additional ideas were added (NGT Stage 2), followed by the round robin (NGT Stage 3) and clarification stage (NGT Stage 4; see Figure 1; Potter et al., 2004). When no further ideas arose and all were discussed, consensus was reached. Participants took a short break while researchers entered key ideas into Mentimeter. Then, participants ranked (NGT Stage 5) using the Mentimeter software on their personal devices.
Data Analysis
Three stages of data analysis were completed to identify the core content and methods to include in an SDLP.
First, before the vNGT, the survey data on the two research questions were downloaded, and initial thematic analysis of Steps 1 and 2 (Potter et al., 2004) was conducted adhering to Braun and Clark’s (2022) six-stage analysis process. This enabled preliminary analysis of the core content and methods to base the vNGT focus group discussion.
The survey’s core content themes were presented to the participants, with each vNGT building further on the combined themes. After completing the vNGT focus groups, thematic data from Question 1 (What is the core content) and content analysis of Question 2 (What are the teaching methods) data were further analyzed across the three groups. Thematic data analysis was completed initially by the primary author (J.W.), and subsequently, 10% of the data were coded by two other researchers (A.M.B. and C.A.U.) for consistency (O’Connor & Joffe, 2020). Content analysis was used for Question 2 because the data’s homogeneity necessitated pattern analysis over thematic exploration (Braun & Clarke, 2022). Discrepancies were discussed until a consensus was reached. Simple tabulations quantified mean ranks of idea importance.
Third, the Mentimeter software calculated weighted averages for each content and teaching method. Experts’ item mean scores (with SDs) were tabulated and ranked by importance. Demographic data from Qualtrics were summarized and presented descriptively.
The survey themes from the focus groups (FGs) were analyzed and tabulated (see Table 2). As three FGs were conducted, participants in each had to rank all items because simple ratings could not be aggregated across groups. The additional ideas/themes identified by participants during the vNGT focus groups were combined into Table 2—and can be identified by an asterisk (*). Finally, the themes were associated with Ryle’s (1946) structure for Ways of Knowing: knowing what, knowing how, and doing (see Figure 2).
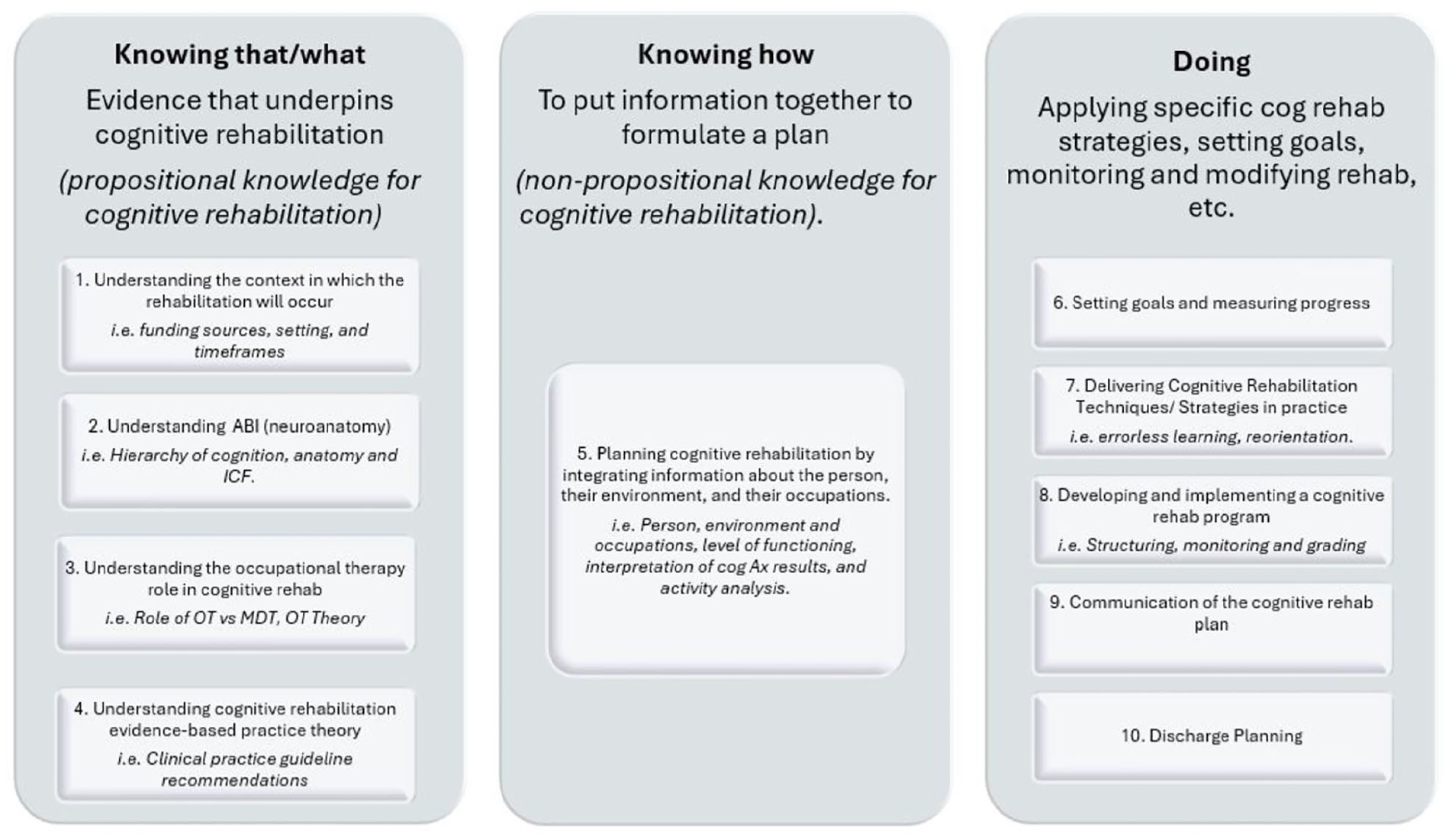
Thematic Representation of the Content of a Learning Package on Cognitive Rehabilitation, Drawing on Ryle’s (1946) Classification
Results
Participant Characteristics
Twenty-three occupational therapists completed the survey, with 22 consenting to participate in one of three vNGTs (see Table 1). Two groups had seven participants, and one group had eight—all ideal numbers for vNGT (McMillan et al., 2016). One participant withdrew due to personal reasons, leaving three groups of seven. Each group lasted 90 min.
Demographic Details of the Expert Occupational Therapy Participants (n = 23).
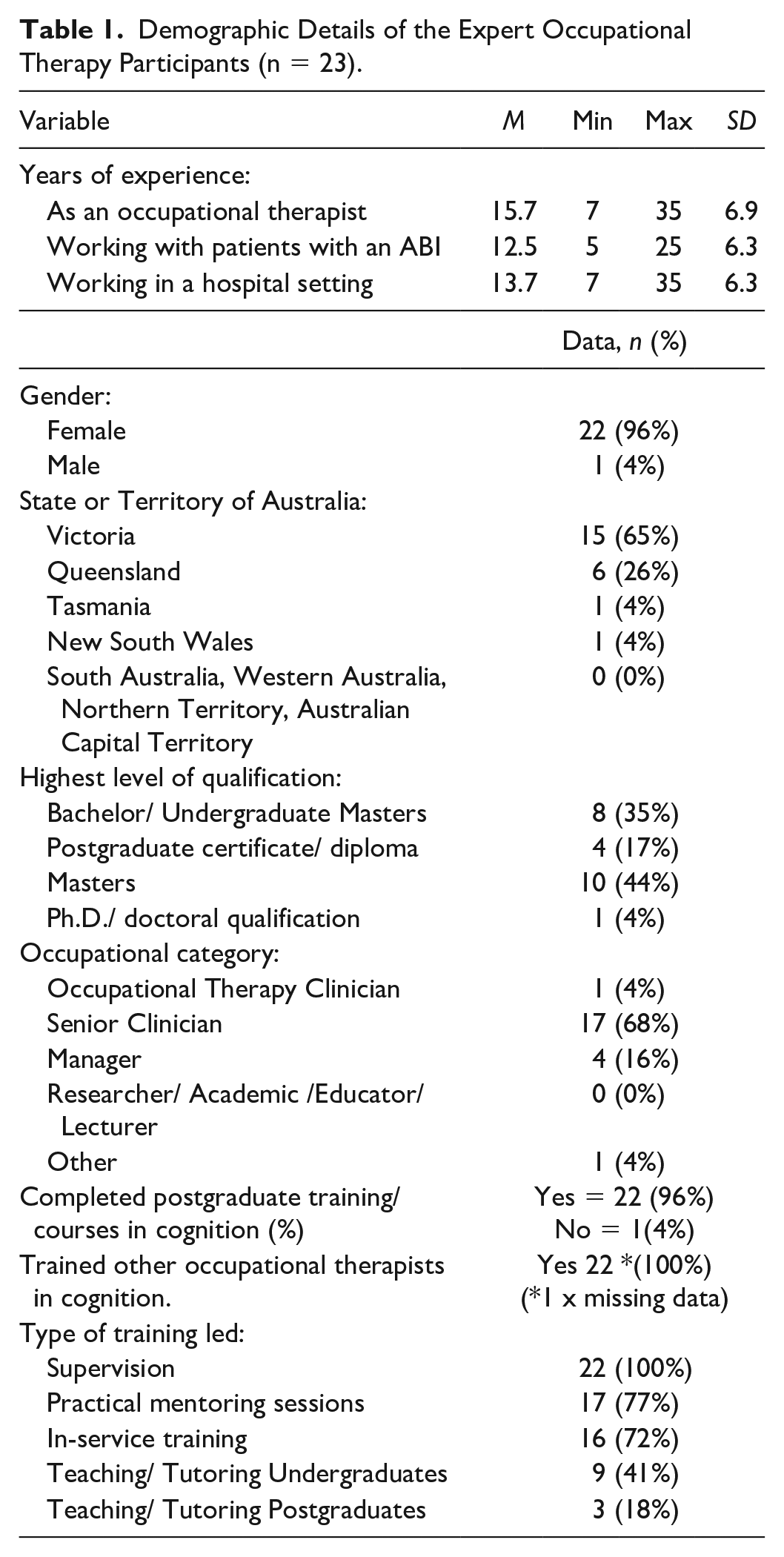
Most participants were classified as senior clinicians (68%) and self-identified as highly experienced occupational therapists, having worked with ABI patients for an average of 12.5 years (SD = 3.6; see Table 1). Nearly all participants (96%) had completed postqualification cognitive rehabilitation training, such as Braintree or ACRM training. In addition, over half of the participants (65%) had completed or were engaged in postgraduate studies. All participants had trained or supervised occupational therapists in cognitive rehabilitation (100%). They were experienced in providing practical mentoring sessions (77%) and in-service training (72%). Nearly half had experience using educational methods alongside their clinical expertise, with 41% having taught undergraduate and 18% having delivered postgraduate occupational therapy training (Table 1).
Content of the Learning Package
Ten themes related to the learning package’s content were highlighted and mapped to Ryle’s (1946) Ways of Knowing (see Figure 2 and Table 2). The most frequently reported themes were (a) understanding cognitive rehabilitation and EBP theory, (b) delivering cognitive rehabilitation strategies, (c) goal setting, and (d) functional neuroanatomy of cognition.
Expert-Identified Content for a Cognitive Rehabilitation Learning Package for Novice Occupational Therapists.
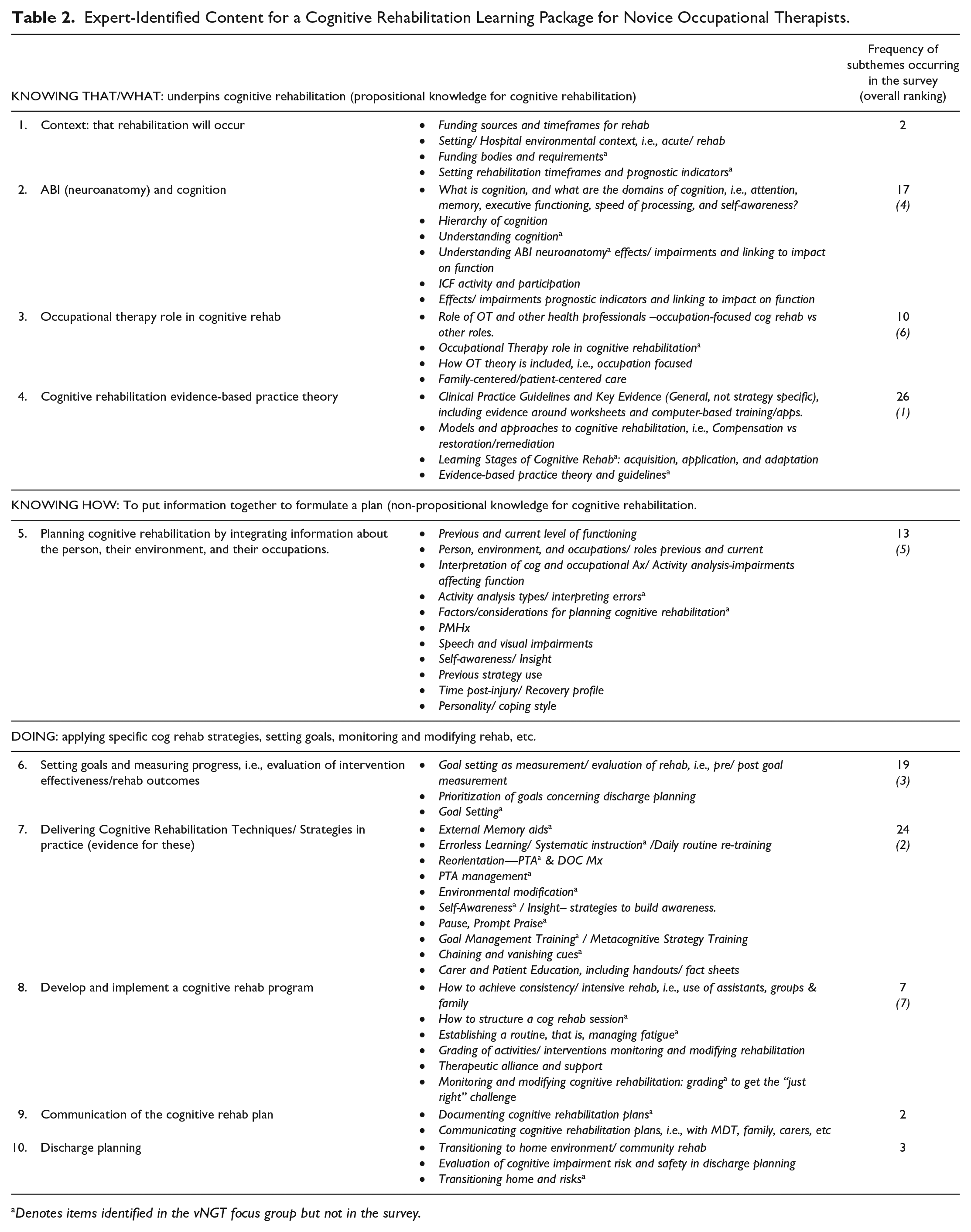
Denotes items identified in the vNGT focus group but not in the survey.
The Mentimeter ratings indicated that experts’ top five rated areas were (a) activity analysis and interpreting errors, (b) monitoring and modifying cognitive rehabilitation, (c) evidence-based theory and guidelines, (d) understanding cognition and its domains, and (e) goal setting (see Table 3).
Importance of Content and Methods for Inclusion in a Self-Directed Learning Package, Weighted Average Ranking From Most to Least Important.
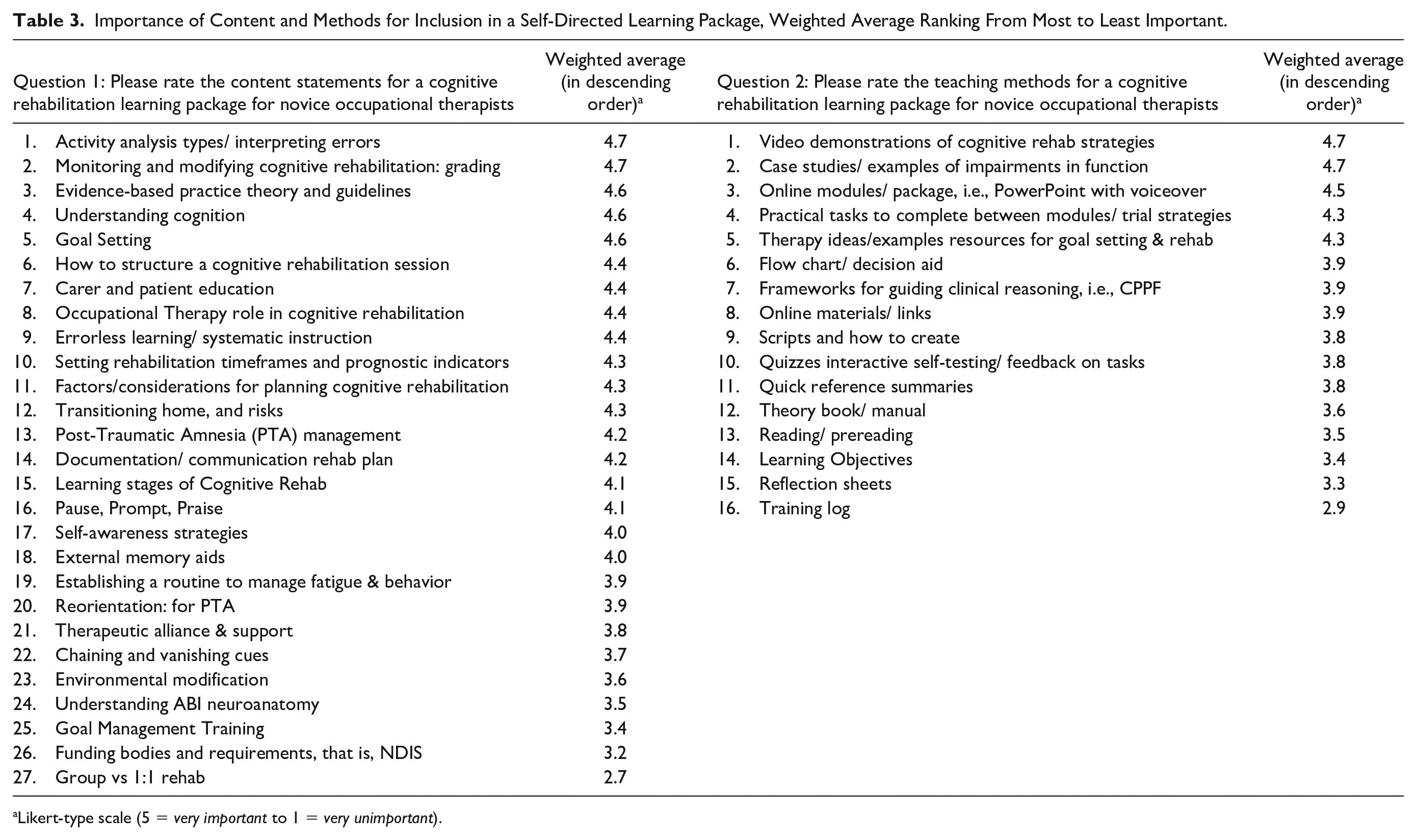
Likert-type scale (5 = very important to 1 = very unimportant).
Participants ranked the five most essential teaching methods as (a) video demonstrations, (b) case studies/examples of functional impairments, (c) online modules/packages, (d) activities to trial strategies, and (e) therapy ideas and resources.
Delivery Methods for the Learning Package
The experts’ content analysis of delivery methods identified 15 items (see Table 2). The most frequently suggested methods were (a) case studies/case examples (n = 21); (b) videos (n = 15); (c) online modules, that is, PowerPoint packages with voiceover (n = 10); (d) interactive elements, that is, self-testing quizzes; and so on (n = 7). The Mentimeter results were consistent with the content analysis, noting the methods ranked highest by participants were (a) video demonstrations, (b) case studies/case examples, (c) online modules/packages with voiceover, and (d) practical tasks to trial strategies (see Table 3).
Discussion
The vNGT focus groups enabled the rapid assimilation of experts’ perspectives on the content and teaching methods for an SDLP designed for novice occupational therapists to support clinical reasoning when planning cognitive rehabilitation. Experts identified that key content should include EBP theory and guidelines, delivering cognitive rehabilitation strategies, setting goals and measuring progress, understanding neuroanatomy and cognition, and planning cognitive rehabilitation. Experts ranked the modification of cognitive rehabilitation through activity analysis and understanding the evidence-based guidelines as key areas to address.
Experts identified that the SDLP delivery should include video demonstrations, case studies showcasing difficulties encountered in daily routines, an online package with voiceover, practical activities, and resources to aid in goal setting and rehabilitation planning. The content analysis aligned with Mentimeter ratings, where experts ranked these three methods as the priority teaching tools. These methods correspond with the literature, underscoring the importance of providing real-life examples to enhance clinical reasoning among novice occupational therapists (Neistadt, 1998). Participants emphasized the importance of using case studies, including video case studies, to develop clinical reasoning, which is consistent with current literature on approaches to enhance education (Burke et al., 2024; Rodríguez-Bailón et al., 2021; Schettino & Capone, 2022). In addition, participants recognized reflection, self-assessment, and EBP resources as methods to support novice clinicians, aligning with occupational therapy literature on developing expertise (Benfield, 2025).
Experts ranked activity analysis highly, indicating that novice occupational therapists must develop skills to identify functional errors and reason about patient performance before planning cognitive rehabilitation. This analysis connects directly to planning cognitive rehabilitation by integrating information about the individual, environment, and occupations. In hospitals, occupational therapists must apply clinical reasoning to analyze errors from standardized and functional tasks for effective discharge recommendations (Giles et al., 2020). This is supported by Bottari and colleagues (2007), who found that even expert occupational therapists require contextual information concerning the person, environment, and occupations to analyze errors, target treatment, and plan discharge accurately. Hence, an essential component of a learning package will be to facilitate novices to consider the patient’s individual factors, environment, and occupations when analyzing errors.
Participants raised the topic of cognitive assessment in both the survey and during vNGT focus groups. While the primary focus of the research question was on rehabilitation rather than assessment, the experts considered assessment an essential component of occupational therapists’ clinical reasoning in planning rehabilitation. Consequently, this suggests that the topic of assessment needs to be incorporated into the SDLP module through the exploration of cognitive impairments and functional performance errors to inform the development of effective cognitive rehabilitation strategies.
Identified content not prioritized through the ranking process included environmental modification, understanding neuroanatomy of ABI, goal management framework/training (GMF/T), funding bodies, and group versus 1:1 rehabilitation. There are several potential reasons why experts did not prioritize these themes. One reason is the perception that specific topics, such as ABI neuroanatomy, are more suitable for undergraduate-level content education. In addition, some themes, including GMF, may be considered more relevant to outpatient than inpatient settings. Furthermore, topics like funding may not be viewed as directly pertinent to providing cognitive rehabilitation. While this content does not need to be covered in any detail (if at all) within an SDLP, neuroanatomy, given its association with functional outcomes, should be included in introductory modules related to procedural reasoning.
Streamlining the Five-Step NGT process by conducting initial brainstorming through an online survey was advantageous. This approach helped navigate the complex nature of the questions and facilitated thematic assimilation before the group discussion. Furthermore, using an online rather than a traditional face-to-face focus group enabled occupational therapists across Australia to participate, reducing geographical and time barriers that might impact recruitment. The participants were highly experienced in cognitive rehabilitation and most had postgraduate education, supporting the validity of the findings (Murphy et al., 1998).
Limitations
Online data collection methods are commonplace following the COVID-19 pandemic (Willemsen et al., 2022). However, a potential limitation of this study is that many participants were drawn from one country and only two of the eight states and territories; they were predominantly from the states where the lead author had preexisting professional networks. It is also noted that definitions of expertise are not well-established in occupational therapy, and the definition of “experts” in cognitive rehabilitation was developed for use in this study. While 41% of participants had educational experience, it is important to note that they were primarily clinical experts. As such, while they understood the clinical needs of novices, they may have lacked expertise in relation to approaches for delivering cognitive rehabilitation education. Furthermore, it is acknowledged that identifying experts is challenging. This study listed several criteria that participants needed to meet to qualify as an expert, including clinicians’ self-identification, which relies on their insight into their abilities. Future studies need to consider whether self-identification of expertise is sufficiently reliable, particularly given the emerging perspective of adaptive expertise (Benfield, 2025) and how this might be operationalized to identify experts.
Finally, applying a 5-point Likert-type scale in this study may not have allowed for granularity in the Mentimeter ratings. Experts considered many themes as important or very important; thus, adopting a more refined scaling approach could have improved the ability to differentiate between the varying levels of importance assigned to each theme.
Implications for Practice and Future Research
The findings indicate that an SDLP to enhance the clinical reasoning of novice clinicians in cognitive rehabilitation should incorporate videos and case studies demonstrating the application of EBP guidelines to set goals, structure, modify, and complete occupation-based cognitive rehabilitation. For clinical educators who seek to develop clinical reasoning among their new graduate occupational therapists, there should be an emphasis on staff improving their understanding of cognitive impairments and interpretation of cognitive errors during activity analysis. This may help prepare occupational therapists to work with patients who have acquired brain injuries more effectively.
For novice occupational therapists, the findings highlight key priority areas that they should focus on and actively engage with. New graduates can significantly enhance their skills in this field by concentrating on essential aspects of cognitive rehabilitation, such as their understanding of cognitive impairments and interpretation of cognitive errors during activity analysis. Furthermore, for mentors and hospital-based educators, the recommendations for SDLP content and delivery methods may be employed to develop competencies and generate practical tutorial topics for staff. The priorities identified from this study can now be used to develop an SDLP to support novice occupational therapists’ clinical reasoning when planning cognitive rehabilitation, and the effectiveness of such learning packages can be assessed.
Conclusion
Many novices struggle with their clinical reasoning when planning cognitive rehabilitation following assessment for their patients with ABI. Hence, this study aimed to determine what experts perceive novice occupational therapists need from an SDLP to enhance clinical reasoning when working with inpatients with cognitive impairments following ABI. Experts identified that the key content of an SDLP should include evidence-based cognitive rehabilitation practice, neuroanatomy, goal setting, interpreting errors, and planning and delivering rehabilitation strategies. To teach this content via an SDLP, experts recommended methods to enhance clinical reasoning should include case studies, videos, online modules, and self-testing. Through identifying these learning priorities and content, future studies can now develop and evaluate an SDLP. This SDLP aims to foster the development of clinical reasoning among inpatient novice occupational therapists, ultimately enhancing the delivery of cognitive rehabilitation for inpatients with brain injuries.
Footnotes
Acknowledgements
The authors express gratitude to the expert participants for their time and acknowledge Dr. Karen Roberts, Alfred Health’s Occupational Therapy Manager, for her support in allowing researchers and participants time release to engage in the study.
Authors’ Note
All authors have been involved in the study’s implementation and in the decision to prepare and submit the article, accept responsibility for its publication, and be accountable for its publication.
Data Availability Statement
The data supporting this study’s findings are available on request from the corresponding author. The data is not publicly available due to privacy or ethical restrictions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: J.W. is supported by an Australian Government Research Training Program (RTP) Fee-Offset Scholarship through Federation University Australia. N.A.L. is supported by a Heart Foundation (Australia) Future Leader Fellowship (#2).
Ethical Approval
This study was given ethical clearance by the Federation University Human Research Ethics Committee (2022/055).
Informed Consent
Before beginning the survey, each participant electronically signed consent and eligibility forms using the Qualtrics online platform. If participants consented to be contacted for the focus group, they provided their details to the researcher.