
Abstract
Attention deficit/hyperactivity disorder (ADHD) is characterized by inattention, hyperactivity, and impulsivity, as children may present developmental and chronic impairments in cognitive–emotional and sensory-motor aspects. This study examined the changes in self-efficacy, muscle tone, and mood following a single session of Equine-Assisted Occupational Therapy (EAOT) within Attention Skills Therapy (ASTride) intervention, designed to improve emotional and cognitive functions. Notably, 31 children diagnosed with ADHD aged 6–12 (mean age 10.06) years. A preliminary study of pre- and post-single 45-min session was performed, using the New General Self-efficacy Scale (NGSE), the Moos Scale Questionnaire (MSQ), and the prone extension test. A significant improvement in self-efficacy and in positive mood, and a decrease in negative mood were found, along with a significant improvement in core muscles. This study provides preliminary evidence supporting the effectiveness of EAOT for children with ADHD regarding emotional and sensory-motor (vestibular) functions.
Plain Language Summary
Children with attention deficit/hyperactivity disorder (ADHD) often struggle with emotional and motor challenges, including difficulties with regulating their mood and maintaining motor control. Traditional treatments such as medication and therapy focus on cognitive and emotional skills, but there is increasing interest in complementary interventions that can address both physical and emotional aspects simultaneously. One such approach is Equine-Assisted Occupational Therapy (EAOT), which involves working with horses to promote emotional regulation, motor coordination, and overall well-being. This study explores the effects of a single session of EAOT, using the ASTride protocol, on children with ADHD. The ASTride intervention combines sensory, cognitive, and emotional elements, using horse care, riding exercises, and reflective activities to improve attention, mood, and self-regulation. The session involves structured activities, such as preparing the horse, riding, and practicing motor skills, all while being guided by an occupational therapist and a certified riding instructor. Results showed that after just one session, children demonstrated significant improvements in mood, including increased feelings of calm, self-efficacy, and control. They also showed enhanced motor skills, as reflected in their ability to maintain posture and balance during the riding exercises. These improvements suggest that EAOT could be a valuable addition to traditional ADHD treatments, offering both emotional and motor benefits. Although the study was preliminary and involved a small number of participants, it highlights the potential of EAOT as a promising intervention for children with ADHD. Future research is needed to confirm these findings and explore the long-term effects of this approach.
Keywords
Introduction
Attention deficit/hyperactivity disorder (ADHD)—a neurodevelopmental disorder characterized by inattention, hyperactivity, and impulsivity symptoms—is one of the most common pediatric diagnoses. Approximately 11% of children aged 3–17 years are diagnosed with ADHD, with boys twice as likely to be diagnosed (Banaschewski et al., 2018). Impairment of social, behavioral, or psychological development resulting in weak psychosocial functioning and high prevalence of emotional problems is common in children and adolescents with ADHD (Wehmeier et al., 2010). These emotional problems include impulsiveness, deficient self-regulation, anxiety, depression, low self-esteem, aggressive behavior, and lower self-efficacy (Banaschewski et al., 2018; Colomer et al., 2017; Heiman et al., 2014). Self-efficacy—the belief in one’s own capabilities—can affect cognitive aspects, such as attention, memory, problem-solving, and decision-making along with self-regulation (Heiman et al., 2014). Self-regulation—the ability to recognize and control one’s behavior, emotions, and general mood—is needed for everyday functioning and daily living (Cibrian et al., 2022). Deficits in these psychological functions can lead to significant difficulties in academic achievements, and in social and personal relationships (Wehmeier et al., 2010).
Motor impairment is prevalent in children with ADHD, with approximately 50% meeting the criteria for Developmental Coordination Disorder (DCD)—characterized by motor skills that are significantly below age-expected levels despite opportunities to acquire and develop the skills (Bart et al., 2013). Evidence suggests that motor impairment in ADHD does not simply reflect delayed development, but rather an uneven profile of impairment across different motor skills (Farran et al., 2020). Children with ADHD frequently display clumsiness and encounter challenges with both gross and fine motor movements and maintaining balance (Bart et al., 2013). Some of these difficulties may result from abnormal muscle tone (Gillberg, 2003) or low muscular strength and endurance (Jeoung, 2014).
The current recommendation for the most effective intervention for children with ADHD is a combination of administration-approved pharmacotherapy. Stimulant medication (methylphenidate and amphetamine) is the most common pharmacotherapy to reduce ADHD symptoms (Banaschewski et al., 2018). Other, non-pharmacological, interventions include psychological interventions, such as psychotherapy, behavioral therapy, psychoeducation for parents, and expressive therapies (Pelham & Fabiano, 2008). Additional approaches are based on the principle of brain plasticity and rely on intensive repetitive training and immediate feedback (Dovis et al., 2015).
Successful occupational therapy (OT) interventions for children with ADHD are client-centered and occupation-based. They focus on personal functional goals and include strategy acquisition through cognitive training of single or multiple domains of executive functions, such as working memory, inhibition, or cognitive flexibility (Hahn-Markowitz et al., 2017). These include the Cog-Fun intervention—designed to improve executive functions by embedding cognitive strategies into meaningful everyday activities (Hahn-Markowitz et al., 2020)—and the POET intervention—a collaborative program designed to improve children’s executive functions and daily performance by integrating parents into the therapeutic process (Frisch et al., 2020). Another OT intervention includes the sensory integration approach, developed by Ayres (1972), as a neurophysiological approach based on the association between sensory processing and behavior. Sensory processing is defined as the capacity of the central nervous system to regulate and organize the degree, intensity, and nature of an individual’s active responses to sensory information in a graded and adaptive manner (Miller & Lane, 2000). The sensory systems are the somatosensory, visual, auditory, olfactory, gustatory, vestibular, and interoceptive systems (Mahler, 2015). According to Ayres’ (1972) theory, impaired sensory processing might result in various learning, development, or emotional problems. Sensory integrative treatment emphasizes not just the provision of sensory input but also the child’s active engagement with it. The therapy encourages the child to respond adaptively to sensory stimuli by modifying the environment and by providing “just right challenge” activities. This process promotes the development of self-regulation and the ability to organize sensory information effectively in real time. As a result, children can interact more effectively with their environment and improve their functional abilities in daily activities (Zimmer et al., 2012).
Although these approaches show substantial evidence for improving executive functions and functional/academic skills, they do not address the psychological difficulties children with ADHD experience (Pelham & Fabiano, 2008). These various modes of intervention may be respectively efficacious; however, there is a growing need for interventions that concomitantly address both cognitive and emotional aspects of ADHD.
Equine-Assisted Services
Animals are increasingly used in interventions to improve human health, quality of life, and participation, enhancing physiological, cognitive, and social functions (Bass et al., 2009). Equine-assisted services (EAS) are a variety of multimodal and complex therapeutic activities designed for the achievement of therapeutic goals through the interaction of clients with equines (Wood et al., 2021). Equine-Assisted Occupational Therapy (EAOT), under the therapy division of EAS, incorporates OT approaches with the equine surroundings, using the horse as a therapy partner, aiming to promote meaningful participation in everyday occupations and well-being. Using sensory-motor and cognitive OT interventions methods can be naturally integrated within the equine and the equine environment (Helmer et al., 2024; Wood et al., 2021).
Studies have shown that horse–rider interactions improve both physiological and emotional well-being, reducing anxiety and stress, boosting self-perception, and fostering positive emotions and safe attachment (Helmer et al., 2024; Weldon, 2017). The physical interaction with the horse releases endorphins, increasing confidence and feelings of being loved (Fine, 2019; Weldon, 2017), and promoting a more positive self-perception (Beetz et al., 2012). Riding not only affects emotional aspects but also cognitive functions, including executive functions and inhibition (Gilboa & Helmer, 2020), while enhancing proprioception and physical regulation. The physical horse–rider interaction provides immediate feedback, fostering physical and mental self-regulation for the rider (So et al., 2017). Riders also develop trust with their horse, learning to manage it while caring for and fulfilling all its needs (Bachi et al., 2012). These effects have yet to be studied in children with ADHD.
Efficacy of EAS for Children With ADHD
EAS address core ADHD symptoms, cognitive–emotional challenges, and sensory-motor functions. However, evidence regarding the efficacy of EAOT for children with ADHD is limited. Existing research refers to the immediate feedback—enabling physical and mental self-regulation—riders receive from the horse (Bass et al., 2009; So et al., 2017; Souilm, 2023).
The animal–human relationship evokes attachment behavior, along with reinforcement of positive actions (Holm et al., 2014). It provides a sense of confidence, enhances self-control, and is perceived as a social connection and relationship to the participant (Fine, 2019). Furthermore, the horse and the environment increase motivation while requiring full attention and engagement, thus reducing negative emotional symptoms and enhancing positive emotions (Bracher, 2000; Weldon, 2017).
The rider–horse interaction involves extensive sensory-motor stimuli, including the vestibular, proprioceptive, tactile, and olfactory. Engel (1984) described the effects of vestibular stimulation in improving sensory integrative function. Sensory integrative treatment focuses on sensory input and its continual interaction with motion. Sensory integration plays an integral role in EAS, particularly with regard to tactile stimulation, continual motion, and subsequent vestibular and proprioceptive input (Bracher, 2000). It is suggested that sensory stimulation of both ground-level and mounted activities can help modulate physiological arousal levels, promote motor planning and function, and improve attention and emotional aspects, thus increasing engagement in activities (Bracher, 2000; Miller & Lane, 2000; Weldon, 2017).
Using the ASTride Protocol for EAOT
The ASTride protocol is a structured intervention model developed for EAOT targeting children with ADHD. Consisting of 12 weekly 45-min sessions led by an OT, EAS professional, it incorporates three OT methods: Sensory Integration (Ayres, 1972), Cognitive Orientation to Daily Occupation Performance (CO OP) (Polatajko et al., 2001), and the Multi-Context approach (Toglia & Katz, 2011).
The protocol integrates sensory, cognitive, and emotional elements through therapeutic riding to improve self-regulation, executive function, and motor skills. Children acquire strategies while engaging in horse care, executing controlled riding patterns, and reflection on their horse–rider interaction, facilitating emotional awareness and self-efficacy. The learned strategies are later transferred to other settings (Helmer et al., 2024).
Immediate feedback from both the horse and the therapist is the key to the protocol and crucial for developing self-monitoring and adaptive behaviors. ASTride protocol has shown promise in improving attention, mood regulation, strategy acquisition and transfer, and overall participation in everyday activities among children with ADHD (Helmer et al., 2024). This study analyses a single session of children who underwent the ASTride protocol to evaluate its effectiveness in addressing both emotional and motor difficulties in this population. The session included the first stage of the protocol: learning a global strategy using both mounted and unmounted activities.
EAS are found to improve emotional and sensory-motor functions, with preliminary evidence indicating benefits for children with ADHD. However, research is limited, often with small sample sizes and lacking standardized protocols. Combining OT interventions with equine therapy improves body functions and skill acquisition in children with ADHD (Gilboa & Helmer, 2020) and social skills in children with Autism Spectrum Disorder (Bass et al., 2009). Therefore, this study aims to assess the efficacy of a single EAOT session within the ASTride intervention in improving emotional (mood, self-efficacy) and sensory-motor function (prone extension) in children with ADHD, to establish and enhance evidence-based practice.
Method
Study Design
The pilot study uses a one-group pre- and post-test design, following the STROBE checklist. The intervention, part of a 12-week EAOT ASTride intervention (Helmer et al., 2024), engages the child emotionally and cognitively through structured horse care, riding activities, and reflection exercises. Measures were assessed pre and post a single EAOT ASTride session.
Human Ethics Statement
Ethical approval was received, IRB No:0003949-2. All methods were approved and carried out in accordance with the IRB guidelines. Informed consent was obtained from parents or legally authorized representative of the child participants before conducting the study.
Animal Ethics Statement
The experiment with equines was approved by IRB No:0003949-2. All methods were approved and carried out in accordance with the IRB guidelines and ARRIVE guidelines for reporting research involving animals (Xiaoyu et al., 2023).
Participants
The study comprising a convenience sample of 31 participants diagnosed with ADHD, referred to EAS by their pediatricians. Inclusion criteria included (a) children 6–12 years of age; (b) diagnosis of ADHD from a medical professional based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria, with or without medication (e.g., psychostimulant medication); (c) general doctors’ approval and referral for participation in EAS. Exclusion criteria included (a) moderate-to-severe cognitive impairment; (b) neurological disorders (e.g., epilepsy); (c) children with additional developmental disorders (e.g., Autism, Cerebral Palsy [CP]); and (d) children with severe sensory loss (e.g., blindness).
Notably, 33 children who met the inclusion criteria were approached; two participants declined due to time constraints. Participants were sampled within their third to fifth EAS session, as basic riding skills were still being implemented (walk, steer, trot) and all riders were not yet independent in riding.
However, 15 horses from local mixed breeds, aged 8–15 years participated in the study: 10 geldings and 5 mares. All horses were trained for therapeutic riding lessons, with minimum 5-year experience.
Measures
Demographic Questionnaire
Demographic features of the child and parents, including age, marital status, child’s diagnosis and medical treatment, education, and income, were collected.
The Moos Scale Questionnaire
A self-report measure of participants’ views of their own affect and mood, consisting of 20 items on a five-point Likert-type scale, ranging from 1 (not at all appropriate) to 5 (very appropriate) (Moos et al., 1987). The total range score is from 20 to 100. There are two subscales: with 10 positive affect items (e.g., friendly, in control, and happy) and 10 negative affect items (e.g., sad, tired, or worried). A total score is calculated by summing the two subscales. Cronbach’s alpha was .74 (Lackaye & Margalit, 2006). Internal reliability in this study was satisfactory for positive mood (α = .75) and negative mood (α = .61).
The New General Self-Efficacy Scale
An 11-item, five-point Likert-type scale self-report questionnaire designed to measure a general set of expectations that an individual carries into new situations, and their perception regarding their abilities to achieve goals in various situations and overcome challenges (Chen et al., 2001). Total score is calculated by the sum of all items, ranging between 8 and 24. The importance of the NGSE lies in its ability to (a) predict specific self-efficacy (SSE) across situations and tasks, (b) predict general and comprehensive performance criteria, and (c) buffer against the debilitating effects of adverse experiences on subsequent SSE. The NGSE scale has high internal consistency reliability (α = .86 and .90). Test–retest coefficients show that the NGSE scale is stable (r = .67). Content validity was also found. Internal consistency in this study was satisfactory (α = .65).
The Prone Extension Test
A measurement of vestibular functioning used by OTs to assess suspected vestibular system and muscle strength deficits (Gregory-Flock & Yerxa, 1984). The test begins with the child lying prone on a mattress while the examiner guides through three practice stages: lifting the upper body, the lower body, and both simultaneously. Once the child assumed the correct positions—with examiner’s support to prevent fatigue—they rest for a minute before repeating the exercise. Cut-off score is 20 s, indicating good performance (Bart et al., 2007; Bundy & Fisher, 1981). Test–retest reliability coefficient on the duration score was r = .79, and on the quality score r = .77 (Gregory-Flock & Yerxa, 1984).
Procedure
After obtaining ethical approval, eligible participants were recruited from Mount Judea stable, an EAS provider with more than 300 clients. Once the consent form was signed by parents and the assent form signed by the children, participants were asked to complete a 15-min assessment battery, including the Moos Scale Questionnaire (MSQ; Margalit et al., 1991); the New General Self-Efficacy Scale (NGSE) (Chen et al., 2001), and the Prone Extension Test (Gregory-Flock & Yerxa, 1984). All children completed the MSQ and the NGSE independently. Participants repeated the assessments immediately after the intervention session. Assessments were conducted by two blinded OTs. The intervention was provided by a licensed OT and certified advanced therapeutic riding instructor with more than 8 years’ experience (see EAOT intervention below).
EAOT ASTride Intervention
The 45-min treatment session included acquaintance with the horse, tacking-up and preparing for mounting, warm up, acquisition and practice of riding skills, and session summary. During the session, participants learned about horses’ emotions and nonverbal communication, and how their own emotions related. Parents were present during the intervention sessions. Throughout intervention, emphasis was placed on sensory and vestibular input, with frequent changes in rhythm and direction. This included approximately 30 min of intensive aerobic activity, adjusted to rider’s abilities and experience. In addition, cognitive strategies—according to CO-OP principles—were used during skill acquisition. As the CO-OP approach provides a foundational method for task-focused problem-solving and goal-setting, the multicontext helps the child apply these strategies to different contexts and environments, which is crucial for generalizing the learned skills and strategies to different contexts and environments. For example, the children used a checklist while preparing the horses to monitor their performance, later receiving homework to transfer the same strategy for preparing their school backpacks.
Statistical Analysis
Descriptive statistics were obtained on participants. Quantitative data were analyzed using SPSS 27.0. Repeated-measures analysis of variance (ANOVA) test was performed to assess pre–post differences on sequential variables and Wilcoxon test on categorical variables. A p-value of less than .05 was considered statistically significant in all comparisons. Effect size values were computed using Partial eta square, determined as follows: small effect size > .01, medium effect size > .06, and large effect size >.14 (Richardson, 2011).
Results
The study sample included 35 participants diagnosed with ADHD. Four participants declined to participate for scheduling reasons, thus results were analyzed for 31 participants (20 boys, 11 girls; mean age= 10.06 years, SD 2.084). Table 1 lists participant characteristics. Approximately 50% of participants were under medication during the intervention session. We examined differences between children with and without medication in post-intervention improvement in Positive and Negative mood, NGSE, and prone extension test, but found no significant differences (all ps > .05). Therefore, we addressed all participants as one group in the analysis.
Participant Characteristics (N = 31).
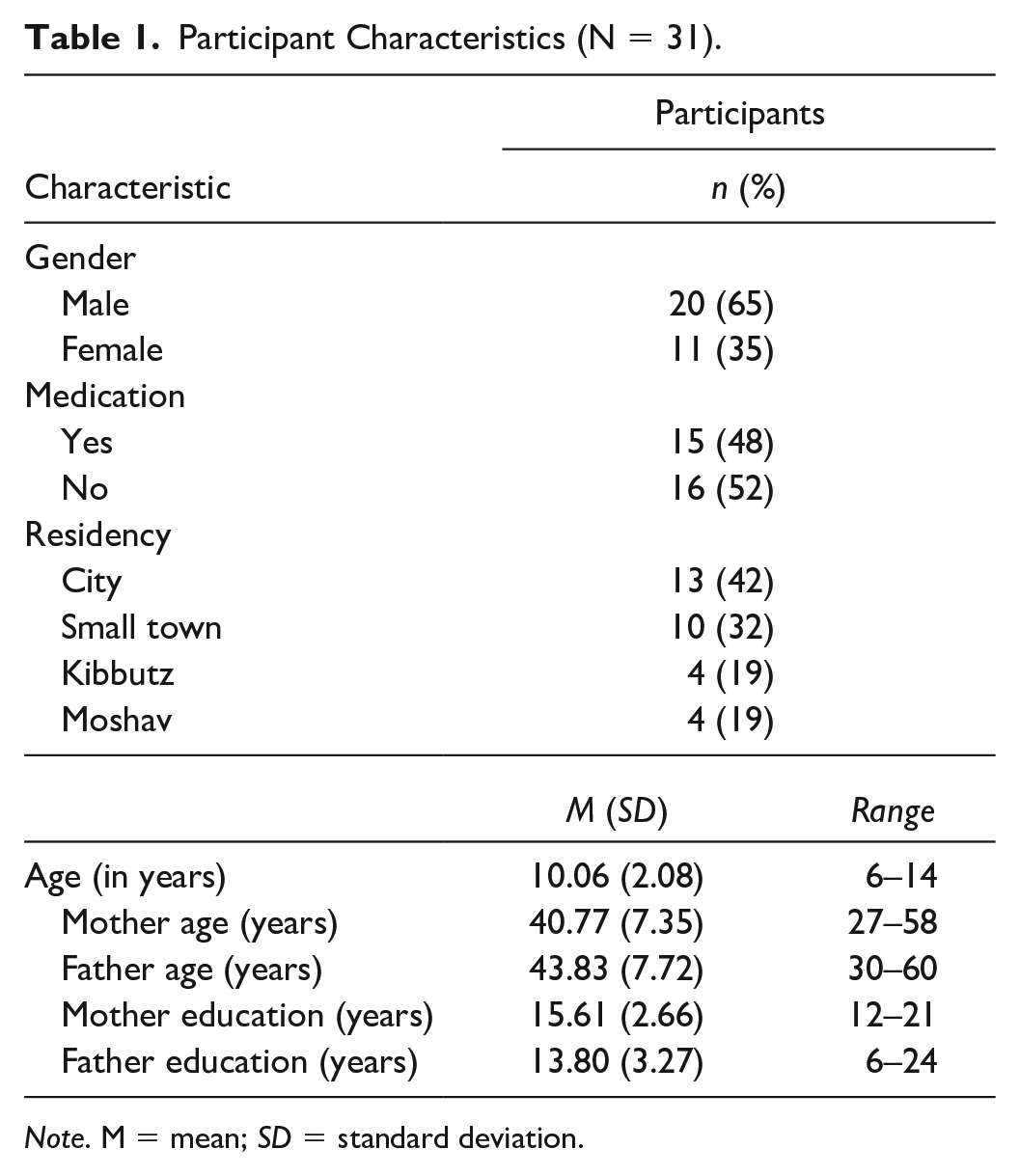
Note. M = mean; SD = standard deviation.
Total positive and negative mood scores were calculated for the MSQ. Results showed significant differences between pre- and post-intervention. The positive mood subscales of Feeling Calm, Successful, Self-efficacy, Can Be Trusted, In Control, Happy, and Determined were increased significantly post-intervention. A statistically significant decrease was found in the negative mood subscales of Sad, Trouble Concentrating, Agitated, Scared, Restless, and Feeling Worried, as seen in Tables 2 and 3. Repeated-measures ANOVA was used on the total positive score of the MSQ. Wilcoxon test was used to assess differences between pre- and post-intervention regarding each separate statement in the positive scale. Statistical significance was found in 11 mood statements and in the total scores (t = 4.94, p < .001) of pre (M = 4.02, SD = 0.62) and post (M = 4.44, SD = 0.55), indicating a more positive mood after intervention. Effect size for positive mood was scored high (.33).
Comparison of Pre–Post Change in Positive Mood According to the MSQ (N = 31).
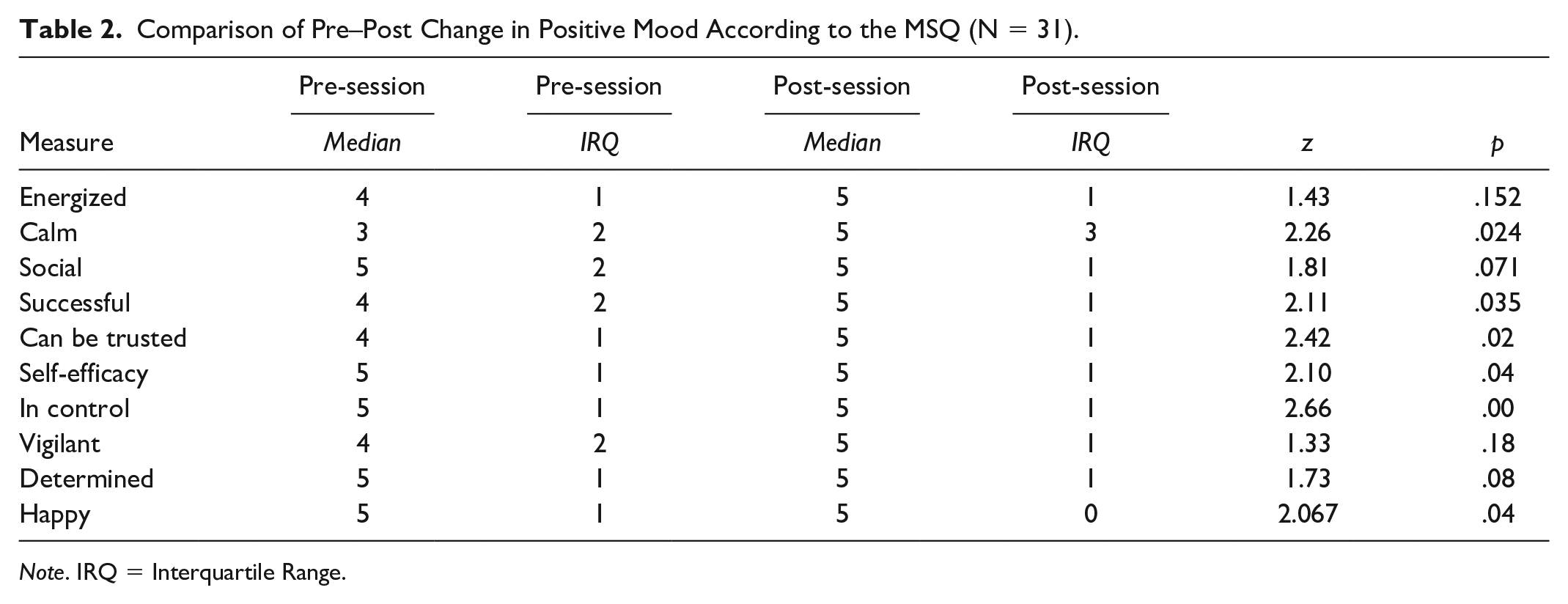
Note. IRQ = Interquartile Range.
Comparison of Pre–Post Change in Negative Mood According to the MSQ (N = 31).
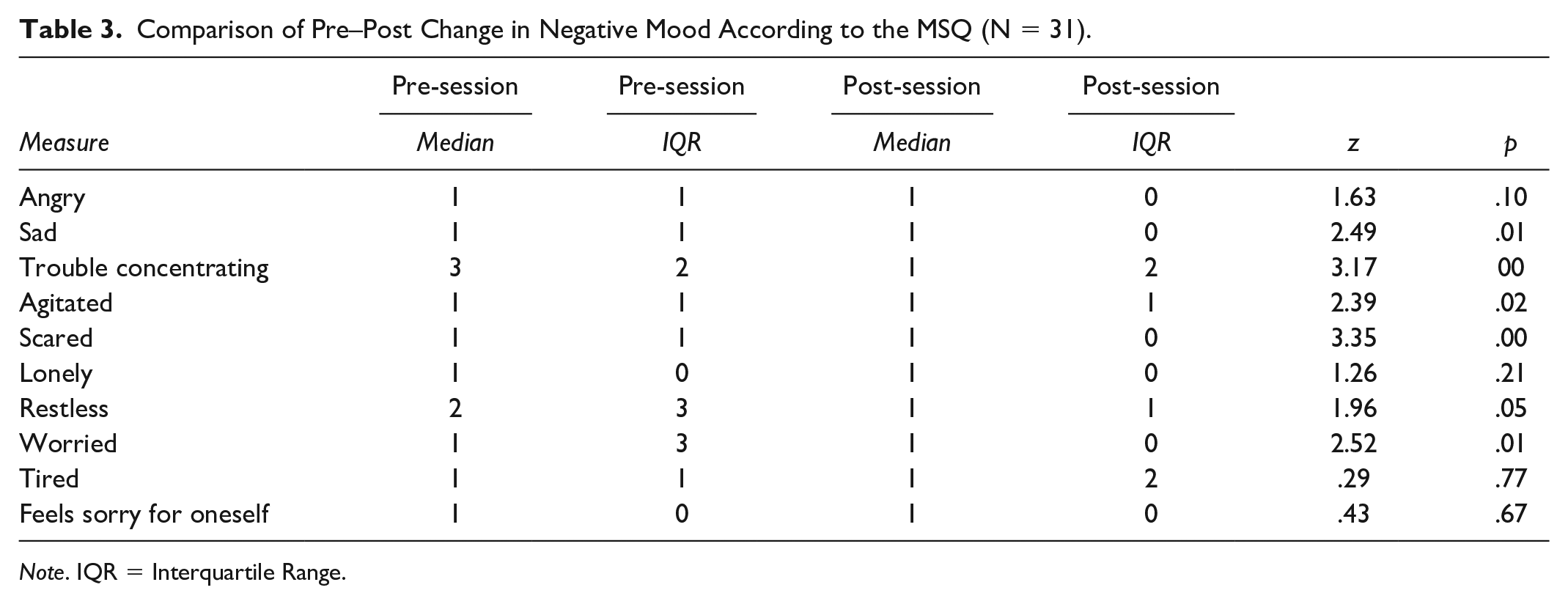
Note. IQR = Interquartile Range.
Repeated-measures ANOVA test was used pre- and post-intervention on the total negative score of the MSQ. Wilcoxon test was used to assess differences between pre- and post-intervention regarding each separate statement in the negative scale. Statistical significance was found in six mood statements and in the total scores pre and post, indicating a more positive mood and decreased negative mood post-intervention. Effect size for total negative mood was scored high (.94) (see Table 3).
Repeated-measures ANOVA test was used to assess perceived self-efficacy using the NGSE and the prone extension test. Statistical significance was found in total scores of perceived self-efficacy pre- and post-intervention, indicating a higher level of self-efficacy post-intervention with a large effect size (.99). A statistically significant difference was found between pre- and post-intervention in the prone extension test (p < .001) with a large effect size of .33. Participants held position longer post-intervention in comparison to pre-intervention (see Table 4).
Comparison of Pre–Post Change and Effect Size Variable for All Measures (N = 31) Using ANOVA Test.
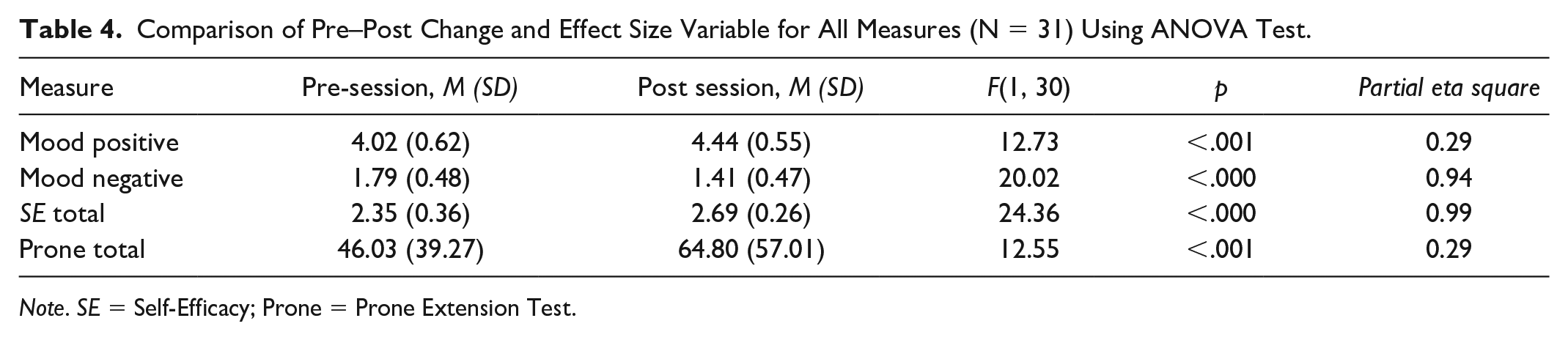
Note. SE = Self-Efficacy; Prone = Prone Extension Test.
Discussion
Children with ADHD are increasingly referred to EAOT, though evidence on its effectiveness is limited. This pilot study aimed to address the lack of evidence and enhance the understanding of how EAOT could benefit clients and support therapeutic goals (White et al., 2020). The study examined the effect of a single session of ASTride intervention on emotional and motor aspects in school-aged children with ADHD. This preliminary study supports the potential of EAOT ASTride intervention for children with ADHD. Literature shows that ADHD treatments that combine medication with other intervention methods are more effective. For example, the combination of Cognitive Behavioral Therapy (CBT) and medication yielded greater results compared with CBT alone in alleviating ADHD symptoms, enhancing organizational skills, and boosting self-esteem (Cherkasova et al., 2020). In our study, children with and without medication presented similar improvement, supporting the advantages of EAOT.
The Effectiveness of EAOT on Emotional Aspects: Mood and Self-Efficacy
This single-session ASTride intervention demonstrated significant improvement of the emotional aspect of children with ADHD, as evidenced by the children’s improved mood and self-efficacy perception post-session. Similarly, in Martin and colleagues’ (2017) qualitative study, children with various diagnoses reported an increased sense of overall mood and self-esteem following EAOT intervention. Improved emotional co-regulation may result from the communication with the horse and the therapist, and exposure to varied sensory stimuli in the EAOT intervention.
The interaction between child and horse enables the child to learn how to detect others’ emotions and develop the capacity to regulate their own emotional state accordingly (Scopa et al., 2019). Verbal cues are needed for communication with the horse, and verbal communication with the therapist is necessary for planning actions, analyzing situations, and following instructions. Gratifying communication with the horse and the therapist may improve the emotional state of the participants (Bart et al., 2009). Moreover, post-session, participants reported they had greater feelings of control, were more determined, and less agitated and restless, supporting improvements in their emotional state.
The intervention incorporated additional forms of communication with the horse, including tactile communication, which provides intensive tactile stimuli that may also affect the emotional aspects. Fine (2019) found that touching and petting an animal causes endorphins to be released within the nervous system, facilitating anxiety while encouraging safe attachment. Touch evokes positive emotions, such as sense of confidence and feeling loved, which contribute to tactile perception, discrimination, motor planning, and emotional responses (Lane et al., 2019), and stimulates the motivational system (Pawling et al., 2017). Accordingly, participants reported being happier, calmer, and less worried post-session.
Riding provides intensive vestibular and proprioceptive input, which is found to decrease anxiety and improve self-efficacy among children with mild developmental disabilities (Bart et al., 2009). During the study, the children practiced various riding exercises, including rhythm changes, such as walk and trot, providing various vestibular and proprioceptive stimuli. These frequent changes enabled the children to monitor self-regulation in ever-changing conditions, reflected in increased positive mood and improved self-efficacy—specifically improvement in the feeling of being in control and successful. This supports a previous study showing that vestibular stimulation can modulate mood and affective processing in healthy participants (Preuss et al., 2014).
People with more positive mood tend to be more confident of success (Brown, 1984). Improving mood through horse riding may help children with ADHD feel more success, as evidenced by increased self-efficacy and determination, and reduced worry by participants post-intervention. This feeling may transfer to other environments, such as educational settings, where ADHD affects the ability to succeed (DuPaul et al., 2011). As children with ADHD often struggle with emotional regulation and hope (Lackaye & Margalit, 2006; Wehmeier et al., 2010), interventions such as EAOT are crucial for facilitating mood and contributing to emotional regulation. Further studies may wish to assess longer EAOT interventions that aim to improve emotional regulation.
The Effectiveness of EAOT on Motor Aspects
Post-intervention showed core muscle activation, which may improve in core strength, as reflected in the prone extension test (Bart et al., 2007; Bundy & Fisher, 1981). This activation may result from the vestibular input and motor activity of the participants while riding. The horse’s reciprocal movement provides somatosensory input—touch, proprioception, and vestibular—and produces pelvic movement in the rider that mimic human ambulation (Bracher, 2000; Uchiyama et al., 2011). In addition, muscle spindles—in reaction to changes in muscle length—activate vestibulospinal and proprioceptive reflexes, influencing muscle tone (Kazemi et al., 2022). Affected core muscles, as the main contributors to trunk and upper body balance and stability, may be the contributing factor to participants’ ability to hold position for longer in the prone extension test post-intervention.
A study on children with CP—a population that suffers from abnormal gait patterns and posture—found that horse riding leads to improved postural control, muscle tone, and equilibrium responses, and decreased muscle weakness (Sterba, 2007). During the riding session, it is necessary for the rider to control his muscles, and thus exercise motor planning and movement (Bracher, 2000). This muscle control may contribute to the improvement in muscle tone and strengthen core muscles. It is important to note that all participants were novice riders and the effect presented in the study may not be present among more experienced riders.
Further studies may wish to assess the length to which these changes last and whether they transfer to other settings. A longer intervention may facilitate emotional difficulties and improve motor function. Improving motor functions and emotional aspects may enhance participation and everyday function in children with ADHD.
Study Limitations
Children were recruited via convenient sample method, with a relatively small sample size, limiting generalizability. As a pilot study of a single 45-min session, results may be influenced by confounding variables, such as change in environment. Future research should assess longer EAOT interventions, including follow-up assessments on mood, self-efficacy, and muscle tone in children with ADHD. This preliminary study does not enable generalization or transfer to other environments. Stronger designs, such as randomized controlled trials, are needed for future studies.
Conclusion
The results of this pilot study demonstrate a positive effect of a single session of ASTride intervention for novice riders with ADHD. The positive results support a more comprehensive investigation using a larger population sample. This study seeks to contribute to the body of knowledge on the improvement of mood, self-perception, and muscle tone in children with ADHD. EAOT has many advantages and can contribute to children with ADHD. However, evidence is scarce, and mechanisms of change are yet to be fully explained. Further research may help practitioners better understand EAOT’s unique contribution.
Footnotes
Acknowledgements
The authors thank all study participants and their families for taking part in this study, and the stables, staff, and horses. All authors have each made a substantial contribution to the concept and design of this study, to the acquisition and data analysis, and to the writing of the manuscript.
Animal Ethics Statement
The experiment with equines was approved by the Sackler Faculty of Medicine of Tel Aviv University (IRB No:0003949-2). All methods were approved and carried out in accordance with the IRB guidelines and ARRIVE guidelines for reporting research involving animals. (NC3RS, 2023).
Compliance With Ethical Standards
No competing financial interests exist. This research has been approved by Tel Aviv University Ethics Committee (Approval no. 00039493). The research is registered in addition at Clinical Trials. gov (Identifier no. NCT05869253), first registration at May 22, 2023.
Data Availability
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
This work was performed in partial fulfillment of the requirements for the PhD degree of Anne Helmer, Sackler Faculty of Medicine, Tel Aviv University, Israel.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human Ethics Statement
Ethical approval was received from the Sackler Faculty of Medicine of Tel Aviv University (IRB No: 0003949-2). All methods were approved and carried out in accordance with the IRB guidelines. Informed consent was obtained from parents or legally authorized representative of the child participants before conducting the study.