
Abstract
Background:
Pre-existing mental health diagnoses may contribute to greater emotional symptom burden and prolonged recovery after concussion.
Hypothesis:
Youth with pre-existing mental health diagnoses will have greater emotional symptom burden, greater risk for delayed return to exercise, and more prolonged recovery from concussion than those without those diagnoses.
Study Design:
Prospective cohort.
Level of Evidence:
Level 3.
Methods:
A prospective registry of youth concussion was examined for differences in emotional symptom burden after injury to develop a predictive risk model for prolonged recovery. The impact of individual and total number of pre-existing mental health diagnoses (0, 1, 2, and 3+) was assessed, and multivariable logistic regression was performed to identify factors associated with prolonged recovery.
Results:
Among a cohort of 3105 youth with concussion, those with a history of mental health diagnoses, in a dose-response fashion, had greater postinjury emotional symptom burden (7 emotional symptoms vs 4; P < 0.01), visio-vestibular dysfunction (65% abnormal vs 56% abnormal; P < 0.01), later return to symptom-limited exercise (23 vs 21 days; P < 0.01), and overall longer concussion recovery (38 days, interquartile range [IQR] 18, 80) versus 25 days (IQR 13, 54; P < 0.01). Boys with prolonged recovery after concussion had greater emotional symptom burden than girls (5 emotional symptoms vs 3; P < 0.01).
Conclusion:
Pre-existing mental health diagnoses are associated with greater postinjury emotional symptom burden and longer concussion recovery in a dose-response fashion. Visiovestibular deficits and delayed return to exercise are also associated with pre-existing mental health diagnoses and prolonged recovery. Boys with prolonged recovery from concussion experience greater emotional symptom burden than girls.
Clinical Relevance:
Addressing pre-existing mental health diagnoses is essential to concussion management. Boys with prolonged recovery from concussion may particularly benefit from interventions to address their higher emotional symptom burden. Interventions, including a home visio-vestibular exercise program and symptom-limited exercise, may contribute to improving time to concussion recovery.
Keywords
Concussions are a common injury in childhood, with an estimated 2 million sport- and recreation-related concussions occurring annually in the United States. 4 In a nationally representative sample of American youth, 18.2% of middle school students and 14.3% of high school students reported sustaining a sport- or physical-activity-related concussion in the last year, 30 comprising a large public health burden with the cost of pediatric concussion estimated to be $4500 per child with persistent symptoms, equaling over $200 million annually. 5 As a form of mild traumatic brain injury, concussions may also have a substantial impact on a child’s participation in activities, such as school and sports, and, consequently, their quality of life. 17
Multiple domains may be affected after concussion, including cognitive, emotional, sleep, visual, and vestibular function.3,9-11,13,16,22,25 Pre-existing conditions involving these domains, including mental health disorders, may be exacerbated by concussion, 22 and interactions between domains of dysfunction may contribute to persisting symptoms, but the characteristics of these interactions are not well understood. The emotional domain may be particularly challenging to assess by clinicians and others working with children and adolescents with concussion, due to stigma attached to various mental health symptoms and diagnoses 28 ; thus, prompt recognition of mental health issues and understanding their interaction with other factors are important first steps toward developing targeted individualized approaches to treatment after concussion. 13
While most children and adolescents will recover from their concussion within a month after injury, approximately 30% go on to have persisting postconcussive symptoms (PPCS) beyond 28 days that can negatively affect quality of life. 35 Risk factors for PPCS have been described and include a previous history of mental health conditions such as anxiety, depression, attention deficit hyperactivity disorder,19,23 but data are conflicting, with some studies indicating no increased risk for PPCS associated with these pre-existing mental health disorders. 35 Visio-vestibular deficits are a common occurrence after concussion and have been shown to be both a key component of the pathophysiology underlying the disruptions in quality of life for pediatric patients after injury and a risk factor for PPCS, 24 and may further add to the symptom burden that concussion patients with pre-existing mental health disorders already bear. However, the interaction between visiovestibular dysfunction, emotional symptom burden, and pre-existing mental health diagnoses is unknown. In addition, early symptom-limited exercise shortly after concussion has been shown to hasten symptom resolution and decrease the risk of developing PPCS.20,21 As a potential active intervention, exercise may be particularly important for those with pre-existing mental health diagnoses where it has been demonstrated to ameliorate depression, anxiety, and dizziness symptoms in general, as well as after concussion.15,18 It is unknown, however, when pediatric patients with emotional symptoms or pre-existing mental health diagnoses return to exercise after concussion. Identifying and addressing these modifiable risk factors for PPCS represents an important opportunity for improving outcomes for children and adolescents with concussion. To our knowledge, there has not been an examination of potential relationship between pre-existing mental health diagnoses, emotional symptom burden after concussion, and visio-vestibular function in concussed pediatric patients. Understanding how modifiable risk factors for PPCS interact with pre-existing mental health diagnoses is a critical gap, limiting opportunities to improve outcomes for a substantial proportion of the pediatric population afflicted with these disorders.
In light of this, our aims for this study were to explore a large prospective registry cohort of pediatric patients diagnosed with concussion, through the lens of the preinjury burden of mental health disorders and their potential impact on postinjury emotional symptom burden and recovery from concussion. We hypothesized that pre-existing mental health diagnoses would predict increased emotional symptom burden among all children and adolescents acutely after concussion, regardless of time to recovery. In addition, we hypothesized that a history of mental health disorders would also confer an increased risk of prolonged recovery, as well as elevated emotional symptom burden in those with prolonged recovery. We also sought to explore the interaction of previous mental health diagnoses and emotional symptom burden with other factors, such as visio-vestibular function and time to return to symptom-limited exercise.
Methods
Patient Cohort
Data for this investigation were collected prospectively through a concussion registry via standardized data collection forms in the electronic health record (EHR), 26 which includes all patients presenting for specialty sports medicine clinical care for concussion at widely geographically distributed care sites (urban and suburban) across a large tertiary care pediatric clinical network. 1 This analysis was limited to patients ages 5 to 18 years diagnosed with a concussion in the specialty care setting of a concussion program, seen within 14 days of injury between January 3, 2017 and March 31, 2023, and followed through clinical recovery. Patients were excluded if they were seen later than 14 days after injury. The diagnosis was made by board-certified pediatric sports medicine physicians according to the criteria outlined in the International Consensus Statement on Concussion in Sport. 27 The study was approved by the Children’s Hospital of Philadelphia Institutional Review Board.
Measures
Patients completed a standardized demographic questionnaire, which included age and patient-reported previous medical history, including self-reported pre-existing mental health diagnoses, such as anxiety, depression, eating disorder, attention deficit/hyperactivity disorder (ADD/ADHD), other learning disability, bipolar disorder, or other psychiatric diagnosis, obtained from patient and parents via standardized questionnaire. A standardized documentation template in the EHR was used by physicians to capture details of the injury at initial visit, as well as current symptom burden via age-appropriate standardized symptom questionnaire, self-reported date of return to symptom-limited exercise (defined as any exertional activity beyond walking), and a clinical examination focusing on the visual and vestibular systems (visio-vestibular examination [VVE]) from both initial and follow-up clinical visits through the end of their clinical course of care.
At each clinical visit, patients completed the Post-Concussion Symptom Inventory (PCSI), with versions validated in children as young as age 5 years, reporting symptoms present at both a preinjury and current postinjury timepoint and has been described previously. 30 For this investigation, a PCSI emotional symptom score was calculated from the 4 questions assessing irritability, sadness, nervousness, and feeling more emotional for teenagers (ages 13-18 years). The PCSI emotional symptom score for children (ages 5-12 years), included the 3 questions feeling grumpy, feeling sad, and feeling nervous.
Each patient was also assessed using a VVE,6-8 which has been demonstrated to be feasible across different healthcare settings and demonstrates fair to moderate inter-rater reliability, with moderate to substantial intra-rater reliability in this age demographic. 6 The VVE has shown to have strong concussion diagnostic capability,7,9,24 as well as being prognostic for prolonged recovery. 24
Outcomes of Interest
Clinical outcomes evaluated in this study included change in PCSI emotional symptom score from preinjury to initial postinjury visit, time to concussion recovery using time in clinical care (time from injury until last clinical visit) as a proxy that has been defined previously, 2 and time to return to symptom-limited exercise (obtained via patient self-report and documented in the EHR). In addition, we investigated the potential association of visio-vestibular deficits with demographic characteristics and previous history of mental health diagnoses, as well as concussion recovery. We defined prolonged concussion recovery as continuing to be in clinical care for the persistence of concussion symptoms <28 days after injury, 35 and we again examined the PCSI emotional symptom score to assess burden for those with prolonged concussion recovery.
Statistical Analyses
Demographics, injury mechanism, and pre-existing mental health diagnoses of the cohort were summarized with descriptive statistics for all categorical variables. Wilcoxon rank sum test or the Kruskal-Wallis test, where appropriate, were used to examine time to concussion recovery and return to symptom-limited exercise across demographic and preinjury mental health diagnoses. Preinjury mental health diagnoses were assessed as present or not present for each mental health diagnosis, as well as categorized by the total sum of preinjury mental health diagnoses into 4 categories (0, 1, 2, and 3+). We compared the proportion of concussion patients with increases in (worsening of) PCSI emotional symptom score as compared with preinjury emotional symptom score across demographic features and pre-existing mental health diagnoses using Pearson’s chi-square test. A similar analysis was used to compare differences in the proportions of participants with abnormal VVE results across demographics and previous mental health diagnoses. A P value <0.05 was used to determine significance in all analyses. To identify the association of pre-existing mental health risk factors with PPCS, a univariable logistic regression was first used to assess the unadjusted association of each of the selected demographic and preinjury mental health diagnoses with the outcome variable of concussion recovery. To examine the main predictor of the total number of mental health diagnoses, as well as to account for multicollinearity, individual pre-existing mental health diagnoses were removed from the multivariable logistic regression. Multicollinearity was determined by a variance inflation factor >5. The multivariable logistic regression adjusted for sociodemographic and clinical characteristics was found to be associated with PPCS in the univariable analysis with a P value <0.05. Adjusted odds ratios and their 95% CIs were used to describe the relationship between previous mental health diagnoses and the outcome variable of prolonged concussion recovery >28 days after injury. The total number of mental health diagnoses was also incorporated into the model to examine for dose-effect on prolonged concussion recovery.
Results
Demographics, Pre-Existing Mental Health Diagnoses, and Injury Characteristics
A total of 3105 pediatric patients, ages 5 to 18 years, diagnosed with concussion, were included in this study. Demographics, including age and sex, as well as injury mechanism (sport or nonsport mechanism of injury [MOI]) are listed in Table 1. Of the 3105 patients, 2150 (69%) reported no pre-existing mental health diagnoses. Relevant previous mental health medical history for enrolled participants included anxiety (18%), ADD/ADHD (13%), learning disabilities (10%), depression (9.5%), disordered eating (1.0%), and bipolar disorder (0.7%).
Characteristics of concussion registry cohort
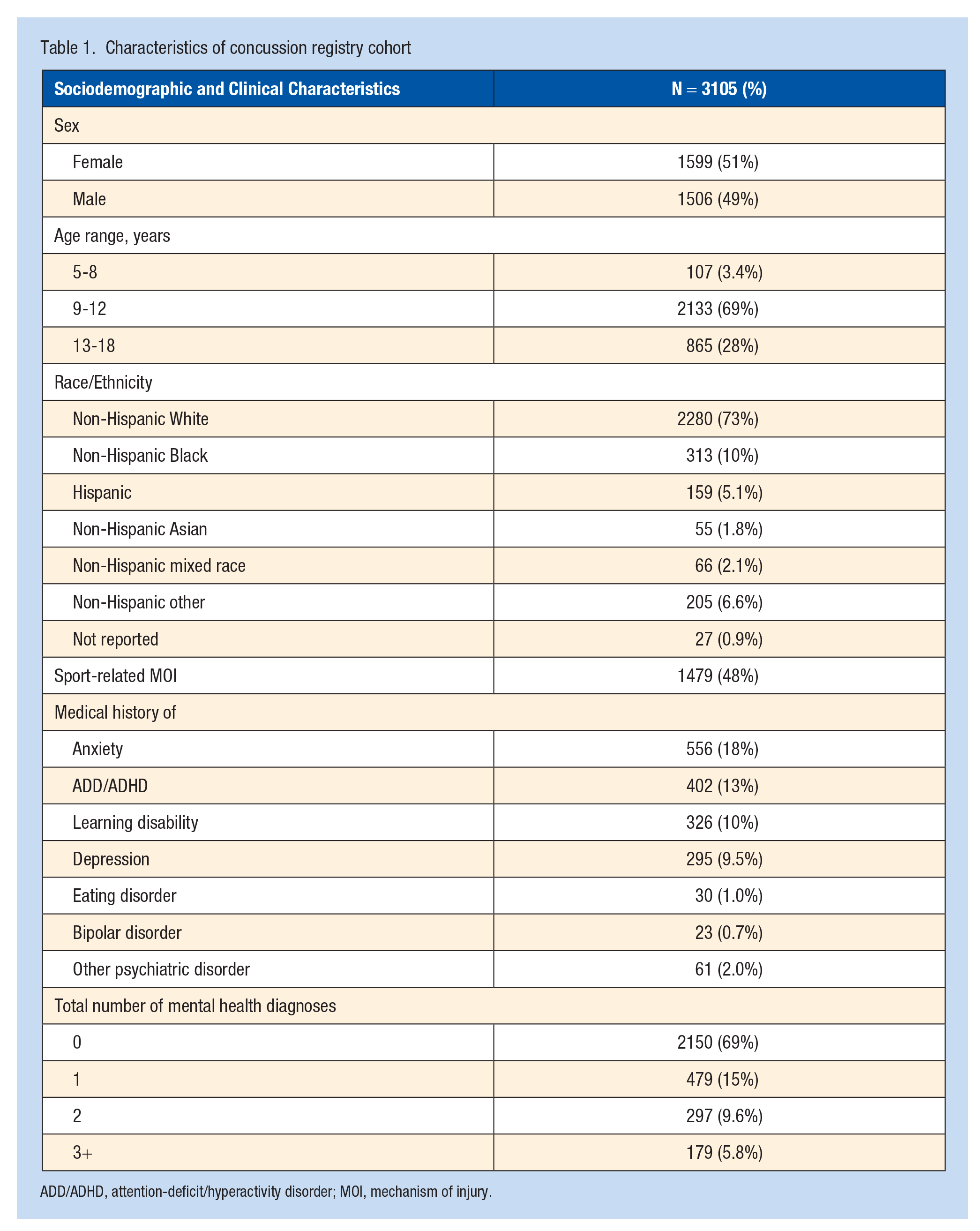
ADD/ADHD, attention-deficit/hyperactivity disorder; MOI, mechanism of injury.
Concussion Recovery
The median days for concussion recovery varied by preinjury mental health diagnosis (Table 2). In days to recovery, those with anxiety (32, IQR [17, 73.5] vs 26, IQR [13, 56]; P < 0.01), learning disabilities (33.5, IQR [15, 81] vs 26, IQR [13, 56]; P < 0.01), depression (34, IQR [18, 72] vs 26, IQR [13, 57]; P < 0.01), and disordered eating (44.5, IQR [21, 91] vs 27, IQR [14, 58]; P < 0.05) all took significantly longer to recover than pediatric patients without those diagnoses. In addition, children and adolescents with any pre-existing mental health diagnosis generally took longer to recover, with a dose-effect response emerging. Median time to recovery increased in stepwise fashion from 25 days (IQR 13, 54) for those with no preinjury mental health diagnoses to a median of 38 days (IQR 18-80) for those with ≥3 pre-existing mental health diagnoses (P < 0.01), and for those with 1 and 2 pre-existing mental health diagnoses recovering in an intermediate 27 (IQR 14, 60) and 32 days (IQR 18, 70).
Influence of mental health diagnoses on concussion recovery
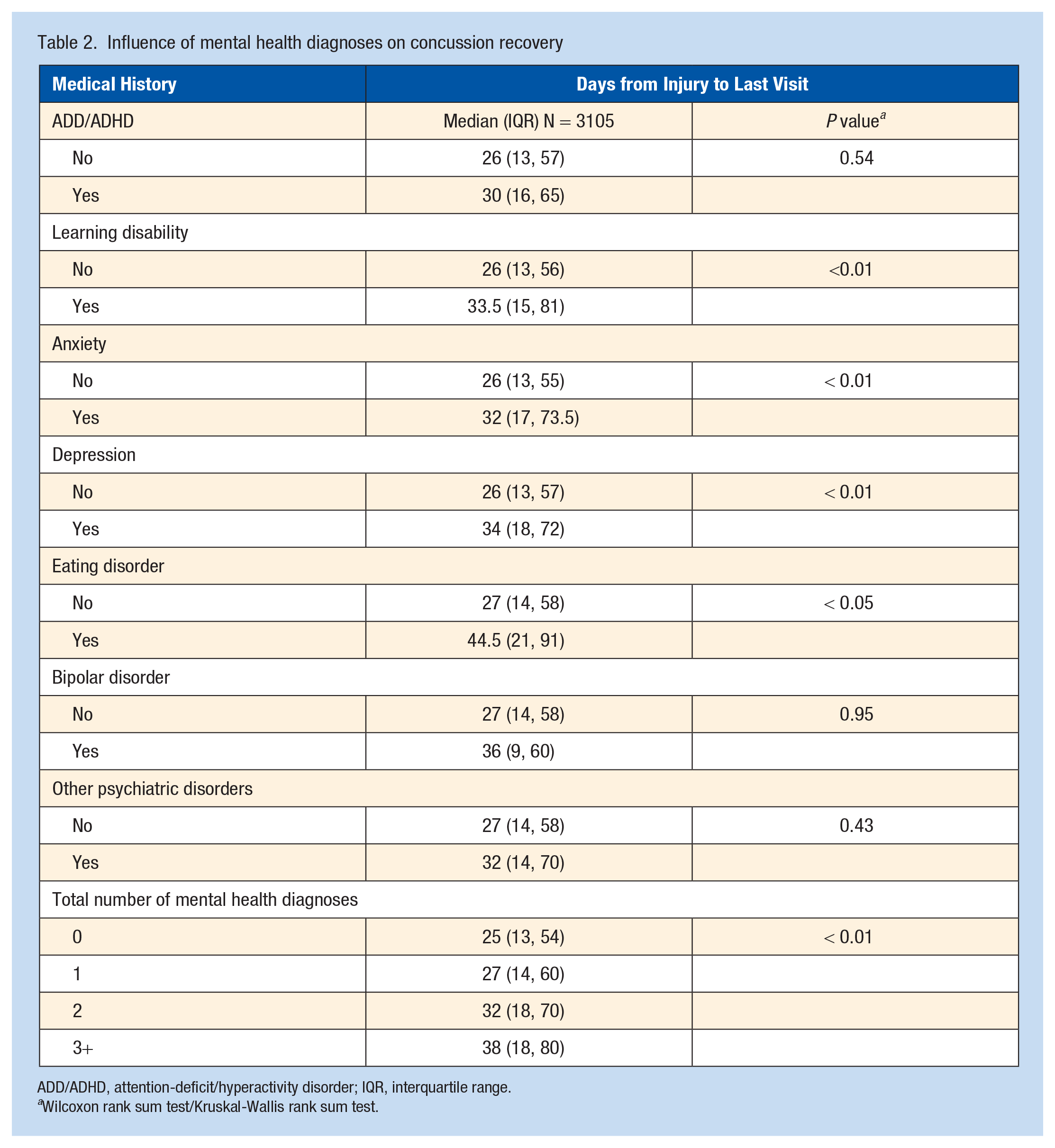
ADD/ADHD, attention-deficit/hyperactivity disorder; IQR, interquartile range.
Wilcoxon rank sum test/Kruskal-Wallis rank sum test.
Risk Factors for Prolonged Concussion Recovery
Of the 3105 concussion patients, 1448 (47%; 95% CI, 45%-48%) had a prolonged recovery. The unadjusted logistic regression analysis evaluating the selected demographics and pre-existing mental health diagnoses of concussion patients as risk factors for prolonged recovery revealed female sex (odds ratio [OR] 2.1; 95% CI [1.8,2.5]), sport-related MOI (OR 0.7; 95% CI [0.61, 0.81], ADD/ADHD (OR 1.3; 95% CI [1.0, 1.6]), learning disability (OR 1.6; 95% CI [1.3, 2.0]), anxiety (OR 1.6; 95% CI [1.3, 1.9]), depression (OR 1.6; 95% CI [1.3, 2.1]), disordered eating (OR 2.3; 95% CI [1.1, 5.2]), bipolar disorder (OR 1.5; 95% CI [0.65, 3.5]), greater number of pre-existing mental health diagnoses (for 3+ mental health diagnoses OR 2.0; 95% CI [1.5, 2.7]), and abnormal VVE at first postinjury visit (OR 4.8; 95% CI [3.9-5.9]) as significant risk factors for predicting prolonged recovery (Appendix Table A1, available in the online version of this article). After adjustment, female sex and sport-related MOI, an increasing number of pre-existing mental health diagnoses (for 3+ mental health diagnoses adjusted OR [aOR] 1.94; 95% CI [1.39-2.70]), and abnormal results for VVE (aOR 4.28; 95% CI [3.48, 5.29]) at first postinjury visit remained significant risk factors for prolonged recovery (Figure 1). Individual mental health diagnoses were excluded from the final regression analysis due to multicollinearity with the total number of mental health diagnoses. In addition, excluding individual mental health diagnoses, rather than the sum of all mental health diagnoses, allowed for examination of the dose-effect response of pre-existing mental health diagnoses. The observed magnitude and direction of association persisted in a sensitivity analysis that excluded 1198 (39%) subjects with missing records for VVE assessment at their initial postinjury visit.
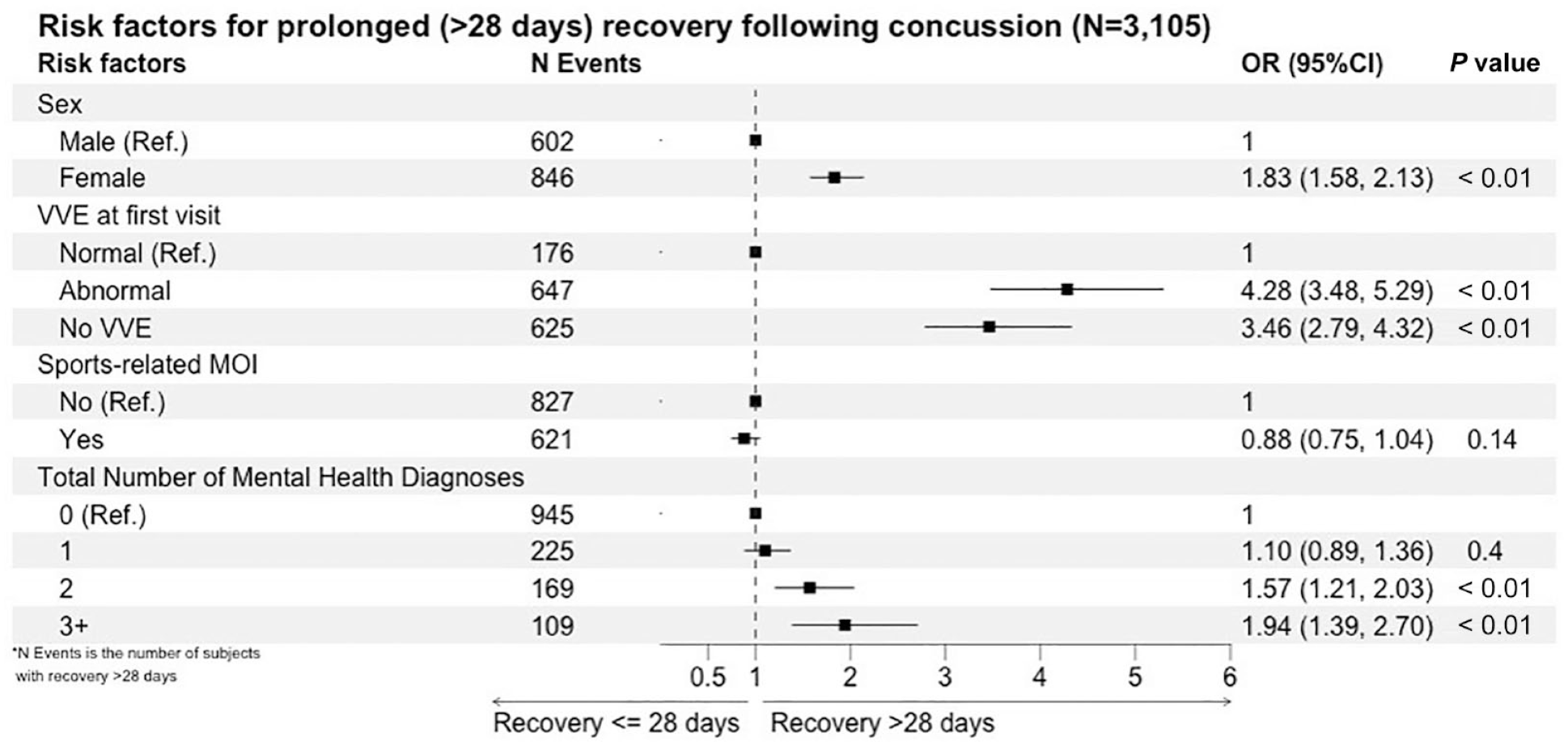
Multivariable logistic regression analysis of risk factors for prolonged concussion recovery. MOI, mechanism of injury; OR, odds ratio; Ref., reference; VVE, visiovestibular examination.
Change in PCSI Emotional Symptom Burden at Initial Postinjury Visit
The proportion of participants whose PCSI emotional symptom score increased from preinjury to initial postinjury visit differed by sociodemographic and clinical characteristics (Table 3). A significantly greater proportion of female patients (32% vs 25% males; P < 0.01), younger children (37% vs 26% adolescents; P < 0.01), and nonsport-related MOI patients (35% vs 23%; P < 0.01) had increased PCSI emotional symptom scores from pre- to postinjury. A significantly greater proportion of the patients with any preinjury mental health diagnosis also demonstrated a significant increase in their PCSI emotional symptom score demonstrating a dose-effect response, with a higher proportion of those with ≥3 pre-existing mental health diagnoses manifesting the greatest increases in emotional symptom burden after concussion (38% vs 34% in those with 2, 30% in those with 1, and 27% in those with no mental health diagnoses; P < 0.01).
Influence of mental health diagnoses on emotional symptom burden after concussion
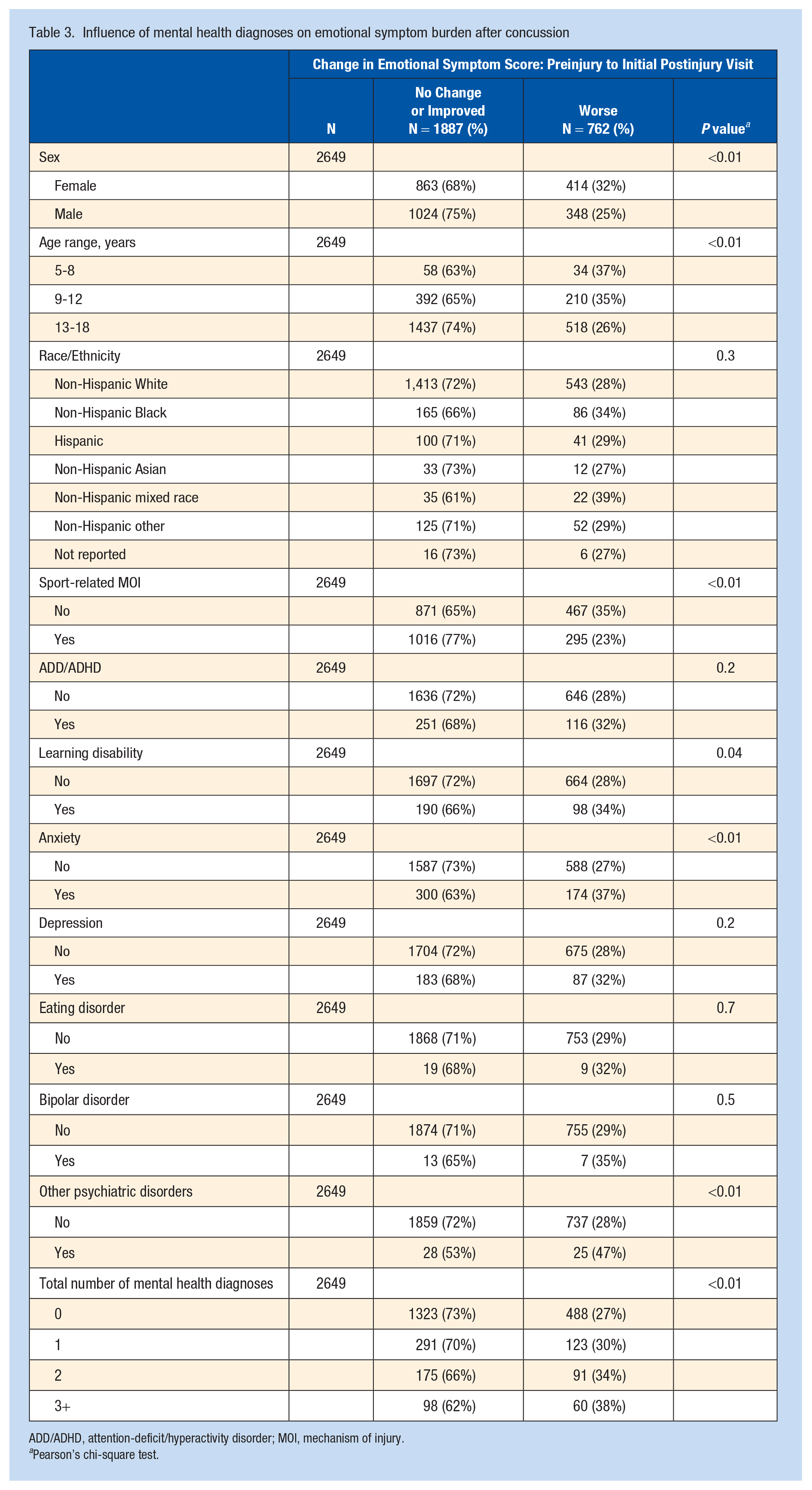
ADD/ADHD, attention-deficit/hyperactivity disorder; MOI, mechanism of injury.
Pearson’s chi-square test.
PCSI Emotional Symptom Burden in Prolonged Concussion Recovery
The PCSI emotional symptom score differed significantly between groups, with male patients (5 symptoms, IQR [1,12] vs 3 in female patients, IQR [0, 8]; P < 0.01), those with nonsport MOI (5, IQR [1, 12] vs 4, IQR [1, 9]; P < 0.05), anxiety (7, IQR [2, 13] vs 4, IQR [0,9]; P < 0.01), depression (8, IQR [3, 14] vs 4, IQR [0,10]; P < 0.01), bipolar (11, IQR [5, 15] vs 4, IQR [1, 10]; P < 0.05), or other psychiatric disorders (8, IQR [5, 14] vs 4, IQR [1,10]; P < 0.01) exhibiting greater emotional symptom burden with prolonged concussion recovery. Patients with 3+ preinjury mental health diagnoses also demonstrated a significantly higher emotional symptom burden (7, IQR [3, 12]) than those with no preinjury mental health diagnoses (4, IQR [0, 9]; P < 0.01). Table 4 displays the comparisons of the PCSI emotional symptom score by pre-existing mental health diagnosis among those patients with PPCS 28 days postinjury (subgroup analysis).
Influence of mental health diagnoses on emotional symptom burden in prolonged concussion recovery
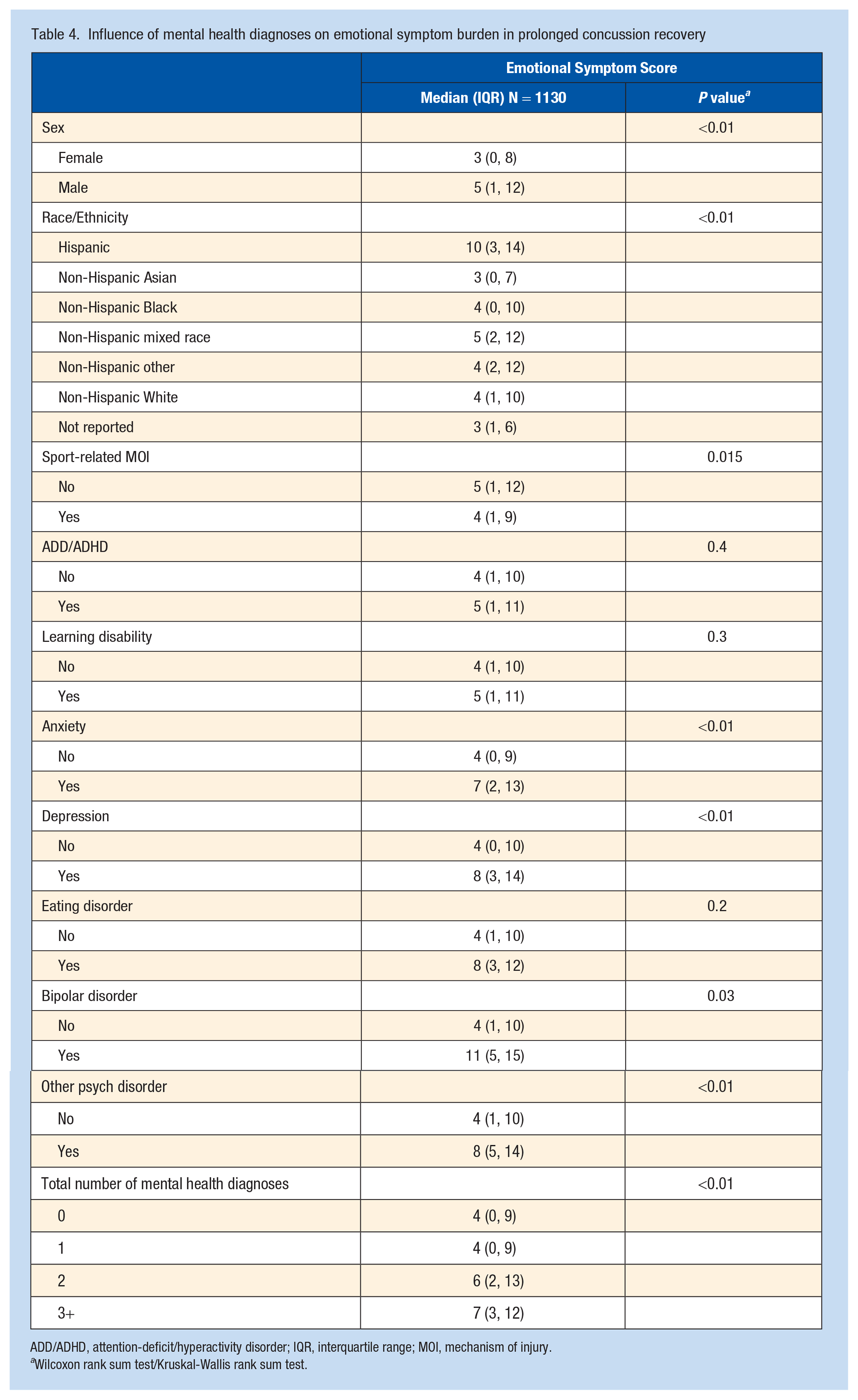
ADD/ADHD, attention-deficit/hyperactivity disorder; IQR, interquartile range; MOI, mechanism of injury.
Wilcoxon rank sum test/Kruskal-Wallis rank sum test.
Visiovestibular Function Association With Demographic Characteristics and Pre-Existing Mental Health Diagnoses
Out of the entire cohort, 1907 (61%) patients had a VVE performed at initial postinjury visit. The proportion of subjects with abnormal VVE results at initial visit was significantly higher in patients with a preinjury diagnosis of anxiety (69% vs 56%; P < 0.01), depression (67% vs 58%; P < 0.01), and any pre-existing mental health diagnoses (P < 0.01) (Table 5).
Association of visiovestibular dysfunction with history of mental health diagnoses
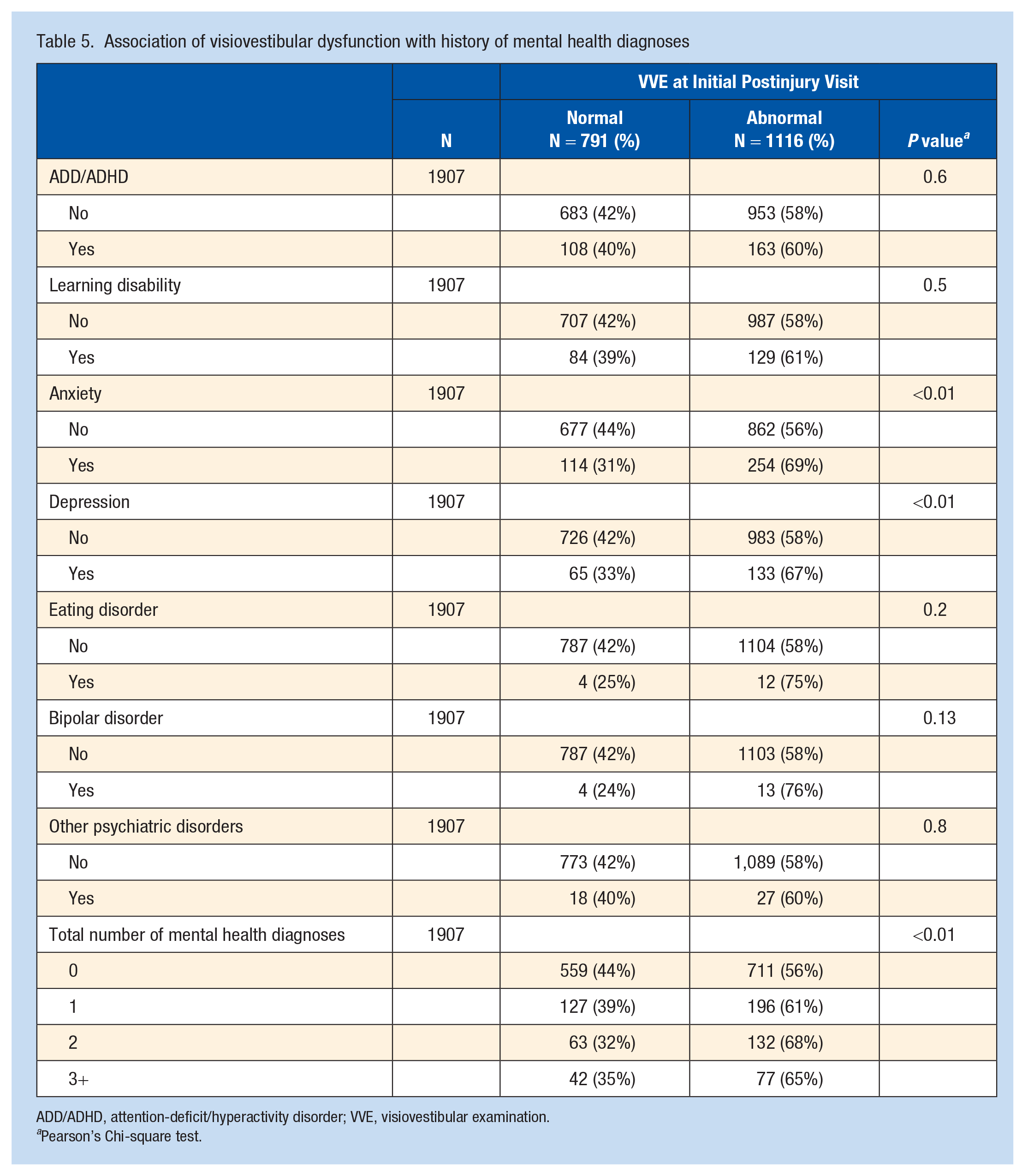
ADD/ADHD, attention-deficit/hyperactivity disorder; VVE, visiovestibular examination.
Pearson’s Chi-square test.
Return to Symptom-Limited Exercise
The median days from injury to return to symptom-limited exercise also varied by sociodemographic and clinical characteristics (Table 6). In our cohort, women (23.5, IQR [14, 38] vs 20, IQR [12, 28]; P < 0.01), older adolescents (22, IQR [13, 33] vs 20, IQR (11, 27] in 5-8 year olds; P < 0.05), and nonsport-related MOI (24, IQR [13, 40] vs 21, IQR [13, 28]; P < 0.01) returned to symptom-limited exercise later. In addition, patients with any previous mental health diagnosis also returned to exercise later (22 days, IQR [12, 30]), with those with ≥3 pre-existing mental health diagnoses returning the latest (23 days, IQR [16, 45]; P < 0.01).
Characteristics of return to symptom-limited exercise after concussion
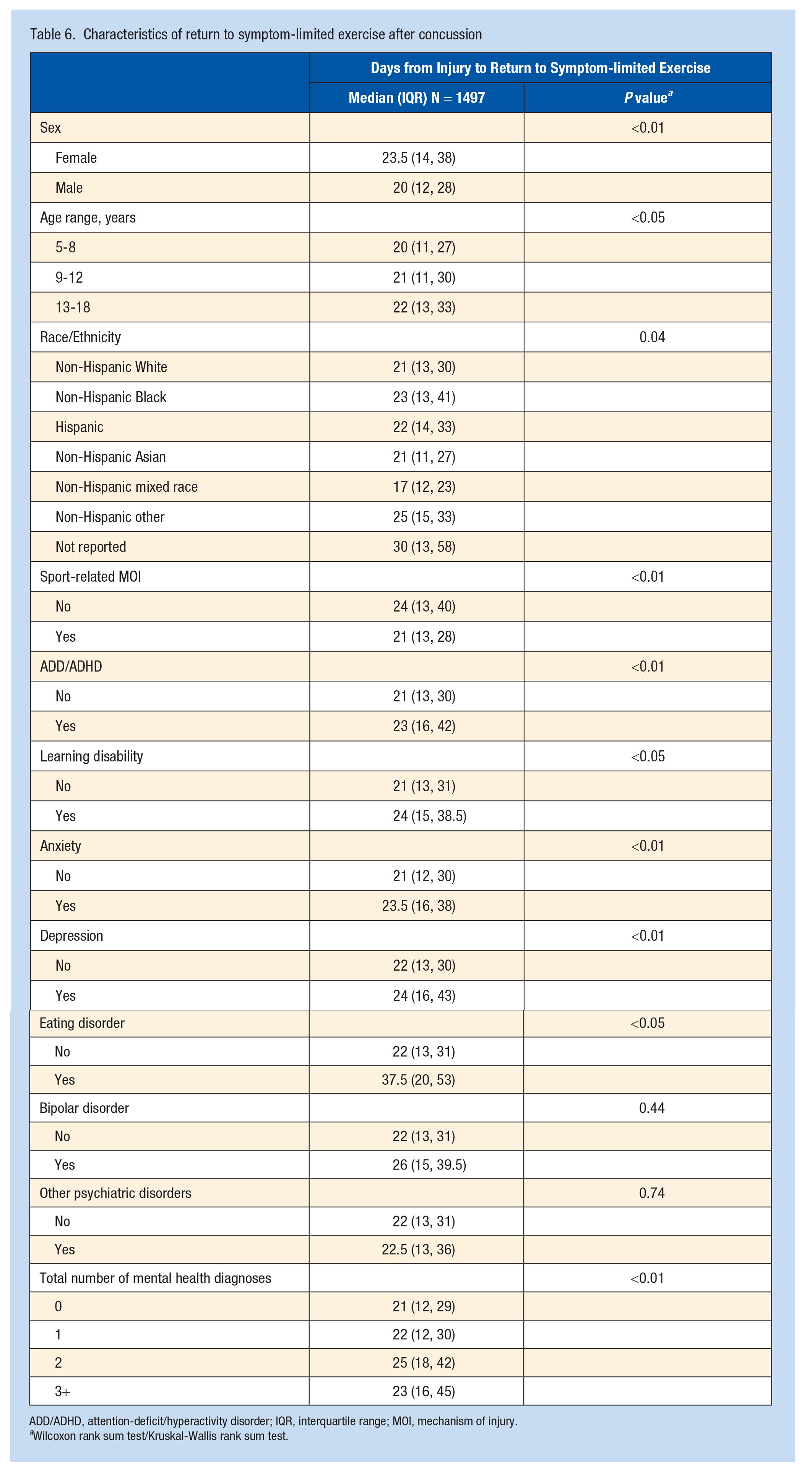
ADD/ADHD, attention-deficit/hyperactivity disorder; IQR, interquartile range; MOI, mechanism of injury.
Wilcoxon rank sum test/Kruskal-Wallis rank sum test.
Discussion
Our analysis of prospectively collected demographic and clinical data from a large registry cohort of pediatric and adolescent patients with concussion demonstrated a substantial burden of pre-existing mental health diagnoses, which had a negative effect on emotional symptom burden after concussion, as well as overall time to recovery from concussion, with implications for clinical management. The rates of pre-existing mental health disorders in our cohort of concussed children and adolescents are higher than in previous reports, including populations of children and adolescents evaluated in the emergency department or the specialty care setting,9,12,35 including our own reports. 9 This may reflect the concerning, ongoing long-term trend that has been reported of the rising prevalence of mental health disorders overall among pediatric patients,31,34 making this an important area for research with substantial clinical implications for the management of pediatric concussion. When examining the direction of emotional symptom burden after concussion, being female, an older adolescent, and having a nonsport MOI were all risk factors for experiencing an increase in emotional symptoms after concussion. In general, those with pre-existing mental health disorders were more likely to experience increases in their emotional symptom burden as assessed by the emotional symptom score on the PCSI. An important clinical implication of our results is the apparent dose-effect of pre-existing mental health conditions and risk for increased emotional symptom burden after concussion, with a greater number of diagnoses predicting a greater change in emotional symptom burden after concussion. This finding underscores the importance of identifying and addressing pre-injury mental health diagnoses, particularly those with >1 diagnosis. Screening, supporting, and referring those patients, when necessary, for additional care is essential.
Regarding concussion recovery, findings from our cohort support previously published data indicating that female sex is a risk factor for a recovery taking >28 days. 35 In our analysis of this cohort, having any preinjury mental health diagnosis, anxiety, a learning disability, disordered eating, or depression were also risk factors, with a dose-effect for those with ≥3 pre-existing mental health diagnoses taking the longest to recover. An important consideration is the fact that many of these mental health diagnoses co-occur. For instance, eating disorders are often associated with anxiety and depression, as is ADD.14,33 These co-occurring mental health diagnoses may present particular barriers to recovery from concussion and may require specialized treatment. Early recognition of these factors with earlier intervention to support these pediatric patients may potentially have a positive impact on outcomes for those with mental health diagnoses, often multiple, co-occurring with concussion.
As expected, our examination of the PCSI emotional symptom score found that those with prolonged recovery with any pre-existing mental health diagnoses had higher emotional symptom burden than those without any mental health diagnoses. However, we found unexpectedly that boys with prolonged recovery had a higher emotional symptom burden than girls with prolonged recovery. This was despite the fact that, overall, girls were more symptomatic acutely after concussion. These findings may indicate that boys with prolonged recovery are a distinct subcohort, warranting further research to understand the various factors contributing to both prolonged recovery, as well as greater relative emotional symptom burden. In addition, the clinical implications to these findings would indicate that active screening, support, and potential early referral for psychological counseling are important interventions to consider in men with persistent postconcussive symptoms.
Our investigation in this cohort found a greater burden of visio-vestibular dysfunction in those with previous mental health disorders, which is a new finding. As a descriptive study, we are not able to determine causality in this relationship; however, the clinical implications are clear: since visio-vestibular dysfunction represent an added symptom burden for pediatric patients with concussion, addressing these deficits in patients with pre-existing mental health disorders may serve to substantially reduce the overall symptom burden in this population. This underscores the importance of a VVE in identifying those at risk for prolonged concussion recovery. In addition to addressing pre-existing mental health disorders, identification of these VVE deficits present targets for active intervention, including active rehabilitative approaches, such as a home visio-vestibular exercise program or formal visio-vestibular physical therapy, for such deficits.29,32 Active management of pediatric patients with concussion with visio-vestibular dysfunction, early initiation of a visio-vestibular home exercise program, or referral for visual or vestibular rehabilitation may reduce some of the concussion symptom burden experienced that may add to the emotional symptom burden in these patients who already have substantial pre- and postinjury mental health burden.
We also examined time to return to symptom-limited exercise after concussion in our cohort because of the important role that early exercise has been demonstrated to play in ameliorating concussion, influencing concussion symptom resolution and time to recovery. In this cohort, female patients, older adolescents, and those with nonsports MOI returned later to symptom-limited exercise compared with their counterparts. Again, across the board, those with pre-existing mental health diagnoses also returned to exercise later, with those having >1 mental health diagnosis returning the latest. Our study design is not able to determine causality in this relationship, whether the mental health diagnoses represented barriers to return to exercise or exercise intolerance prevented earlier return. Nonetheless, this represents an important opportunity for intervention for clinicians. A simple recommendation for symptom-limited exercise shortly after a concussion may have a substantial impact on outcomes for this particularly vulnerable population, reducing concussion symptom burden in those with already higher mental health and emotional symptom burden. 17
Limitations
Our investigation of this prospective registry cohort of pediatric patients with concussions has limitations. An inherent limitation in our study is the potential for undiagnosed mental health disorders in the population who would then also be at risk for prolonged recovery; this limitation, however, would decrease the effect size in recovery time detected between those with and without mental health disorders, indicating that the effect of pre-existing mental health disorders is likely robust, in light of our findings. Our cohort was a specialty care population, which may not be representative of all children and adolescents with concussion who might present to different settings of care such as the emergency department or primary care office. The cohort was also primarily non-Hispanic white, which is not reflective of the general population, and likely reflects important underlying disparities in concussion awareness, identification, and access to care: an area warranting ongoing study to determine the best means by which we can close this gap. In addition, this was not a comprehensive analysis of all the potential factors that may play a role in concussion outcomes, but a focused investigation of the particular impact that pre-existing mental health diagnoses may have on concussion outcome and their interaction with visio-vestibular dysfunction and return to symptom-limited exercise. As a prospective registry of clinically obtained data, another limitation is the missing VVE data for 1198 (39%) of the cohort. To address this, we conducted a sensitivity analysis removing this subcohort and found no change in the observed association.
In addition, as an observational study, we are unable to account for directionality in any inter-relationships in terms of causation. It is possible that the subgroups in our cohort who returned to symptom-limited exercise later were unable to do so due to exercise intolerance and not simply a lack of awareness or recommendation that it was safe and beneficial to do so.
Conclusion
Attention to pre-existing mental health diagnoses as a burden that pediatric patients bring with them to an injury is a critical component of the clinical care of children and adolescents with concussion. In particular, the presence of previous mental health diagnoses, in a dose-response fashion, are associated with greater emotional symptom burden after concussion and prolonged recovery as well, representing important factors in the management of these patients. While female patients continue to appear to have a greater symptom burden after concussion, including emotional symptoms, our study indicates that it is important for clinicians to recognize that male patients with prolonged recovery from concussion may experience greater emotional symptom burden than female patients. Based on our results, providing active management of visio-vestibular dysfunction and recommending symptom-limited exercise, along with providing early support and therapy for emotional symptoms, may have a substantial ameliorative impact on quality of life for these patients with previous mental health diagnoses.
Supplemental Material
sj-docx-1-sph-10.1177_19417381241228870 – Supplemental material for Dose-Response Effect of Mental Health Diagnoses on Concussion Recovery in Children and Adolescents
Supplemental material, sj-docx-1-sph-10.1177_19417381241228870 for Dose-Response Effect of Mental Health Diagnoses on Concussion Recovery in Children and Adolescents by Christina L. Master, Daniel J. Corwin, Daniele Fedonni, Steven B. Ampah, Kaitlyn C. Housel, Catherine McDonald, Kristy B. Arbogast and Matthew F. Grady in Sports Health
Footnotes
The following author declared potential conflicts of interest: C.L.M. has received speaking fees from the AAP, AAOPT, Indiana University, Nationwide Children’s Hospital, and NYU Concussion.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding received from National Institute of Neurological Disorders and Stroke (Award numbers 1K23NS124986-01, 1K23NS128275-01, and 5TR01 Act NS097549 Project 06 Year) and the Children’s Hospital of Philadelphia Frontier Program.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.