
Abstract
Neonatal intensive care unit (NICU) co-occupations may impact parent–infant outcomes. The main objective of this study was to explore relationships between parent and infant outcomes based on whether sensory-based interventions (co-occupations) occurred most often between parent–infant dyads or provider/volunteer–infant dyads. Thirty-five families received the Supporting and Enhancing NICU Sensory Experiences (SENSE) program, which includes education defining specific amounts of sensory exposures for infants to receive each day of NICU hospitalization (with a preference for parent delivery). Infant sensory experiences in the NICU were logged, and dyads were grouped based on who conducted most of the sensory interventions with the infant in the NICU into a Parent–Infant Co-occupation group or Other Administered group. The Parent–Infant Co-occupation group had infants with less lethargy on the NICU Network Neurobehavioral Scale (p = .04), and parents with lower scores on the Parental Stress Scale (p = .003) and State-Trait Anxiety Inventory-state (p = .047). Parent–infant engagement in co-occupations was related to parental mental health and infant neurobehavior.
Keywords
Introduction
Co-occupation is defined as the phenomenon when two or more people engage in a mutual occupation or meaningful activity (Pierce, 2009). This definition has been expanded to include the varying degrees of collective physicality, emotionality, and intentionality inherent in co-occupations, viewing these occupations on a continuum from those required for survival or “essential” to “complex” activities involving shared plans and coordinated actions (Pickens & Pizur-Barnekow, 2009). Theoretically, it is thought that participation in co-occupation contributes to quality of life, with deprivation in co-occupational opportunities seen as disruptive to health and well-being (Pickens & Pizur-Barnekow, 2009).
A main area of interest has been parent–child co-occupations (Pierce, 2009). Co-occupations in infancy and childhood have typically focused on activities such as feeding, bathing, other caregiving activities, and adult–infant play (Aubuchon-Endsley et al., 2020). Both qualitative and quantitative methodology have been employed in the study of this construct (Pickens & Pizur-Barnekow, 2009). Co-occupation within the neonatal intensive care unit (NICU) is an emerging area of interest within occupational science (OS) and occupational therapy (OT). Although OTs have long focused on the importance of facilitating parent–infant co-occupation within this setting, the literature on this construct within the NICU context remains relatively sparse (Cardin, 2020). The provision of sensory interventions to the NICU infant by an adult requires engagement of both parties, with the intention to foster positive experiences to improve infant outcomes. Thus, the provision of positive sensory experiences, such as skin-to-skin care, has also been defined as a co-occupation specific to the neonatal period (Fraga et al., 2019) and has important benefits for both the parent and infant (Gupta et al., 2021). Furthermore, NICU co-occupations can also include other sensory activities like gentle human touch, massage, and reading to the infant.
“Doing with,” “doing to,” “doing for,” and “doing because of” are categories of co-occupation between mother–infant dyads (Doidge, 2012). Even though it is most often the parents who engage in skin-to-skin care co-occupations with their infants, other sensory-based co-occupations can also be conducted by health care professionals and/or volunteers. Therefore, the constructs of “doing with,” “doing to,” “doing for,” and “doing because of” may differ when considering parent–infant versus other adult–infant dyadic co-occupations in the NICU. While literature describes co-occupations between parents and infants, there is no literature, to our knowledge, that specifically defines co-occupations between preterm infants and other adults in the NICU, beyond the parent–infant dyad. Thus, it remains unknown if infants derive similar benefits from engagement in co-occupations with other adults in the NICU as they do through engagement with their parents.
Several studies from diverse disciplines have evaluated constructs closely related to parent–infant co-occupation using varying terminologies such as parental involvement (Skene et al., 2012), presence (Reynolds et al., 2013), engagement (Vittner et al., 2019), and participation (Pineda et al., 2018). Others have defined the time parents spend in the NICU engaging with their infants and related it to parent and infant health outcomes (Klawetter et al., 2019). The constructs of shared physicality, emotionality, and intentionality that is characteristic of co-occupation have been associated with reciprocity, with preliminary evidence describing changes in the expression of reciprocity in co-occupations as infant development progresses across the first 18 months (Aubuchon-Endsley et al., 2020). In addition, co-occupational engagement has been described as being related to the development of infant identity through attachment, joint attention, intersubjectivity, and synchrony between the mother–infant dyad (Whitcomb, 2012).
Within the NICU environment, co-occupation activities have been described as the vehicle through which meaning in mother–infant relationships is produced and embedded (Price & Miner, 2008). This relationship is fundamental as a platform to enable occupations and promote socio-emotional development for the mother–child dyad (Price & Stephenson, 2009). Maternal co-occupations within this context are believed to emerge gradually and are related to the medical and physiological stability of the infant as well as the parents’ conceptualization of their role (Fraga et al., 2019). Parental role development within the NICU is complex, with parents highlighting mixed feelings associated with their ability and confidence in caring for their infant (Obeidat et al., 2009). In addition to challenges in establishing their parental role, parents may also experience anxiety and depression (Harris et al., 2018).
Parents report difficulty engaging in co-occupations with infants in the NICU due to the practical challenges of maintaining proximity to the infant and having to balance the additional cognitive demands of monitoring the infants’ medical and behavioral state during engagement while juggling their relationship with NICU staff (Cardin, 2020). These factors may all contribute to stress related to being a NICU parent and impact the capacity of the parent–infant dyad to engage in co-occupations. Furthermore, the relationship between parental mental health, stress, confidence, and engagement in co-occupations in the NICU has not been fully explored. The actual act of engaging in co-occupations could potentially have a positive impact on all involved parties (Harris et al., 2018; Pineda et al., 2018). Finally, it has been noted that sociodemographic factors may impact parental engagement within the NICU (Pineda et al., 2018; Whitehill et al., 2021). Such contextual factors related to parental occupational engagement within the NICU are important to consider.
The Supporting and Enhancing NICU Sensory Experiences (SENSE) program has been designed to enhance parent-infant co-occupations in the NICU and improve the health and well-being of both parents and preterm infants. Parents are educated to provide specific doses of daily positive sensory exposures to their infants that are tailored to the infants’ postmenstrual age (PMA) and tolerance (Pineda, Smith, et al., 2021). However, parents may not be able to be present in the NICU regularly to engage in these sensory exposures with their infants. Therefore, the use of surrogates/volunteers has been suggested, successfully implemented, and studied (Clubbs et al., 2019). The use of volunteers to read and or provide touch, when parents were not available to engage in the daily recommended positive sensory exposures with their infants, has been deemed acceptable by parents (Lisle et al., 2022; Pineda et al., 2020). Of all the infants enrolled in a previous pilot study and randomized control trial (RCT) on the SENSE program, 85% had the majority of their positive sensory experiences conducted by their parents, while the remainder engaged in most of the experiences with volunteers or health care professionals (Pineda, Roussin, et al., 2021). Although more maternal confidence and better infant neurobehavioral outcomes have been reported among infants engaging in the SENSE program (Pineda et al., 2020; Pineda, Smith, et al., 2021), it is unclear if there are differences in parent and infant outcomes among infants who received most of the sensory exposures from their parents, compared to those who received most of the sensory exposures from health care professionals or volunteers.
This study explored relationships between parent and infant outcomes based on whether sensory-based interventions (co-occupations) occurred most often between parent–infant dyads or provider/volunteer-infant dyads.
Methods
The study site institutional review board approved the study, and parents signed informed consent. The sample size was predetermined, as this study used a sample from two overarching studies (Pineda et al., 2020; Pineda, Smith, et al., 2021) aimed at evaluating the feasibility and efficacy of the SENSE program. Infants were hospitalized in an 85-bed (which transitioned to a 132-bed) level IV NICU during the study period. Infants born ≤32 weeks estimated gestational age (EGA), with no congenital anomalies, were enrolled within 7 days of birth. Families from the overarching studies were included if they received the SENSE program, had at least 75% of the suggested multimodal sensory exposures from week 2 of enrollment until NICU discharge and had parent mental health and infant neurobehavioral outcomes reported at discharge. Multimodal sensory exposures from the first week were not considered in the inclusion criteria, as there could be significant variability in reported sensory exposures during the first week due to the timing of enrollment and medical factors.
Data Collection
Sensory-based intervention/Co-occupational engagement: The SENSE program included parent education with the intent for parents to do prescribed amounts of different sensory-based interventions each day of hospitalization. When parents were unable to engage in these co-occupations with their infants, volunteers or health care professionals implemented positive sensory experiences with the infants. Sensory-based activities included activities such as skin-to-skin holding, gentle human touch, talking, reading, or singing to the infant (Pineda et al., 2020). As part of the SENSE program, the amount of time (minutes) and the person engaging with the infant in the activity was documented daily on log sheets at the infant’s bedside throughout hospitalization.
Dyad group designation: Whether most of the sensory-based interventions were done by parents (engaging in co-occupations with their infants) or by health care professionals and volunteers (“others”) was documented and used to designate dyads to a Parent–Infant Co-occupation group or an Other Administered group, with “other” referring to volunteers or health care professionals. This grouping was used as the primary independent variable.
Sociodemographic and infant medical factors: Sociodemographic information was collected via a parent-report questionnaire completed before NICU discharge and contained information on maternal age, education (some college/higher education or below), current employment, annual income (below or above $25,000), insurance type (private or public), infant race (African American/Black or other), infant sex, and the number of siblings.
Infant medical factors were collected from the electronic medical record and contained information on the length of hospitalization, EGA, PMA at discharge, the mode of delivery (Caesarean section or vaginal delivery), whether the infant was part of a multiple birth, birth weight, Apgar scores at 1 and 5 minutes, the number of days the infants received ventilatory support, and co-morbid medical conditions including retinopathy of prematurity (ROP), patent ductus arteriosus (PDA), sepsis, necrotizing enterocolitis (NEC), periventricular leukomalacia (PVL), and any grade of intraventricular hemorrhage (IVH).
Infant neurobehavioral outcomes: At term equivalent age, infants were assessed using the Hammersmith Neonatal Neurological Examination (HNNE) (Dubowitz et al., 1980), and the NICU Network Neurobehavioral Scale (NNNS) (Tronick & Lester, 2013). Both measures have good clinical utility. The HNNE has good sensitivity (82%) to predict abnormalities on magnetic resonance imaging (MRI; Woodward et al., 2004) and has excellent inter-rater reliability (ICC > .74) (Eeles et al., 2017). The NNNS has adequate reliability and validity, with internal consistency alpha ranging from .87 to .90 (Noble & Boyd, 2012; Tronick & Lester, 2013).
Maternal mental health and parenting confidence: A questionnaire containing several self-report measures was completed by parents before NICU discharge. It contained the State-Trait Anxiety Inventory for adults (STAI) (Speilberger, 1968), Edinburgh Postnatal Depression Scale (EPDS) (Cox et al., 1987), Parental Stress Scale (PSS) (Berry & Jones, 1995), Parental Stressor Scale NICU (PSS NICU) (Miles et al., 1993), Parenting Stress Index (PSI) (Abidin, 1995), Maternal Confidence Questionnaire (MCQ) (Zahr, 1991), and the Infant Care Questionnaire (ICQ) (Secco, 2002). The selected measures are well-researched and are accepted measures related to parent outcomes. The STAI (Cronbach’s ɑ: .87–.92), the EPDS (standardized ɑ: .87), PSS (ɑ: .83), the PSS NICU (ɑ = .89), the PSI (ɑ = .96), and the ICQ (Cronbach’s ɑ: .58–.86) are considered to have good reliability (Abidin, 1995; Berry & Jones, 1995; Cox et al., 1987; Miles et al., 1993; Secco, 2002; Speilberger, 1968). Acceptable test–retest reliability has been reported for the MCQ (ɑ = .89) and the PSS (test–retest coefficient of .81) (Berry & Jones, 1995; Zahr, 1991).
Data Analysis
IBM SPSS version 28 (Armonk, NY) was used to run descriptive statistics to report sociodemographic and infant medical characteristics. Independent samples t-tests, Fisher’s exact tests, and Mann–Whitney U-test were used to investigate differences in infant neurological and parent outcomes based on whether the infants were part of the Parent-Infant Co-occupations group or Other Administered group (two-sided, a = .05). Investigations with continuous dependent variables used independent samples t-test. However, when assumptions of normality were not met, the Mann–Whitney U-test was used, and when cell sizes were small, Fisher’s exact test was used.
Results
Thirty-five preterm infants were included from the overarching studies as depicted in Figure 1. Twenty-eight (80%) infants engaged in most of the sensory-based co-occupations described in the SENSE program with their parents and were designated as the Parent–Infant Co-occupation group. Seven (20%) infants engaged in most of the sensory-based interventions with volunteers or health care professionals and were designated as the Other Administered group.

Participant Selection Process From the Two Overarching Studies.
Table 1 reports the sociodemographic and infant medical characteristics of the sample. There were no differences in infant medical characteristics between the groups. Infants who engaged mostly with their parents were more likely to be female (p = .03) and be part of a family with an annual income of more than $25,000 (p = .04).
Sociodemographic Information and Infant Medical Information by Group.
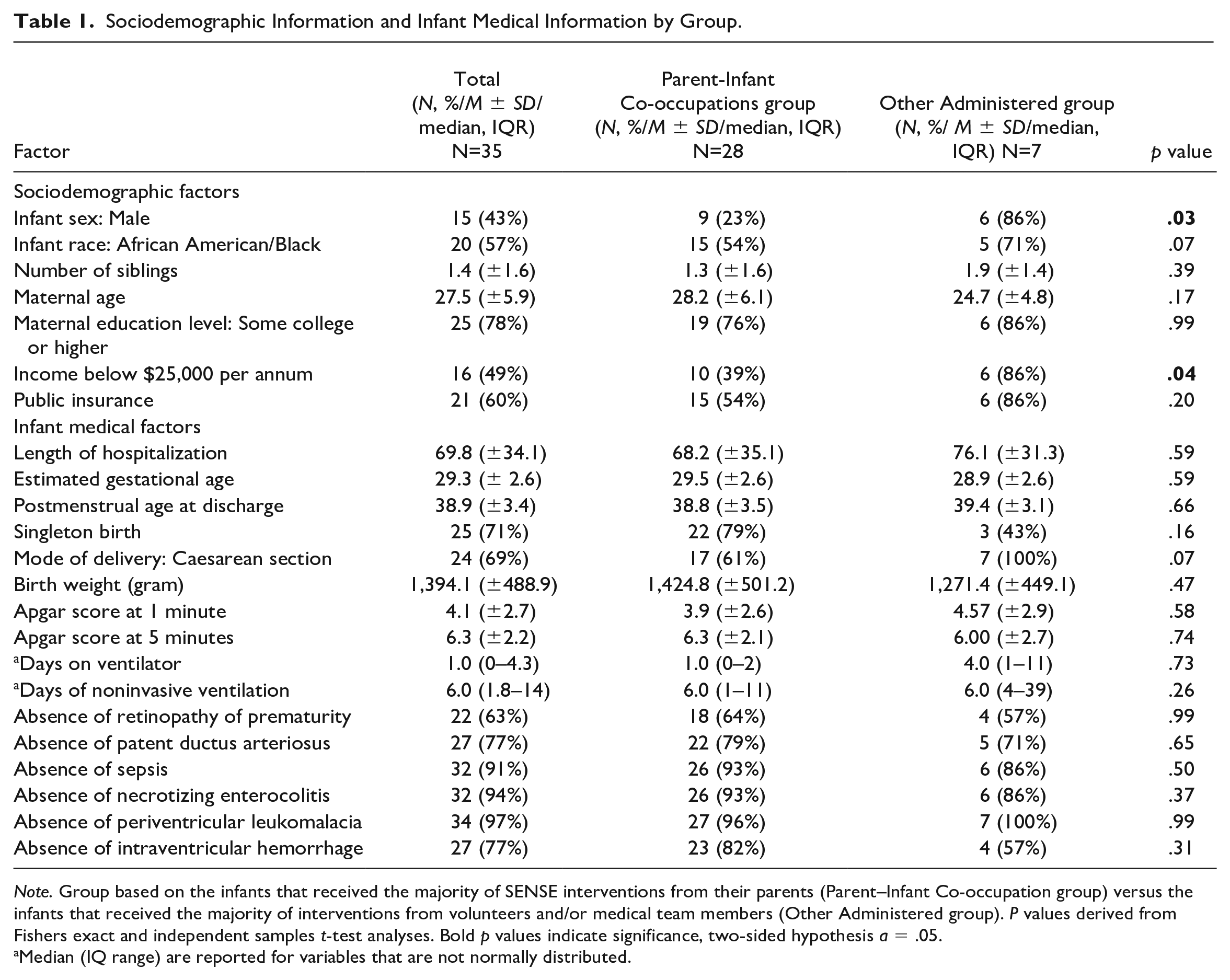
Note. Group based on the infants that received the majority of SENSE interventions from their parents (Parent–Infant Co-occupation group) versus the infants that received the majority of interventions from volunteers and/or medical team members (Other Administered group). P values derived from Fishers exact and independent samples t-test analyses. Bold p values indicate significance, two-sided hypothesis a = .05.
Median (IQ range) are reported for variables that are not normally distributed.
Infant neurobehavioral outcomes at term equivalent age are reported in Table 2. No significant differences were found on the HNNE based on who conducted most of the sensory-based exposures. Infants who formed part of the Parent–Infant Co-occupation group had lower lethargy subscale scores on the NNNS (p = .04). While not significant, associated p values for NNNS attention and regulation subscales were p = .06 for both, with scores trending higher for infants in the Parent–Infant Co-occupation group. No other relationships between the Parent–Infant Co-occupation and Other Administered groups and NNNS scores were observed.
Infant Neurobehavioral Outcomes at Term Equivalent Age by Parent–Infant Co-occupation Group or Other Administered Group.
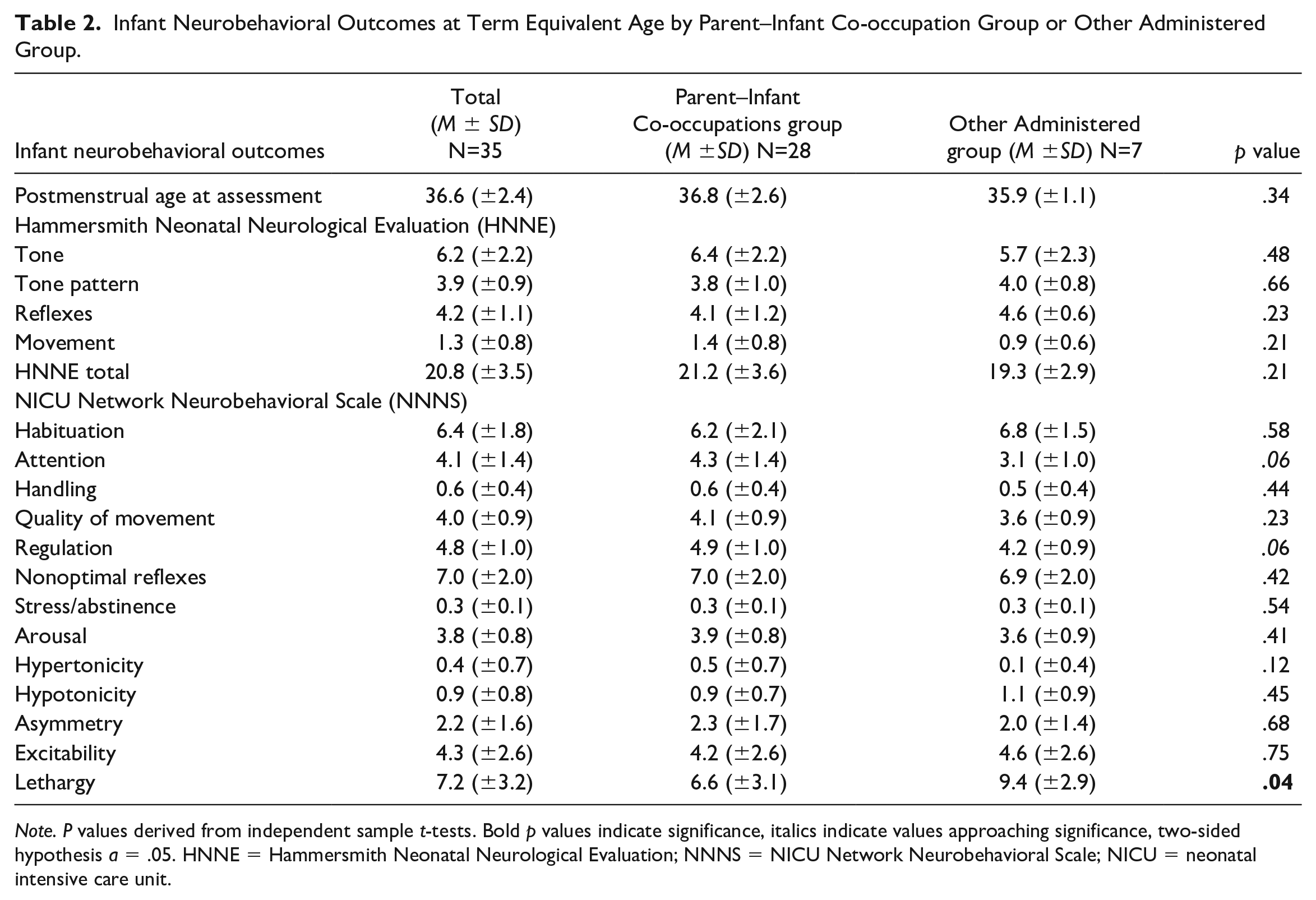
Note. P values derived from independent sample t-tests. Bold p values indicate significance, italics indicate values approaching significance, two-sided hypothesis a = .05. HNNE = Hammersmith Neonatal Neurological Evaluation; NNNS = NICU Network Neurobehavioral Scale; NICU = neonatal intensive care unit.
Parent mental health and parenting outcomes are reported in Table 3. Parents who engaged in the majority of the sensory-based co-occupations with their infants were more likely to have lower STAI-state scores (p = .047). While not significant, the associated p value for STAI-trait was p = .052, trending lower in the Parent–Infant Co-occupation group. Parents in this group also had lower PSS scores (p = .003), PSI stress subscale scores (p = .012), and PSI parent–infant dysfunctional interaction subscale scores (p = .021). No differences were observed in the EPDS, MCQ, ICQ, or PSS NICU scores based on who conducted most of the sensory interventions.
Maternal Mental Health and Parental Outcomes at Discharge Reported by Parent–Infant Co-occupation Group and Other Administered Group.
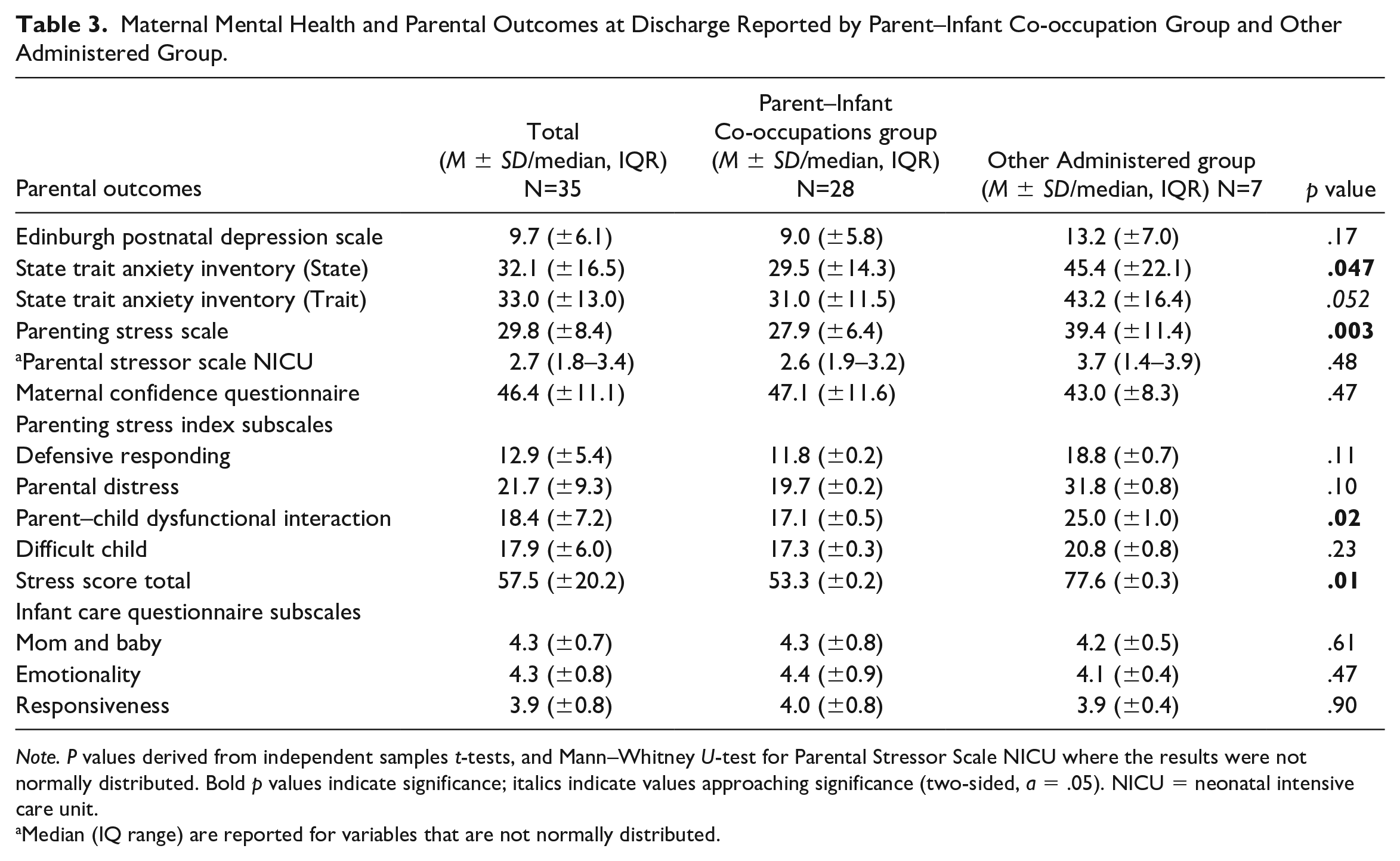
Note. P values derived from independent samples t-tests, and Mann–Whitney U-test for Parental Stressor Scale NICU where the results were not normally distributed. Bold p values indicate significance; italics indicate values approaching significance (two-sided, a = .05). NICU = neonatal intensive care unit.
Median (IQ range) are reported for variables that are not normally distributed.
Discussion
These preliminary results highlight differences in parental stress and anxiety as well as preterm infant neurobehavior related to parent–infant co-occupational engagement compared to sensory-based interventions conducted by health care professionals and volunteers in the NICU. These findings elucidate the importance of parent–infant co-occupations in this setting.
No relationships between infant medical status and the amount of parental engagement in co-occupations in the NICU were observed. These are encouraging results, as it is often reported that interacting and engaging with medically “fragile” infants may hamper engagement in parent–infant co-occupations (Navne et al., 2018). Furthermore, others have reported that parents feel that medical technology is a barrier to their interaction with their infant (Lantz & Ottosson, 2013). However, while medical factors may be a barrier, this study was able to demonstrate that engagement in co-occupations occurs irrespective of the infant’s medical status.
More lethargy was observed among infants in the Other Administered group who had less co-occupational engagement with their parents in this study. This contrasts with previous research that identified more lethargy related to higher parental presence in the NICU (Reynolds et al., 2013). Higher scores on the lethargy NNNS subscale score may be a marker of poorer neurobehavioral performance and has been related to lower language and motor outcomes at 2 years of age in infants born between 32 and 36 weeks EGA (Spittle et al., 2017). Lethargy is an important construct to consider, as some of the sensory-based co-occupations can be performed while the infant is asleep. The infant’s state was not specifically recorded along with the co-occupation that they were engaging in. Sleep has been described as an essential occupation that is important for development and also for fostering a sense of belonging and identity (Leive & Morrison, 2020). The process of preparing for sleep and going to sleep is an essential co-occupation (Aubuchon-Endsley et al., 2020). Although co-occupations typically are implied to be performed by the parent–infant dyad while both are awake, it could be argued that shared intentionality may be present in an activity, such as skin-to-skin holding or gentle human touch, if it is given by a parent or a volunteer to facilitate infant sleep and state regulation. Furthermore, increased attention and regulation scores, along with more optimal lethargy scores have been related to improved cognitive outcomes in infants at age 2 (Spittle et al., 2017). As such, the outcome of less lethargy in infants who engaged in most of their positive sensory co-occupations with their parents, along with higher attention and regulation scores that trended toward significance, suggests the need for further exploration.
The lack of relationships between parent–infant co-occupations versus sensory-based interventions administered by health care professionals or volunteers on other neurobehavioral outcomes (except lethargy) can also provide some insights into the potential importance of others providing sensory-based interventions when parents cannot be present. Similarities in many of the infant neurobehavioral outcomes between the two groups are encouraging preliminary evidence for the potential role of volunteers/surrogates to step in as co-occupational partners with infants when parents are unable to be present in the NICU. Parental presence and holding have been described as a neuroprotective factor to mitigate some of the potential negative effects related to noxious overexposure in the NICU environment (Reynolds et al., 2013). However, many families face broad challenges that may limit their availability to be present and interact with their infants in the NICU (Head Zauche et al., 2020). Although mitigating these factors to encourage optimal parental engagement in the NICU is the priority, this might not always be feasible. There may be a need for volunteers to step in as temporary, surrogate co-occupational partners to provide positive sensory exposures to high-risk infants in the NICU. This can decrease possible occupational deprivation experienced by infants with limited parental presence in the NICU. Co-occupational deprivation, as a potential influence on outcomes when surrogates are not available, is an important area for future inquiry. Future studies are also needed on the use of sensory support teams in the NICU to augment interactions conducted by parents to decrease the risk of occupational deprivation for infants experiencing low parental presence in NICUs. This could hypothetically equalize the developmental benefits that infants may experience from engagement in positive sensory-based co-occupations.
There were relationships between parent–infant engagement related to sociodemographic factors, which is consistent with other reports (Pineda et al., 2018). Previous studies have noted that families experiencing sociodemographic challenges may face significant barriers to being present in the NICU (Sigurdson et al., 2020; Whitehill et al., 2021). Families who perceive the NICU as more stressful may have lower presence during their infants’ hospitalization (Head Zauche et al., 2020). Parents who have received the SENSE program have reported that the use of volunteers engaging in co-occupations with their infants did put them at ease when they were unable to attend frequently (Lisle et al., 2022); however, this did not seem to decrease their reports of stress. With relationships observed in this study between parents conducting most of the sensory-based interventions and decreased reports of parental stress, it remains unclear whether engagement in more co-occupations with the infants played a role in decreasing parental stress and anxiety in this group or if parents with more stress experienced more barriers to engaging in co-occupations with their infants.
Through engagement in co-occupations, enhanced confidence and competence within the parental role have been reported (Price & Stephenson, 2009). In addition, more engagement in the NICU has been related to less parental role alteration and more parenting confidence (Harris et al., 2018). However, our results on participating in co-occupations in the NICU did not align with these findings. In our sample, there were no differences in either maternal confidence at discharge or perceived competence in parenting related to more parental engagement in co-occupations during NICU hospitalization. Future trials to explore this using properly powered samples are warranted.
It is possible that the beneficial effects of engaging in co-occupations reported in other studies may be negated by the stressful nature of the NICU admission. Facilitating co-occupations has been highlighted as an important factor to empower parents to advocate more effectively for their child’s needs in the case of older children with disabilities (Price & Stephenson, 2009). It may be important for occupational therapists to explore barriers that families may face in terms of accessing the NICU and engaging in co-occupations while they are present to ensure that parents have the opportunity to engage in positive co-occupations with their infants. Parents may need additional support beyond the reassurance that their infant is receiving positive sensory experiences in their absence to effectively implement holistic family-centered care tailored both to the occupational needs of the infants as well as their parents during the NICU admission.
This study had several limitations. The first relates to the measure of co-occupation. Co-occupational engagement was logged as time spent engaging with the infant in sensory-based activities, which largely relates to only one dimension of co-occupation: shared physicality. Shared intentionality and emotionality are presumed to be present; however, these constructs were not specifically documented or tracked throughout the study. In addition, it is possible that families with lower levels of engagement in the sensory-based co-occupations may have been engaging in other untracked co-occupations (such as feeding, bathing, or other caregiving activities), and the effect would not be fully represented within the data for this study. Finally, the exclusion of infants with low levels of engagement in sensory-based co-occupations for this analysis did limit potential confounding effects of tailored sensory exposures on infant neurobehavioral outcomes; however, it may also have removed a subset of families who may have been facing additional barriers or challenges that were not adequately substituted by volunteer or health care professional supportive interventions. As a secondary analysis of data derived from two overarching studies, this study may not have been sufficiently powered to detect the relationships intended, resulting in risk of type II error, but sets the stage for future inquiry. Due to the multiple relationships assessed in this study, there is risk for type I error. Parental stress and anxiety were measured at NICU discharge and were not specifically recorded during or directly after engagement in co-occupations with their infants, which limits the findings. Furthermore, there are limitations in reporting sensory exposures on bedside logs across different people within the NICU, and the subjective element related to the quality of the interaction or experience (over quantity) is missing from the sensory exposure reporting.
Conclusion
This study showed that parents (compared to others) who participated in most of the documented sensory-based interventions with their infants in the NICU had differences in parental stress and anxiety. Infants demonstrated variation in NNNS lethargy outcomes, yet no other neurobehavioral differences were detected based on group membership between infants who engaged mostly in co-occupations with their parents compared to those that engaged mostly with volunteers or health care professionals during their NICU admission. Parental stress and anxiety should be further explored to determine their significance as barriers or facilitators to engagement in parent–infant co-occupations. The construct of co-occupation requires further expansion and interpretation within the context of the NICU.
Footnotes
Acknowledgements
The authors wish to thank Bethany Gruskin, Delaney Smith, Carolyn Ibrahim, Jessica Roussin, and Tiffany Le for their help with organizing the data from the overarching studies. The authors wish to thank the PhD cohort at the Chan Division of Occupational Science and Occupational Therapy at the University of Southern California for feedback and direction on the first draft of this manuscript.
Research ethics and patient consent
This research was approved by the Human Research Protection Office at Washington University in St Louis, MO, and parents signed informed consent. There was also a ceded review at the University of Southern California.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Two of the authors (J.S. and R.P.) are also authors of the SENSE program. A SENSE program user fee is paid to gain access to the SENSE program for research and clinical practice. The user fee supports the cost of distribution, and the authors do not derive any direct financial benefit from the user fees.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this manuscript was supported by the Gordon and Betty Moore Foundation, the Washington University Institute of Clinical and Translational Sciences grant (grant no. UL1TR002345) from the National Center for Advancing Translational Institute of Health, and the Intellectual and Developmental Disabilities Research Center at Washington University (NIH/National Institute of Child Health and Human Development P30 HD062171).